Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DR. AJIN JAYAN THOMAS,
Department of Physiotherapy,
Dr. D. Y. Patil University,
Nerul, Navi Mumbai.
“Metabolic
syndrome is a cluster of the
most dangerous cardiovascular risk factors
namely diabetes, abdominal obesity, high
cholesterol and elevated blood pressure”.
1923, Kylin described the clustering of hyperglycemia,
hyperurecemia and hypertension.
1988, Reaven- “Syndrome X” referred to a group of
connected disorders characterized by impaired
glucose tolerance, dyslipidemia, hypertension,
associated with increased risk of type 2 diabetes and
cardiovascular disease.
Syndrome X
Insulin resistance syndrome
Metabolic syndrome X
Cardiometabolic syndrome
Dysmetabolic syndrome
Deadly quartet
Multiple metabolic syndrome
World Health Organization (WHO) 1998
Adult Treatment Panel III, 2003
International Diabetes Foundation (IDF), 2005
American Association of Clinical Endocrinologists
(2003)
European Group for the Study of Insulin Resistance,
EGIR
American Heart Association (AHA) and National
Heart, Lung and Blood Institute (NHLBI), 2005
ANY 3 OF 5 CONSTITUTE DIAGNOSIS OF METABOLIC
SYNDROME
Elevated Waist Circumference (cutoff for Asian Population)
90 cm (35 inches) in Men 80 cm (31 inches) in Women
Elevated Triglycerides
150 mg/dL(1.7 mmol/L) Or On drug treatment for elevated TG
Reduced HDL-C
<40 mg/dL in men /<50 mg/dL in women Or On drug treatment for
reduced HDL-C
Elevated Blood Pressure
130 mm Hg systolic blood pressure Or 85 mm Hg diastolic blood
pressure Or On antihypertensive drug treatment
Elevated Fasting Glucose
100 mg/dL Or On drug treatment for elevated glucose
Viswanathan Mohan and Mohan Deepa, (2006) The
prevalence rates were 25.8% in India, 13% in China, 30%
in Iran, 28% in Korea,, 22% in Hong Kong, 18.5% in
Vietnam, 17% in Oman and 15.2 % in Taiwan.
Rajeev Gupta et al., (2004) studied 1800 Indians. MetS
was present in 31.6% subjects; prevalence was 22.9% in
men and 39.9% in women.
Ford Earl S. et al., (2002) studied the prevalence rates
among American adults and found that the prevalence of
MetS was 23.7% . Thus they concluded that 47 million
adults in the United States had metabolic syndrome.
Causes 2-3 fold increase in cardiovascular risk of
mortality.
Considered as a risk factor for CHD and precursor of
Diabetes mellitus (up to 5% fold increase in risk).
Even with 2 to 3 components- increased mortality
from CVD and CHD.
Risk of stroke increases 3 fold.
Reduced cardiorespiratory fitness.
Associated with: Essential hypertension, Polycystic
ovarian syndrome, Nonalcoholic fatty liver disease
Gallstone disease, Cancer (i.e., breast cancer), Sleep
apnea
Review
medical history and co-morbiditieshyperlipidemia with coronary heart disease (CHD),
cardiovascular disease, cerebrovascular disease,
peripheral vascular disease, diabetes, hypertension,
renal disease, thyroid disease, surgical history, and
obesity.
Vital signs and physical data (blood pressure, heart
rate, waist circumference, weight, height, BMI, body
fat).
Review relevant tests, lab values FBS, Hgb A1C, fasting
lipid profile.
Obtain comprehensive diet history including dietary
intake data.
Assess physical activity pattern: type of physical
activity, frequency, duration, tolerance, and
motivation
Identify the risk category by using the Framingham
Point Scores and PROCAM risk score.
Cardiorespiratory Fitness: Six Minute Walk Test /
Exercise Tolerance Test.
FIRST LINE THERAPY……LIFESTYLE MODIFICATION
WEIGHT REDUCTION
DIETERY MODIFICATIONS
PHYSICAL ACTIVITY
WEIGHT REDUCTION :
Reduce calorie intake and Exercise
Reduction in 1 kg of body weight causes 2-5%
reduction in visceral fat.
Realistic Goal………. 7-10% reduction of body weight
in 6-12 months.
DIETARY MODIFICATIONS
Adequate fluid consumption- 1.5 liters / day
Limit salt intake up to 6 g/day
Calories based on individual needs, initiate plan to
achieve reasonable weight (BMI between 18 and 24
kg/m2)
Select 5 to 6 servings/day of fruits and vegetables and
6 servings/day of whole-grain products.
Choose foods with lower glycemic index.
Use olive oil instead of sunflower oil/coconut oil/palm
oil in preparation of food.
Low fat diary products- yogurt & cheese everyday,
reduce butter and cream.
Vegetables and fruits everyday.
A FEW TIMES A WEEK……..
Fish: Herring, Mackerel, Salmon, Sardine and Tuna- A
high intake of omega-3 fatty acids is associated with a
lower risk of coronary heart disease.
Meat: Poultry recommended over beef, pork and lamb
due to lower content of fat and saturated fatty acids.
Red meat only 2-3 times a month.
Eggs : 2-3 eggs a week ("hidden" eggs in baked or
cooked food (e.g. cake, biscuits).
Alcohol:
May be good for you…….. Don’t start for health
reasons…..but reduce amount to 1-2 glasses of wine.
PHYSICAL ACTIVITY
Moderate intensity, continuous or intermittent,
more than 30 minutes, 5 days a week, resistance
training for 2 days a week.
Reduces blood glucose, SBP/DBP, LDL TG, visceral
body fat,
Increase in HDL, improves cardio-vascular risk
factors,
Improves functional capacity.
Sean Carroll and Mike Dudfield, Insulin sensitivity improves by 60%
(2004)
Reduction in body weight 8% (without
systematic review
calorie restriction)
25 RCT’s Reviewed
Reduction in incidence of DM by 41-58%
Reduction in 3mmHg of SBP/DBP by 3-9%
weight loss
Recommendation:
CLINICAL
TRIALS
NEEDED
IN
ETHINIC
MINORITY
POPULATIONS SUCH AS INDIANS
Katzmarzyk P. T et al.,
(2003).
HERITAGE Family Study
20 wk of aerobic exercise training
Overall reduction in prevalence of MetS
reduced from 16.9 to 11.8 %
Rennie K. L et al., (2003)
Reduced BMI and increased cardiovascular
5153 white European participants
fitness.
moderate and vigorous physical Reduction in cluster of risk factors.
leisure-time activities
Kerry J. Stewart et al., (2005)
51 men and 53 women with MetS.
6 months exercise
Increased aerobic and muscle fitness, lean
mass, and HDL and reduced total and
abdominal fat. Diastolic BP was reduced .
Orchard TJ, Temprosa M,
Goldberg R, et al
(2005)
3234 participants
150 minutes of exercise per week
3 year follow up.
Incidence of the metabolic syndrome was reduced
by 41% in the lifestyle intervention group and by
17% in the metformin group
Christos Pistavos et al.,
(2006)
Systematic review of 13 studies on
effect of exercise on MetS
Decreased risk of CHD mortality
Reduced risk of developing DM
Ex shown to modify blood lipid profiles
Improvements difficult to maintain
Tjonnas AE, Lee SJ, Rogonmo
O, et al
(2008)
Aerobic interval training vs.
continuous moderate exercise
32 patients
Increase of 25% in HDL levels, improvement in
insulin sensitivity, aerobic capacity in interval
training group.
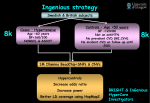
28 male patients between the ages of 40-55 years
Total exercise time for both groups was 45 minutes, 5
days a week for two weeks.
The interval training group during their 25 minutes of
resistance exercise alternated between 30% of baseline
peak work rate for 2 minutes and then 70% of baseline
peak work rate for 3 minutes on the cycle ergometer.
The conventional group (Group B) during the 25
minutes of resistance exercise performed cycling at
50% of the baseline peak work rate
Out come: Six Minute Walk Distance
RESULTS
All participants showed significant improvement in
the six minute walk distances.
Statistically significant difference between the post
test six minute walk distances of the two groups.
Interval training group showed more improvement in
their six minute walk distances.
Negative correlation of age with 6MWD
Postive correlation of height with 6MWD
Weight had no correlation with 6MWD
PREVENTION
Public Education about Metabolic syndrome
Screening for at risk individuals:
Family history
Blood Sugar / Hgb A1C, Lipids, Blood pressure
Smoking/Tobacco use
Activity Level / Dietary habits
Exercise prescription
Dietary advice
HELP PREVENT INDIA FROM BECOMING
CARDIOVASCULAR DISEASE CAPITAL OF THE
WORLD
THANK YOU
09769441388
[email protected]