Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Bevacizumab wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Fundus photography wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
Retinal waves wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
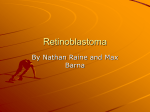
CLINICAL SCIENCES ONLINE FIRST Intra-arterial Chemotherapy for Retinoblastoma Report No. 2, Treatment Complications Carol L. Shields, MD; Carlos G. Bianciotto, MD; Pascal Jabbour, MD; Gregory C. Griffin, MD; Aparna Ramasubramanian, MD; Robert Rosenwasser, MD; Jerry A. Shields, MD Objective: To describe treatment complications following intra-arterial chemotherapy (IAC) for retinoblastoma. Methods: A retrospective interventional series of ophthalmic artery cannulation for IAC injection (3 planned sessions at 1-month intervals) was undertaken. Thirty-eight catheterizations of 17 eyes of 17 patients were performed from September 2008 to September 2010. Fluoroscopy of the ophthalmic artery was performed before and immediately after treatment. Heparin was given during the procedure and aspirin (40 mg) was given orally for 1 week. The treatment complications were determined. Results: Only 17 of 190 children were selected for treat- ment with IAC during this period. Following successful ophthalmic artery cannulation in 16 cases, there was no evidence of metastasis, stroke, brain injury, or persistent systemic toxic effects. Fluoroscopy demonstrated patent ophthalmic artery immediately before and after IAC injection in each case. Following therapy, orbital and adnexal findings at 1 month included eyelid edema (n=13), blepha- W Author Affiliations: Ocular Oncology Service, Wills Eye Institute (Drs C. L. Shields, Bianciotto, Ramasubramanian, and J. A. Shields), Division of Neurovascular and Endovascular Surgery, Department of Neurological Surgery (Drs Jabbour and Rosenwasser), and Division of Pediatric Hematology/Oncology, Department of Pediatrics, Nemours/Alfred I. duPont Hospital for Children (Dr Griffin), Thomas Jefferson University, Philadelphia, Pennsylvania. roptosis (n=10), cilia loss (n=1), and orbital congestion with temporary dysmotility (n=12). These findings resolved within 6 months in all cases. Following therapy, vascular findings included ophthalmic artery stenosis (permanent in 3 cases, temporary in 1 case), confirmed on fluoroscopy in 3 cases. Concomitant central or branch retinal artery occlusion was noted (permanent in 2 cases, temporary in 1 case). Subtle retinal pigment epithelial mottling in 9 cases that slowly evolved to later-onset underlying choroidal atrophy in 5 cases was noted. Conclusions: Treatment with IAC for retinoblastoma can lead to mild and severe short-term ocular complications, including eyelid edema as well as potentially blinding vascular obstruction. This procedure should be used with caution. Arch Ophthalmol. 2011;129(11):1407-1415. Published online June 13, 2011. doi:10.1001/archophthalmol.2011.151 ITH MOST NEW therapies, there is an initial enthusiasm for the developing alternative treatment; later, the limitations, indications, and complications are more precisely defined.1 With regard to retinoblastoma therapies, the enthusiasm for external beam radiotherapy was dampened when intermediate-term dry eye, cataract, sunken socket, and facial deformity were noted and See also pages 1399, 1458, 1487, 1490, and 1492 nearly abandoned when long-term second cancers were realized.2,3 With chemoreduction, the initial dramatic response of advanced retinoblastoma to the 3-drug regimen was extraordinarily impressive, until it was realized later that subretinal and vitreous seed recurrence was a problem.4 Similarly with plaque radiotherapy, the prelimi- ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1407 nary remarkable tumor control was occasionally followed by ischemic retinopathy, hemorrhage, and vision loss.5 Intra-arterial chemotherapy (IAC) for retinoblastoma has been heralded as a novel method for precise delivery of a small dose of chemotherapy into the ophthalmic artery, minimizing systemic chemotherapy toxic effects.1,6 Infusion of IAC for retinoblastoma was previously explored in the 1950s by Reese et al7 and in the 1960s by Kiribuchi.8 Reese and coworkers evaluated 31 children with retinoblastoma treated with internal carotid artery chemotherapy and radiotherapy and found this combination more effective than radiotherapy alone. More recently, Japanese collaborators improved the technique by entering the carotid region from a remote femoral artery access.9 They delivered chemotherapy into the internal carotid artery at the branch point of the ophthalmic artery (without entering the artery) by occluding further distal flow in the internal carotid artery using balloon WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. obstruction. They described the safety of this technique with hundreds of cannulations and no sign of stroke, but detailed data regarding tumor control and treatment complications were lacking in their articles.9,10 Gobin and Abramson11 and Gobin et al12 in the United States devised a refined approach with direct catheter entry into the proximal portion of the ophthalmic artery for deliver of chemotherapy to the eye. With this approach, Abramson et al13-15 provided initial observations of impressive tumor response, even in eyes with advanced retinoblastoma.Regardingtreatmentcomplications,theyobserved that “the only adverse ophthalmic findings were occasional transient lid edema, forehead hyperemia, and loss of nasal lashes.”15 However, other information (from the same group of investigators) remarked on more serious complications including femoral artery occlusion for 1 week and leukopenia in fewer than 10%, and they identified that “there were 4/46 severe ocular complications which consisted of avascular retinopathies resulting in blindness.”12 Further investigation of published reports has revealed illustrations documenting outstanding tumor regression but with visible complications of diffuse retinal pigment epithelial (RPE) alterations and choroidal ischemia.15 We have described our experience with somewhat impressive short-term control of retinoblastoma using IAC in selected cases.16 Herein, we delineate the ocular and systemic complications using this technique. METHODS Institutional review board permission was obtained for this ongoing prospective study on September 15, 2008. Inclusion criteria were the presence of viable unilateral or bilateral retinoblastoma in patients aged 4 months or older in whom the only other options would be enucleation, external beam radiotherapy, or systemic chemoreduction. Patients were excluded if the retinoblastoma could be controlled with more conservative methods of cryotherapy, thermotherapy, or plaque radiotherapy. Patients and parents were informed of the risks of ophthalmic artery cannulation, including brain or orbital hemorrhage, infection, and inflammation, visual loss, loss of the eye, anaphylaxis, stroke, and death. Patients and parents were informed of the unknown risks of systemic metastasis from retinoblastoma using this technique and long-term ocular and systemic toxic effects. Exclusion criteria included opaque or hazy media that precluded visualization of the fundus, fresh or recurrent retinoblastoma that could be amenable to other conservative therapies, and clinical evidence suggestive of retinoblastoma invasion into the optic nerve, choroid, sclera, or orbit or distant metastasis. The details of the technique of examination and follow-up are described in a separate article.16 Each patient was examined initially in the office and then under anesthesia by one of us (C.L.S.) with clinical evaluation and large fundus drawings, fundus photography, and fluorescein angiography of all tumors in each eye. The IAC was performed under anticoagulation with intravenous heparin (75 IU/kg) and has been described previously.16,17 Chemotherapy diluted in 30 mL of saline was delivered using a pulsatile, nonlaminated technique manually over 30 minutes. The selected chemotherapy drug was melphalan (5 mg) in all cases and additional carboplatin (30 mg) was used in cases 1 through 6 based on previously documented efficacy.18 Carboplatin was later discontinued after observations of ophthalmic or retinal vascular attenuation as platinum-based drugs have been recognized to have a sclerosing effect.19 A postinfusion arteriogram was taken to confirm patency of the ophthalmic artery. Following catheter withdrawal, oral aspirin (40 mg) was delivered for 2 weeks. Follow-up ophthalmic examination was provided at 1 month, and a second treatment with IAC was performed as necessary and then repeated 1 month later if necessary. Thereafter, ophthalmic examination was provided every 2 to 3 months. Documentation was made in each case with large fundus drawing, fundus photography with a Retcam camera (Massie Industries, Dublin, California), fluorescein angiography, and electroretinography. All data were collected in a retrospective fashion. Each patient was evaluated for age at diagnosis (months), race (African American, Asian, Hispanic, white), sex (male, female), and hereditary pattern (sporadic, familial). Before and following IAC, each patient was assessed for metastatic disease, second cancer, pinealoblastoma, and damage to the central nervous system manifesting as neurological deficit or stroke. The orbit and adnexa were evaluated for permanent or temporary eyelid edema, blepharoptosis, forehead erythema, eyelash loss, and dysfunction of the extraocular muscles. The globe was assessed for patency of the vascular flow to the eye including the internal carotid artery, ophthalmic artery, central retinal artery, branch retinal artery, retinal venous drainage, and choroidal vascular bed. The fundus was evaluated for the status of the retina, RPE, and optic nerve. New or preexisting neovascularization of the iris with or without neovascular glaucoma was recorded. RESULTS Seventeen patients were included in this study on IAC for retinoblastoma. The mean patient age at IAC was 20 months (range, 4-74 months). Cannulation into the proximal region of the ophthalmic artery was possible in 16 patients. In 1 patient, cannulation was not possible owing to internal carotid artery anomalous pattern with a 360° loop and severe spasm during the procedure. This patient was subsequently treated with intravenous chemoreduction. A total of 37 of 38 catheterizations of the ophthalmic artery were successful for delivery of chemotherapy. All catheterizations were unilateral. The mean number of catheterizations per eye for control of retinoblastoma was 2.25 (median, 2; range, 1-4). Following IAC, complete response of the main tumor was achieved in 14 cases (88%), partial response was found in 2 cases (12%), and no response was observed in 0 cases.16 Globe classification, tumor features, treatment parameters, and tumor control for this cohort of 17 patients are detailed in a separate article.16 The systemic and ocular complications of IAC for retinoblastoma are listed in Table 1 and Table 2 (Figures 1, 2, 3, 4, and 5). No patients developed metastasis, second cancer, or pinealoblastoma during a mean of 13 months of follow-up. No patients developed neurological defect, internal carotid artery occlusion, femoral artery occlusion, or stroke. One patient with anomalous internal carotid artery had a spasm during cannulation and the procedure was discontinued. Transient cytopenia was present in 6 cases with spontaneous recovery in all cases without the need for transfusion. Ophthalmic adverse effects included eyelid edema (n = 13), blepharoptosis (n = 10), and cilia loss (n = 1) (Figure 1). There were no cases of forehead erythema. Congested orbit with temporary extraocular muscle dysfunction was found in 12 eyes. These external findings ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1408 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. Table 1. Systemic and Brain Complications From Intra-arterial Chemotherapy for Retinoblastoma Systemic Patient No. Brain Metastasis Second Cancer Pinealoblastoma Transient Cytopenia Neurological Defect Internal Carotid Artery Stroke MRI Result No No No No No No No No No No No No No No No No No 0 No No No No No No No No No No No No No No No No No 0 No No No No No No No No No No No No No No No No No 0 No Mild No No Mild No Mild Mild Mild No No No No No Mild No No 6 No No No No No No No No No No No No No No No No No 0 Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Spasm a No No No 1 No No No No No No No No No No No No No No No No No 0 Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl Nl 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Total, No. Abbreviations: MRI, magnetic resonance imaging; Nl, normal. a Transient carotid spasm occurred, so the procedure was discontinued. The patient was treated successfully with intravenous chemoreduction. Table 2. Ocular Complications From Intra-arterial Chemotherapy for Retinoblastoma Globe Orbit and Adnexa Transient Extraocular Muscle Ophthalmic Retinal Retinal Retina Patient No. Eyelid Forehead Eyelashes Restriction Artery Artery Vein Detachment 1 2a E, P E, P Nl Nl Nl Nl Mild Mild 3 4 5 6 7 E, P E E, P Nl E Nl Nl Nl Nl Nl Nl Nl Nl Nl Loss 8 9c 10 11 12 E E, P Nl E, P E, P Nl Nl Nl Nl Nl 13 E, P 14 15 16 17 Total, No. Nl E, P E, P Nl 13 RPE Mottling Choroidal Vascular Atrophy Optic Nerve Atrophy NVI NVG Nl VH, no view Nl Nl Nl CRAO BRAO Nl VH, no view Nl Nl Nl NA Nl SRD No No VH, no view No No No No VH, no view VH, no view Yes, new Yes, new Mod Mild Mild Nl Mild Nl VH, no view b Nl Nl Nl Stenosis Stenosis No No No No SRD No No Yes, diffuse Yes, diffuse No No No No Yes No No No No No No No No No No No Nl Nl Nl Nl Nl Mod Nl Mild Nl Mild Nl Nl Nl Nl Nl Nl Nl Nl BRAO Nl Nl Nl Nl Nl Nl No TRD No No No Yes, diffuse Yes, focal Yes, diffuse Yes, diffuse Yes but extensive subretinal seeding Yes, focal No view Yes, diffuse Yes, diffuse No No No view Yes, diffuse Yes, diffuse No No No view No No No No Yes, old No No No Nl Nl Nl Nl Nl Nl No No No Nl Nl Nl Nl 0 Nl Nl Nl Nl 1 Nl Mild Mod Mild 12 NA Stenosis d Nl Nl 4 NA BRAO d Nl Nl 5 NA Nl Nl Nl 0 NA No No No 3 Yes, focal but previous SRD NA Yes, focal No No 9 No Yes, old No No Yes but total SRD No NA Yes, focal No No 5 NA No No No 1 NA No No No 3 NA No No No 2 No Abbreviations: BRAO, branch retinal artery obstruction; CRAO, central retinal artery obstruction; E, edema; Mod, moderate; NA, not applicable; Nl, normal; NVG, neovascular glaucoma; NVI; neovascularization of the iris; P, ptosis; RPE, retinal pigment epithelium; SRD, serous retinal detachment; TRD, traction retinal detachment; VH, vitreous hemorrhage. a Vitreous hemorrhage was present at the initial visit and worsened following chemotherapy. b An ophthalmic arteriogram showed stenosis of the artery, despite no view. c The patient had NVI at the initial visit with progression to NVG following chemotherapy, leading to enucleation despite tumor control. d Stenosis was found at month 1 and resolved by month 2. resolved in every case by 2 months, but blepharoptosis resolved more slowly over 4 to 6 months. In 1 case, the dysmotility respected the distribution of the third cra- nial nerve and persisted for 4 months. Occlusive vasculopathy was noted in the ophthalmic artery in 4 cases and diagnosed by funduscopy in 3 of those cases. In 1 case, ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1409 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. A B Figure 1. Eyelid findings following intra-arterial chemotherapy for retinoblastoma. A, Case 2, with eyelid edema 1 week after intra-arterial chemotherapy. B, Case 8, with no eyelid abnormality 1 year after intra-arterial chemotherapy. A B C D Figure 2. Retinal pigment epithelial (RPE) alterations after intra-arterial chemotherapy (IAC) for retinoblastoma. A and B, Case 4. Peripheral retinoblastoma with vitreous seeding was treated with IAC. Note the normal RPE at the nasal juxtapapillary region at the initial visit (A) and mild RPE alterations following 1 cycle of IAC (B). C and D, Case 10. C, Recurrent retinoblastoma on the temporal margin of the regressed tumor (at the photograph’s edge) following chemoreduction was treated with IAC. Note the unaffected RPE superior to the calcified mass at the time of the first IAC treatment (C) and then moderate RPE alterations with choroidal atrophy 6 months later (D). preexisting mild vitreous hemorrhage worsened following IAC and there was no view of the fundus. However, on arteriography, the ophthalmic artery showed stenosis and further therapy was discontinued. Of those with clinically visible ophthalmic artery occlusion, the main fundus features included central retinal artery obstruc- tion (n=1), multifocal branch retinal artery obstruction (n=3), and evidence of choroidal atrophy (n=2). In 1 case, the ophthalmic artery obstruction and related branch retinal artery obstruction resolved completely within 1 month. In 1 case, the choroid was camouflaged by extensive confluent subretinal seeding. ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1410 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. A B C D Figure 3. Evolution of retinal pigment epithelial alterations after intra-arterial chemotherapy for retinoblastoma in case 8. Macular retinoblastoma (A) was treated with 1 cycle of IAC, with complete response at 1 month (B). Nasal retinal pigment epithelial alterations were barely visible at 1 month (C) but evolved to a broad, subtle, linear retinal pigment epithelial atrophy at 11 months’ follow-up (D), despite no further chemotherapy. There were no visible emboli in any artery on ophthalmoscopy or fluorescein angiography. On fluorescein angiography, the 3 cases of posttreatment central retinal artery obstruction and branch retinal artery obstruction showed slow perfusion of the attenuated retinal arteries. Despite the poor flow, no iris neovascularization, neovascular glaucoma, or pain developed. One patient who initially had mild vitreous hemorrhage (presumably from pretreatment retinal neovascularization) eventually developed dense vitreous hemorrhage and neovascular glaucoma and required enucleation. Of the 5 eyes with iris neovascularization before treatment, only 1 had persistent neovascularization after treatment (requiring enucleation) and the remainder showed resolution of neovascularization with tumor regression and resolution of the retinal detachment. Following IAC, attenuation of the choroidal vascular bed was found in 5 cases. Of 13 patients followed up for 6 months or longer, choroidal atrophy was noted in 4 of the 9 patients (44%) in whom a clear view of the choroid was obtained. This finding was noted in 1 of 3 patients followed up for less than 6 months. This finding initially manifested as focal or diffuse RPE mottling with gradual loss of the choriocapillaris and, in some cases, the larger choroidal vessels. Following IAC, RPE mottling was detected in 9 eyes and with gradual progression over time (Figure 3 and Figure 5). In 3 eyes, there was poor to no view of the RPE due to overlying vitreous hemorrhage or confluent subretinal seeds. COMMENT We have used IAC for longer than 2 years in the management of selected cases of retinoblastoma.16 We have observed both complete response and less impressive partial response of retinoblastoma. We have used this therapy for primary as well as recurrent retinoblastoma. In a separate article describing our 2-year experience with this approach, we found 100% tumor control for primary retinoblastoma in group C and D eyes and 33% control for group E eyes.16 However, we use this new therapy with caution because of the potential for local ocular toxic effects. ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1411 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. A B C D Figure 4. Transient ophthalmic artery obstruction following intra-arterial chemotherapy for retinoblastoma in case 15. Macular retinoblastoma (A) with retinal detachment showed enhancement on fluorescein angiography (B) and good peripheral retinal perfusion. Following 1 cycle of intra-arterial chemotherapy, there was ophthalmic artery stenosis with poor retinal and choroidal perfusion clinically (C) and angiographically (D). Retinal perfusion improved to normal by 2 months’ follow-up and no further chemotherapy was delivered. Several benefits of IAC should be highlighted, including the localized chemotherapy injection, few necessary sessions (approximately 2 doses), 1-day delivery, and systemic tolerance. On the other hand, several concerns about IAC should be realized, including the potential for vascular injury or toxic effects, end-organ ischemia, and fluoroscopic-related radiation exposure. Following IAC, some mild and some severe shortterm effects should be anticipated. The mild short-term effects included eyelid edema, blepharoptosis, and orbital congestion, sometimes with temporary dysmotility. These findings were common and typically resolved within a few months, leaving minimal or no residua and without need for surgical repair. In 1 case of dysmotility, the features were consistent with transient oculomotor (third nerve) palsy. This finding has been previously observed in 3 of 7 patients (43%).20 The more serious short-term effects involved acute and chronic vascular insult, particularly to the ophthalmic, retinal, and choroidal vessels. Ophthalmic artery stenosis or obstruction manifested with pale optic nerve, reduced retinal blood flow, and patchy reduction in choroidal blood flow. In our series, occlusion or stenosis of the ophthalmic artery was observed in 4 cases, with reso- lution in 1 case by 1 month of follow-up. In 3 cases, the stenosis was confirmed under fluoroscopy at attempted catheterization for a repeated dose. No affected eyes developed neovascularization of the disc or retina, neovascular glaucoma, or pain or required enucleation for this finding. The specific pathogenesis of the vascular insult remains unknown, but it could be secondary to catheterrelated injury to the endothelium, chemotherapy toxic effects on the vessel or specifically the endothelium, or embolization from foreign body contamination or chemotherapy precipitation. There were no clinically visible emboli in any case. The prefluoroscopy and postfluoroscopy findings showed that the ophthalmic artery was patent at the time of IAC in all cases, suggesting a lack of catheter-related dissection, trauma, or embolism. The onset of ophthalmic and retinal arterial obstruction was often evident by the 1-month follow-up, whereas the choroidal vascular atrophy generally took several months to become apparent, showing slow progression. These findings might suggest chemotherapy toxic effects. This finding of ischemia has been previously recognized as a serious short-term risk of this therapy. Gobin et al noted that 4 of 46 eyes (9%) had “severe ocular com- ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1412 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. A B C D Figure 5. Nontransient ophthalmic artery obstruction following intra-arterial chemotherapy for retinoblastoma in case 6. Macular retinoblastoma (A) showed complete response following 1 cycle of intra-arterial chemotherapy (B). However, the intact nasal retina before treatment (C) showed broad choroidal atrophy at 1 year following treatment (D). plications which consisted of avascular retinopathies resulting in blindness.”12 We speculate that this finding could be overlooked in some cases, particularly if fluorescein angiography is not used. We perform fluorescein angiography at each session to confirm ocular blood flow. Occasionally, the retinal vessels appear intact clinically and the attenuation is detected only by fluorescein angiography. We encourage all centers using IAC to carefully study the ocular blood flow using fluorescein angiography. In comparison, our experience with intravenous chemoreduction in more than 500 children has revealed no similar incident of postchemotherapy ophthalmic, retinal, or choroidal ischemia. In contrast to the abrupt finding of ophthalmic or retinal vascular obstruction, the choroidal ischemic process manifested more slowly, with patchy focal areas of subtle RPE alterations that gradually evolved over several months into RPE atrophy, then choriocapillaris and occasionally large choroidal vessel atrophy. The features of choroidal atrophy were mild in most cases. It is recognized that the presence of serous retinal detachment or even a large tumor base could lead to chronic underlying RPE alterations, but in these cases, the RPE atrophy has been diffuse in previously uninvolved areas. The evolving sequence of diffuse, homogeneous choroidal atrophy might be suggestive of slow-onset involutional atrophy (Figure 3), perhaps from chemotherapy toxic effects more so than an acute embolic or traumatic event, which would more likely produce sector damage. Scrutiny of previously published articles reveals printed illustrations showing choroidal atrophy that was not recognized by the authors.15,21 We speculate that subtle cases could be overlooked and this finding could be much more common than anticipated. Furthermore, we have examined in consultation children who were treated with IAC at other centers in whom choroidal atrophy was unequivocally evident over time. This finding can be subtle and delayed over several months.22 Munier et al22 identified sector choroidal atrophy as a particular concern in 15% of cases. The implications of choroidal atrophy on ultimate visual acuity in children could be profound. However, it should be realized that most of these eyes would have otherwise been enucleated and had complete loss of vision. Intra-arterial chemotherapy has been used for other systemic malignant neoplasms, and the technique has been complicated by vascular toxic effects, similar to our experience with retinoblastoma. For example, Madaje- ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1413 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. wicz et al23 found IAC to be more beneficial for survival if delivered before rather than along with radiotherapy for glioblastoma multiforme. However, other trials showed contrasting findings.24,25 Grimson et al24 emphasized that IAC for brain malignant neoplasms could lead to dosedependent eye pain, vision loss, and encephalopathy, particularly if the injection into the internal carotid artery was below the take-off of the ophthalmic artery. Shapiro et al25 compared IAC vs intravenous chemotherapy in 448 patients with malignant glioma and showed reduced survival for the IAC group plus related toxic effects of encephalopathy (9.5%) and ipsilateral vision loss (15.5%). Fortunately, we have not witnessed any evidence of toxic effects in the brain in our patients during this 2-year period. For pediatric malignant neoplasms, IAC has been used for osteosarcoma. When used as a monotherapy, intraarterial infusion of cisplatin appeared to be more effective against osteosarcoma than intravenous infusion.26 However, other reports showed that intra-arterial superiority was diminished when multiagent therapy was needed.27,28 One report entitled “Intraarterial Chemotherapy for Osteosarcoma: Does the Result Really Justify the Effort?” by Bielack et al28 highlighted the risks of this procedure. They indicated that the risks and discomforts of IAC for osteosarcoma were considerable, intractable pain occurred in more than 50% of the infusions, and local complications of vasculopathic ischemic necrosis, thrombosis, infection, and neuropathy were found. With regard to retinoblastoma, a major concern is the potential for metastatic disease, especially if the eye shows features of high-risk retinoblastoma with tumor invasion into the choroid or postlaminar optic nerve. Often this is not clinically apparent and is found only on histopathologic examination following enucleation.29-32 In a comprehensive histopathologic analysis of nearly 300 eyes, high-risk features were found in 18.5% of cases, with retrolaminar optic nerve invasion in 10.4% and massive choroidal invasion in 8.1%.32 Eyes with high-risk features develop metastasis (leading to death) in 24%, unless intervention with systemic intravenous chemotherapy is delivered, reducing the metastatic rate to 4%.33 Intra-arterial chemotherapy is designed to selectively treat the eye and would likely be insufficient for remote subclinical metastatic disease. Over time, this could be a threat to the patient’s life prognosis. Fortunately, in our series, there was no evidence of metastatic retinoblastoma. However, we are aware of 3 cases of metastatic retinoblastoma from other centers using this technique. The technique of IAC requires fluoroscopy for accurate guidance of the catheter. The cumulative radiation exposure with potential risk for toxic effects has been explored by Vijayakrishnan et al.34 They found doses of 19 173 mrad to the affected eye, 3533 mrad to the contralateral eye, and 5560 mrad to the brain. Other sensitive organs like thyroid, bone marrow, and gonads received a small dose far below the minimal toxic level, but the dose to the lens was possibly cataractogenic. They cautioned that fluoroscopic use should be minimized to avoid radiation-related toxic effects in these patients. In summary, despite dramatic response of retinoblastoma to IAC,1,6,13-16 there is concern for toxic effects from both chemotherapy and radiotherapy exposure. With this in mind, we cautiously use IAC for retinoblastoma in selected cases. Submitted for Publication: January 6, 2011; final revision received April 5, 2011; accepted April 6, 2011. Published Online: June 13, 2011. doi:10.1001 /archophthalmol.2011.151 Correspondence: Carol L. Shields, MD, Ocular Oncology Service, Ste 1440, Wills Eye Institute, 840 Walnut St, Philadelphia, PA 19107 (carol.shields@shieldsoncology .com). Author Contributions: Dr C. L. Shields had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Financial Disclosure: None reported. Funding/Support: This study was supported by the Eye Tumor Research Foundation, Philadelphia, Pennsylvania (Drs C. L. Shields and J. A. Shields). Role of the Sponsor: The funder had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript. REFERENCES 1. Shields CL, Shields JA. Intra-arterial chemotherapy for retinoblastoma: the beginning of a long journey. Clin Experiment Ophthalmol. 2010;38(6):638-643. 2. Shields JA, Shields CL. Management of retinoblastoma. In: Shields JA, Shields CL, eds. Intraocular Tumors: An Atlas and Textbook. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:333-352. 3. Roarty JD, McLean IW, Zimmerman LE. Incidence of second neoplasms in patients with bilateral retinoblastoma. Ophthalmology. 1988;95(11):1583-1587. 4. Shields CL, Mashayekhi A, Cater J, Shelil A, Meadows AT, Shields JA. Chemoreduction for retinoblastoma: analysis of tumor control and risks for recurrence in 457 tumors. Am J Ophthalmol. 2004;138(3):329-337. 5. Shields CL, Shields JA, De Potter P, et al. Plaque radiotherapy in the management of retinoblastoma: use as a primary and secondary treatment. Ophthalmology. 1993;100(2):216-224. 6. Shields CL, Shields JA. Retinoblastoma management: advances in enucleation, intravenous chemoreduction, and intra-arterial chemotherapy. Curr Opin Ophthalmol. 2010;21(3):203-212. 7. Reese AB, Hyman GA, Tapley ND, Forrest AW. The treatment of retinoblastoma by x-ray and triethylene melamine. AMA Arch Ophthalmol. 1958;60(5):897906. 8. Kiribuchi M. Retrograde infusion of anti-cancer drugs to ophthalmic artery for intraocular malignant tumors [in Japanese]. Nippon Ganka Gakkai Zasshi. 1966; 70(11):1829-1833. 9. Yamane T, Kaneko A, Mohri M. The technique of ophthalmic arterial infusion therapy for patients with intraocular retinoblastoma. Int J Clin Oncol. 2004;9(2): 69-73. 10. Suzuki S, Kaneko A. Management of intraocular retinoblastoma and ocular prognosis. Int J Clin Oncol. 2004;9(1):1-6. 11. Gobin P, Abramson DA. A phase I/II study of intra-arterial (ophthalmic artery) chemotherapy for intraocular retinoblastoma [abstract 60]. J Vasc Interv Radiol. 2008;19(2)(suppl):s24-s25. doi:10.1016/j.jvir.2007.12.067. 12. Gobin P, Marr B, Dunkel I, Brodie S, Abramson D. Intra-arterial chemotherapy (chemosurgery) in the ophthalmic artery for the treatment of retinoblastoma in children: 3 year experience. J Neurointerv Surg. 2009;1(1):77-78. doi:10.1136 /jnis.2009.000851n. 13. Abramson DH, Dunkel IJ, Brodie SE, Kim JW, Gobin YP. A phase I/II study of direct intraarterial (ophthalmic artery) chemotherapy with melphalan for intraocular retinoblastoma initial results. Ophthalmology. 2008;115(8):1398-1404. 14. Abramson DH. Super selective ophthalmic artery delivery of chemotherapy for intraocular retinoblastoma: ‘chemosurgery’ the first Stallard lecture. Br J Ophthalmol. 2010;94(4):396-399. 15. Abramson DH, Dunkel IJ, Brodie SE, Marr B, Gobin YP. Superselective ophthal- ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1414 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved. 16. 17. 18. 19. 20. 21. 22. 23. 24. mic artery chemotherapy as primary treatment for retinoblastoma (chemosurgery). Ophthalmology. 2010;117(8):1623-1629. Shields CL, Bianciotto CG, Jabbour P, et al. Intra-arterial chemotherapy for retinoblastoma: report No. 1, control of retinal tumors, subretinal seeds, and vitreous seeds[publishedonlineJune13,2011].ArchOphthalmol.doi:10.1001/archophthalmol . 2011.150. Shields CL, Ramasubramanian A, Rosenwasser R, Shields JA. Superselective catheterization of the ophthalmic artery for intraarterial chemotherapy for retinoblastoma. Retina. 2009;29(8):1207-1209. Inomata M, Kaneko A. Chemosensitivity profiles of primary and cultured human retinoblastoma cells in a human tumor clonogenic assay. Jpn J Cancer Res. 1987; 78(8):858-868. Mathews J, Goel R, Evans WK, Shamji F, Stewart DJ. Arterial occlusion in patients with peripheral vascular disease treated with platinum-based regimens for lung cancer. Cancer Chemother Pharmacol. 1997;40(1):19-22. Smith V, Kingston JE, Hungerford JL, et al. Complications of direct intraophthalmic artery melphalan treatment for refractory retinoblastoma. Paper presented at: American Academy of Ophthalmology 2010 Joint Meeting; October 17, 2010; Chicago, IL. Abramson DH, Dunkel IJ, Brodie SE, Marr B, Gobin YP. Bilateral superselective ophthalmic artery chemotherapy for bilateral retinoblastoma: tandem therapy. Arch Ophthalmol. 2010;128(3):370-372. Munier FL, Beck-Popovic M, Balmer A, Gaillard MC, Bovey E, Binaghi S. Occurrence of sectoral choroidal occlusive vasculopathy and retinal arteriolar embolization after superselective ophthalmic artery chemotherapy for advanced intraocular retinoblastoma. Retina. 2011;31(3):566-573. Madajewicz S, Chowhan N, Tfayli A, et al. Therapy for patients with high grade astrocytoma using intraarterial chemotherapy and radiation therapy. Cancer. 2000; 88(10):2350-2356. Grimson BS, Mahaley MS Jr, Dubey HD, Dudka L. Ophthalmic and central ner- 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. vous system complications following intracarotid BCNU (carmustine). J Clin Neuroophthalmol. 1981;1(4):261-264. Shapiro WR, Green SB, Burger PC, et al. A randomized comparison of intraarterial vs intravenous BCNU, with or without intravenous 5-fluorouracil, for newly diagnosed patients with malignant glioma. J Neurosurg. 1992;76(5):772-781. Jaffe N, Prudich J, Knapp J, et al. Treatment of primary osteosarcoma with intra-arterial and intravenous high-dose methotrexate. J Clin Oncol. 1983;1(7):428-431. Winkler K, Bielack S, Delling G, et al. Effect of intraarterial vs intravenous cisplatin in addition to systemic doxorubicin, high-dose methotrexate, and ifosfamide on histologic tumor response in osteosarcoma (study COSS-86). Cancer. 1990;66(8):1703-1710. Bielack SS, Bieling P, Erttmann R, Winkler K. Intraarterial chemotherapy for osteosarcoma: does the result really justify the effort? In: Humphrey CB, ed. Osteosarcoma in Adolescent and Young Adults. Boston, MA: Kluwer Academic Publishers; 1993:85-92. Magramm I, Abramson DH, Ellsworth RM. Optic nerve involvement in retinoblastoma. Ophthalmology. 1989;96(2):217-222. Shields CL, Shields JA, Baez K, Cater JR, De Potter P. Optic nerve invasion of retinoblastoma: metastatic potential and clinical risk factors. Cancer. 1994; 73(3):692-698. Shields CL, Shields JA, Baez KA, Cater J, De Potter PV. Choroidal invasion of retinoblastoma: metastatic potential and clinical risk factors. Br J Ophthalmol. 1993;77(9):544-548. Eagle RC Jr. High-risk features and tumor differentiation in retinoblastoma: a retrospective histopathologic study. Arch Pathol Lab Med. 2009;133(8):1203-1209. Honavar SG, Singh AD, Shields CL, et al. Postenucleation adjuvant therapy in high-risk retinoblastoma. Arch Ophthalmol. 2002;120(7):923-931. Vijayakrishnan R, Shields CL, Ramasubramanian A, Emrich J, Rosenwasser R, Shields JA. Irradiation toxic effects during intra-arterial chemotherapy for retinoblastoma: should we be concerned? Arch Ophthalmol. 2010;128(11):1427-1431. Visit www.archophthalmol.com. As an individual subscriber you can search the full text of Archives of Ophthalmology or all 10 JAMA & Archives Journals. Advanced Search enables you to search by citation, title, author, keywords, and date ranges. You can search by journal or by topic collection. Finally, you can choose to search only tables and figures. ARCH OPHTHALMOL / VOL 129 (NO. 11), NOV 2011 1415 WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at , on December 1, 2011 ©2011 American Medical Association. All rights reserved.