Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
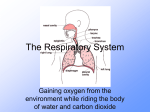
221 CARDIOPULMONARY ANATOMY AND PHYSIOLOGY Chapter 1 Main function of lungs – bring atmospheric gases into contact with the blood Ventilation – The process of moving gas in and out of the lungs Respiration – moving oxygen and carbon dioxide between air and blood Upper Airways Most important function warms humidifies filters Consists of nose oral cavity (mouth) pharynx (throat) larynx (“voice box”) inspired gas (air) 1. Nose Air conditioning and filtering device Nose is more resistant to airflow than mouth Despite that resistance: Most adults breathe through the nose at times of rest ***High nasal resistance from swollen mucous and rapid breathing from exercise usually cause people to switch to mouth breathing. NASAL CAVITY Septum Cartilage – Divides nose Right and Left Nostril Clinically = Right and Left NASAL FOSSAE Some deflection occurs slightly to the left Clinical Significance ___________________ Difficulty breathing through nose? Deviated Septum? (Next Slide) Nasal Cavity - Anatomical Structures CONCHAE Three Conchae bones Superior, Middle, Inferior Create Turbulence AKA Turbinates Conchae – covered with mucous membranes Main purpose is to filter, humidification, heat inhaled air Nasal Fossae Source: mayoclinic.com/health/medical/IM02743 3. Pharynx Greek – “throat” Comprised of 3 landmarks Where the Nasal Cavity ends all the way down right before the Larynx and Trachea- Fig 1-1 page 3 1. Nasopharynx -behind nasal cavity down to soft palate 2. Oropharynx -behind oral cavity from soft palate to base of tongue 3. Laryngopharynx aka Hypopharynx - below base of tongue and above larynx By the time air reaches the nasopharynx, inspired air gains water vapor and heat from the nose and humidification Concept Question 1-1, pg. 5 Answer: Nasal Cannula: At what flow rate does the nose lose its ability to humidify oxygen? Recommendation: Ventilator Artificial Nose – or HME Drawback If – thick secretions - Back to the Pharynx NASOPHARYNX- pg 5 Connected to the middle ear by the Eustachian Tubes aka _______________ AUDITORY TUBES Eustachian Tube Ear Drum Outer Inner Middle Middle Ear = Space behind ear drum Pharynx (cont) pg 6 The laryngopharynx (hypopharynx) separates the Esophagus and Trachea. (digestive &respiratory tracts) Sensory & motor nerves effect on pharyngeal muscles prevents food and liquid aspiration in the trachea PHARYNGEAL REFLEX Stimulation of this nerve = Gag & Swallow Deeply unconscious patients may lose gag reflex Aspiration risks increase Intubation and mechanical ventilation is necessary Pharyngeal Muscle Tone pg 6 Loss in muscle tone Base of tongue may fall back and occlude the laryngopharynx Snoring Excessive occlusion/blockage = apnea • Apnea = No air movement… No breathing Intubation Often done in patients who need support in ventilation Endotrachael Tube is inserted into the trachea (Nasally, Orally, Tracheostomy) Pharynx C – Sniffing position. Pulls the tongue forward out of the way of the airway. Best for intubation Fig. 1-5 Pharynx 4. LARYNX •Sometimes called the “VOICEBOX” •Vocal cords control the size of the opening of the trachea (glottis) •Main Cartilage of the Larynx (the middle of neck) is the Thyroid Cartilage, aka “ADAM’S APPLE” • Function – Speech and __________________ Epiglottis – Flap Larynx – aka Voice Box Cartilage beneath it – Thyroid Cartilage “Adam’s Apple At the opening of the Larynx Epiglottis The epiglottis does not “seal” the airway, instead, the upward movement of the larynx toward the base of the tongue pushes the epiglottis down, diverting food away from the glottis. Left – No breathing or swallowing Right – Swallow is initiated. Larynx moves up…. Forces the epiglottis to bend down Left – Epiglottis bends downward… Redirects from the the larynx and trachea… Doesn’t seal it… just diverts food to the esophagus Right – Food passes to Esophagus Left – After a complete swallow, the Epiglottis starts lifting up again Right – Epiglottis continues to lift up now as the patient begins to exhales Left – as exhalation continues to the oropharynx, epiglottis is now nearly shut Right – As the air flows out the mouth, epiglottis is completely shut Epiglottitis Life Threatening Drooling/Difficulty Swallowing/Breathing Intubation INTUBATION VISUAL Thyroid and Cricoid Thyroid is what we refer to as the Adams Apple… It encloses the main cavity of the Larynx Fig. 1-6 Cricoid Narrowest portion of the upper airway in the infant Not the narrowest in the adult, however passing Endotracheal through may still be difficult Vocal Cords Form triangular opening into trachea narrowest part of adult larynx Can open and close when closed allows pressure generation needed to cough • Cough = important defense mechanism for lung artificial airway removes vocal cords’ ability to seal airway and cough effectively Vocal cord edema (croup - Pediatrics; stridor - ETT) Laryngospasm during extubation - hoarseness Upper Airway Summary The nose alters inspired air by: A. Humidifying, cooling, and reducing flow velocity B. Cooling, filtering, and humidifying C. Humidifying, filtering, and warming D. Warming, reducing flow velocity, and filtering Upper Airway Summary The ________ is referred to as the voicebox A. Pharynx B. Larynx C. Trachea D. Cricoid Upper Airway Summary The Adam’s Apple is the name given to the: A. Thyroid B. Larynx C. Trachea D. Cricoid Airways Vs. Alveoli Lower Airways pg 10 Dichotomous branching pattern from trachea Each airway divides into two smaller airways (See next slide) Each bifurcation creates new generation of airways Tracheobronchial “tree” Figure 1-8 Lower Airways Also referred to as: Conducting Airways No gas exchange takes place This are can be obstructed with secretions and mucus This is part one of the lung… the other part is the parenchyma where the alveoli and tissues exist. Fig. 1-8 Trachea and Main Bronchi Trachea 8-20 C-shaped cartilages Begins at 6th cervical vertbra 11 cm long in adults 1.5-2.5 cm in diameter Carina – point of division fig-1-8 bifurcation of trachea into right and left bronchi right bronchus at 20-30 degrees from midline left bronchus at 45-55 degrees from midline • smaller in diameter, but twice as long air is 100% saturated and at 37o C at this point • ISB (Isothermic Saturation Boundary… See Fig. 1-10) Application During intubation, if the Tube is pushed too far, it most likely will enter the ____________________________ Chest Auscultation Chest Excursion Carina Conducting Airways No gas exchange takes place This area can be obstructed with secretions and mucus Lung parenchyma where the alveoli and tissues exist is where gas exchange starts Conducting Airway Anatomy Conduit or passage or pathway Airways: trachea to just before alveolar level: no gas exchange conduit for air to reach alveoli 23-27 subdivisions beginning at trachea Right and left mainstem bronchi position patients during PD&P. Fig. 1-12 Problem with airway disease Obstruction Airflow resistance Lung Parenchyma ACINUS (pg 14) Functional tissue of the lung Contains elastic fibers surrounds airways Gas Exchange takes place Elastic fibers can be destroyed by disease Emphysema Prevents air from escaping the lung during exhalation • “Air Trapping” The Acinus THE ACINUS IS THE FUNCTIONAL RESPIRATORY UNIT OF THE LUNGS. Fig. 1-13 ( ALL ALVEOLI ARE CONTAINED IN THE ACINUS) EACH TERMINAL BRONCHIOLE GIVES RISE TO AN ACINUS. Alveoli and Capillaries (Alveoli-Capillary Membrane) Alveoli 300 million (300 x 106) alveoli in adult lungs 100 to 300 microns (m) in diameter Pulmonary capillaries in contact with alveolar membrane just large enough to allow passage of red blood cells facilitate gas exchange Alveoli and Capillaries Fig. 1-17 Problem with Alveolar Disease Compliance Elastance Restriction- where volume is restricted Alveolar Disease Alveolar Collapse Atelectasis ?? Clinical focus 1-5 Resistance Compliance Elastance Airflow Obstruction Distending Properties Recoiling Properties Summary Patients requiring a tracheostomy would benefit most from: A. High airflows provided to the trachea B. Dehumidified air provided to the airway C. Cool mist for adequate hydration D. Heated, humidified inspired air CPR is often done outside the hospital setting. An important technique in ventilating the patient involves tilting the victim’s head back and thrusting the jaw forward. This is done to allow: A. Better blood flow to the head B. Air forced into the mouth easier passage to the lungs C. Easier mouth alignment D. Reducing the chance of damage to the upper airways Certain lung diseases impair the A-C membrane’s gas-diffusing capabilities. An important consequence of this would be: A. A decrease in blood oxygen levels B. A decrease in blood carbon dioxide levels C. An increase in blood oxygen levels D. An increase in blood oxygen levels and carbon dioxide levels