Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
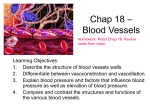
Chapter 18: The Cardiovascular system: Blood Vessels Objectives: 1. Describe the three layers that typically form the wall of a blood vessel, and state the function of each. 2. Define vasoconstriction and vasodilation. 3. Compare and contrast the structure and function of the three types of arteries. 4. Describe the structure and functions of veins, and explain how veins differ from arteries. 5. Describe the structure and function of a capillary bed. 6. Define blood flow, blood pressure, and resistance, and explain the relationship between these factors. 7. List and explain the factors that influence blood pressure, and describe how blood pressure is regulated. 8. Define hypertension. Describe both its symptoms and consequences. 9. Explain how blood flow is regulated in the body in general and in its specific organs. 10. Outline the factors involved in capillary dynamics, and explain the significance of each. 11. Define circulatory shock. List several possible causes. 12. Provide examples of changes that often occur in blood vessels as a person ages. Layers of blood vessels See figure 18.1 1. Lumen: the empty space inside the blood vessel 2. Tunica interna: innermost layer of endothelium, made of simple squamous epithelium (slick) 3. Tunica media: middle layer of circular smooth muscle and sheets of elastin. Innervated by vasomotor nerve fibers of sympathetic division of ANS. 4. Tunica externa (adventitia): collagen fibers with nerve fibers, lymph vessels, some elastin, and blood vessels. Vasoconstriction: contraction of smooth muscle to decrease diameter of lumen Vasodilation: relaxation of smooth muscle layer to increase diameter of lumen Types of Blood Vessels: See Table 18.1, figure 18.2 Arteries: carry blood away from heart 1. Elastic: thick walled near heart (aorta & branches). Largest in diameter and most elastic. Large lumen gives low-resistance (conducting arteries). If arteriosclerotic (hard), they may balloon out into aneurysms. 2. Muscular or distributing: deliver blood to specific body organs. Have thickest tunica media layer, active in vasoconstriction. 3. Arterioles: smallest artery, narrow down to single layer of smooth muscle. Controls blood flow into capillaries through response to neural and chemical influence. Constriction of arterioles bypasses tissues served, dilation floods tissues served. Capillaries: smallest vessels w/ just thin tunica interna. Just large enough for RBC’s to slip through single file. Designed for exchange of materials (gases, nutrients, wastes) between blood and interstitial fluid. See figure 18.3 1. Continuous: most common, found in skin and muscles, uninterrupted lining 2. Fenestrated: have pores covered by a membrane, for active absorption or filtration (small intestine, kidneys) 3. Sinusoid: leaky capillaries to allow large molecules and blood cells to pass, as in liver, bone marrow, lymphoid tissue and some endocrine glands. Blood flows sluggishly to provide time for modification (nutrients into liver, bacteria destroyed and removed) 4. Capillary beds: interweaving networks with shunts. See figure 18.4 Venules: post capillary venules are extremely porous for fluid and WBC’s to leave blood stream (as in inflammation). Large venules have thin tunica media and externa. Veins: walls are thinner and lumen larger, but they do possess all three tunics as in arteries. Tunica media contains little smooth muscle and externa is thickest. 65% of blood in body is found in veins at any one time (blood reservoir). Venous valves prevent backflow of blood and are formed from folds of tunica interna (similar to semilunar valves). Most valves in veins of limbs. 1.Varicose: tortuous (twisty) and dilated due to incompetent valves; gravity and pressure affect them. Varicose veins in anus are hemorrhoids. 2. Anastomoses: connect vein to vein, artery to artery or artery to vein Physiology of Circulation 1. Blood flow: actual volume flowing through a vessel, organ, or circulation in time (ml/min) = Cardiac output. 2. Blood pressure: force/unit area exerted on wall of blood vessel (mmHg). Systemic arterial pressure greatest in largest arteries near heart. The differences in blood pressure keep blood moving. 3. Resistance: opposition to flow, measure of amount of friction; peripheral resistance (PR) a. Blood viscosity: internal resistance to flow due to thickness or stickiness of fluid. viscosity, resistance, blood pressure b. Total blood vessel length: the longer the length of vessel, the greater the resistance, (an extra lb or 2 of fat requires miles of small vessels to serve it) c. Blood vessel diameter: fluid close to the wall is slowed by friction. The blood in the center flows freely. Resistance = 1/r4 Systemic blood pressure: greatest pressure near pump, this generates blood flow and pressure results when flow is opposed by resistance. See figure 18.5 Arterial blood pressure: 1. How much elastic arteries close to heart can be stretched (compliance or distensibility) 2. Volume of blood forced into arteries at any time. It is pulsatile. Systolic pressure = 120 mmHg, Diastolic pressure = 70-80 mmHg. The difference is pulse pressure. Mean arterial pressure (MAP): it is the pressure that propels the blood to the tissues throughout the cardiac cycle. MAP = diastolic pressure + pulse pressure (sys-dia) 3 120/80 pressure = 93 mmHg MAP Capillary blood pressure: 40 mmHg by the time it reaches the capillaries and 20 mmHg by the time it leaves but 1. capillaries are fragile and 2. permeable and force filtrate or nutrients out of blood to interstitial space. Venous blood pressure: steady and changes little. No measurable BP in vena cava. Venous return See figure 18.6 1. Respiratory pump: pressure changes in ventral body cavity during breathing pushes blood up toward heart. 2. Muscular pump: skeletal muscle activity, along w/ valves keep venous blood moving in one direction toward heart. Maintaining blood pressure: BP = CO x PR (and blood volume) See figure 18.7 Main factors affecting CO = venous return (for stroke volume) and neural/hormonal control (for HR). Parasympathetic cardioinhibitory center (through vagus nerve) is in charge of the resting heart rate. During this time, SV is controlled by EDV (by venous return). During stress, heart rate increases, SV increases due to contractility (and therefore, ESV) and therefore CO and MAP Short-term neural controls of peripheral resistance Alter blood distribution to tissues in response to demands (ex. shunt blood away from GI tract during sympathetic stimulation) Maintain MAP by altering blood vessel diameter (through vasoconstriction and vasodilation) Vasomotor center: found in medulla oblongata w/ cardiac center; integrates blood pressure control by altering CO and blood vessel diameter. 1. Baroreceptors: pressure receptors in carotid sinuses (to protect brain) and aorta (to keep up BP in systemic circ.) send signals to vasomotor center when BP rises and stretches the receptors. This inhibits the center in the medulla, resulting in vasodilation. A signal is also sent to stimulate parasympathetic division to slow heart rate. See figure 18.8 A drop in MAP initiates vasomotor reflex to increase HR and CO. 2. Chemoreceptor initiated reflexes: (carotid and aortic bodies) a drop in O2 or pH in aortic arch causes an increase in cardiac output and vasoconstriction. Short-term chemical controls See Table 18.2: O2 and CO2 act on chemoreceptors but other chemicals act directly on smooth muscle or vasomotor center. See figure 18.14 1. Adrenal medulla hormones: NE is vasoconstrictive. Epinephrine raises cardiac output by increasing permeability to calcium. 2. Atrial natriuretic peptide: acts on blood volume and kidneys to lower BP. Antagonistic to aldosterone, the kidneys will be stimulated to excrete Na + (and water follows salt) to lower blood volume and also causes generalized vasodilation. 3. ADH: in response to dropping BP, this causes intense vasoconstriction during hemorrhage and water retention by kidneys. 4. Angiotensin II: causes vasoconstriction in response to low BP. 5. Endothelium derived factors: endothelin is a potent vasoconstrictor that allows calcium entry into smooth muscle, in response to low BP. 6. Nitric oxide: causes vasodilation, released from endothelium of blood vessels during high BP. Shortlived, but helps return BP to normal after sympathetic stimulation. 7. Inflammatory chemicals: histamine causes vasodilation 8. Alcohol: lowers BP by inhibiting ADH, depresses vasomotor center and is a vasodilator in skin Long-term mechanisms and renal regulation See figure 18.9: a rising blood volume causing a rise in BP stimulates kidneys to elimination water, which reduces blood volume and blood pressure. A drop in blood volume causes kidneys to retain water and raise blood volume and pressure. See figure 18.10 1. Direct renal mechanism: when there is a rise in blood volume or pressure, the kidneys filter faster, which decreases the time for reabsorpion of filtrate (namely water) and more fluid leaves as urine. A drop in blood volume or pressure means water is conserved and returned to the blood stream during slower filtration. 2. Indirect renal mechanism: renin-angiotensin mechanism from low BP is activated. Juxtaglomerular cells of the kidney release rennin into blood that triggers production of angiotensin II. It is a potent vasoconstrictor that increases rate of blood delivery to kidneys. It also stimulates release of aldosterone from adrenal cortex and release of ADH. This then causes an increase in blood pressure. Chronic hypertension: can be caused by diet, obesity, age, race, heredity, stress, smoking. Ways to treat: diuretics, betablockers, calcium channel blockers, block epinephrine receptors, ACE inhibitors (angiotensin converting enzyme) Capillary dynamics See figure 18.13 Vasomotion: slow and intermittent flow of blood through capillaries Diffusion: O2 and CO2, most nutrients and metabolic wastes pass between blood and interstitial fluid by diffusion. See figure 18.15 Hydrostatic pressure (HP): force exerted by a fluid pressing against a wall. HP is the same as capillary blood pressure (HPC). It tends to force fluids through capillary walls. HPC is higher at the arterial end than the venous end. BP is opposed by HPIF acting outside the capillaries, pushing fluid in. The net HP is the difference of HPC and HPIF . Colloid osmotic pressure: created by presence in a fluid of large, nondiffusible molecules (plasma proteins, namely albumin) that are prevented from moving through the capillary membrane. These molecules draw water toward them whenever water concentration in their vicinity is relatively lowerthan on the opposite side of the capillary membrane (ie. In the tissues). OPC pulls water back into capillary blood. Hydrostatic-Osmotic pressure interactions See figure 18.16 Net filtration pressure (NFP): fluid out at arterial end, osmotic forces dominate at venous end. Net loss (more out than in) = 1.5 ml/min, returned to circulation by lymphatics. Circulatory shock: blood vessels are inadequately filled Hypovolemic shock: large scale blood or fluid loss (hemorrhaging, vomiting, dehydration, diarrhea, burns) See figure 18.17 a rise in heart rate to compensate results in a weak, thready pulse an increase in vasoconstriction occurs to enhance venous return a sharp drop in BP is a late, but serious, sign Vascular shock: blood volume is normal and constant. Poor circulation due to extreme vasodilation (expansion of vascular bed). PR drops, followed by a rapidly dropping BP. Anaphylaxis, septicemia (bacterial toxins are vasodilators), failure of sympathetic NS, even sunbathing can cause this. Anaphylaxis: loss of vasomotor tone due to an allergic reaction or other cause of the release of histamine (a potent vasodilator) Cardiogenic shock: pump failure, due to multiple myocardial infarcts Atherosclerosis: aorta and coronary arteries most affected. Damage to endothelium triggers repair processes that can go haywire, especially if many LDL’s (with cholesterol) are present. These LDL’s deliver cholesterol to tissues which further complicates repair and proliferation of tunica interna and media work to decrease the diameter of the lumen. Thrombi can develop and block even more. Treatment/prevention: lower cholesterol and LDL, raise HDL. Reduce inflammation, coronary bypass surgery, balloon angioplasty, change lifestyle.