Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
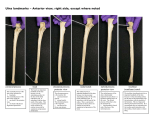
The Elbow Joint (ArticulatioCubiti) By Prof. Dr. Muhammad Imran Qureshi Type Of the Joint: Compound Synovial Humeroulnar articulation Humeroradial articulation Superior Radioulnar articulation Variety Of the Joint: Uniaxial of Hinge Variety (Ginglymus) The requisites of a hinge are that: The capsule must be loose in front and behind to permit flexion and extension, and Strong collateral ligaments must be present to prevent medial and lateral movements. Articular Surfaces: The articular surfaces are covered with Hyaline Cartilage. They are: At the lower end of the Humerus, there is a lateral “Capitulum” and medial “Trochlea”. The trochlea is not a simple pulley because its medial flange exceeds the lateral one, thus projecting at a lower level (0.6mm). This means that the plane of the joint is about 2cms distal to the inter epicondylar line and is tilted inferomedially. The Trochlea is also widest posteriorly, and here its lateral edge is sharp. The trochlea has an asymmetrical saller surface, largely concave transversely and convex anteroposteriorly. The medial surface of the trochlea is NOT covered with hyaline cartilage. On the Upper end of the Radius is its disc shaped “Head”, which is covered with hyaline cartilage that extends onto its circumference and thereby into the proximal radioulnar joint. The rim of the radial head, which is more prominent medially, fits the groove between the humeral capitulum and trochlea. The superior surface of the head is shallowly concave. 1 On the Upper end of the Ulna is its “Trochlear Notch” (Semilunar notch), which is formed by the Olecranon and coronoid processes of the ulna. These two processes of the ulnar notch are usually separated by a rough strip devoid of articular cartilage and covered by fibroadipose tissue and synovial membrane. On the lateral surface of the coronoid process of the ulna, there is a concave facet called Radial notch of the Ulna. It forms about one fifth of a circle. Fibrous Capsule: On The Humerus: The capsule is attached laterally to the articular margins of the capitulum. Anteriorly, it leaves the superior articular margin of the capitulum and passes on above the margins of the radial and coronoid fossae. From here, it passes on to the articular margins of the medial flange of the trochlea and with it passes posteriorly. Here, it leaves the superior articular margin of the posterior aspect of the trochlea and passes above the Olecranon fossa, from where it reaches the lateral flange of the trochlea and thence to the articular margin of the capitulum. On The Ulna: From the humerus, the fibres of the capsule pass to the ulna, where they are attached to the articular margins of the Trochlear notch of Ulna and the anterior and posterior margins of the radial notch of ulna. On The Radius: The capsule is NOT attached to the radius. It is attached to the Annular Ligament instead. The anterior part of the capsule is irregularly arranged, and some of the deeper fibres of Brachialis are inserted into it. The posterior part of the capsule is thin and may be deficient medially. It is protected by the Triceps. 2 Synovial Capsule / Membrane: On the Humerus, It is attached to the articular margins of the capitulum and the Trochlea and lines the two anterior and one posterior fossae. From here, it is reflected to line the inner aspect of the fibrous capsule. On the Ulna, it follows the articular margins of the Olecranon and Coronoid processes, and the anterior and posterior lips of the radial notch of the ulna. On the Radius, it is attached to the lower margin of its cylindrical articular surface of its head. From the articular margin of the head of radius, it hangs down between the annular ligament and the neck of the radius (which it encircles like a sleeve and thus preventing friction between the two). Ligaments of the joint: Only Extracapsular Ligaments are present in this joint. They are: Ulnar (Medial) Collateral Ligament: It is Triangular in shape and comprises of the following THREE bands: Anterior Band: It is the strongest of the three. On the Humerus, it is attached to the medial epicondyle and passes down to be attached to a tubercle on the medial border of coronoid process of the ulna. Posterior Band: It passes from the same tubercle on the medial border of the ulna to the medial border of the olecranon process. Middle Band: It spans (bridges the gap) between the anterior and posterior bands. (Forms carpet for the ulnar nerve on its way to the forearm) Radial (Lateral) Collateral Ligament: It is a flat triangular band, one end of which is attached to the lateral humeral epicondyle (below the common extensor origin), while the other end fans out and its fibres blend with the fibres of the annular ligament. (It is not attached to radius) 3 Annular Ligament: It is attached to the anterior and posterior lips of the radial notch of the ulna. Around the radial head, it is wide, while around its neck, it is narrow. Quadrate Ligament: Though NOT a part of the joint, it plays a vital role in preventing the herniation of the synovial membrane between the anterior and posterior edges of the annular ligament. It is attached to the neck of the radius proximal to its tuberosity to the upper part of the supinator fossa of the ulna just distal to the radial notch. It prevents herniation of the synovial membrane as it forms a sleeve around the radial neck. Blood Supply of the joint: Branches from the arteries which anastomose around it. Nerve Supply of the joint: It follows the Hilton’s Law. Musculocutaneous nerve. Median nerve. Ulnar nerve. Radial nerve. Movements of the joint: Flexion: It is produced by the Brachialis and the Biceps brachii, assisted by all the muscles that cross the joint whose line of pull passes in front of the axis of flexion and extension. Approximation of the ventral surfaces of the arm and forearm limit it. The range is about 140o. Extension: Triceps brachii is the prime mover, assisted by all the muscles that cross the joint whose line of pull passes behind the axis of flexion and extension. Stability Of the joint: It depends upon THREE factors: Bony Factors Ligamentous Factors, and Muscular Factors Bony Factors: The joint is quite secure when extended. In this position, the Olecranon process of the ulna fits into the Olecranon fossa of 4 the humerus….. The joint is said to be locked (Secure). Only fracture of the Olecranon process will make the joint unstable. However, when the joint is flexed, the Olecranon process is out of the Olecranon fossa of the humerus. So in this position, any force applied in the direction of Olecranon process may cause it to dislocate posteriorly with or without fracture of the Coronoid process of the ulna. Ligamentous Factors: The anterior and posterior parts of the capsule arelax and weak, making anterior or posterior dislocation possible (depending on the circumstances) The collateral Ligaments are very strong, securing the joint from both sides. Thus lateral dislocation is not possible. The Annular Ligament is cup shaped, being wider above and narrow below, so the head of the radius is also secure within this ligament. Since this ligament acquires the cup shape gradually during development, avulsion of the head of radius is a common phenomenon in young children. Muscular Factors: The Brachialis passes just in front of the capsule of the joint and is inserted just below the joint into the Ulnar tuberosity, so it gives anterior support. On the Lateral and medial sides, the tendons of origin of the common extensors and flexors reinforce the collateral ligaments. Posteriorly, since the Triceps tendon is inserted on the Olecranon process of the ulna, its support is negligible. 5