Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
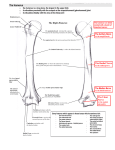
Variations in Measurements of Upper and Lower Ends of Humerus 1 PRIYA RANGANATH†, 2BALASUBRAMANYAM V†† ANJALI T. OLLAPALLY*, ARUN ALEX* & BIBIN SEBASTIAN* 1 Bangalore Medical College & Research Institute, Bangalore 560002, Karnataka 2 St. John’s Medical College, Bangalore 560034, Karnataka KEY WORDS: Measurements. Variation. Humerus. Upper and lower ends. Bangalore sample. ABSTRACT: The present study was conducted on 40 humeri (18 left and 22 right). In this study, at the upper end, the average of the circumference of anatomical neck was 12.98 cm, surgical neck was 8.84 cm, width of bicipital groove was 0.76 cm, surface area of the head was 24.41 sq.cm. At the lower end, the circumference of medial part of trochlea was 5.23 cm, middle part was 3.4 cm, lateral part was 4.3 cm, capitulum was 3.65 cm, length of medial epicondyle was 1.85 cm and volume of olecranon fossa was 1.59 ml. Ten humeri (4 of left side (10%) and 6 of right side (15%)) had supratrochlear foramen. Associate Professor, Anatomy Professor, Anatomy * Students, St. John’s Medical College the acromion in the shoulder region and covered by the deltoid. It produces the shoulder’s round contour. The greater tubercle continues towards the shaft as the lateral lip of the intertubercular sulcus. Between the tubercles is the intertubercular sulcus or the bicipital groove. The upper end of the humerus tapers into the shaft as an ill-defined ‘surgical neck’. The lower end of humerus is wider transversely and has articular and non-articular parts. The articular part joints with radius & ulna at the elbow and is divided into a lateral, convex capitulum and a medial, pulley-shaped trochlea. Non-articular condyle includes medial and lateral epicondyles, olecranon, coronoid and radial fossae. The capitulum is less than half a sphere, it includes anterior and inferior surfaces of condyle laterally, but not its posterior surface. It articulates with discoid radial head, which abuts inferior surface in full extension but slides on to the anterior surface during flexion. The trochlea is like part of a pulley, occupying anterior, inferior and posterior surfaces of humeral condyle medially; it is separated laterally form capitulum by a faint groove; all aspects of its medial margin project. It articulates with trochlear notch of ulna. In extension the South Asian Anthropologist, 2011, 11(2): 181-183 New Series ©SERIALS INTRODUCTION The humerus is the longest and largest bone in the upper limb. It has two expanded portions (the upper and the lower ends) and a shaft. The upper end includes a head, neck and greater and lesser tubercles. The head forms about one-third of a sphere. The articular surface is covered by hyaline cartilage. The humeral articular surface is about four times the area of the glenoid cavity of the scapula, only part of it being in the glenoid contact in any position of the joint. The anatomical neck is a slight constriction directly adjoining the articular head’s margin. It indicates the line of capsular attachment of the shoulder joint, except at the intertubercular sulcus. The lesser tuberosity projects prominently forward just beyond the anatomical neck and continues downwards as the medial lip of the intertubercular sulcus. It has a smooth muscular impression palpable through the deltoid. The greater tuberosity is the most lateral part of the upper end of the humerus and it projects above † †† 181 182 Priya Ranganath, Balasubramanyam V., Anjali T. Ollapally, Arun Alex & Bibin Sebastian inferoposterior trochlear circumference contacts the ulna, but in flexion trochlear notch slides on to the anterior aspect, the posterior being uncovered. The projecting medial trochlear edge is a main determinant of the angulation between long axes of humerus and ulna when the forearm is extended and supinated. The medial epicondyle is a blunt medial projection on the medial condyle; it is subcutaneous and usually visible in passive flexion. Its smooth posterior surface is crossed by ulnar nerve in a shallow sulcus as it enters the forearm, and here the nerve can be rolled against the bone. If it is jarred against the epicondyle, characteristic tingling sensations result. Distally anterior epicondylar surface is marked by attachment of superficial forearm flexors. Medial humeral border ends at medial epicondyle and is distally the medial supracondylar ridge. A deep hollow, olecranon fossa, on the condyle’s posterior surface, proximal to trochlea, contains apex of olecranon in an extended elbow. Its floor is always thin and may be deficient. It is occasionally perforated to form a supratrochlear foramen or septal aperture (Williams,’95). Due to the variations in measurements of the upper and lower ends of humerus and its involvement in various types of fractures, the present study was conducted. MATERIALS AND METHODS The present study was conducted on 40 humeri (18 left and 22 right) of unknown sex and age available at the Department of Anatomy, St. John’s Medical College, Bangalore. The bones were studied for variations in the upper and lower end. The parameters observed were 1. circumference of anatomical neck 2. circumference of surgical neck 3. width of bicipital groove 4. surface area of head 5. circumference of medial part of trochlea 6. circumference of middle part of trochlea 7. circumference of lateral part of trochlea 8. circumference of capitulum 9. length of medial epicondyle 10. volume of olecranon fossa The circumferences, width of bicipital groove at the upper end of bicipital groove, and length of medial epicondyle were measured by using a thread and a ruler. The boundary of the head was traced on a tracing paper and the resulting figure was placed on graph sheet to calculate the surface area. The volume of the fossa was measured by filling the fossa with water and measuring the amount of water using measuring jar. RESULTS In the present study, the following measurements were observed: 1. circumference of anatomical neck: 13.05 cm (left) and 12.92 cm (right) 2. circumference of surgical neck: 8.76 cm (left) and 8.92 cm (right) 3. width of bicipital groove: 0.77 cm (left) and 0.75 cm (right) 4. surface area of head: 23.75 sq.cm (left) and 25.06 sq.cm (right) 5. Circumference of medial part of trochlea was 5.09 ± 0.64 cm (left) and 5.35 ± 0.59 cm (right) 6. Circumference of middle part of trochlea was 3.41 ± 0.46 cm (left) and 3.39 ± 0.48 cm (right) 7. Circumference of lateral part of trochlea was 4.17 ± 0.7 cm (left) and 4.4 ± 0.49 cm (right) 8. Circumference of capitulum was 3.57 ± 0.4 cm (left) and 3.74 ± 0.47 cm (right) 9. Length of medial epicondyle was 1.88 ± 0.39 cm (left) and 3.74 ± 0.47 cm (right) 10. Volume of olecranon fossa was 1.48 ± 0.25 ml (left) and 1.68 ± 0.42 ml (right) Four humeri of left side (10%) and 6 of right side (15%) had supratrochlear foramen. DISCUSSION In the present study of the upper end of humerus, the average of the circumference of anatomical neck was 12.98 cm, surgical neck was 8.84 cm, width of bicipital groove was 0.76 cm, surface area of the head was 24.41 sq.cm. These measurements could not be compared with other authors because of lack of published material. Variations in Measurement of Upper and Lower Ends of Humerus Regarding the lower end of humerus, supratrochlear foramen or septal apertures may occur in 4-13% of individuals, more frequently on the left side and in females. Racial variations of 4.1-58% have been reported (Bergman,’54). In an examination of 1744 arm bones, septal apertures were found in 4.2% of whites and 12.8% of American Negroes (Trotter,’43). In the present study, ten humeri (25%) had supratrochlear foramen. The difference could be due to ethnic variations in the population group studied. The average of the circumference of medial part of trochlea was 5.23 cm, middle part was 3.4 cm, lateral part was 4.3 cm, capitulum was 3.65 cm, length of medial epicondyle was 1.85 cm, volume of olecranon fossa was 1.59 ml. These measurements could not be compared with the other authors, as there was no published information available. The axillary and the posterior circumflex humeral vessels wind around the surgical neck. Dislocations and fractures tend to occur here resulting in injury to the nerve and vessels. Since the head of the humerus does not fit exactly into the glenoid cavity of the scapula, dislocations are very common in the shoulder joint. Fractures are also common at this site, and with the advent of prostheses for compound fractures, a particular size is required for different individuals. So there is a need for manufacturers of prostheses and the orthopedician to know the variations in measurements of the upper end of humerus while using prostheses to suit different population groups. The medial epicondyle can be avulsed by the medial collateral ligaments of elbow joint if the forearm is forcibly abducted. The ulnar nerve can be injured at the time of the fracture, can become involved later in the repair process of the fracture (in the callus), or can undergo irritation on the irregular bony surface after the bone fragments are reunited. Due to fracture at this level, damage to or pressure on the brachial artery can occur; the circulation of the forearm may be interfered with (Snell, 2000). Most adult distal humeral fractures involve the articular surface. Lateral condylar fractures are much commoner than medial fractures. Jupiter has classified bicolumn fractures based on orientation of major fracture lines. The AO/ASIS classification is being used more frequently: 183 Type A: Periarticular / extra-articular distal humerus fractures: A1, avulsion fracture; A2, metaphyseal: A3, metaphyseal with comminution. Type B: Partial intra-articular fracture with or without column involvement: B1, lateral condylar: B2, medial condylar; B3, articular fracture without column. Type C: Entire articular fracture with both column disruption; C1, no significant articular or metaphyseal comminution; C2, no articular comminution but significant metaphyseal comminution; C3, both articular and metaphyseal comminution. Classification of capitulum fractures: Type I: Hahn-Steinthal: fracture in coronal plane Type II: Kocher-Lorenz: sleeve fracture of articular surface with little osseous bone. Type III: comminuted. Classification of olecranon fractures: common with varied mechanisms of injury and fracture patterns. Multiple classification patterns have been developed; no single system is accepted widely (Miller, 2000). The knowledge of these variations is important in orthopedics while operating on a fracture when they use different types of nails and screws for a compound fracture. Since there are ethnic variations in the size and shape of the upper and lower end of humerus, this study could be useful in manufacturing the instruments which will be suitable for different population groups. REFERENCES CITED Williams, P. L., L. H. Bannister, M. M. Berry, P. Collins, M. Dyson, J.E. Dussek, and M. W. J. Ferguson 1995. In: Gray’s Anatomy, 38th edition, p 623-625, Churchill Livingstone: London. Snell, R. S. 2000. In: Clinical Anatomy for Medical Students, pp. 499, 6th edition. Lippincott, Williams and Wilkins : Philadelphia. Miller, M. D. 2000. In: Review of Orthopedics, pp. 500-502. 3rd edition. W. B. Saunder’s Company: Philadelphia. Bergman, R. A., A. K. Afifi and R. Miyauchi 1954. In: Illustrated Encyclopedia of Human Anatomic Variation: opus V: Arm: humerus. skeletal systems: upper limb. Trotter, M. 1943. Septal apertures in the humerus of American Whites and Negroes. Am. J. Phys. Anthropol., 19: 213-227.