Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Urinary tract infection wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Antimicrobial surface wikipedia , lookup
Infection control wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Neonatal infection wikipedia , lookup
Triclocarban wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
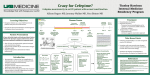
Cefepime for amp-C producing enterobacteriaceae Cefepime is a fourth generation cephalosporin with activity against a variety of gram positive and gram negative bacterial species, including methicillin sensitive staphylococcus aureus (MSSA) and Pseudomonas aeruginosa. It is FDA approved for use as monotherapy in febrile neutropenia, in combination with metronidazole for intra-abdominal infections, for pneumonia (including severe pneumonia with pathogens such as P. aeruginosa, Klebsiella pneumoniae, and Enterobacter spp.), and for complicated UTI, among other indications1. Unlike other cephalosporins, cefepime is a poor inducer of and relatively more stable to the AmpC β-lactamase produced by organisms such as Serratia spp, Providencia spp, Indole-positive Proteus (Morganella morganii), Citrobacter spp, and Enterobacter spp (SPICE). The AmpC β-lactamase confers resistance to penicillins and most β-lactamase inhibitor combinations, 1st – 3rd generation cephalosporins, ceftaroline, and aztreonam2. Resistance emerges as a result of de-repression of the AmpC β-lactamase gene in the presence of an inducing antibiotic, or via selection of stable de-repressed subpopulations on therapy. The most common inducing antibiotics are 3rd generation cephalosporins3. Carbapenems have been used to successfully treat a variety of infections with SPICE organisms, but these bacteria may also exhibit resistance to carbapenems. In the setting of increased incidence of carbapenem resistant enterobacteriaceae (CRE) associated with antimicrobial use in general and carbapenem use in particular4, research into the use of cefepime as a carbapenem-sparing agent for the treatment of infections with SPICE organisms has been recently published. Tamma and colleagues at the Johns Hopkins Institutions and the University of Maryland School of Medicine investigated patients admitted between 2/2010 and 1/2012 with culture confirmed bloodstream infections, pneumonia (using BAL cultures), or intra-abdominal (using intra-abdominal fluid cultures) infections with Enterobacter spp, Serratia marcescens, or Citrobacter spp. demonstrating production of AmpC β-lactamase by 2 separate lab tests. Patients who received either meropenem or cefepime empirically and as definitive therapy for at least 72 hours were included for analysis. Patients with 1 or more isolate testing negative for the production of AmpC β-lactamase by either lab method were excluded. Overall, 96% of confirmed AmpC β-lactamase producing organisms were susceptible to cefepime, and 97% to meropenem. Propensity score matching yielded 32 matched pairs for analysis. Clinical characteristics were similar in the propensity matched analysis, and no difference in mortality or hospital length of stay was observed. A majority of patients in both groups (93%) had adequate source control (removal of infected central lines or drainage of fluid collections). The authors concluded that cefepime may be a reasonable option for the treatment of invasive infections due to AmpC βlactamase–producing organisms, particularly when adequate source control is achieved5. Siedner and colleagues at Brigham and Women’s Hospital and Massachusetts General Hospital investigated all cases of Enterobacter spp. bacteremia admitted between 2005 and 2011, comparing inhospital mortality and persistent bacteremia (≥1 day after antibacterial initiation) between patients who received therapy with any antimicrobial. Of 368 patients who received antimicrobial therapy for Enterobacter spp. bacteremia, 16 received monotherapy with a carbapenem (imipenem or meropenem) 36 received monotherapy with cefepime; 136 received any treatment with cefepime and 74 received any treatment with a carbapenem. No significant difference in persistent bacteremia or in-hospital mortality was observed. The authors concluded that cefepime has a similar efficacy as carbapenems for the treatment of Enterobacter spp. bacteremia6. Based on these data, cefepime is a reliable treatment option for invasive infections with AmpC β-lactamase producing pathogens, and is preferable for use in order to reduce selection pressure on carbapenems and preserve their activity in the setting of increasing bacterial resistance. SMC 10/2014 Resources: 1. Maxipime I.V. [package insert]. Lake Forest, IL: Hospira Inc; February 2014. 2. Jacoby GA et al. Amp-C beta-lactamases. Clin Microbiol Rev 2009;(22):161-182. 3. Blanchette LM et al. Clinical comparison of ertapenem and cefepime for treatment of infections caused by AmpC beta-lactamase-producing Enterobacteriaceae. Scandinavian Journal of Infectious Diseases. 2014; Early Online: 1-6. 4. Patel et al. Clinical epidemiology of carbapenem-intermediate or –resistant Enterobacteriaceae. Journal of Antimicrobial Chemotherapy 2011;(66):1600–1608 5. Tamma PD et al. The Use of Cefepime for Treating AmpC β-Lactamase–Producing Enterobacteriaceae. Clinical Infectious Diseases 2013;57(6):781–8. 6. Siedner MJ et al. Cefepime vs Other Antibacterial Agents for the Treatment of Enterobacter Species Bacteremia. 2014;58(11):1554–63. SMC 10/2014