Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
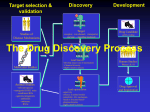
INTRODUCTION TO PHARMACOLOGY Pharmacology Introduction Outcomes Briefly discuss professional principles relevant to drug administration Briefly discuss ethical principles applied to drug administration Explain the nurses roles in ‘health education’ related to medication Define Pharmacology Define Pharmacotherapuetics Define Pharmacokinetics Define Pharmacodynamics Define the words drug and medicine Outline the history of drug development State four sources of drugs, giving one example from each source Explain drug names- giving one example from the BNF Pharmacology Introduction Outcomes State three different ways in which drugs work (pharmacodynamics) giving examples of drugs from each group. Briefly explain what is meant by therapeutic range Briefly explain why side effects may occur in addition to ‘desired’ effects Define and outline types of adverse drug reactions State the role of the MHRA List three types of drug interaction Outline the stages of clinical trials Case Example 1 Lauren (age 21years) was prescribed Clozapine whilst in hospital to treat her schizophrenia. She has been taking this medication for one year now and her mental health has improved considerably. She has been discharged from hospital (under Section 25) and is living in supported accommodation near her mother. Since staring on the medication she has experienced a number of side effects. She feels tired much of the time, has gained 4 stone in weight, is always constipated and has excessive saliva production (hyper salivation) (she is too embarrassed to stay overnight at a friend’s home). Since she is feeling a lot better mentally, and is getting really fed up with the side effects of her medication, she decides to stop taking the Clozapine. She intends to discuss this with her CPN when he next visits her (he is off sick at present and they have been too short staffed to send anyone else!). Discuss!! Case example 2 Student nurse Helen was on her first clinical placement and had been on the ward for a few days. She was asked by the nurse in charge to give a patient (Mr Y) a suppository, as he was complaining of constipation. She was instructed to use the ‘PR’ tray from the clinical room. She followed the correct procedure (as taught by the clinical teacher) with respect to inserting the suppository (e.g. maintaining patient dignity, ensuring correct patient position and effective communication). The suppository was inserted and the patient advised to ring for the nurse as soon as he needed the toilet. Half an hour passed and the patient expressed concern that the suppository had not worked (at all) and this had never been the case previously. It transpired that the usual suppository (‘glycerin’) was not on the PR tray and the student had used one called ‘aminophylline’. Discuss!! Case example 3 Mr Edwards (age 67) has had NIDDM for more than 15 years. Initially, his condition was controlled with diet alone but for the last 5 years he has needed oral hypoglycaemic agents. He attends all his GP and diabetic clinic appointments and seems to be complying with both diet and medication regimes. He is a keen gardener lost confidence in going to his garden alone as he has had a number of episodes of nausea, sweating, tremors, dizziness and palpitations that occur mostly in the late morning. His prescription drugs have not been changed for a number of years and he is not feverish, has no pain, nor is he exhibiting any signs of illness other than these worrying episodes. His main concern is that these symptoms will occur when he is driving. Discuss! Case Example 4 Mr Edwards (Age 67–man diagnosed with NIDDM) also has been medically managed for his hypertension for the last 15 years has hypertension. He was taking an ACE inhibitor to control his Hypertension was had now been prescribed a Diuretic as well. He returned to talk to the practice nurse to complain that his dizziness had returned, particularly when he stood up and he had actually stumbled with this a couple of times. The Practice nurse reviewed his Blood pressure (lying and standing) and noticed that at there was a difference. Discuss the advice you would offer Mt Edwards Case Example 5 A doctor was deputising for a colleague absent on leave. After a particularly demanding night, he was asked, in the early hours of the morning, to see a premature infant with congestive heart failure. He was not normally responsible for the care of premature infants but he requested Digoxin to be given intramuscularly and calculated (by mental arithmetic) that the dose should be 0.6 mg. Just as he settled down for a restorative nap, the nurse phoned to ask whether the dose shouldn’t be 0.06 mg as she had had to open two ampoules. Without thinking he told her to “give it as I ordered”. An hour later, he was called to the ward because the baby had suffered a cardiac arrest. Discuss!! http://www.medicalprotection.org/uk/booklets/common-problems-hospital/prescribing-for-children accessed 20/08/2012 ‘Justification for study’ The nurse with knowledge and understanding of pharmacology will be more confident in drug administration Who is responsible for ‘health education’ with respect to medication? What professional principles are relevant? What ethical principles can be applied to the issue of patients being educated about their medication? Some Clinical Practice Considerations The patient may ask: How quickly will the drug work? (e.g. analgesic) Do I take the tablets with food or on an empty stomach? (e.g. antibiotics) Can I take my other tablets (OTC medication) with the medicine I have been prescribed? (e.g. aspirin) Does it matter if I take the tablets at different times? (e.g. antibiotics) The nurse needs to be able to give the patient accurate information and ‘empower’ the patient to be able to self medicate ‘Justification’ King RL (2004) Nurses’ perceptions of their pharmacology educational needs Journal of Advanced Nursing45(4), 392–400 Background: Lack of science teaching in nurse education Theory–practice gap in this area of the curriculum Findings: Limited understanding of the subject Dissatisfaction with the teaching of pharmacology, Resulting anxiety on qualifying Conclusion: Nurses have a limited understanding of pharmacology They recognize the need for pharmacology knowledge in practice. Improved pharmacology teaching might increase nurses’ confidence in: drug administration + patient education, and decrease anxieties related to these roles ‘Justification’ Latter S Rycroft-Malone J Yerrell P Shaw D (2000) Evaluating educational preparation for a health education role in practice: the case of medication education Current health care policy highlights the importance of nurses contributing to educating patients about medication. Findings (of the study) highlighted the importance of: * sufficient taught pharmacology * an evidence-based curriculum * practice-based learning J Adv Nurs. 2000 Nov;32(5):1282-90. The NMC (2008) Medicine Management guidelines directs us all to address our Knowledge and competence for safe medicines storage and administration. ‘Justification’ The Impact of Drug Errors Patients, their relatives and professionals can experience considerable trauma and there can be a substantial additional cost to the NHS (Armitage 2004) Appropriate (and Inappropriate) use of drugs Drugs are used to: * Cure or Arrest DISEASE * Relieve SYMPTOMS * Obtain a DIAGNOSIS * PREVENT disease occurring (Some situations when they should NOT be used: To make the patient ‘easier to manage’! When they will do more harm than good) Nurses need knowledge of pharmacology Nurses need to: Obtain drug HISTORIES ASSESS patients taking drugs ADMINISTER drugs EDUCATE patients MONITOR, record, evaluate and REPORT patient responses to drugs AND … counsel patients having drug rehabilitation Science of Pharmacology Pharmacology Science (logos) of drugs (pharmakon) PharmacoTHERAPEUTICS = use of drugs to treat disease Assessment Implementation Monitoring and Reassessment/evaluation Science of Pharmacology PharmacoKINETICS = Absorption, distribution, metabolism & excretion of drugs (what the body does to the drug) PharmacoDYNAMICS = Biochemical & physical effects of drugs; Mechanisms of drug action (what the drug does to the body) TOXICOLOGY = toxicity & adverse effects of drugs Drugs and Medicines A DRUG is any chemical (except food) that will bring about a response in the body * All drugs are TOXIC (potentially) * All drugs produce SIDE EFFECTS * Interactions can occur between drugs (or between drugs and food) A MEDICINE is a drug that has been ‘modified’ so that it is suitable for administration The (very brief!) History of Pharmacology Oldest Science (originally a brand of magic!) Opium used for thousands of years Samuel Dale (London) catalogued existing knowledge of drugs Descriptive Pharmacopoeia Early in 19th Century began experiments to establish WHY drugs worked (beginning of real pharmacology) Discoveries of the 19th Century include: 1842 ether 1847 chloroform History of Pharmacology Some key discoveries of the 20th Century: 1922 Insulin 1941 Penicillin (first treatment) 1952 Chlorpromazine 1957 Benzodiazepine derivatives 1958 Haloperidol 1961-1967 Levodopa Sources of drugs / medicines Plant products or Plants: Fox Glove DIGOXIN Poppy OPIUM Belladonna ATROPINE Coffee CAFFEINE Tobacco NICOTINE Animal products Premarin (conjugated Oestrogen) from Pregnant Mares Insulin from pigs & cows Heparin from pigs & cows Inorganic compounds (compounds with no Carbon) * Zinc + Sulphate ions Zinc Sulphate (Calamine lotion) * Aluminium +Hydroxyl Aluminium hydroxide * KCl Synthetic sources Drugs made in LABORATORY Most drugs today made in labs = safer Many drugs are synthetic copies of naturally occurring substances e.g. steroids Insulin (biosynthetic human insulin / recombinant or DNAderived insulin) Plasmid from E coli cell Plasmid opened by an enzyme Human insulin gene inserted Recombination (new insulin gene + plasmid) Cell division cells produce human insulin Recombined plasmid put into host E Coli cell Drug Names Chemical Describes actual Compound ? ? Generic Official Medical name for active substance Brand Name Name chosen by manufacturer DIAZEPAM SODIUM VALPROATE VALIUM EPILIM Pharmacodynamics Involves study of the effects of the drug in the body & its mechanisms of action What Drugs Do REPLACE natural body substances E.g. thyroxine, insulin Act against ABNORMAL cells or invading ORGANISMS E.g. chemotherapeutic agents, antibiotics What Drugs Do Interfere with cell FUNCTION Act at RECEPTOR SITES intensifying cell activity (agonists) or reducing activity (antagonists) Clozapine administration was found to produce dopamine2 (D-2) and serotonin2 (5-HT2) receptor blockade’ Inhibit ENZYMES neostigmine inhibits cholinesterase Therapeutic Effect Dose THERAPEUTIC RANGE Time Side Effects A drug, once absorbed to the circulation, will be distributed throughout the body affecting other parts SIDE EFFECTS Examples Drug Side effect Clozapine Constipation, Hyper salivation, Iron Constipation, Nausea Codeine Constipation Morphine Constipation Adverse Reactions ‘Any response to a drug which is noxious, unintended and occurs at doses used in man for prophylaxis, diagnosis or therapy’ ADVERSE REACTION (WHO) Adverse reactions: * may be due to ALLERGY or GENETIC absence of specific enzymes * may be predictable or unpredictable * may be TERATOGENIC (causing embryonic deformities) * are IATROGENIC (caused by practitioners) The Medicines and Healthcare products Regulatory Agency (MHRA) The Medicines and Healthcare products Regulatory Agency (MHRA) is the government agency which is responsible for ensuring that medicines and medical devices work, and are acceptably safe. • The MHRA website http://mhra.gov.uk SUSPECTED ADVERSE DRUG REACTIONS If you are suspicious that an adverse reaction may be related to a drug or combination of drugs please complete this Yellow Card. PATIENT DETAILS SUSPECTED DRUG(S) SUSPECTED REACTION(S) OUTCOME OTHER DRUGS (including self-medication & herbal remedies) Additional relevant information The MHRA REGULATES: Controlled substances EXAMPLES: Opiates Generic / proprietary drugs Paracetamol Orphan drugs Rare diseases/small populations Over-the-counter Prescription Nurse (OTC) drugs Paracetamol Only Medicines (POM)Warfarin Prescriber’s Extended Formulary Minor ailments, minor injuries, health promotion & palliative care Drug Interactions These interactions may be beneficial or harmful and include: Alterations in ABSORPTION Altered METABOLISM of other drugs Competition for RECEPTORS Some important interactions: Oral anticoagulants and aspirin Development of new drugs Preclinical trials New drugs or treatment approaches : often tested first on animals (or live human cells in test tubes). Scientists identify an approach that is most likely to succeed, and then carry out preliminary research into safety and effectiveness. Phase 1 studies: Early Clinical Trials These first trials usually involve a small number of individuals (less than 100) who are healthy. However … there are times when the new compound is tested first in people who have the condition that the drug is meant to treat (especially when the drug is meant to treat a very serious disease and The objective= is likely to have serious side to find out if the effects). new drug is safe. Phase 2 Continuing Clinical Trials If the new compound is considered safe on animals, testing is expanded to see if it is effective, Trials include people who have the disease or Condition against which the researchers think a new compound will be effective. Phase 3 studies A drug is tested in several hundred to several thousand subjects. This large-scale testing provides more information about: *the drug's effectiveness, *possible side effects, and *safety in a broader range of people. Drug Trials Recall that Six men were treated in intensive care after experiencing a serious reaction to a drug taken during a clinical drugs trial in north-west London in 2006 The six healthy men, all under 40, had volunteered to take part in a trial of an anti-inflammatory drug, to treat conditions such as rheumatoid arthritis and leukaemia, being tested at an independent research unit based at Northwick Park Hospital. The six suffered multiple organ failure, and two were said to be critically ill. Another two men, who had been given a dummy version of the drug in the trial, did not fall ill. The trial was stopped as soon as the men fell ill. http://news.bbc.co.uk/1/hi/england/london/4807042.stm Accessed 20/08/2012 Drug trials also don’t always bring about what they are expected to do – The sceince does not work out: http://www.wired.co.uk/magazine/archive/2012/02/features/trials- and-errors accessed 07/11/2013 ‘Homework’! – Check the ingredients of four or five different OTC drugs for comparison and to familiarize yourself with the difficulty a layperson may encounter while trying to find this information. Give rationale for why some drugs need to be kept under lock and key on the hospital unit. Discuss this with your mentor. Familiarize yourself with 4 or 5 drugs that are often prescribed & administered in your placement setting. Outline the role of the nurse in the safe administration of these drugs. Discuss this with your mentor & your clinical teacher.