Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
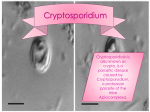
CRYPTOSPORIDIOSIS OPPORTUNISTIC INFECTION PREPARED BY Gerald Anthon Chuwa Head Parasitology section BMC. Introduction • Cryptosporidium infection (cryptosporidiosis) is a gastrointestinal disease whose primary symptom is diarrhea. • The illness begins when the tiny cryptosporidium parasites enter your body and travel to your small intestine. • Cryptosporidium then begins its life cycle inside your body — burrowing into the walls of your intestines and then later infective oocysts being shed in your feces. • In most healthy people, a cryptosporidium infection produces a bout of watery diarrhea and the infection usually goes away within a week or two. • In a patient with a compromised immune system, a cryptosporidium infection can become life-threatening without proper treatment. • You can help prevent cryptosporidium by practicing good hygiene and by avoiding drinking water that hasn't been boiled or filtered. MORPHOLOGY • Cryptosporidium species are able to infect and reproduce in the epithelial cell lining of the GI and respiratory tracts without causing cytopathic effects. HISTORY • This protozoan parasite was first described by Ernest Edward Tyzzer an American parasitologist in 1912. • Many outbreaks were associated with municipal water supplies and in swimming pools. • C hominis and C parvum cause most human infections. In immunocompeten t individuals, the organisms are primarily localized to the distal small intestines, whereas in immunocompromised hosts, the parasites have been identified throughout the gut, biliary tract, and respiratory tract. • Transmission • The disease is transmitted via the fecal-oral route from infected hosts. Most sporadic infections occur through person-to-person contact. • Nonetheless, transmission can also occur following animal contact, ingestion of water (mainly during swimming), or through food. Extensive waterborne outbreaks have resulted from contamination of municipal water and recreational waters (eg, swimming pools, ponds, lakes). • Cryptosporidium has emerged as the most frequently recognized cause of recreational water–associated outbreaks of gastroenteritis, particularly in treated (disinfected) venues. • This is because in the oocyst stage of its life cycle, Cryptosporidium can resist disinfection, including chlorination, and can survive for a prolonged period in the environment Cryptosporidium oocysts stained by modified Zn stain. Mature oocyst containing two sporocysts each with 4sporozoites LIFE CYCLE • Life cycle • Cryptosporidium does not multiply outside of the host. Cryptosporidium can complete its life cycle within a single host, including its asexual (merogony) and sexual (sporogony) reproductive cycles. • Infection is initiated by ingestion of oocysts, which are activated in the stomach and upper intestines to release 4 infective sporozoites (see the first image below). These motile sporozoites bind to the receptors on the surface of the intestinal epithelial cells and are ingested into a parasitophorous vacuole near the surface of the epithelial cell, separated from the cytoplasm by a dense layer. • Once inside the epithelial cell, the parasite goes through a series of sexual and asexual multiplication steps leading to the production of oocysts. Two morphologic forms of the oocysts have been described: • thin-walled oocysts (asexual stage) excyst within the same host (causing self-infection), whereas the thick-walled oocysts (sexual stage) are shed into the environment. Oocyst shedding can continue for weeks after a patient experiences clinical improvement. Diagrammatic representation of life cycle of cryptosporidium. Symptoms The first signs and symptoms usually appear two to seven days after infection with cryptosporidium and may include: Watery diarrhea Dehydration Weight loss Stomach cramps or pain Fever Nausea Vomiting • Symptoms may last for up to two weeks, though they may come and go sporadically for up to a month, even in people with healthy immune systems. Some people with cryptosporidium infection may have no symptoms Causes • Cryptosporidium infection begins when you ingest the cells of one of nearly a dozen species of the one-celled cryptosporidium parasite. The Cryptosporidium parvum (C. parvum) species is responsible for the majority of infections in humans. • These parasites then travel to your intestinal tract, where they settle into the walls of your intestines. Eventually, more cells are produced and shed in massive quantities into your feces, where they are highly contagious • You can become infected with cryptosporidium by touching anything that has come in contact with contaminated feces. Methods of infection include: • Swallowing or putting something contaminated with cryptosporidium into your mouth • Drinking water contaminated with cryptosporidium • Swimming in water contaminated with cryptosporidium and accidentally swallowing some of it Eating uncooked food contaminated with cryptosporidium Touching your hand to your mouth if your hand has been in contact with a contaminated surface or object Having close contact with other infected people or animals — especially their feces — which can allow the parasite to be transmitted from your hands to your mouth • If you have a compromised immune system from HIV/AIDS, you're more susceptible to illness from cryptosporidium than is a person with a healthy immune system. People with HIV/AIDS can develop severe symptoms and a chronic, persistent form of disease that may be difficult to treat • Cryptosporidium is one of the most common causes of diarrhea in humans. This parasite is difficult to eradicate because it's resistant to many chlorine-based disinfectants and can't be effectively removed by many filters. Cryptosporidium can also survive in the environment for many months at varying temperatures, though the parasite can be destroyed by freezing or boiling. Risk factors • People who are at increased risk of developing cryptosporidiosis include: • Those who are exposed to contaminated water • Children, particularly those wearing diapers, who attend child care centers • Parents of infected children • Child care workers Animal handlers Those who engage in oral-to-anal sexual activity International travelers, especially those traveling to developing countries Backpackers, hikers and campers who drink untreated, unfiltered wate • Swimmers who swallow water in pools, lakes and rivers People who drink water from shallow, unprotected wells Complications Complications of cryptosporidium infection include: • Malnutrition resulting from poor absorption of nutrients from your intestinal tract (malabsorption) • Severe dehydration • Significant weight loss (wasting) • Inflammation of a bile duct — the passage between your liver, gallbladder and small intestine • Inflammation of your gallbladder, liver or pancreas • Cryptosporidium infection itself isn't lifethreatening. However, if you've had a transplant or if you have a weakened immune system, developing complications can be dangerous. DIAGNOSIS • You may undergo the following tests to diagnose cryptosporidium infection: • Acid-staining test. The simplest way to diagnose cryptosporidium infection is a method called an acid-staining test, which identifies cryptosporidium under a microscope. To obtain cells for the analysis, your doctor might ask for a stool sample, or in more extreme cases, take a tissue sample (biopsy) from your intestine for the test Modified Ziehl Neelsen stain • Make a faecal smear from suspected material in normal saline. • Allow the smear to dry • Fix the smear in methyl alcohol for 15 minutes. • Stain the smear with carbol fuchsin for 15 minutes • Decolourise with 1% acid alcohol to remove excess stain. • Counterstain with methylene blue for 30 seconds • Dry the film and examine using the high power objective. • Other tests. Once it's clear that your infection is cryptosporidium, you may need further testing to check for development of serious complications. For example, checking liver and gallbladder function may determine whether the infection has spread. C. parvum - Cysts in stool Acid fast • If you have both AIDS and cryptosporidiosis, a T cell count — which measures the level of a certain white blood cell that's part of your immune system — can help predict the duration of the cryptosporidiosis. A high T cell count means you're more likely to recover quickly, while a low count means you may need to be monitored for further complications. Treatment • There's no commonly advised specific treatment for cryptosporidiosis, and recovery usually depends on the health of your immune system. Most healthy people recover within two weeks without medical attention. • If you have a compromised immune system, the illness can last and lead to significant malnutrition and wasting. The goal of treatment is to alleviate symptoms and improve your immune response. Cryptosporidium treatment options include • Anti-parasitic drugs. Medications such as nitazoxanide (Alinia) can help alleviate diarrhea by attacking the metabolic processes of the cryptosporidium organisms. Azithromycin (Zithromax) may be given along with one of these medications in people with compromised immune systems • Anti-motility agents. These medications slow down the movements of your intestines and increase fluid absorption to relieve diarrhea and restore normal stools. Anti-motility drugs include loperamide and its derivatives (Imodium A-D, others). Talk with your doctor before taking any of these medications. • Fluid replacement. You'll need oral or intravenous replacement of fluids and electrolytes — minerals such as sodium, potassium and calcium that maintain the balance of fluids in your body — lost to persistent diarrhea. These precautions will help keep your body hydrated and functioning properly. • Anti-retroviral therapies. If you have HIV/AIDS, highly active anti-retroviral therapy (HAART) can reduce the viral load in your body and boost your immune response. Restoring your immune system to a certain level may completely resolve symptoms of cryptosporidiosis. Prevention and control. • Cryptosporidium infection is contagious, so take precautions to avoid spreading the parasite to other people. • All preventive methods aim to reduce or prevent the transmission of the cryptosporidium germs that are shed in human and animal feces. Precautions are especially important for people with compromised immune systems. Follow these suggestions • Practice good hygiene. Wash your hands with soap and water after using the toilet, changing diapers, and before and after eating. Thoroughly wash all fruits and vegetables that you will eat raw, and avoid eating any food you suspect might be contaminated. • Purify drinking water if you have a weakened immune system or are traveling in an area with a high risk of infection. Methods include boiling — at least one minute at a rolling boil — or filtering, although filtering may not be as effective as • boiling. Limit swimming activities in lakes, streams and public swimming pools, especially if the water is likely to be contaminated or if you have a compromised immune system. Avoid fecal exposure during sexual activity • Avoid fecal exposure during sexual activity. • Handle newborn farm and domestic animals with care. Be sure to wash your hands after handling the animals. • Always refrain from swimming anytime you're experiencing diarrhea. If you know you've had a cryptosporidium infection, don't go swimming for at least two weeks after your symptoms subside because you may still be contagious Situation at BMC No scientific study has been conducted to understand the morbidity and mortality. Specimens from suspected cases are sent to laboratory for modified Zn stain to demonstrate the parasites. As from January to May 2014 the laboratory received 12 faecal specimens for modified Zn stain an average of 2 samples per month. • Out of 12 received samples 4 were positive and 8 were negative.