Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
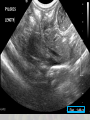
Hypertrophic Pyloric Stenosis – Familial and Genetic Correlates Cordelie Witt 7/17/14 Cases • 4 week old male monozygotic twins born at 35-4/7 weeks via planned C-section • Both twins simultaneously evaluated at OSH; workup diagnosed hypertrophic pyloric stenosis • Transferred to Seattle Children’s Hospital for management Cases • Twin A: 2.87 kg. 2 days nonbloody, nonbilious projectile emesis with every feed – No other medical problems, good weight gain since birth. No known family history of pyloric stenosis – Bottle fed; using soy-based formula – Palpable epigastric mass – Na 143, K 4.6, Cl 104, CO2 26, glucose 63 – US: 3.77 mm wall thickness, channel length 15 mm Cases • Twin B: 2.51 kg. 4 days nonbloody, nonbilious projectile emesis with almost all feeds – h/o periodic desaturations and apnea in the first 2 weeks of life, poor weight gain since birth – Na 143, K 3.9, Cl 102, CO2 28, glucose 41 (corrected to 96 preop) – Palpable epigastric mass – US: 4.51 mm wall thickness, channel length 14.9 mm Cases • Twins were taken to the operating room sequentially; each underwent: – Suctioning – Rapid sequence intubation – Ramstedt pyloromyotomy • Twin A: 23 mm pyloromyotomy • Twin B: 21 mm pyloromyotomy • Both did well postoperatively and were discharged home on POD1 Risk factors for pyloric stenosis • • • • • • • • • • • Male > female; 4-5x Caucasian Family history of pyloric stenosis Multiples First-born child Younger maternal age Genetic syndromes Bottle feeding Macrolide antibiotic exposure (erythromycin) ?Prostaglandin exposure ?Acid exposure Risk factors for pyloric stenosis • • • • • • • • • • • Male > female; 4-5x Caucasian Family history of pyloric stenosis Multiples First-born child Younger maternal age Genetic syndromes Bottle feeding Macrolide antibiotic exposure (erythromycin) ?Prostaglandin exposure ?Acid exposure Familial pyloric stenosis • Familial aggregation described since 1934 (Cockayne) • Multitude of case studies of both monozygotic and dizygotic twins with pyloric stenosis – Gezer et al (Clinical Genetics 2014) – monozygotic male twins , presented at age 4.5 and 5 weeks – Kundal et al (BMJ 2013) – dizygotic male twins, presented at day of life 45 – Yang et al (Pediatric Child Health 2008) – 3 sets of dizygotic twins, one set of monozygotic twins. Monozygotic twins were female; one dizygotic twin was female. Presented between 3.5 and 8 weeks of life – Sheldon (1938) – 23 pairs of twins amongst 1000 cases of pyloric stenosis – Many more! Familial Aggregation and Heritability of Pyloric Stenosis Krough et al, JAMA 2010 • Cohort study of all children born in Denmark between 1977 and 2008 – Civil Registration System, Danish Family Relations Database, and Danish National Patient Registry (all hospital discharge diagnoses and operations) – Followed for first year of life – Cohort size: 1,999,738 (1,948,616 person-years) – 3362 children had surgery for pyloric stenosis • Overall rate 1.7 /thousand person-years • Rate in singletons: 1.8 /thousand person-years • Rate in twins: 3.1 /thousand person-years – 81.5% of patients with pyloric stenosis were male Familial Aggregation and Heritability of Pyloric Stenosis • Rate ratios Krough et al, JAMA 2010 – Monozygotic twins: 182 • 46% of children with an affected monozygotic twin developed pyloric stenosis! – – – – – Dizygotic twins: 29.4 Siblings: 18.5 Half-siblings: 4.99 Cousins: 3.06 Half-cousins: 1.60 • Rate ratios were NOT affected by sex • Heritability: 87% PS - heritability theories • Carter ( 1961 and 1969) and Falconer (1965): polygenic inheritance with a threshold effect – Sex-modified risk PS - heritability theories • Single Major Locus model – Kidd and Spence, 1976 – Single heritable gene, modified by environmental factors Identifying genetic loci • Common Variants near MBNL1 and NKX2-5 are Associated with Infantile Hypertrophic Pyloric Stenosis (Feenstra et al, Nature Genetics, June 2013) – Genome-Wide Association Study – 1001 surgery-confirmed cases, 2401 controls from Denmark • All cases were surgery-confirmed, singletons, and without major congenital malformations – Identified 3 SNPs that reached significance • rs11712066, near MBNL1 (chromosome 2) • rs573872, near MBNL1 • rs29784, near NKX2-5 (chromosome 5) – The 3 SNPs showed no heterogeneity of effects between sexes • Study findings supported by replication analysis on an additional 796 cases and 876 controls by Everett and Chung Genetic loci • MBNL1: encodes “musclebind” proteins; these proteins regulate alternative splicing in early postnatal period; involved in muscle tissue remodeling • NKX2-5: encodes homeobox transcription factor involved in cardiac formation and development and embryonic gut development including pyloric sphincter muscle tissue – Chicken and mice: Nkx2-5 expression occurs in a ring of mesenchyme at the foregut-midgut junction during development – Suppression of Nkx2-5 activity in pyloric sphincter results in loss of the sphincter endodermal phenotype – Ectopic expression of Nkx2-5 pyloric sphincter-like structure in chicken gizzard More genetic loci • Genome-wide linkage analysis in families with infantile hypertrophic pyloric stenosis indicates novel susceptibility loci (Svenningsson et al, Journal of Human Genetics, December 2011) – Genome-wide linkage analysis in 37 Swedish families with 2-5 affected individuals each; total 94 affected and 184 total • Added 31 British families where linkage favored – Genotyping and linkage analysis • 2q24, 7p22 were significant; 6p21 and 12q24 were suggestive Candidate genes identified • GLP-2 (2q24) – GI hormone, stimulates epithelial cell proliferation, inhibits apoptosis, regulates motility • NPY (7p22) – inhibitory effect on smooth muscle cells • NOS1 (12q24) – smooth muscle relaxation • MLN (12q24) – encodes motilin, which induces GI contraction. (*erythromycin is a motilin agonist) Nitric Oxide • Chung et al (American Journal of Human Genetics, Feb 1996) studied 27 families (21 had at least 3 affected individuals). There were 229 individuals total; 87 had pyloric stenosis. – Analyzed 2 NOS1 polymorphisms; found significant transmission disequilibrium between one allele (NOS1a) and PS • Serra et al (Journal of Pediatric Surgery, May 2011) investigated NOS1 sequence variations in a case control study of 43 patients and 47 controls; 19 polymorphisms were found but none were significantly associated Nitric oxide • NOS1 gene (12q24) encodes neuronal nitric oxide synthase; NO contributes to smooth muscle relaxation – NOS1 gene expression reduced in pyloric stenosis muscle tissue – NOS1 knockout mouse model: pyloric stenosis-like phenotype with distended stomach, thickened pylorus Other identified sites • Other studies have identified additional candidate sites, including: 16p12-p13, 11q14-q22, Xq23, 16q24… • There are also a multitude of studies investigating environmental factors associated with hypertrophic pyloric stenosis Conclusions • Pyloric stenosis is highly, but not completely, heritable • A multitude of studies suggests a strong genetic basis for hypertrophic pyloric stenosis; however, inheritance appears polygenic and may be heterogeneous across different populations. It also appears to be influenced or triggered by multiple environmental factors References • • • • • • • • • • • • Gezer HO, Oguzkurt P, Temiz A, Hicsonmez A. Hypertrophic pyloric stenosis in twins; genetic or environmental factors. Clin Genet. 2014 Apr 12. doi: 10.1111/cge.12399. [Epub ahead of print] PubMed PMID: 24724922. Kundal VK, Gajdhar M, Shukla AK, Kundal R. Infantile hypertrophic pyloric stenosis in twins. BMJ Case Rep. 2013 Apr 9;2013. pii: bcr2013008779. doi: 10.1136/bcr-2013-008779. PubMed PMID: 23576655. Yang G, Brisseau G, Yanchar NL. Infantile hypertrophic pyloric stenosis: An association in twins? Paediatr Child Health. 2008 May;13(5):383-5. PubMed PMID: 19412365; PubMed Central PMCID: PMC2532891. Krogh C, Fischer TK, Skotte L, Biggar RJ, Øyen N, Skytthe A, Goertz S, Christensen K, Wohlfahrt J, Melbye M. Familial aggregation and heritability of pyloric stenosis. JAMA. 2010 Jun 16;303(23):2393-9. doi: 10.1001/jama.2010.784. PubMed PMID: 20551410. Carter CO, Evans KA. Inheritance of congenital pyloric stenosis. J Med Genet. 1969 Sep;6(3):233-54. PubMed PMID: 5345095; PubMed Central PMCID: PMC1468738. Falconer DS. The inheritance of liability to certain diseases, estimated from the incidence among relatives. Ann Hum Genet. 1965;29(51):51-76. Kidd KK, Spence MA. Genetic analyses of pyloric stenosis suggesting a specific maternal effect. J Med Genet. 1976 Aug;13(4):290-4. PubMed PMID: 986474; PubMed Central PMCID: PMC1013418. Feenstra B, Geller F, Krogh C, Hollegaard MV, Gørtz S, Boyd HA, Murray JC, Hougaard DM, Melbye M. Common variants near MBNL1 and NKX2-5 are associated with infantile hypertrophic pyloric stenosis. Nat Genet. 2012 Feb 5;44(3):334-7. doi: 10.1038/ng.1067. PubMed PMID: 22306654; PubMed Central PMCID: PMC3693399. Everett KV, Chung EM. Confirmation of two novel loci for infantile hypertrophic pyloric stenosis on chromosomes 3 and 5. J Hum Genet. 2013 Apr;58(4):236-7. doi: 10.1038/jhg.2013.10. Epub 2013 Feb 21. PubMed PMID: 23426030. Svenningsson A, Söderhäll C, Persson S, Lundberg F, Luthman H, Chung E, Gardiner M, Kockum I, Nordenskjöld A. Genome-wide linkage analysis in families with infantile hypertrophic pyloric stenosis indicates novel susceptibility loci. J Hum Genet. 2012 Feb;57(2):115-21. doi: 10.1038/jhg.2011.137. Epub 2011 Dec 8. PubMed PMID: 22158425. Chung E, Curtis D, Chen G, Marsden PA, Twells R, Xu W, Gardiner M. Genetic evidence for the neuronal nitric oxide synthase gene (NOS1) as a susceptibility locus for infantile pyloric stenosis. Am J Hum Genet. 1996 Feb;58(2):363-70. PubMed PMID: 8571963; PubMed Central PMCID: PMC1914525. Serra A, Schuchardt K, Genuneit J, Leriche C, Fitze G. Genomic variants in the coding region of neuronal nitric oxide synthase (NOS1) in infantile hypertrophic pyloric stenosis. J Pediatr Surg. 2011 Oct;46(10):1903-8. doi: 10.1016/j.jpedsurg.2011.05.021. PubMed PMID: 22008325. Thank you!