Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
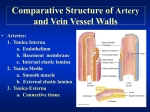
Ch. 20: Blood Vessels and Circulation I. General Vessel Anatomy (A) Circulatory Routes: Heart-> arteries -> arterioles-> capillaries -> venules-> veins-> heart. Deviations: -1- portal systems – capillary to capillary. Between the hypothalamus and anterior pituitary, between intestines and liver (hepatic portal). -2- anastomoses – merging of vessels. Arteriovenous (shunts); arterial (collateral routes); venous (alternative drainage routes). (B) Vessel Walls -1- tunica externa/ advetitia: loose CT, contains vasa vasorum. -2- tunica media: usually thickest. Smooth muscle, collagen. Vasoconstriction vs. vasodilation. -3- tunica interna/ intima: endothelium- simple squamous ET. (C) Arteries and Metarterioles relatively thick muscular walls -1- conducting (elastic) arteries: largest. -2- distributing (muscular) arteries -3- resistance (small) arteries: don’t have names. Smallest ones are arterioles: constrict and dilate. -4- metarterioles: link arterioles to capillaries, separated by pre-capillary sphincter. (D) Capillaries – exchange vessels. Walls only with endothelium and basement membranes. -1- capillary beds – metarteriole becomes a thoroughfare channel in middle. Fill when pre-capillary sphincter open. ~75% closed at any given time. -2- types: a. continuous = most. b. fenestrated: holes in endothelium. In kidneys, choroid plexus. Sinusoids = irregular spaces, not vessels. In liver, marrow, spleen. (E) Veins – receive tributaries. Venules exchange some fluid. Venous sinuses with no smooth muscle, e.g. coronary sinus. Very low BP. Thin walls, less muscle and elastic tissue. Valves prevent backflow. Varicose veins, hemorrhoids in anal canal- distended due to pressure. 15 II. Blood Pressure, Resistance and Flow Perfusion = flow/ volume/ time. ml/ min/ g. Hemodynamics: physical properties of blood flow. Based on pressure and resistance. Flow is related to the difference in pressure divided by resistance. (A) Blood Pressure – ranges between systolic and diastolic. Normal ~ 120/ 75 mmHg. The difference between the two is pulse pressure, indicates stress on small arteries, as does MAP = mean arterial pressure (closer to diastolic than the average). Greater than 140/ 90 = hypertension. Creates risk for aneurysm. Rises with age. Hypotension – too low. (B) Resistance – peripheral (in blood vessels). Dependent upon: -1- blood viscosity. -2- vessel length. -3- vessel radius. Affected by vasomotion (dilation and constriction). A very powerful effect. (C) Regulation of BP and Flow -1- local control = autoregulation. Hypoxia, increasing CO2, H+, lactic acid, lead to vasodilation. Platelets release vasoactive chemicals. Ischemia leads to reactive hyperemia. Long-term hypoxia -> angiogenesis. -2- neural control: vasomotor center of medulla. Sympathetic responsevasodilation in skeletal and cardiac muscle. Coordinates baroreflexes and chemoreflexes (pH, O2, CO2). Receptors in aorta and carotid arteries. Medullary ischemic reflex responds to decreased brain perfusion. -3- hormonal control: a. angiotensin II: causes vasoconstriction. Created by ACE (angiotensinconverting enzyme). ACE inhibitors treat hypertension. b. aldosterone: increases Na+ retention. c. ANP: decreases Na+ retention. d. ADH (vasopressin): increases water retention. May cause vasoconstriction. e. epinephrine and norepinephrine: cause vasoconstriction. (D) Vasomotion & Routing of Blood Flow Vasoconstriction in one area directs blood to other areas. 16 III. Capillary Exchange Through endothelial intercellular clefts, fenestrations (when present), endothelial cell cytoplasm. (A) Diffusion – most important. Glucose, O2, CO2, wastes. (B) Transcytosis – via pinocytosis, then exocytosis. Fatty acids, albumin, come hormones (insulin). (C) Filtration & Reabsorption – filtration from arterial capillaries; reabsorption into venous capillaries. Opposite forces= hydrostatic pressure and COP (colloid osmotic pressure). (D) Edema – fluid retention, caused by: -1- increased capillary filtration: due to increased BP or permeability. -2- decreased caplllary reabsorption: due to low blood albumin. -3- obstructed lymphatic drainage. IV. Venous Return & Circulatory Shock (A) Mechanisms of Venous Return -1- pressure gradient, based on pressure generated by heart. -2- gravity – works for upper body. -3- skeletal muscle pump. -4- thoracic (respiratory) pump. -5- cardiac suction – when atria expand during ventricular systole. (B) Venous Return and Physical Activity Enhanced by increased CO2 and BP. Lack of exercise leads to venous pooling. Can cause syncope (dizziness). (C) Circulatory Shock -1- cardiogenic shock, due to diminished pumping (MI). -2- low venous return (LVR) shock. a. hypovolumic most common, blood loss or dehydration. b. obstructed venous return – due to tumor, aneurysm. c. venous pooling (vascular) shock. May be neurogenic, loss of vasomotor tone. Septic shock from bacterial toxins; anaphylactic shock from severe allergies. 17 responses: compensated lead to recovery; decompensated lead to positive feedback and death. V. Special Circulatory Routes (A) Brain: very little fluctuation in cerebral perfusion. Local control important, mostly via pH. Brief cerebral ischemia = TIAs. When infarction (tissue death) = CVA = stroke. (B) Skeletal Muscle: perfusion highly variable. Contraction compresses blood vessels. (C) Lungs: pulmonary circulation with lower pressure. Slows blood down for gas exchange, makes capillaries more absorptive. When pulmonary pressure increases, edema in lungs. VI. Blood Vessel Anatomy Study from Figures 20.20: Arteries; 20.32: Veins. 18