Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
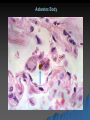
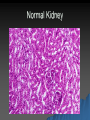
Environment Pathology and Disease Bethy S Hernowo Faculty Of Medicine Universitas Padjadjaran Environmental Disease ٭Diseases & lesions caused by chemical or physical injuries ٭Environmental disease : common ٭ILO (International Labor Organization) estimated : 1.1 million people, work-relate Sources of Exposure Environmental – Man-made Intentional (Hg, Minimata, Japan) Accidental – methyl isocyanate, Bhopal, India – radiation, Chernobyl – Natural (H2S/CO/CO2, Cameroon) Occupational (mining, dye, chemical) Iatrogenic (drugs) Self-administered (substance abuse, suicide) Mechanisms of Toxicity Corrosive, tissue destruction (acids, alkali) – desiccation – protein destruction denaturation hydrolysis – fat saponification Inhibition of enzyme activity cyanide: cytochrome oxidase ABSORPTION and DISTRIBUTIONS of TOXICANTS Environmental Pollution Air pollution 1. Outdoor Air Pollution 1.1. Ozone 1.2. Nitrogen dioxide 1.3. Sulfur dioxide 1.4. Carbon monoxide 1.5. Lead 1.6 Particulates Major Outdoor Air pollutants Air pollutants Origin(s) Ozone Interactions of oxygen with various pollutants such as oxide of nitrogen, sulfur, & hydrocarbons Nitrogen dioxide Come, & wood Sulfur dioxide Combustion of fossil fuel such as coal, gasoline, & wood Consequences Is highly reactive & oxidizes polyunsaturated lipids that become irritants & induce release of inflammatory mediators affecting all airways down to bronchoalveolar junctions Dissolves in secretions in airways to form nitric & nitrous acids, which irritate & damage linings of airway Yields sulfuric acid, bisulfites, and sulfites, which irritate & damage linings of airways; together with nitric acid, contributes to acid rain Carbon monoxide Incomplete combustion of gasoline, oil, wood, and natural gas Lead Discussed in a subsequent section particulates Great variety of finely divided (and therefore airborne) pollutants ranging from relatively innocuous plaster dust to highly dangerous asbestos dust May include lead, ash, hydrocarbon residues, and other industrial and nuclear wastes Combines with hemoglobin to displace oxyhaemogloblin & thus induce systemic asphyxia Major contributor to smog & a major cause of respiratory disease Patterns Of Lung injury Related To Air Pollution Lung response Pathogenic Mechanism(s) Acute or chronic inflammation (e.c. Chronic bronchitis) Emphysema Asthma Hypersensitivity pneumonia Pneumoconiosis Direct cell injury Neoplasia Enhanced proteolysis Allergic or irritant effect Immunologic injury Fibrotic reactions caused by cytokines released from macrophages & other recruited leucocytes Mutagenic & promoting effects Air pollution 2. Indoor Air Pollution 2.1. Tobacco smoke 2.2. Carbon monoxide 2.3. Nitrogen dioxide 2.4. Wood Smoke 2.5. Formaldehyde 2.5. Radon 2.6. Asbestos fibers 2.7. Manufactured mineral fibers 2.8 Bioaerosol Health Effects Of Indoor Air Pollutans Toxic And carcinogenic Metals Heavy Metal Toxic Agents Mercury (HgCl2 , ATN; org Hg, CNS function) Lead ( inhibits heme synthesis, CNS function, kidneys, GI) – 2-11% of children in US exceed 10 μg/dL Arsenic Iron Industrial Exposures Organ/System Effect Toxicant Cadiovascular Heart disease Carbon,monoxide,lead,solvents, cobalt,cadmium Respiratory Nasal cancer Lung cancer Isopropyl alcohol,wood dust Radon,asbestos,silica,bis(Chloromethyl)ether,nickel,arsenic, Chromium,mustard gas Grain dust,coal dust,cadmium Berylium,isocyanates Silica,asbestos,cobalt COPD Hypersensitivity Fibrosis Nervous Peripheral neuropathies Ataxic gait Central nervous depression Cataracts Solvents,acrylamide,methyl Chloride,mercury,lead,arsenic, DDT Chlordane,toluen,acryllamide, Mercury Alcohols,ketones,aldehydes, Solventsradiation Ultraviolet URINARY Toxicity REPRODUCTIVE Male infertility Female infertility Teratogenesis HEMATOPOIEIC Leukemia Mercury,lead,glycols ethers, Solvents Napthylamines,4aminobiphenyl,benzidine, Rubber products Lead,pthalate plasticizers Cadmium,lead Mercury,polychlorinated Biphenyls Benzene,radon,uranium SKIN Foloculitis and acneiform Dermatosis Cancer Polychlorinated bipyhenyls, Herbicides Ultraviolet radiation GASTROINTESTINAL Liver angiosarcoma Vinyl chloride Bladder cancer Pneumoconiosis ٭The non-neoplastic lung reaction to inhalation of mineral dust ٭Agent : coal dust, silica, asbestos, beryllium ٭Coal Workers’ Pneumoconiosis (CWP) Spectrum of lung finding in coal workers 1. Asymptomatic anthracosis 2. Simple Coal workers pneumoconiosis 3. Progressive massive fibrosis (PMF) Mineral Dust –Induced Lung Disease Pathogenesis of Pneumoconiosis Morphology 1. 2. Pulmonary anthracosis Inhaled carbon pigment is engulfed by alveolar or interstitial macrophage, then accumulate in connective tissue linear streak & aggregates pigment identify pulmonary lymphatic & mark the pulmonary lymph node Simple CWP Characterized : coal macules & coal nodule. coal macules consist : dust-laden macrophages. The lesion scattered, but uppers lobes & upper zones of the lower lobes more heavily involved Morphology 3. Caplan syndrome Coexistence of rheumatoid arthritis with a pneumoconiosis development distinctive nodular develop fairly rapidly The nodular lesions central necrosis surrounded by palisading fibroblast, palsma cells, macrophages containing coal dust & collagen The syndrome also occur in asbestosis & silicosis Clinical course CWP 1. 2. 3. 4. CWP usually benign produce little decrement in lung function Minority cases pulmonary dysfunction, hypertension & cor pulmonale CWP PMF (progressive massive fibrosis) linked variety factors : coal dust exposure level & total dust burden PMF tendency to progress even absence exposure Silicosis ٭Caused by inhalation crystalline silica ٭Occupations associated development silicosis : quarry mining, sandblasting, drilling, tunneling, & stone cutting ٭Incidence : 1500 cases each year in US ٭Silica : 1. Crystalline : quartz, cristobalite, tridymite ( most toxic and fibrogenic) 2. Amorphous forms (most commonly implicated in silicosis) Classification Silicosis 1. 2. 3. 4. Acute silicosis : exposure very high level of silica & develops quickly Chronic ( nodular ) silicosis: exposure over prolonged periods Characteristic fibrotic nodules of silicosis Complicated ( conglomerate silicosis) result progression of chronic silicosis Other pulmonary disease : silicosis Morphology Gross : Characteristic nodule in early stage: tiny, barely palpable, discrete, pale-to-blackened, nodules in upper zones Microscopically : silicotics nodule demonstrates concentrically arranged hyalinized collagen fibers surrounding an amorphous center. Microscopically: Silicosis Clinical course ≈ Chronic silicosis detected routine chest radiographs (asymptomatic) ≈ Radiographs : fine nodularity in the upper zones function : normal/ moderately affected ≈ Most patients do not develop shortness of breath until late in the course ≈ The disease slow to kill Asbestosis » Asbestos family of crystalline hydrated silicates » Occupotional exposure to asbestos, linked to: 1. Parenchymal interstitial fibrosis (asbestosis) 2. Bronchogenic carcinoma 3. Pleural effusions 4. Localized fibrous plaque, rarely diffuse fibrous plaque 5. Malignant pleural & peritoneal mesothelioma 6. Laryngeal carcinoma Pathogenesis Asbestosis ٭Dictate : concentration, size, shape & solubility of different forms asbestos ٭Two forms asbestos: 1. Serpentine (fiber is curly & flexible) : Chrysotile 2. Amphibole (fiber is straight, stiff,& brittle) more pathogenic ٭The greater pathogenicity amphiboles related: 1. Chrysotiles impacted respiratory removed mucociliary trapped gradually leached from tissue 2. Amphiboles align themselvesairstream deliver deeper penetrate epithelial cells reach interstitium Morphology Gross: diffuse pulmonary interstitial fibrosis Microscopically : Characteristic asbestos bodies : golden brown, fusiform or beaded rods with a translucent center. They consist of asbestos fibers coated with an iron containing proteinaceous material. Pleural plaque : well-circumscribes plaque of dense collagens Asbestos Body Clinical course ≈ Indistinguishable from other diffuse interstitial lung disease ≈ Typically, progressively worsening dyspnea appears 10-20 years after exposure ≈ The disease may static or progress to congestive heart failure, cor pulmonale and death. Tobacco Smoking 400,000 deaths/yr (21% of all deaths in US) 50 Million smokers in US Smoke composition – carcinogens (polycyclic HC, bnaphthylamine, nitrosamines) Irritants and toxins – ammonia, formaldehyde, oxides of nitrogen CO Nicotine Relative Disease Risks Associated with Smoking Lung Ca death Mouth Ca Larynx Ca Esophogus Ca CAD >35 yo Cerebro VD >35 yo COPD Male 22 27 10 8 3 4 10 Female 12 6 18 10 2 5 10 Ill health effects of smoking partially reversible Tobacco smoke Adverse effects of smoking Injury By Chemical Agents Mechanisms of chemical injury: 1. Dose 2. Requirement for metabolic conversion 3. Sites of absorption, accumulation, or excretion 4. Individual variation 5. The capacity of the chemical to induce an immune response 6. Unintentional transmission of infections Injury by Therapeutic Agents (adverse Drug Reactions) Exogenous Estrogens And Oral Contraceptives Exogenous Estrogens ( alone & usually natural estrogen) Adverse effects of estrogen therapy : » Endometrial carcinoma » Breat carcinoma » Thromboembolism » Cardiovascular disease 1. 2. Oral contraseptives Adverse effects of oral contraseptives ( contain synthetic estrogens & always with progestin) 1.Breast carcinoma 6.Hypertension 2.Endometrial cancer 7. Hepatic adenoma 3.Cervical cancer 8. Gallbladder disease 4.Ovarian cancer 9. Cadiovascular 5.Thromboembolism disease Acetaminophen ≈ When taken very large doses hepatic necrosis ≈ The window therapeutic dose : 0,5 gr ≈ Toxic dose : 15-25 gr ≈ Toxicity begins : nausea, vomiting, diarrhea, sometimes shock and jaundice ≈ Serious overdose : liver failure, renal and myocardial damage Aspirin (Acetylsalicylic Acid) ≈ Overdose ( 2-4 gr) : accidental ingestion of large number table young children ≈ Suicidal ( 10-30 gr) adult ≈ Effects : at first : respiratory alkalosis metabolic acidosis death ≈ Chronic : take > 3 gr daily headache, dizziness, tinnitus, difficulty hearing, mental confusion, nausea, vomiting and diarrhea Injury by Non therapeutic Toxic Agents 1. Lead poisoning 2. Carbon monoxide 3. Alcohol and drug abuse Clinical And Pathologic Features Of Lead Poisoning Lead Lines Lead causes injury by its multiple metabolic effects: 1. 2. 3. 4. 5. High affinity for sulfhydryl groups & interferes with enzymes Competes with calcium Interferes with membraneassociated enzymes Interferes with nerve transmission and brain Membrane effects damage the kidneys Morphology Major target of Lead toxicity : blood, CNS, GIT and kidneys 1. Blood changes characteristic result lead accumulation occur fairly early. 2. Brain damage is prone to occur in children 3. GIT : colic, extremely severe 4. Kidney : proximal tubular damage with intranuclear lead inclusions. Normal Kidney Acute Tubular Necrosis Carbon Monoxide ٭Nonirritating, colorless, tasteless, odorless imperfect oxidation of carboneceous materials continues to be cause accidental & suicidal death ٭CO kills by inducing CNS depression ٭CO act as a systemic asphyxiant carboxyhemoglobin incapable carrying oxygen ٭Acute Poisoning: generalized cherry-red color skin & mucous membrane ٭chronic poisoning : evoke widespread ischemic changes in the CNS Classification Of Drugs Of Abuse Class Examples Sedatives & hypnotics CNS symphatomimetics or stimulants Alcohol, barbiturates Cocaine, amphetamines Ritalin, weight loss products Opioids Heroin, morphine, methadone Cannabinoids Marijuana, hashish Hallucinogens or psychedelics Lysergic acid diethylamide (LSD),mescaline Aerosol sprays,glues,toluene Inhalants Nonprescription drugs Ingredients :Atrophine, scopolamin, antihistamine, weak analgesics Alcohol And Drugs Of Abuse 1. Ethanol 2. Cocaine 3. Heroin 4. Marijuana 5. Other Illicit drugs Metabolism of Ethanol Ethanol Adverse effects of ethanol: 1. Acute alcoholism effects mainly CNS induced hepatic & gastric changes 2. Chronic alcoholism morphologic alterations liver & stomach Normal Liver Fatty Change in Liver Fatty Change in Liver Cocaine Manifestations of acute cocaine toxicity 1. Sympathetic nervous system stimulation dilatated pupils, vasoconstriction 2. Lethal arrhythmias & myocardial infarction 3. Cerebral infarction & intracranial hemorrhage 4. Rhabdomyolysis 5. In pregnant women spontaneous abortion Manifestations of chronic toxicity 1. Perforation nasal septum 2. Decreased lung diffusing capacity 3. Dilated cardiomyopathy Effect of cocaine on neurotransmitters CNS Synapse Sympathetic Neuron-target Cell Interfere Heroin ≈ Effects : euphoria, hallucinations, somnolence & sedations ≈ Heroin adversed physical effects, related to 1. Pharmacologic action of the agent 2. Reactions to the cutting agents/contaminations 3. Hypersensitivity reactions 4. Diseases contracted incident use needle : ٭Sudden death ٭Pulmonary complication ٭Infectious complications ٭Cutaneous lesions ٭Kidney disease Marijuana 1. 2. 3. 4. Effects: Distorts sensory perception & impairs motor coordination Lung laryngitis, bronchitis, cough, hoarseness increased risk for cancer Increased heart rate and blood pressure angina Induce chromosomal damage Other Illicit Drugs The variety of drug try by those seeking new experiences Range : various stimulants (amphetamines) to depressants (benzodiazepines) to hallucinogens (ectasy) Dangerous combination : alcohol & driving Injury By physical Agents 1. 2. 3. 4. 5. ◊ Mechanical Trauma Abrasion Contusion Laceration Incised wound Puncture wound Thermal Injury Thermal burns Hyperthermia Hypothermia Injury By physical Agents Abrasion : A wound produced by scraping or rubbing Contusion : A wound produced by a blunt object damage blood vessels & extravasation Injury By physical Agents Laceration : A tear or disruptive stretching of tissue force by blunt object Injury By physical Agents Puncture wound : caused by a long narrow instrument Penetrating when the instruments pieces the tissue & Perforating when it traverses a tissue to also create an exit wound Thermal injury Gross: Full-thickness burn are white or charred, dry and anesthetic, depending on the depht, partial-thickness burns are mottled with blisters & painful ◊ Microscopically: Devitalized tissue coagulative necrosis, adjacent to vital tissue accumulates inflammatory cells & exudation Hyperthermia Heat cramps loss of electrolytes via sweating Heat exhaustion onset sudden, most common hyperthermic syndrome failure Cardiovascular system to compensate for hypovolemia Heat stroke high ambient temperatures & high humidity thermoregulatory mechanism fail Hypothermia 1. 2. Local reaction. Chilling or freezing of cells & tissues causes injury in two ways Direct effects mediated by physical dislocations within cells, high salt consentration Indirect effects exerted by circulatory changed Electrical Injury 1. 2. Electrical injuries death arise from low-voltage or high-power lines or lighting Two types of injuries Burns Ventricular fibrillation or cardiac & respiratory center standstill Injury Produced By Ionizing Radiation Effects of ionizing radiation on DNA Injury Produced By Ionizing Radiation Overview of the major morphologic consequences of radiation injury