Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
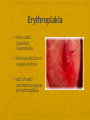
Dental Health & Prevention Teach children to brush early Take children to the dentist by 1 years old Consider Fluoride Varnish when teeth first appear Fluoride Varnish All solutions Fluoride Varnish Cavity Shield Varnish Duraflor Enamel Pro Barnish Lor-Opal Varnish Vanish Dental Health & Prevention Fluoride Varnish Inform any discoloration will be gone in 8 hours Apply varnish 2 – 4 times a year No food or drink 60 minutes after application No brushing for 12 hours after application Remove plaque and debris from teeth with gauze But don’t dry , salvia needed set properly Pain on the varnish on all sides of the teeth Fine thin film Billable 99211 Oral Health Taking an oral history Who is your dentist? When was your last visit? What did the dentist do for you? How often do you brush/floss? Are you having any problems with your teeth, chewing, tasting, swallowing Oral Health Taking an oral history Do your gums bleed when you brush? Do you find blood on the pillow case? Do you smoke, or chew tobacco? So you use sun screen on your lips? Do you have any sores/lumps in your mouth? Oral Health Taking an oral history Do you engage in contact sports? Do you (children) use fluoride? Does your mouth hurt? Do you have any questions about your oral health? Oral Health A complete oral exam is recommended Prompt referral Bleeding gums white spots lesions along the gum line Decayed or loose teeth Ulcerations Leukoplakia or Erythroplakia Lumps or Swelling Hairy Leukoplakia Oral hairy leukoplakia may look like oral candidiasis (thrush). Thrush can be scraped off. The white ridges of oral hairy leukoplakia do not scrape off. Occurs in people who have HIV and who have moderate to severe immune system damage. Erythroplakia Also called Speckled Leukoplakia More predictive of neoplasm than Leukoplakia 90% of early carcinomas appear as erythroplakia What about Fluoride? Dental fluorosis is an irreversible condition caused by excessive ingestion of fluoride during the tooth forming years. Mild Fluorosis The white opaque areas in the enamel of the teeth are more extensive but do not involve as much as 50 percent of the tooth." Severe Fluorosis All enamel surfaces are affected and hypoplasia is so marked that the general form of the tooth may be affected. The major diagnostic sign of this classification is discrete or confluent pitting. Brown stains are widespread and teeth often present a corrodedlike appearance. Oral Health Dietary fluoride: Liquid form with and without vitamins and in chewable tablets, dosed by age range. Additional topical fluoride in toothpaste: age 2 –3 yrs (a pea size amount) until age 6 Parents should assume primary responsibility for brushing until child has enough dexterity to do it on their own Age 7 begin dental flossing under supervision Oral Major risk factors Use of tobacco (increases risk 6-28 times) Tobacco and alcohol account for 90% of cases Age Screening for oral cancer Lip, tongue, pharynx, oral cavity 30,000 cases per year 5 year survival 52% Oral Cancer Oral leukoplakia Needs biopsy Recommendations Early detection has better prognosis ? No proof better outcomes Oral leukoplakia: form of premalignancy ACS:oral exam every 3 years after age 40 Canadian task force: annual exam by provider or DDS over age 60 with risks Counsel regarding risks of tobacco and alcohol Patients undergoing cancer tx can benefit by seeing a dentist before tx begins. Dental Prevention Visit a dental care provider regularly, floss & brush daily, brush with a fluoride toothpaste Use mouth rinses for plaque prevention Don’t put infants to bed with a bottle Fluoride supplements for children in communities without adequate fluoridation Older Adults – Oral Care Risks: Poor oral hygiene Decreased salivary flow Lack of professional care Dentures Older Adults – Oral Care Brush and floss See the dentist (cost, transportation) Use soft toothbrush with light pressure Implanted joints, valves, some murmurs antibiotic Rx for dental repair Diabetes need special care Dentures are not to be worn continuously It is better if they fit Vision Screening Visual Impairment Undetected visual problems Common in preschool children Estimated prevalence of 5-10% Risk Factors Risk factors in newborns Family History of ocular malformations Congenital cataracts Ocular tumors Premature birth Birth to mother who suffer from rubella herpes or toxoplasmosis Amblyopia Amblyopia reduced vision in an eye that has not received adequate use Strabismus Strabismus crossed-eyes, is a vision condition in which a person can not align both eyes simultaneously under normal conditions Screening Stereoacuity testing more effective than visual acuity for these conditions (random dot sensitivity 54-64%, specificity of 87-90% PPV 57%, NPV 93%) Snellen, Landolt C, tumbling E, Allen picture cards, grating cards Snellen letters sensitivity of 25-37% Early detection and treatment improves prognosis for normal eye development Visual Impairment Elderly Snellen visual acuity Causes: presbyopia, cataract, age-related macular degeneration, glaucoma >75 yo have 5% MD & 5% glaucoma, 40% cataract Routine screening for acuity is recommended Frequency left to clinical discretion No routine rx for ophthalmoscopy if symptomatic Cataracts Prevention Sun Glasses Risk Genetic Blue Eyes Corticosteroids Vision through a Cataract Recommendations for Adults There is no data to determine the incremental benefit of routine screening of asymptomatic adults to detect early refractory errors compared to waiting for patients to present with complaints of visual problems Glaucoma Slowly progressive loss of vision associated with damage to the optic nerve Inc IOP common, but not diagnostic criterion Visual fields and fundoscopic/slit lamp examination 2nd leading cause of irreversible blindness in the US Congenital; Open-angle: most common; Closed –angle; Secondary Screening Tonometry Schiotz, applanation, air puff devices Measures IOP Accuracy and reliability varies by device Experience of examiner Physiologic variations in the patient Tonometry Slit Lamp Exam Ophthalmoscope Detects changes in the optic nerve head that often precede visual deficits pallor, cupping, hemorrhage Interobserver variation Slit Lamp Exam Screening Perimetry: gold standard Visual stimuli varying brightness throughout visual field Takes 45 min, not feasible for screening Sensitivity in excess of 90% with specificity of 70-88% Perimetry Early Detection Visual deficits from glaucoma generally not reversible Early treatment can prevent or delay progression Controversial role of increased IOP High risk patients: blacks over 40yo, whites over 65yo; Diabetics; Severe myopia Recommendations American academy of Ophth Comprehensive eye exam by ophth all adults 40yo; Younger for blacks Canadian task force Insufficient evidence to recommend for against screening Guide to Clinical Preventive Services: insufficient evidence for or against routine screening by primary care clinicians: effective screening best done by specialists with specialized equipment to measure visual fields and evaluate the optic disc Hearing Hearing School aged children and adults Pure-tone audiometry Problems Improper technique Background noise Unintentional or intentional misreporting by subject Hearing Older adults Questioning them about their hearing, counseling about the availability of hearing aid devices, and making referrals. Pt inquiry or evidence of impairment: audiometric testing and otoscopic examination. Hearing Screen high risk infants evoked oto-acoustic emission auditory brainstem response High risk: Risk for congenital or parentally acquired hearing loss: herpes, syphilis, rubella, CMV, toxo, low birth weight, meningitis,….). Evoked Otoacoustic Emission Test Measures an acoustic response produced in inner ear – bounces back out of ear in response to sound stimuli Place small probe with microphone and speaker in infant’s ear With infant resting quietly, sounds are generated and responses that come back from cochlea are recorded. Cochlea processes sound – electrical stimuli sent to brainstem Second separate sound comes back out into canal – otoacoustic emission If there are emissions for those sounds critical to speech comprehension, then infant has “passed” hearing screen. Auditory Brainstem Response ABR test is reliable, objective, noninvasive and painless. Brain wave activity in the auditory centers of the brain is recorded in response to a series of clicks presented to each ear Measures readiness for language development. Auditory Brainstem Response Testing