Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
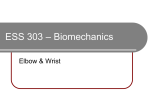
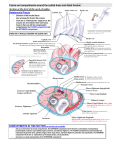
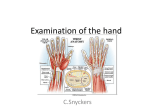
TSM77: ANATOMY OF THE WRIST 14/11/08 LEARNING OUTCOMES Describe the structure of the wrist joint and the normal range of movement ANATOMY OF THE WRIST JOINT The wrist joint (or carpus) is the point of articulation between the distal radius and carpal bones o The ulna does not articulate directly with any of the carpal bones o The carpal bones articulate distally with the five metacarpal bones at the base of the digits o The phalanges are the bones of the digits themselves – three in each finger, two in the thumb The ulnar and radial arteries both pass superficially into the wrist to supply structures of the hand o The ulnar artery passes medially from the flexor compartment just lateral to the ulnar nerve o The radial artery passes laterally from the extensor compartment There are eight carpal bones arranged roughly in two rows: o Proximal row (lateral to medial) Scaphoid – articulates with distal radius Lunate – articulates with distal radius Triquetrum – slightly anterior displacement in relation to the above Pisiform – point of insertion flexor carpi ulnaris (see below) o Distal row (lateral to medial) Trapezium – articulates with the first metacarpal Trapezoid – articulates with the second metacarpal Capitate – articulates with the third metacarpal Hamate – articulates with the fourth and fifth metacarpals o Can be remembered with the mnemonic some lovers try positions that they cannot handle MUSCLES ACTING AT THE WRIST Muscles acting on the wrist itself are contained in the two compartments of the forearm o Tendons entering the hand are covered by the two retinacula – strong fibrous bands o The flexor retinaculum forms the roof of the carpal tunnel (see below) The flexor compartment muscles all have common flexor origin – medial epicondyle of humerus o Superficial layer – all wrist flexors Flexor carpi radialis – inserts onto 2nd metacarpal – also radial abductor Palmaris longus – inserts onto flexor retinaculum Flexor carpi ulnaris – inserts onto pisiform – also ulnar abductor o The median nerve supplies the former two whilst the ulnar nerve supplies the latter The extensor compartment muscles all have common extensor origin – lateral epicondyle of humerus o Superficial layer – both wrist extensors Extensor carpi radialis – inserts onto 2nd/3rd metacarpals – also radial abductor Extensor carpi ulnaris – inserts onto 5th metacarpal – also ulnar abductor o Both of the above are supplied by the radial nerve Explain the causes and consequences of nerve compression syndromes Nerve compression distorts the structural elements of the nerve (fascicles) and impedes blood supply o This is most likely to occur at joints or where nerves pass through narrow tunnels o Ulnar nerve – second most common; often at the elbow (see case 32) o Radial nerve – at the elbow; generalised extensor paralysis of hand / wrist o Median nerve – most common; often at the carpal tunnel The carpal tunnel is formed by the carpals inferiorly and laterally and the flexor retinaculum superiorly o The median nerve passes laterally just deep to the flexor retinaculum o The tendon of flexor pollicis longus passes lateral to the median nerve o All eight tendons of flexor digitorum superficialis and profundus pass centrally o No blood vessels pass through the carpal tunnel Carpal tunnel syndrome involves elevated pressure in the tunnel – up to 15-fold o Often uncertain aetiology – affects females more than males (3:1) o May be associated with repetitive tasks over a long period of time o Can result from rheumatoid arthritis (swelling of synovial sheathes) or oedema o Symptoms arise due to compression of the median nerve: Pain and paraesthesia over its sensory distribution (lateral palm etc.) Weakness of thenar muscles – impaired thumb opposition o Percussion of the nerve at the wrist exacerbates symptoms – Tinel’s sign o Treatment involves anti-inflammatories and surgery in severe cases