Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
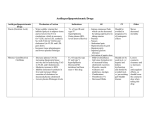
Chronic Care Programme Treatment guidelines Hyperlipidaemia Chronic condition Consultations protocols Preferred treating provider Notes preferred as indicated by option referral protocols apply Maximum consultations per annum Initial consultation Follow-up consultation Tariff codes Option/plan Provider GMHPP Gold Options G1000, G500 and G200. Blue Options B300 and B200. GMISHPP General Practitioner Pulmonologist Physician Gastroenterologist Neurologist Cardiologist Paediatrician Cardiology Paediatrician Mild to Moderate New Patient Existing Patient New Patient 1 0 1 1 0183; 0142; 0187; 0108 1 3 Mild to Moderate New Patient Existing Patient Consultation: Dietician Initial consultation Follow-up consultation Tariff codes 1 0 Severe Existing Patient 1 2 Severe New Patient Existing Patient 0 1 1 0 0 1 051 Mild to Moderate New Patient Existing Patient Consultation: Dietician Initial consultation Follow-up consultation Tariff codes 1 0 Severe New Patient Existing Patient 0 0 2 0 0 1 053 Investigations protocols Type Provider Tariff code Urine dipstick (per stick, irrespective of the number of tests on stick) Blood glucose ECG without effort Chol/HDL/LDL/Trig TSH Serum urea Serum creatinine Serum potassium GP; Specialist; Pathologist GP; Specialist; Pathologist GP or Specialist (see list) Pathologist Pathologist Pathologist Pathologist Pathologist Maximum investigations per annum New Existing New patient patient patient Existing patient 4188 1 1 2 2 4057; 4050 1 0 1 0 1232 1 1 1 1 4025 4507 4151 4032 4113 2 1 1 1 1 1 0 0 0 0 3 1 1 1 1 3 0 1 1 1 Serum sodium Aspartate aminotransferase (AST) Alanine aminotransferase (ALT) Creatine Kinase (CK) CXR Pathologist Pathologist 4114 4130 1 1 0 1 1 1 1 1 Pathologist 4131 1 1 1 1 Pathologist Pathologist 4132 3445 1 0 1 0 1 1 1 1 E78.1-E78.5 ICD 10 coding General Hyperlipidemia, hyperlipoproteinemia or dyslipidemia is the presence of raised or abnormal levels of lipids and/or lipoproteins in the blood. Lipids (fatty molecules) are transported in a protein capsule, and the density of the lipids and type of protein determines the fate of the particle and its influence on metabolism. Lipid and lipoprotein abnormalities are extremely common in the general population, and are regarded as a highly modifiable risk factor for cardiovascular disease due to the influence of cholesterol, one of the most clinically relevant lipid substances, on atherosclerosis. In addition, some forms may predispose to acute pancreatitis Classification Hyperlipidemias are classified according to the Fredrickson classification which is based on the pattern of lipoproteins on electrophoresis or ultracentrifugation.[1] It was later adopted by the World Health Organization (WHO). It does not directly account for HDL, and it does not distinguish among the different genes that may be partially responsible for some of these conditions. It remains a popular system of classification, but is considered dated by many. Fredrickson classification of Hyperlipidemias Problems Labs description Hyperlipoproteinemia Synonyms Type I Buerger-Gruetz syndrome, Primary hyperlipoproteinaemia, or Familial hyperchylomicronemia Decreased lipoprotein lipase Elevated Diet Control (LPL) or Chylomicrons altered ApoC2 Type IIa Polygenic hypercholesterolaemia or Familial hypercholesterolemia LDL receptor deficiency Bile Acid Elevated LDL Sequestrants, only Statins, Niacin Type IIb Combined hyperlipidemia Decreased LDL receptor and Increased ApoB Elevated LDL Statins, and VLDL Niacin, and Gemfibrozil Triglycerides Type III Familial Defect in Dysbetalipoproteinemia ApoE Increased IDL Treatment Drug of choice: Type IV Type V synthesis Gemfibrozil Endogenous Hyperlipemia Increased VLDL production Increased and VLDL Decreased elimination Drug of choice: Niacin Familial Hypertriglyceridemia Increased VLDL production and Decreased LPL Increased Niacin, VLDL and Gemfibrozil Chylomicrons Hyperlipoproteinemia type I This very rare form (also known as Buerger-Gruetz syndrome, primary hyperlipoproteinaemia, or familial hyperchylomicronemia) is due to a deficiency of lipoprotein lipase (LPL) or altered apolipoprotein C2, resulting in elevated chylomicrons, the particles that transfer fatty acids from the digestive tract to the liver. Lipoprotein lipase is also responsible for the initial breakdown of endogenously made triacylglycerides in the form of very low density lipoprotein (VLDL). As such, one would expect a defect in LPL to also result in elevated VLDL. Its prevalence is 0.1% of the population. Hyperlipoproteinemia type II Hyperlipoproteinemia type II, by far the most common form, is further classified into type IIa and type IIb, depending mainly on whether there is elevation in the triglyceride level in addition to LDL cholesterol. Type IIa This may be sporadic (due to dietary factors), polygenic, or truly familial as a result of a mutation either in the LDL receptor gene on chromosome 19 (0.2% of the population) or the ApoB gene (0.2%). The familial form is characterized by tendon xanthoma, xanthelasma and premature cardiovascular disease. Type IIb The high VLDL levels are due to overproduction of substrates, including triglycerides, acetyl CoA, and an increase in B-100 synthesis. They may also be caused by the decreased clearance of LDL. Prevalence in the population is 10%. Familial combined hyperlipoproteinemia (FCH) Secondary combined hyperlipoproteinemia (usually in the context of metabolic syndrome, for which it is a diagnostic criterion) Treatment While dietary modification is the initial approach, many patients require treatment with statins (HMG-CoA reductase inhibitors) to reduce cardiovascular risk. If the triglyceride level is markedly raised, fibrates may be preferable due to their beneficial effects. Combination treatment of statins and fibrates, while highly effective, causes a markedly increased risk of myopathy and rhabdomyolysis and is therefore only done under close supervision. Other agents commonly added to statins are ezetimibe, niacin and bile acid sequestrants. There is some evidence for benefit of plant sterol-containing products and ω3-fatty acids[2] Hyperlipoproteinemia type III This form is due to high chylomicrons and IDL (intermediate density lipoprotein). Also known as broad beta disease or dysbetalipoproteinemia, the most common cause for this form is the presence of ApoE E2/E2 genotype. It is due to cholesterol-rich VLDL (β-VLDL). Prevalence is 0.02% of the population. Hyperlipoproteinemia type IV This form is due to high triglycerides. It is also known as hypertriglyceridemia (or pure hypertriglyceridemia). According to the NCEP-ATPIII definition of high triglycerides (>200 mg/dl), prevalence is about 16% of adult population.[3] Hyperlipoproteinemia type V This type is very similar to type I, but with high VLDL in addition to chylomicrons. It is also associated with glucose intolerance and hyperuricemia Unclassified forms Non-classified forms are extremely rare: Hypo-alpha lipoproteinemia Hypo-beta lipoproteinemia (prevalence 0.01-0.1%) Signs and symptoms A combination of heredity and diet is responsible for the majority of fat disorders. It is not so much the cholesterol in the diet that is the problem, because that accounts for only 10% of the body’s store. It is the other fats in the diet that alter the way the body handles its cholesterol. There is a convincing relation between fats in the diet and the incidence of atherosclerosis. The guilty fats are mostly the animal fats, but palm and coconut oil are also harmful. These fats are called saturated fats for the chemical reason that most of their carbon atoms have as many hydrogen atoms attached as they can accommodate. More important than the kind of fat is the amount of fat. For many people, fat is half of their diet. A quarter to a fifth is a much healthier fraction, the rest of the diet being made up of complex carbohydrates and protein. This disease is silent for decades, until the first episode of heart disease or stroke. Diagnosis It would be easier if simple cholesterol and triglyceride tests were all it took to assess the risk of atherosclerosis. But the important information is which package the cholesterol is in—the LDLs or the HDLs. That takes a more elaborate testing process. To complicate matters further, the amount of fats in the blood varies greatly in relation to the last meal—how long ago it was and what kind of food was eaten. A true estimate of the risk comes from several tests several weeks apart all done after at least twelve hours of fasting. Treatment Diet and lifestyle change are the primary focus for most cholesterol problems. It is a mistake to think that a pill will reverse the effects of a bad diet, obesity, smoking, excess alcohol, stress, and inactivity. Reducing the amount of fat in the diet by at least half is the most important move to make. Much of the food eaten to satisfy a “sweet tooth” is higher in fat than in sugar. A switch away from saturated fats is the next step, but the rush to polyunsaturated fats was ill-conceived. These, and particularly the hydrogenated fats in margarine, have problems of their own. They raise the risk of cancer and are considered more dangerous than animal fat by many experts. Theory supports population studies that suggest monounsaturated olive oil may be the healthiest of all. There was a tremendous push at the end of the 20th century to use lipid-lowering medications. The most popular and most expensive agents, the “statins,” hinder the body’s production of cholesterol and sometimes damage the liver as a side effect. Their full name is 3-hydroxy-3methylglutaryl-coemzyme A (HMG-CoA) reductase inhibitors. Their generic names are cervistatin, fluvastatin, lovastatin, pravastatin, and simvastatin. Studies show that these do lower cholesterol. Only recently, though, has any evidence appeared that this affects health and longevity. Earlier studies showed, in fact, an increased death rate among users of the first class of lipid-altering agents—the fibric acid derivatives. The chain of events connecting raised HDL and lowered LDL cholesterol to longer, healthier lives is still to be forged. High-tech methods of rapidly reducing very high blood fat levels are performed for those rare disorders that require it. There are resins that bind cholesterol in the intestines. They taste awful, feel like glue and routinely cause gas, bloating, and constipation. For acute cases, there is a filtering system that takes fats directly out of the blood. Niacin (nicotinic acid) lowers cholesterol very effectively and was the first medication proven to improve overall life expectancy. It can also be liver toxic, and the usual formulation causes a hot flash in many people. This can be overcome by taking a couple of aspirins half-an hour before the niacin, or by taking a special preparation called “flush free,” “inositol-bound” or inositol hexanicotinate. Omega-3 oil is a special kind found mostly in certain kinds of fish. It is beneficial in lowering cholesterol. An herbal alternative called gugulipid, Commiphora mukul, an extract of an Indian plant, is supposed to work the same way as the expensive and liver toxic cholesterol-lowering medications. Alternative treatment To lower cholesterol, naturopathic medicine, traditional Chinese medicine, and ayurvedic medicine may be considered. Some herbal therapies include gugulipid, alfalfa (Medicago sativa), Asian ginseng (Panax ginseng), and fenugreek (Trigonella foenumgraecum). Garlic (Allium sativum) and onions are also reported to have cholesterol-lowering effects. In naturopathic medicine, the liver is considered to be an organ that needs cleansing and rebalancing. The liver is often treated with a botanical formula that will act as a bitter to stimulate bile flow in the liver. Before initiating alternative therapies, medical consultation is strongly advised. Medicine formularies Plan or option [Link to appropriate Mediscor formulary] GMHPP Gold Options G1000, G500 and G200 Blue Options B300 and B00 GMISHPP Blue Option B100 [Core] n/a Prognosis The prognosis is good for Type 1 hyperlipoproteinemia with treatment; without treatment, death may result. For Type 2 the prognosis is poor even with treatment. The prognosis for type 3 is good when the prescribed diet is strictly followed. For types 4 and 5 the prognosis is uncertain, due to the risk of developing premature coronary artery disease and pancreatitis, respectively. Prevention Genetic inheritance cannot be changed, but its effects may be modified with proper treatment. Family members of an individual with hyperlipoproteinemia should consider having their blood lipids assessed. The sooner any problems are identified, the better the chances of limiting or preventing the associated health risks. Anyone with a family history of disorders leading to hyperlipoproteinemia also may benefit from genetic testing and counselling to assist them in making reproductive decisions References Frederickson DS, Lee RS. A system for phenotyping hyperlipidemia. Circulation 1965;31:321-7. PMID 14262568. 1. Thompson GR. Management of dyslipidaemia. Heart 2004;90:949-55. PMID 15253984. 2. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult treatment Panel III) Final Report. Circulation 2002; 106; page 3240 OMIM Type I Type IIa Type IIb Online 'Mendelian Inheritance in Man' (OMIM) 238600 Online 'Mendelian Inheritance in Man' (OMIM) 144400 Type III GPnotebook WebMD -1389035478 at GPnotebook . -1664090094 at GPnotebook . Others MeritCare Merck -1375338454 at GPnotebook . 630849560 at GPnotebook WebMD Yahoo Type IV Online 'Mendelian Inheritance in Man' (OMIM) 144600 -1362100182 at GPnotebook WebMD Yahoo Type V Online 'Mendelian Inheritance in Man' (OMIM) 144600 -1355481046 at GPnotebook . . Inborn error of lipid metabolism - dyslipidemia (E78 and E71.3, 272) Hyperlipidemia Hypercholesterolemia/Hypertriglyceridemia (Familial hypercholesterolemia, Combined hyperlipidemia) - Xanthoma Hypoalphalipoproteinemia/HDL (Lecithin cholesterol acyltransferase deficiency, Tangier disease) Hypolipoproteinemia Hypobetalipoproteinemia/LDL (Abetalipoproteinemia, Apolipoprotein B deficiency) Lipodystrophy Barraquer-Simons syndrome transport: Carnitine (Primary, I, II, -acylcarnitine) Adrenoleukodystrophy Fatty acid metabolism deficiency beta oxidation: Acyl CoA dehydrogenase (Short-chain, Medium-chain, Long-chain 3-hydroxy, Very long-chain) - Mitochondrial trifunctional protein deficiency to acetyl-CoA: Malonic aciduria Cholesterol synthesis Smith-Lemli-Opitz syndrome Other Sjögren-Larsson syndrome - Lipomatosis - Adiposis dolorosa see also lipid metabolism enzymes, lipoprotein metabolism