Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
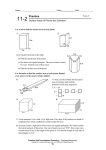
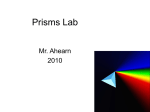
American Academy of Optometry: Case Report Rehabilitation of hemianopsia using expansion prism therapy combined with scanning training Kasey Suckow, O.D. Resident: Ocular Disease / Low Vision Rehab Hines & Jesse Brown VA Chicago 1157 W Diversey Pkwy Apt 408 Chicago, IL 60614 [email protected] Abstract Scanning training to make the patient more aware of environmental conditions / hazards is often used in conjunction with expansion prism therapy to rehabilitate patients with hemianopsia . A scanning training video and two cases are presented. Case Report Case History #1: Patient #1, a 67WM reported to clinic initially with a left homonymous hemianopia secondary to a recent stroke. He had several functional complaints caused by field loss such as bumping into people on the left, problems walking and avoiding object on the left, difficulty in the kitchen, and problems shaving the left side of his face. He had no head tilt noted on initial presentation. His medical history was significant for hypertension, stroke, high cholesterol, renal failure and acid reflux. Pertinent findings #1: His corrected visual acuity was 20/25 OD and 20/20 OS. Humphery visual field testing confirmed the left homonymous hemianopia previously. All other findings were within normal limits. Case History #2: Patient #2, a 74WM reported to with longstanding left homonymous hemianopia secondary to a gunshot wound occurring in 1954. His only previous vision training included a recommendation that he turn his head to the left to view. He had been referred from his primary eye care doctor for visual training. His medical history was significant for HTN, traumatic brain injury secondary to gunshot wound, and a significant fall causing cerebral hemorrhage and subsequent hospitalization for the past 18 months. Pertinent findings #2: His best corrected visual acuity was 20/40 OD and 20/32 OS. His visual field loss had been confirmed previously by HVF testing. He also displayed a left head tilt with normal posture, and was aware of his missing field. All other findings were within normal limits. He did not state any visual goals or problems with mobility at this time, but was interested in trying expansion prism therapy to improve his overall function. Differential diagnosis: Although visual field loss is relatively straightforward to diagnose with visual field testing, it is also important to distinguish field loss from visual neglect, or spatial inattention. A very deep case of neglect can present very similarly to a hemianopia. This is a very important distinction because patients with neglect will require longer rehabilitation programs secondary to greater functional disabilities6. One of the differences between a true hemianopia and neglect lies within the patient’s perception. A patient with only field loss will be aware of their lost field and will have functional complaints. A patient with field loss and/or neglect will not attend to and may not even notice the missing field. In both of the two cases mentioned above the patients were aware of their missing field and had corresponding complaints in terms of orientation and mobility. Neglect typically occurs on the left field secondary to organization of neural processing. Research into this area indicates that the left hemisphere of the brain attends only the right visual field, whereas the right brain hemisphere attends to both sides of the visual fields7. Therefore when the right hemisphere is damaged there is no cortical substrate attending to the left visual field. Neglect can be diagnosed with a number of different tests. Line bisection is a quick test that differentiates between field loss and neglect8-9. A patient with left neglect will bisect a line towards the right, whereas a patient who is aware of the loss will compensate and bisect the line closer to the middle, if not slightly skewed towards the left10. Other test strategies include simultaneous presentation on confrontation fields, drawing, copying, and cross-out tasks8-10. If the etiology of field loss is unclear a MRI should be performed to locate the lesion, injury, or stroke. Diagnosis: In both cases mentioned above field defects were confirmed with Humphrey visual field testing. Diagnosis is typically made with Goldmann visual field testing, or Humphrey automated testing. Due to the nature of strokes and traumatic brain injury these tests can be difficult and fatiguing for these patients alternative simplified testing can be implemented11. Another test that can be useful to determine prognosis for visual therapy is Amsler grid testing. This is useful for determining the degree of macular sparing11. This is especially pertinent for when initiating reading therapy. Treatment and Management: Treatment of these disorders is aimed at increasing awareness through prism or scanning therapy. Scanning therapy uses trained, intentional head and eye movements for spotting objects in the area of lost field. While this therapy proves beneficial to patients, it does not increase the field of view and requires quite a bit of effort and training to become natural. To increase the rate of success in the two cases presented, scanning therapy was incorporated along with the prism therapy. Scanning training is aimed at teaching the patient to never go where their vision has not gone. This means training in eye positioning, head positioning, and the use of quick, accurate eye movements to scan into the non-seeing field. The first step is to teach the patient to walk with his or her eyes turned towards the scotoma, thus pushing it out of the way. The next step is to work with turns. Bumping into objects after making a sudden turn into the scotoma is common, so patients are trained to stop prior to making a turn and quickly scan the area before proceeding. Eye movements for quick scanning are also taught, as the patient has to constantly be scanning between the seeing and non-seeing field. When large angle scans are needed, such as when crossing streets, a head turn can be added in to gain more range. Some studies have theorized that scanning therapy may reconstitute some of the visual field, by stimulating the zone between the damaged and intact fields. These findings have been inconsistent and no definite conclusions can be drawn as to whether the field is enlarged, or the patient has developed better visual searching skills12. In fact, field testing with scanning laser ophthalmoscope (SLO) where fixation is monitored within one degree, disputes the reconstitution theory13. Yoked prisms are another option for shifting the field of view. This can be particularly useful within the central 20 degrees of field. Prism adaptation to yoked prism has been proposed as a mechanism to help with patients exhibiting visual neglect, but there have not been any conclusive studies performed14. Expansion prism therapy actually increases the patient’s field of view4. It does so by creating peripheral diplopia, or confusion from the overlap of normal field and prismatically shifted field. Monocular inferior and superiorly placed prisms (40 diopters) shift the images from non-seeing to seeing field, allowing the patient to spot images in the periphery. Once the images are spotted in the periphery they can be attended without diplopia through the central portion of the lens. Perimetric visual field testing indicates that expansion prism therapy increases the superior and inferior field of view by around 20 degrees4. Field expansion and Visual Field Testing with Left Homonymous Hemianopia4. Fitting protocol4 with scanning training video: Both patients were fit using the Eli Peli Protocol for Prism Expansion Therapy4. Forty diopter Fresnel prisms were fit monocularly in the superior and inferior portion of lens on the side of the defect. Prisms used are 8 x 22mm segments, which can be cut in office, or ordered precut. The upper prism was fit first with the inferior portion of the prism placed at 6mm above the center of the pupil. The superior field generally contains fewer obstacles and thus less important to orientation and mobility. This makes the superior prisms easier to adapt to4. The diplopia was demonstrated to patients by presenting targets within and outside of normal field. Patients were instructed to fixate through the central portion of the lens. If an object was spotted in the periphery through the prism the patient was too move their head up to attend the object through the central portion of the lens, thus avoiding diplopia. Patients were also instructed on walking, spotting, central viewing, and on general cleaning and care of prisms. Prism Expansion Therapy with Left Homonymous Hemianopia4. After the initial fit and instruction the patients were sent home for a 2-3 week trial period. If the patient noted improvement and was able to adapt, prism was fit into the lower portion of the lens at 6mm below the center of the pupil. Again the patient is sent home for a 2-3 week trial period. Upon returning, if the experience was positive the patient was fit with permanent prisms. Response to treatment: Follow Up Pt #1: At the first follow-up with superior prism fitting, the patient noted improvement. The fitting protocol was continued with the lower prism segment. At this point the patient was lost to follow-up secondary to health problems with his kidneys. He set up appointments within low vision clinic and with low vision therapy, but was unable to make them. He did not present to clinic again until several months later now seeking to reinitiate prism therapy. He had lost the fresnel prisms around one month after initial fit, but he did notice a vast improvement in his functioning and avoidance of objects on left side. He noted his experience was extremely positive and was looking forward to getting permanent prism in his spectacle prescription. The fitting protocol was started again and patient is currently undergoing adaptation of prism with positive subjective results. Response to treatment: Follow Up Pt #2: Upon returning to clinic after initial fit with superior prism, the patient did not notice a significant improvement in his visual performance and wished to discontinue the fitting. The patient was proficient with scanning techniques and required no additional training at that time. He returned to clinic with trouble reading in dim lighting and seeing the projected hymns at church. He did not wish to initiate prism therapy again, as he did not see any improvement. His needs were addressed with devices and lighting. Fitting him with permanent prisms would have been inappropriate because of poor adaptation, and more importantly, he also had history of diminished balance and falls. An inferiorly shifted field secondary to prism may disorient a patient, and may be a potential risk factor for falls. It has been shown that the reduced depth perception occurring inferiorly with bifocals is a risk factor for falls14. It is possible that prisms may also be a risk factor and further studies should be performed to ascertain the relationship. Conclusion: Although many patients with hemanopic field loss have very good acuity, it is important to address the functional loss and subsequent effects on orientation and mobility. Even a small increase in an individual’s ability to function can have a significant impact in their daily lives. Many of these effects can be achieved with scanning and expansion prism therapy. Patient #1 had a very positive response both types of therapy. Although he noted disturbance with diplopia he was extremely motivated and appreciated the increased field. In general he had not adapted to his field loss as well as the second patient, and had several functional complaints concerning activities of daily living. Also, he had not developed a compensating head tilt or posture and was having significant problems scanning into his non-seeing field. Patient #2 had a very different response to the prism and scanning therapy. He noted disturbance with peripheral confusion. Further complicating the success rate is how proficient he had become over the past 53 years with development of his own scanning techniques and head posture. He noticed a difference with the prism, but preferred to use his own scanning strategies. The main differences between these two case presentations was length of field loss, level of functional compensation, etiology of field loss, and age at time of field loss. All of these factors may contribute to prognosis with prism therapy, but the level of previous functional compensation appears to play a key role. The different responses to prism in the two cases above illustrate how important scanning therapy is in addition to field expansion. In his initial study, Dr. Peli also noted a similar outcome with a patient who had developed good scanning and compensation strategies prior to prism therapy4. Because case presentation and cognitive functioning varies so much between these patients it is difficult to predict who will be successful. Although the two patients described above had essentially the same amount of field loss, they had entirely different responses to expansion prism therapy. Although there is little data analyzing the factors contributing to success with therapy, some studies indicate age16 and binocular vision disorders4 may play a role in determining outcome. Until these factors have been studied more thoroughly it is important to look at the patient’s overall needs, motivation, goals, as well as risk factors for falls when considering initiating therapy. Visual field loss is a prevalent condition in the clinical population. It affects not only the success rate of rehabilitation, but an individual’s quality of life. Therapy options should be discussed and offered to any patient presenting with hemianopia. Bibliography 1. Zhang, Xiaojun MD, et al. Homonymous Hemianopia in Stroke. Journal of Neuro-Ophthalmology. Volume 26 (3), September 2006, pp180-183. 2. Neyer, et al. Prevalence of Stroke—United States, 2005. Journal of the American Medical Association. Volume 298(3), 18 July 2007, p 279–281. 3. Kerkhoff G, Munssinger U, Meier K. Neurovisual rehabilitation in cerebral blindness. Arch Neurol 1994;51:474–81. 4. Peli, Eli MSc, OD, FAAO. Field Expansion for Homonymous Hemianopia by Optically Induced Peripheral Exotropia. Optometry and Vision Science. Volume 77 (9), Sept 2000. pp 453-464. 5. A.R. Bowers, K. Keeney, D. Apfelbaum and E. Peli. Multi-Site Extended Wear Trial of Peripheral Prisms Visual Field Expansion Device for Patients with Hemianopia. Invest Ophthalmol Vis Sci 2006;47: E-Abstract 3489 6. Kaira, L. PhD, FRCP; et al. The Influence of Visual Neglect on Stroke Rehabilitation. Stroke. Volume 28(7), July 1997:1386-1391. 7. Mangun GR, Hillyard SA, Luck SJ, Handy T, Plager R, eg al. Monitoring the visual workd: hemispheric asymmetries and subcortical processes in attention. Journal of Cognitive Neuroscience. 1994;6:267-75. 8. Azouvi P, Bartolomeo P, Beis J-M, et al. A battery of tests for the quantitative assessment of unilateral neglect. Restor Neurol Neurosci 2006; 24:273–285.. 9. Bartolomeo, Paolo. Visual Neglect. Current Opinion in Neurology. Volume 20(4), August 2007. p 381-386. 10. Barton JJ, Black, SE. Line Bisection in Hemianopia. Journal of Neurosurg Psychiatry. 1998; 64:660-662. 11. Suter, P OD. Peripheral Visual Field Loss & Visual Neglect Diagnosis and Treatment. Journal of Behavioral Optometry. Volume 18 2007.(3) pp78-83. 12. Bouwmeester, Lies; Heutink, Joost; Lucas, Cees. The Effect of Visual Training for Patients withVisual Field Defects Due to Brain Damage: a Systematic Review. Journal of Neurology, Neuropsychiatry, & Psychiatry. Volume 78(6), June 2007. pp555-564. 13. Jamara, Richard J OD FAAO; VanDeVelde, Frans MD; Peli, Eli MSc, OD, FAAO. Scanning Eye Movements in Homonymous Hemianopia Documented by Scanning Laser Ophthalmoscope Retinal Perimetry. Optometry and Vision Science. Volume 80(7), July 2003, pp 495-504. 14. Rousseaux, Marc MD, PhD; et al. Ineffectiveness of Prism Adaptation on Spatial Neglect Signs. Stroke. Volume 37(2), February 2006, pp 542-543. 15. BIFOCALS AND FALLS ARTICLE 16. Pambakian, ALM; Mannan, SK, HodgsonTL; Kennard,C. Saccadic Visual Search Training: a Treatment for Patients with Homonymous Hemianopia. Journal of Neurology, Neurosurgery, and Psychiatry. Volume 75 (10), Oct 2004. pp 14431448.