Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
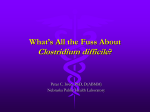
The Impact Of Clostridium difficile infection: a review of the literature Elham .A. Draa*, Ali. S. Arebi*, Safwan .Alarabi*. * Department of Medicine, Zawia Teaching Hospital, faculty of medicine University of Zawia, Zawia, Libya. Abstract Clostridium difficile is anaerobic Gram-positive, spore-forming bacterium that now recognized as the major cause of Antibiotic-associated diarrhea (AAD) worldwide. C. difficile is being increasingly seen in human’s infections, particularly under conditions of perturbed microbiota such as antibiotic treatment. The spectrum of gastrointestinal infections caused by C.difficile is a broad ranging from asymptomatic colonization to severe pseudomembranous colitis (PMC), resulting in a relatively high morbidity and mortality rate, and raised health care costs .We reviewed the pathogenesis, epidemiology, risk factor management and prevention of C. difficile-associated diarrhea (CDAD). key words Clostridium difficile, Antibiotic-associated diarrhea (AAD), pseudomembranous colitis (PMC), Nosocomial infection, C. difficile-associated diarrhea (CDAD). Introduction Clostridium difficile is anaerobic Gram-positive, spore-forming bacillus, which has been recognized as the most frequent cause of hospital-acquired infectious diarrhea worldwide, accounting for up to 1 of every 200 patients who are admitted to hospital, 20% of cases of nosocomial diarrhea1 and 15% of all antibiotic treatment associated diarrhea2. The spectrum of enteric disease caused by C. difficile is a broad ranging from asymptomatic colonization to mild self-limiting antibiotic-associated diarrhea and can progress to more severe pseudomembranous colitis (PMC) and life threatening fulminant colitis. Complications include the development of recurrent C. difficile-associated diarrhea (CDAD) in 20 -30% of cases, ileus or toxic megacolon colonic perforation and death2, 3. The CDAD is a term used to describe the symptomatic manifestation of disease therefore excluding the asymptomatic carrier. The majority of hospital patients with CDAD are elderly, and generally have been on antimicrobials that decrease the “ colonization resistance” of the colon leading to C. difficile colonization and production of C. difficile two toxins which contribute to disease pathogenesis3,4 . The transmission of C. difficile assisted by its ability to form spores that are resistant to many disinfectants allowing it to remain viable in the hospital environment for long periods of time1,5 . Historical background C. difficile was first described in 1935 when Hall and O’Toole discovered a new anaerobe during their study of the development of normal bacterial flora in neonates2,6.The bacterium was name Bacillus difficilis because of the difficulty in isolating it, the bacterium was found to be non pathogenic in newborns infants, but pathogenic in experimental animals due to the presence of a lethal toxin7. C. difficile was presented in the stools of healthy neonates and was classified as a commensal; Staphylococcus aureus was originally implicated as the causative organism of (AAD) and PMC. This view did not change until the 1970s when a prospective study of 200 patients treated with the antibiotic clindamycin, of whom 21% developed diarrhea and 10% had PMC by endoscopy. Consequent lab testing of stool specimens proved the presence of C. difficile toxin 1,8. Over the last 25 years, many studies have been published on the bacterium and the spectrum of associated diseases. In most patients, C. difficile infection does not progress to PMC, because of increased awareness and better laboratory diagnosis of CDAD has become a popular way of describing the disease7. General Microbiology The Clostridium difficile is an anaerobic spore bearing (subterminal) bacillus, belongs to the division Firmicutes, family of the Clostridiaceae and the genus Clostridium. C. difficile is a bacillus of approximately 3-5 μm in length. The genus Clostridium (clostridia) present as Gram-positive, rod-shaped, in Gram staining. The clostridia are ancient bacteria that live in virtually all of the anaerobic habitats of nature where organic compounds are including soils, aquatic sediments and the intestinal tracts of animals8 . C. difficile is able to form structures within the vegetative cell which are called endospores or spores (Figure 1). The non-sporing cell is named as “vegetative”. Spores of C. difficile are resistant to exposure to heat, chemical disinfection, alcohol, air and drying. Upon dehydration the resultant spore formed is oval and terminal in position, and can survive for up to 6 months in the environment 12,13. Recently studies suggest that non-chlorine-based detergents encourage sporulation in C. difficile strains, indicating the importance of choice of cleaning agents used in hospitals 14. It has been shown that C. difficile spore might contribute to recurrent CDAD cases after discontinues treatment, re-infection with new strain occurred in to one half of recurrent cases while the remaining patients relapsed with the –one third original strain15 Figure 1: C. difficile endospores appear clear, vegetative cells dark . Adapted from C. difficile © 2006, Kenneth Todar University of Wisconsin-Madison http://textbookofbacteriology.net/clostridia_2.html (permission taken from Kenneth Todar) Epidemiology C. difficile is spore forming bacteria which can be part of the normal intestinal flora as many as 50% of children under the age of two and less frequently in individuals over two years of age. The organism is carried in gastrointestinal tract (GIT) in approximately 3 % of the general population and 30 % in hospitalized. People requiring prolonged use of antibiotics and the elderly are at a greater risk of acquiring this disease, and can be affected even by low doses. Since the bacteria are found in faeces, a patient who has CDAD excretes large numbers of the spores in their liquid faeces, these can contaminate items or surfaces around the patient’s bed including keypads, equipment, the toilet areas ,sluices, commodes, bedpan and washers. Further the spores can survive for a long time and can be a source of hand-to-mouth infection for others. Healthcare workers can also spread the bacteria to other patients or contaminate surfaces through hand contact, in most cases the disease develops after cross-infection from another patient, either through direct patient to patient contact, via healthcare staff, or via a contaminated environment.7 Incidence The reported incidence of CDAD ranges from 0 to 15 cases per 100 patients in health-care settings during a non-outbreak period, but can raise to 16 and 20 cases per 100 patients during an outbreak2. The incidence of CDAD has however continued to increase since the 1990s despite established infection control programs and effective treatments. Variation in healthcare facilities, the patient’s age and condition, and antibiotics use all contribute to the likely hood of an outbreak2. Generall, the prevalence of CDAD in community or outpatient settings is typically lower (7– 12 cases per 100,000 person-years), but attention has been focused on community acquired CDAD as the number of reported cases is increasing. Since 2003, the incidence of CDAD in many US Canadian and European hospitals has increased markedly, also associated with increased frequency of severe or fulminant disease and recurrent CDAD2,7. Moreover, the mortality due to C. difficile infection in England and Wales rose from 3,757 in 2005 to 6,480 in 2006, an increase of 72% . Age-standardised C. difficile mortality rates were increased by 77% among males, and 66 % among females between 2005 and 2006. Accuracy of reporting has been believed as one of the causes for the statistical increase. PCR ribotype 027outbreaks were reported in 7 hospitals in the Netherlands from April 2005 to February 2006. One hospital detected at the same time a second outbreak due to a toxin A– negative C. difficile PCR ribotype 017 toxinotype VIII strain. ® VIII. The 017 strain had a deletion of the toxin A gene, didnot contain genes for binary toxin production, and had a normal tcdC gene15,16 Clinical features Gastrointestinal The spectrum of disease severity ranges from uncomplicated diarrhea to colitis or PMC and rarely, ileus or toxic megacolon. Symptoms typically occur within 48h of infection with C. difficile and most patients who are infected in hospital become infected within 3 weeks of admission. Less frequently, the onset of symptoms can be delayed by up to 2–3 months9 . The clinical presentation of CDAD typically includes mild or severe diarrhea and lower abdominal cramping pain but can also present with systemic symptom as fever, nausea, anorexia and leukocytosis, they may have hypovolemia, shock, and hypoalbuminemia due to oozing albumin from the blood plasma into the colonic lumen10, acute diarrhea with hypoalbuminemia is a good indicator of C. difficile intestinal disease. Stools are usually not grossly bloody, but they can be11. Occult blood is present in 30% of patients. Fecal leukocytosis is also present in one third of the patients. Colitis, when present, is usually most severe in the rectum and distal colon but it can be present on the right side of the colon. 1-3% of patients develop fulminant colitis, in which case the patient may not have diarrhea but develop signs and symptoms of severe toxicity with fever and diffuse abdominal pain and distension which might result in fatal disease, due to bowel perforation and peritonitis24. Physicians rarely suspect C. difficile disease in the absence of diarrhea7, 25. The presence of PMC suggests an advanced stage of the disease, and although considered “nonspecific,” it is highly indicative of C. difficile infection; it is almost restricted to the colon and rectum and is well defined histopathologically. Pseudomembranous can be visualized by sigmoidoscopy or colonoscopy, as loss of the mucosal folds and plaques with hemorrhagic spots and deep ulceration. Microscopically, this pseudomembrane appears as fibrinous exudates containing epithelial cells, mucin and leucocytes25. Severely ill patients may have no diarrhoea as a characterized feature of toxic megacolon or paralytic ileus because of loss of colonic muscular tone. Toxic megacolon may be associated with severe sepsis and multiple organ dysfunctions26. Mortality associated with toxic megacolon is high, ranging from 25% to 40%. Recurrent diarrhoea is seen in 15–30% of cases27. Despite the infection of the immediately adjacent right colon, the involvement of the distal third of small intestine in infections with C. difficile is rare. Previously reported studies of patients with small bowel involvement have had their intestine altered surgically, which may be a predisposing factor of small bowel susceptibility to pseudomembranous enteritis28. Extra intestinal Clostridium difficile has rarely been isolated from extra intestinal sites. Apart from a few case reports and small case series, the clinical features of extra colonic C. difficile infections have not been studied systematically, probably, the organism has low pathogenic potential outside the intestinal tract. The manifestations of infection include, bacteremia, visceral abscess formation subphrenic, splenic, pancreatic and left iliacus muscle abscess)28, infection of implanted prosthetic devices29, encephalopathy, reactive arthritis, and osteomyelitis30. Cellulites and necrotizing fasciitis of the thigh31. C. Difficile Pathogenesis and Toxins C. difficile infection is commonly related to hospitalization, causes antibiotic associated diarrhea and more serious intestinal conditions such as colitis and PMC. However, CDAD is also increasing in occurrence and severity as a community-acquired disease, probably due to use of proton pump inhibitors36,37. These conditions generally result from overgrowth of C. difficile in the colon, usually after the normal flora has been disturbed by antimicrobial chemotherapy allowing C. difficile to flourish in the intestinal tract. C. difficile then proliferates and produce toxins that causes a watery diarrhea(TcdA and TcdB), if it lacks the gene for toxin production, no disease develops6.This protective effect of the normal microflora is often referred to as “colonization resistance” because it can act as a barrier against infection with C. difficile38. Table1: Antimicrobial agents that induce C. difficile-associated diarrhea and colitis, Adapted from Ciaràn Kelly (British Society of Gastroenterology Meeting 2008,10-13 March, Birmingham oral presentation). Frequent Infrequent Rare Ampicillin Chloramphenicol Metronidazole amoxicillin Trimethoprim Parenteral aminoglycoside Cephalosporins Macrolide Vancomycin Clindamycin Sulfonamide Quinolones I Tetracycline Uncolonized patient Antibiotic exposure +PPI Disruption of colonic micro flora C. difficile ingestion and colonization ______________________________________ Good IgG response Asymptomatic and carrier state Poor or partial IgG response Production of C. difficile toxin A and B Activation of macrophages and mast Cells, Upregulation of cytokines and other mediators of inflammation Clinical disease Figure 2: Pathogenesis of C. difficile Infection. Modified from reference5. The carrier proportion of hospital patients can be as high as 16-35% of inpatients39. CDAD is considered as health-care associated, when diarrhoea starts after at least 48h after admission to the hospital, or onset in the community within 4 weeks after discharge. A case is community acquired when symptoms occur within 48h of admission and without previous hospitalization in the last 12 weeks40. C. difficile multiply and produces two toxins: Toxin A is referred to as an enterotoxin because it causes fluid accumulation in the bowel. Toxin B (cytotoxin) is an extremely Lethal (cytopathic ) toxin. The C. difficile toxins damage colonocytes, impaired cell migration, and cause apoptosis5. C. difficile does not invade the colonic mucosa, the disease does not develop if no toxins are produced5. Even when a toxin is produced, some people became carriers or develop a mild, self-limited diarrhea while others developed severe colitis and may have recurrence of the disease. Serum antibody levels in response to the toxin may modulate disease pathogenesis. Generally, C. difficile disease is caused by genotypes and strains that are resistant to the used antibiotic. Penicillins, cephalosporins and clindamycin are drugs that may precipitate disease7. However, even vancomycin- the effective drug in treating C. difficile infection can cause the disease, this probably happens because vancomycin suppresses both normal flora and the vegetative forms of C. difficile, but not its spores. When vancomycin treatment is stopped, the spores germinate and the new vegetative forms, flourish in the altered bacterial environment7. Risk Factors and Risk Group Although current antibiotic treatment is one of the most important risk factors, the host and environmental factors may also play a role. The major risk factors are highly variable depending on age, duration of hospitalization, and severity of underlying disease23, 41, 42. In patients older than 60 years, the CDAD incidence amongst 5133 cases was ten-fold higher than younger patients41. In a study on 73 patients in an outbreak situation, the mean age was 74 years. Risk factors for CDAD typically include host factors (advanced age, impaired immune status, co morbidities, etc.), increase in exposure to C. difficile spores (longer length hospital stays, the health-care environment, infected roommates, contaminated hands, etc.), and factors causing disruption of protective colonic microflora layer (antibiotic medications, various procedures, repeated enemas, prolonged nasogastric tube insertion and gastrointestinal tract surgery increase a person's risk of developing the disease ). Risk factors for CDAD are shown in Table2. Table2: Risk factors for health-care associated and community acquired CDAD. The contents of the table are from references2. Health-care-associated Risk factor CDAD Community-acquired CDAD Broad-spectrum antibiotics Usually no antibiotic Disruption of normal colonic Medications exposure microflora Surgery Some fluoroquinolones Chronic gastrointestinal conditions Hospital environmental Home surfaces Exposure to C. difficile surfaces Family members spores Infected roommates Pets Hand carriage by health-care Personnel Impaired immune system Host factors Young children Low production of anti-toxin Post-partum women A and/or B antibodies Use of PPIs Comorbidities Advanced age Strain type (outbreaks) Microbial factors Table3: The main C. difficile virulence factors Sporulation capacity Two high-molecular-weight toxins:Toxin Aenterotoxin or TcdA Toxin B cytotoxin or TcdB Bacterial factors A binary toxin ( CDT) Motility/ chemotaxis Adhesion Surface layer protein (SLP) Flagella Host factors Cytoskeletal rearrangement Microtubules Micro filaments Tyrosine phosphorylation Proinflammatory -IL 8 induction Diagnosis A diagnosis of CDAD generally requires both clinical and laboratory and exclusion of other etiologies of diarrhea, such as drugs or chronic intestinal conditions, C. difficile diarrhea is confirmed by the presence of toxin in stool specimen. A positive culture for C. difficile without a toxin assay is not sufficient to make the diagnosis of CDAD. Stool cultures may be complicated by the finding of non-toxigenic strains of the bacterium, so the most reliable and widely used tests involve detection for the presence of the toxin A and/or toxin B in the stool, although atypical toxin variant strains (A–B+) can also cause symptoms (Table 4). Interestingly, some patients have stool assays positive for toxin but they do not exhibit disease symptoms (asymptomatic carriers). On the other hand, the lack of a toxin-positive stool assay does not rule out CDAD. The toxins are very unstable. They degrade at room temperature and cannot be detected two hours after collection of stool specimen, leading to false negative results (29-56% of cases). Methods to reduce the percentage of false negative results include the use of rapid enzyme immunoassays that identify both toxin A and toxin B, repeat stool assays and investigate the isolate for toxin44 . The most highly sensitive diagnostic test for C. difficile detection is both cell culture cytotoxin assay as well as anaerobic culture of organisms, although there is no accepted standard, the cell cytotoxicity assay is considered the “gold standard”44,45, while some microbiologists used toxinogenic culture as the “gold standard”46 . Endoscopy, although with poor sensitivity, macroscopic diagnosis of CDAD can be made by rectoscopy, sigmoidoscopy or colonoscopy for direct visualization of the colonic mucosa and detection of pseudo membranes44. However, a negative result does not exclude infection because diarrhoea can develop without pseudomembranes47. Endoscopy is usually recommended when patients have ileus and are unable to produce watery or loose faecal samples so it helps to obtain a stool sample for toxin assay48,49. A computed tomography scaning is often diagnostic of C difficile colitis, provided physicians think of this disease in the absence of diarrhea. Table 4: Stool Tests for Diagnosis of C. Difficile Infection. Adapted from reference61 Test Disadvantages Detects Advantages Polymerase Toxin A or B high requires expertise in chain reaction genes in isolates or sensitivity97% molecular directly in faeces specificity100 diagnostic techniques Latex bacterial enzyme fast poor sensitivity and agglutination (glutamate inexpensive specificity assay Dehydrogenase) easy to perform Enzyme Ttoxin A or B fast not as sensitive as easy to perform cytotoxin assay immunoassay high specificity Cytotoxin assay requires tissue Toxin B GSold standard culture facility Highly sensitive takes 24-48 hours 94%-100% False-positives Highly specific Results vary with 99%-100% experience Of the technologist Culture Toxigenic and Non toxigenic C. sensitive requires anaerobic Difficile allows strain culture typing in not specific for epidemics toxin producing bacteria takes 2-5 days Treatment for C. difficile-associated disease The management of CDAD remains problematic (Table 5). The first approach to the treatment, as soon as C. difficile disease is diagnosed, is withdrawal or change the precipitating antibiotic with lower CDAD risk antibiotic50, studies show number of patients respond well to this approach and additional treatment is required45. Severe cases may require antibiotic treatment, the most common treatments are oral vancomycin or oral metronidazole . Additionally another approach for treatment or prophylaxis is probiotics therapy, where use of non-pathogenic organisms helps to prevent colonization of C. difficile51,52. Agents that inhibit toxin A binding such as cholestyramine and immunotherapy with antitoxin A antibodies have also been applied53. Patients must be monitored for dehydration and electrolyte imbalance after prolonged diarrhea. Antidiarrheal agents such as Lomotil or Imodium should not be taken as they have been shown to increase the severity of symptoms and precipitate megacolon. C. difficile infections usually can be treated successfully with a 10 day course of antibiotics including metronidazole or vancomycin. Although, resistance to metronidazole and vancomycin has been reported but so far has not been a significant clinical problem. It is suggested that patients with C .difficile infection who require long-term antibiotic therapy (e.g. those with bacterial endocarditis or osteomyelitis) should maintain metronidazole or vancomycin therapy for 1 week after completion of longterm antibiotic therapy53. Table 5: Standard therapy for Clostridium difficile infection, Adapted from reference 53 Disease characteristic Regimen Metronidazole 250mg orally (P.O) four times Mild disease (no systemic dailyv for 500 mg three times a day for 10-14 symptom only mild diarrhea) days Moderate disease (fever, Vancomycin HCl ,125-500 mg P.O four times profuse diarrhea, abdominal daily for10-14 days pain leukocytosis) Severe disease (Paralytic Surgical consult and intraluminal ileus, toxic megacolon sepsis, vancomycin dehydration) Inability to take medication Intraluminal vancomycin with or without intravenous Metronidazol Therapy for recurrent C. difficile infection The main complication of CDAD treatment is the relapse, of which occurs in about 20 to 25% of cases. The symptoms usually return after 3 to 21 days (average,6) from withdrawal of metronidazole or vancomycin. Assays for C. difficile toxin are not immediately necessary after finishing treatment course, at which the results could be confusing, as about one third of patients with successful therapy are positive in assays. Most recurrent C.D infection respond to another course of standard antibiotics doses for 10 days, while 3 to 5 % of patients have more than six relapses54,58. Management is controversial, and the course may involve complications and considerable expense57. For repeated relapses, therapy for four to six weeks is recommended to control C. difficile infection, these prolonged treatment include the administration of pulsed doses of vancomycin (125 mg every other day which can maintain C. difficile in the spore form and has minimum effects on the colonic flora), the use of 4g of cholestyramine three times daily to absorb C. difficile toxin , or the use of agents such as probiotics Saccharomyces boulardii or Lactobacillus56,58. The use of intravenous immunoglobulin has been suggested, based on recent data show that patients with relapses have diminished plasma concentrations of IgG antibodies against toxin A58. Reconstituting normal flora by enemas and infusion of donor feces show good response rates but this solution is not ideal, due to possible risk of transmission of retroviruses or other agents59. Prevention and control Prevention and control of CDAD in hospitals basically depend on two factors: limiting use of antibiotic and interruption of transmission of C. difficile by infection control strategies. In many cases stoppage of suspected antibiotic is enough, metronidazole is a commonly used drug with vancomycin for severe cases. Recently, use of probiotics for prevention, vaccination against C.difficile and colonization with nontoxigenic C.difficile strains has also been suggested. The vegetative form of C. difficile is largely found on fecally-contaminated surfaces and may be killed by EPA- hospital-use disinfectant products or by exposure to air. However, it is important to note that disinfectants (alcohol solution) or disinfectant-detergents used on environmental surfaces are not effective against the spore form of C. difficile. Hand hygiene, washing practice techniques and the proper handling of contaminated wastes (including diapers) are absolutely effective in preventing the spread of the disease and interruption of the disease transmission from person to person via the hands. Environmental surfaces contaminated with C. difficile spores should be cleaned with an effective disinfectant (bleach), aggressive cleaning and disinfection is effective in reducing the number of C. difficile positive cultures in the environment60. In the case of a C. difficile outbreak, isolation of patients with CDAD and education of staff with attention to traditional hand washing with soap and water for the mechanical removal and rinsing of spores from the hands is recommended. No sharing electronic thermometers, clean surfaces in bathrooms, kitchens and other areas on a regular basis with household detergent/ a chlorine containing disinfectant is recomended60. Reference List (1) Tedesco FJ, Barton RW, Alpers DH. Clindamycin-associated colitis. A prospective study. Ann Intern Med 1974 Oct;81(4):429-33. (2) Hurley BW, Nguyen CC. The spectrum of pseudomembranous enterocolitis and antibiotic-associated diarrhea. Arch Intern Med 2002 Oct 28;162(19):2177-84. (3) Elliott B, Chang BJ, Golledge CL, Riley TV. Clostridium difficile-associated diarrhoea. Intern Med J 2007 Aug;37(8):561-8. (4) Loo VG, Bourgault AM, Poirier L, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med 2011;365:1693-703. (5) Schroeder MS. Clostridium difficile--associated diarrhea. Am Fam Physician 2005 Mar 1;71(5):921-8. (6) Gupta A, Khanna S. Community-acquired Clostridium difficile infection: an increasing public health threat. Infect Drug Resist. 2014;7:63–72.PubMed (7) McFarland LV. Update on the changing epidemiology of Clostridium difficile associated disease. Nat Clin Pract Gastroenterol Hepatol 2008 Jan;5(1):40-8. (8) Jackson S, Calos M, Myers A, Self WT. Analysis of proline reduction in the nosocomial pathogen Clostridium difficile. J Bacteriol 2006 Dec;188(24):8487-95. (9) Quirk M. Clostridium difficile epidemic strain far reaching. Lancet Infect Dis 2006 Feb;6(2):74. (10) Bartlett JG. Clinical practice. Antibiotic-associated diarrhea. N Engl J Med 2002 Jan 31;346(5):334-9. (11) Monaghan T, Boswell T, Mahida YR. Recent advances in Clostridium difficile associateddisease. Gut 2008 Jun;57(6):850-60. (12) Buggy BP, Hawkins CC, Fekety R. Effect of adding sodium taurocholate to selective media on the recovery of Clostridium difficile from environmental surfaces. J Clin Microbiol 1985 Apr;21(4):636-7. (13) Wilson KH, Kennedy MJ, Fekety FR. Use of sodium taurocholate to enhance spore recovery on a medium selective for Clostridium difficile. J Clin Microbiol 1982 Mar;15(3):443-6. (14) Wilcox MH, Fawley WN. Hospital disinfectants and spore formation by Clostridium difficile. Lancet 2000 Oct 14;356(9238):1324. (15) Tang-Feldman Y, Mayo S, Silva JJ, Jr., Cohen SH. Molecular analysis of Clostridium difficile strains isolated from 18 cases of recurrent clostridium difficile-associated diarrhea. J Clin Microbiol 2003 Jul;41(7):3413- 3414 (16) Kuijper EJ, Van den Berg RJ, Debast S, Visser CE, Veenendaal D, Troelstra A, et al. Clostridium difficile ribotype 027, toxinotype III, the Netherlands. Emerg Infect Dis 2006 May;12(5):827-30. (17) Johnson S, Sambol SP, Brazier JS, Delmee M, Avesani V, Merrigan MM, et al. International typing study of toxin A-negative, toxin B-positive Clostridium difficile variants. J Clin Microbiol 2003 Apr;41(4):1543-7. (18) Rupnik M, Kato N, Grabnar M, Kato H. New types of toxin A-negative, toxin Bpositive strains among Clostridium difficile isolates from Asia. J Clin Microbiol 2003 Mar;41(3):1118-25. (19) Al-Barrak A, Embil J, Dyck B, Olekson K, Nicoll D, Alfa M, et al. An outbreak of toxin A negative, toxin B positive Clostridium difficile-associated diarrhea in a Canadian tertiary-care hospital. Can Commun Dis Rep 1999 Apr 1;25(7):65-9. (20) Alfa MJ, Kabani A, Lyerly D, Moncrief S, Neville LM, Al-Barrak A, et al. Characterization of a toxin A-negative, toxin B-positive strain of Clostridium difficile responsible for a nosocomial outbreak of Clostridium difficile-associated diarrhea. J Clin Microbiol 2000 Jul;38(7):2706-14. (21) Kato H, Kato N, Watanabe K, Iwai N, Nakamura H, Yamamoto T, et al. Identification of toxin A-negative, toxin B-positive Clostridium difficile by PCR. J Clin Microbiol 1998 Aug;36(8):2178-82. (22) Kuijper EJ, de WJ, Kato H, Kato N, van Dam AP, van d, V, et al. Nosocomial outbreak of Clostridium difficile-associated diarrhoea due to a clindamycin-resistant enterotoxin A-negative strain. Eur J Clin Microbiol Infect Dis 2001 Aug;20(8):528-34. (23) Kyne L, Merry C, O'Connell B, Kelly A, Keane C, O'Neill D. Factors associated with prolonged symptoms and severe disease due to Clostridium difficile. Age Ageing 1999 Mar;28(2):107-13. (24) Koss K, Clark MA, Sanders DS, Morton D, Keighley MR, Goh J. The outcome of surgery in fulminant Clostridium difficile colitis. Colorectal Dis 2006 Feb;8(2):149-54. (25) Barroso LA, Wang SZ, Phelps CJ, Johnson JL, Wilkins TD. Nucleotide sequence of Clostridium difficile toxin B gene. Nucleic Acids Res 1990 Jul 11;18(13):4004. (26) Dobson G, Hickey C, Trinder J. Clostridium difficile colitis causing toxic megacolon, severe sepsis and multiple organ dysfunction syndrome. Intensive Care Med 2003 Jun;29(6):1030. (27) Maroo S, LaMont JT. Recurrent clostridium difficile. Gastroenterology 2006 Apr;130(4):1311-6. (28) Jacobs A, Barnard K, Fishel R, Gradon JD. Extracolonic manifestations of Clostridium difficile infections. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2001 Mar;80(2):88-101. (29) McCarthy J, Stingemore N. Clostridium difficile infection of a prosthetic joint presenting 12 months after antibiotic-associated diarrhoea. J Infect 1999 Jul;39(1):94-6. (30) Riley TV, Karthigasu KT. Chronic osteomyelitis due to Clostridium difficile. Br Med J (Clin Res Ed) 1982 Apr 24;284(6324):1217-8. (31) Bhargava A, Sen P, Swaminathan A, Ogbolu C, Chechko S, Stone F. Rapidly progressive necrotizing fasciitis and gangrene due to Clostridium difficile: case report. Clin Infect Dis 2000 Jun;30(6):954-5. (36) Dial S, Delaney JA, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA 2005 Dec 21;294(23):2989-95. (37) Dial S, Delaney JA, Schneider V, Suissa S. Proton pump inhibitor use and risk of community-acquired Clostridium difficile-associated disease defined by prescription for oral vancomycin therapy. CMAJ 2006 Sep 26;175(7):745-8. (38) Macdonald TT. The mucosal immune system. Parasite Immunol 2003 May;25(5):23546. (39) Aslam S, Hamill RJ, Musher DM. Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis 2005 Sep;5(9):549-57. (40) Kuijper EJ, Coignard B, Tull P. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin Microbiol Infect 2006 Oct;12 Suppl 6:2-18. (41) Karlstrom O, Fryklund B, Tullus K, Burman LG. A prospective nationwide study of Clostridium difficile-associated diarrhea in Sweden. The Swedish C. difficile Study Group. Clin Infect Dis 1998 Jan;26(1):141-5. (42) Kyne L, Sougioultzis S, McFarland LV, Kelly CP. Underlying disease severity as a major risk factor for nosocomial Clostridium difficile diarrhea. Infect Control Hosp Epidemiol 2002 Nov;23(11):653-9. (43) Banno Y, Kobayashi T, Kono H, Watanabe K, Ueno K, Nozawa Y. Biochemical characterization and biologic actions of two toxins (D-1 and D-2) from Clostridium difficile. Rev Infect Dis 1984 Mar;6 Suppl 1:S11-S20. . (44) Delmee M, Van BJ, Simon A, Janssens M, Avesani V. Laboratory diagnosis of Clostridium difficile-associated diarrhoea: a plea for culture. J Med Microbiol 2005 Feb;54(Pt 2):187-91. (45) Bartlett JG. Antibiotic-associated diarrhea. Clin Infect Dis 1992 Oct;15(4):573-81. (46) Zheng L, Keller SF, Lyerly DM, Carman RJ, Genheimer CW, Gleaves CA, et al. Multicenter evaluation of a new screening test that detects Clostridium difficile in fecal specimens. J Clin Microbiol 2004 Aug;42(8):3837-40. (47) Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ 2004 Jul 6;171(1):51-8. (48) Fekety R. Guidelines for the diagnosis and management of Clostridium difficile associated diarrhea and colitis. American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 1997 May;92(5):739-50. (49) . Brecher SM, Novak-Weekley SM, Nagy E.Laboratory diagnosis of Clostridium difficile infections. Clin Infect Dis. 2013;57(8):1175-1181 (50) Riley TV, Cooper M, Bell B, Golledge CL. Community-acquired Clostridium difficile associated diarrhea. Clin Infect Dis 1995 Jun;20 Suppl 2:S263-S265. (51) Clayton L Golledge, Thomas V Riley. Natural therapy for infectious diseases. The Medical Journal of Australia MJA ; 1996;-164. (52) Lewis SJ, Freedman AR. Review article: the use of biotherapeutic agents in the prevention and treatment of gastrointestinal disease. Aliment Pharmacol Ther 1998 Sep;12(9):807-22. (53) Sunenshine RH, McDonald LC. Clostridium difficile-associated disease: new challenges from an established pathogen. Cleve Clin J Med 2006 Feb;73(2):187-97. (54) Bartlett JG. Management of Clostridium difficile infection and other antibioticassociated diarrhoeas. Eur J Gastroenterol Hepatol 1996 Nov;8(11):1054-61. (55) Bartlett JG. Treatment of Clostridium difficile colitis. Gastroenterology 1985 Nov;89(5):1192-5. (65) McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW, Moyer KA, et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994 Jun 22;271(24):1913-8. (57) McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW, Greenberg RN. Recurrent Clostridium difficile disease: epidemiology and clinical characteristics. Infect Control Hosp Epidemiol 1999 Jan;20(1):43-50.98 (58) Gorbach SL, Chang TW, Goldin B. Successful treatment of relapsing Clostridium difficile colitis with Lactobacillus GG. Lancet 1987 Dec 26;2(8574):1519. (59) van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG, et al. (2013) Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 368: 407-415. (60) Siegel JD, Rhinehart E, Jackson M, Chiarello L. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am J Infect Control 2007 Dec;35(10 Suppl 2):S65-164. (61) Drudy D, O'Donoghue DP, Baird A, Fenelon L, O'farrelly C. Flow cytometric analysis of Clostridium difficile adherence to human intestinal epithelial cells. J Med Microbiol 2001 Jun;50(6):526-34.