Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
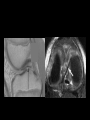
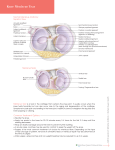
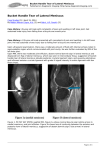
Basic Knee Imaging RSSA Durban 2008 Richard de Villiers Van Wageningen and Partners Aims • Anatomy of the Meniscus • Imaging protocol Terminology • Speak the same language as your referrer • Keep up to date with the relevant terminology Anatomy • Meniscal anatomy • Attachments Basic anatomy Medial meniscus Lateral meniscus Morphology • Wedge-shaped • Semilunar ( C -shaped) • Surface – Superior • concave – Inferior • flat • Fibrocartilage (collagen fibres) • Fibres – superficial – circumferential hoop – radial tie A.Superficial layer a ° °° ° °° ° ° °° ° ° ° °°° ° °°°° ° °°°° ° ° °°°°° ° ° ° °°° °°° °°°° ° ° ° °°°°° °°° ° °°° °° ° °° ° ° ° ° ° °° ° ° ° ° °°°° ° ° °° ° ° ° ° ° °° ° ° mesh-like matrix of fine fibrils measuring 100μ Superficial layer a 100 micrometre B.Circumferential hoop fibres b ° °° ° °° ° ° ° °° °° °°° ° °°°° ° °°°° °°° °°°°° ° °°°°°°° °°°° ° ° ° °°°°°° °° ° °°° ° ° ° °° ° °° ° ° °° ° ° ° ° °°°° ° °°° ° ° ° ° ° °° ° ° c rope-like collagen fibre bundles c. smaller radial fibres - reeinforcement a b C. Radial Tie fibres b ° °° ° °° ° ° ° °° °° °°° ° °°°° ° °°°° °°° °°°°° ° °°°°°°° °°°° ° ° ° °°°°°° °° ° °°° ° ° ° - reinforcement °° ° °° ° ° °° ° ° ° ° °°°° ° °°° ° ° ° ° ° °° ° ° c Terminology Red-white zone Free edge Menisco-capsular junction Peripheral zone Central zone (outer) Inner Red zone White zone Vascularity – From the genicular vessels – Extent • Medial (10-30% of width) • Lateral (10-25% of width) Arnoczky SP (1992) In: Mow VC, Arnoczky SP, Jackson DW (Eds) Knee meniscus: Basic and clinical foundations. Raven Press, New York Zones Relevance – If tear involves outer, vascular 1/3 (3-5 mm from capsule) • Surgical repair / or conservative – If tear involves inner,non-vascular 1/3 • Partial / total meniscectomy Medial Meniscus • Size (AH < PH) – AH ( 7.6 mm) – Body ( 9.6 mm) – PH ( 10.6mm) Lateral meniscus • Size ( AH = PH) – AH (10.2 mm) – Body (11.6 mm) – PH (10.6 mm) Attachments Menisci maintained in optimal position Various direct and indirect attachments to the tibia and femur. Peripheral attachments to capsule Medial Meniscus • Attachments – AH • Transverse ligament • Anterior root ligament – Body (capsular) • Meniscofemoral • Meniscotibial ( coronary) • Minor capsular attachments – PH • Posterior root ligament Radiologist attending this lecture according to the attendance register Lateral meniscus • Attachments – AH • Transverse meniscal ligament • Root ligament – Body • Capsular ligaments – Superior and inferior – To ITB – NOT attached to the LCL – PH • Meniscofemoral ligaments – Humphrey and Wrisberg • Popliteomeniscal ligaments – Meniscal struts • Root ligament Transverse meniscal ligament • The menisci are attached to each other anteriorly by the transverse ligament • 44 - 58 % incidence Transverse ligament Transverse meniscal ligament Root attachments Cannabis sativa – Durban Poison • • • Critical attachment sites to the central tibial plateau. Resist hoop stress Well-defined relations to each other and to the cruciate ligament insertions • The Meniscal Roots: Gross Anatomic Correlation with 3-T MRI Findings Am. J. Roentgenol., May 2007; 188: W446 - W450 Jeffrey M. Brody, Michael J. Hulstyn, Braden C. Fleming, and Glenn A. Tung . Anterior root ligament of MM Anterior root ligament of MM Posterior root ligament of MM Posterior root attachment MM Anterior root ligament of lateral meniscus Posterior root ligament of lateral meniscus Meniscofemoral ligaments • Ligaments of Humphrey and Wrisberg. • Superomedially • Posterior horn of the lateral meniscus to the lateral aspect of the medial femoral condyle. • Name based on their location • Either 70% • Both 6% • Minor role Ligament of Wrisberg • Posterior • Larger • Inserts into the medial femoral condyle. Ligament of Humphrey • Anterior • Smaller • 1/3 of PCL diameter Popliteomeniscal ligaments • Superior and inferior struts • Anchor the posterior horn of the lateral meniscus to the capsule Popliteomeniscal ligaments p MM capsular attachments Meniscotibial/femoral ligaments • MM attached via the deep portion of the MCL and the • meniscofemoral (f) and • meniscotibial (t) ligaments MM Capsular attachments Meniscotibial/femoral ligaments Minor capsular attachments • Periphery of menisci usually attach to capsule via synovial attachments MM synovial attachments to capsule LM to ITB LM not attached to LCL Oblique menisco-meniscal ligament • Normal variant • runs obliquely from the anterior horn of one meniscus to the posterior horn of the opposite meniscus. • 1% to 4% • mimic a meniscal tear Orthopod training to perform meniscectomy MRI Protocols • • • • Our institution 1.5 T Siemens Symphony Dedicated knee coil Well-trained, dedicated MR technicians • • Sagittal, axial and coronal PD/ PDFS – PD for anatomy – PDFS for pathology Occasionally – MR arthrogram ( ? CT > MR) • Post-surgical ? Meniscal retear • Stability of osteochondral lesion • Plica – WE-DESS • 1mm cuts : subtle meniscal & chondral abN • 3D MPR – GRE • Subtle meniscal abN – T1 • Fracture/ tumour – T2 • Ganglion/cyst – PC-T1FS • Synovitis • Infection • Tumour Thank you • www.samsig.co.za