Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
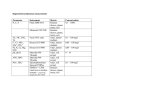
WHI BAA-24: Metabolomics of CHD in the WHI PI: Kathryn Rexrode, MD, MPH Brigham and Women’s Hospital [email protected] WHI Genetics SIG, May 22, 2013 Background • Many of the strongest risk factors for CVD in women are associated with altered metabolism, but exactly how these metabolic perturbations directly impact the pathophysiology of CHD is not clear. • Metabolite profiling techniques (metabolomics) provide a tool for measuring a full profile of small-molecule metabolites, providing a comprehensive picture of an individual’s metabolic status. • These methods have been applied by our group (Clary Clish) to identify a panel of metabolites that predicted incident diabetes over 12 years. (Wang T, et al. Nat Med 2011;17:448-453.) • Although preliminary results for CHD are promising, only small studies with short duration of follow-up have examined these compounds prospectively for CHD. • This project will measure a well-validated metabolomic profile, and test specific metabolic hypotheses for incident CHD. In addition, the proposal will examine how hormone therapy (HT) changes metabolomic profiles, and whether these changes explain the increased risk observed for combined HT. Specific Aims 1. To test individual metabolite and metabolomic profiles associated with incident CHD in women. (Using 400 CHD cases and 400 controls in the WHI-OS, with replication among the 342 cases and 342 controls in the WHI-HT placebo arms). a) To test specific metabolic hypotheses regarding CHD, including Branched-chain amino acids (AA) and aromatic AA, small and medium-chain acylcarnitines, metabolites of dietary phosphotidylcholine, urea cycle metabolite, and desaturation of lipids. b) Agnostic examination of metabolites and metabolomic profiles associated with CHD. 2. To compare changes in metabolomic profiles from baseline to year 1 in E-alone, E+P and placebo controls in the WHI-HT, and to test whether these changes explain the increased risk of CHD with E+P, but not E alone, in the HT trials. 3. To explore the relationship of metabolomic profiles with previously measured clinical parameters, biomarkers and genomic data. (Including blood pressure, waist circumference, body mass index,markers of lipoproteins, inflammation, endothelial function, insulin resistance and thrombosis/fibrinolysis, as well as genomic data). Specific metabolite hypotheses Table 2. Specific hypotheses and metabolites to be tested in this proposal. Specific hypotheses associated with CHD Metabolites Branched-chain amino acids (CAA) and aromatic amino acids (AAA) Small and medium-chain acylcarnitines BCAA: leucine, isoleucine, and valine AAA: phenylalanine and tyrosine Acylcarinitines and dicarboxylacylcarinitines Metabolites of dietary phosphotidylcholine Urea cycle metabolites Trimethylamine N-oxide [TMAO], as well as choline, and betaine Arginine, histidine, and citrulline Desaturation of lipids Triacylglycerols An agnostic evaluation of the complete metabolomic profile (>300 metabolites) will also be performed using principal component analysis, as well as network and pathway approaches. Study Overview • Metabolomic profiles of >300 metabolites will be measured at Broad Institute (Clary Clish) on a total of 2210 women in the WHI (1105 cases and 1105 controls) using a nested case-control design and building upon prior datsets used for biomarker and GWAS studies whenever possible. • Baseline profiles will be measured on enrollment samples from 400 incident CHD cases and 400 controls in the WHI-OS, and on all CHD cases and controls from the WHI-HT trials both at WHI enrollment and year 1. • A two-phase analysis will be conducted with a “discovery cohort” of 400 CHD cases in the WHI-OS, and a “validation cohort” using the 342 CHD cases and matched controls among the placebo arm of the WHI HT trials. • The effect of HT on metabolomic profiles from baseline to year 1 will be compared in estrogen plus progestin (E+P), estrogen alone (E-alone) and placebo arms, and then the degree to which this mediates the observed risk of CHD with E+P will be tested. • Metabolomic data will be integrated with prior clinical, biomarker and genomic data from each of these cohorts using network and pathways approaches. Study design according to specific aim Specific Aim Substudy Analysis Sample year Cases/ controls Aim 1- initial WHI-OS Risk of CHD (initial) WHI baseline 400/400 Aim 1-validation WHI-HT Risk of CHD (validation) WHI baseline 342/342 placebo arms (baseline also used for 2b) Aim 2 a Aim 2b Aim 3 WHI-HT WHI-HT All metabolomics samples Metabolomic change with HT baseline; Year-1 Metabolomic change mediation of CHD risk Year-1 Network analyses of metabolomics, clinical data, biomarkers and genomic data WHI baseline; Year-1 363/363 active arms 363/363 active arms 227/227 placebo arms Variable (1105/1105) Aim 1 will involved a total of 1632 samples (400 pairs of participants from baseline OS and 342 pairs of participants from HT-placebo arms, plus 10% QC). Aim 2 will involve a total of 2849 samples (including 752 baseline samples already measured in aim1). A total of 363 pairs of participants in the HT-active arms for both baseline and year 1 (1597 samples including QC) and 227 pairs of participants in the HT-placebo arms for year 1 measures (500 samples including QC) will be measured for aim 2. Aim 3 will utilize all 3729 samples that will be measured in the proposal. Potential impact of the study • By focusing on molecules that are proximate in the biologic causal pathway, perhaps direct mediators of CHD risk, the likelihood of identifying pharmacologic targets is increased. • Understanding differences in metabolomic profiles between the two hormone therapy arms in the WHI-CT, and whether these differences might mediate impact the difference in CHD risk between the two arms, may have direct clinical implications. • The proposed study: – is of substantially larger size than prior metabolomic studies, – will test a large panel of well-validated metabolites, and – will focus on women who may have substantial differences in levels than men due to sex hormone or other sex-related factors. Investigative team • Brigham and Women’s • Broad Institute: Hospital: Clary Clish, PhD Kathy Rexrode, MD, MPH • University of Christine Albert, MD, MPH Massachusetts: JoAnn Manson, MD, DrPH Raji Balasubramanian, ScD Nina Paynter, ScD • Fred Hutchinson/ WHINancy Cook, ScD CCC: Lesley Tinker, PhD