Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
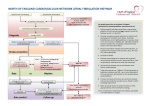
Stroke prevention and risk management for patients with non-valvular atrial fibrillation Dr Bruce Campbell Consultant Neurologist, Head of Hyperacute Stroke Royal Melbourne Hospital University of Melbourne Australia Disclosure: AntiCoagAF app $1.99 - Proceeds to RMH Neuroscience Foundation Key messages – personal viewpoint: Anticoagulants are grossly underutilised in Australia (and worldwide) unnecessary strokes & disability Act of omission vs act of commission discrepancy in prescriber thinking regarding risk-benefit Age discrimination, lack of creativity and effort to circumvent relative contraindications Myths about NOACs versus warfarin Who needs anticoagulation? Mechanical heart valves Deep venous thrombosis/Pulmonary embolism Primary/secondary prevention of ischemic stroke (AF+) Miscellaneous – antiphospholipid syndrome, nephrotic syndrome… Who needs anticoagulation? How much AF is enough? Clinically evident/symptomatic episodes are the tip of the iceberg Paroxysmal AF has similar stroke risk to permanent AF However 30sec of AF on a holter monitor (minimum definition) may have different risk to several hours Spontaneous echo contrast (clot) can develop over ~20mins Who needs anticoagulation? s t n How hard should we look? ie t a p e k -lead ECG After a stroke or TIA the standardtr12 o s n i +/- Holter monitor misses paroxysmal AF! F A y r ta o s f ly tion l a c i ta i n l i i l c hab r 6 months 8.9% o t e i n ng r o m u ri 12 months 12.4% o t d e u 36 months 30.0% in t n Co CRYSTAL-AF Sanna NEJM 2014 Who needs anticoagulation? 2 ≥ Risk stratification for atrial fibrillation: CHADS2 S D CHADS2 HA Annual stroke risk C y l l a C – congestive heart failure atic0 ted 1.9% m i ca o t d1 u n a i 2.8% H – hypertension e n k io o t r t a l A – age >75 ic s agu 2 4.0% m ico e h t c n D - diabetes s a i 3 5.9% . n e . a i r e t S2 Af – previous stroke/TIA 4 8.5% (2 points) Need to review regularly in those not yet taking anticoagulant 5 12.5% 6 18.2% Atrial fibrillation – CHA2DS2-VASc score Lip et al, Chest 2010 ?? Aspirin?? Meta-analysis: 19% reduction in stroke (nonsignificant) Only SPAF-1 showed a significant reduction in stroke (by 42%) but heterogeneity between warfarin eligible and ineligible patients AVERROES trial – apixaban 5mg BD same risk of ICH (0.4%pa) and much more effective (dabigatran rate of ICH similar) NICE (UK) 2014 recommendations: “Do not offer aspirin monotherapy solely for stroke prevention to people with atrial fibrillation.” Warfarin or NOAC/DOAC? Figures obtained by the ABC reveal Pradaxa has been associated with 280 deaths in Australia and 1,400 adverse drug reactions in the past five years, including abdominal bleeding, brain haemorrhages, strokes and heart attacks. By comparison, the older blood-thinning drug Warfarin has been linked to 30 deaths and 270 reactions over the same period – Sophie Scott, ABC News Medical Reporter. Warfarin or NOAC? Warfarin Comment “Tried and tested” Would warfarin be licensed today? “Reversible” Mortality after ICH no different for warfarin vs NOAC despite “reversal” “Able to monitor” NOACS can be monitored but more specialised testing required “Can use if poor renal function” True but bleeding risk increases nonetheless If you are going to use warfarin target INR 2.5 and do not accept INR <2.0! (not protective) Warfarin or NOAC? NOAC Comment “No need for monitoring” Still need to periodically check CrCl “No major food and drug interactions” “Easy adherence” Less than warfarin but there are some Perhaps but if miss doses rapidly unprotected due to shorter half-life Dabigatran: increased effect with strong P-gp inhibitors eg ketoconazole (also amiodarone, verapamil but dose adjustment not recommended), decreased effect with rifampicin Xa inhibitors: increased effect with combined P-gp and CYP3A4 inhibitors - azole-antimycotics (ketoconazole, itraconazole, voriconazole, posaconazole), HIV protease inhibitors (e.g. ritonavir, indinavir, lopinavir) decreased effect with combined P-gp and CYP3A4 inducers - rifampicin, phenytoin, carbamazepine, phenobarbital or St. John’s Wort Evidence for novel anticoagulants Primary/secondary prevention of ischemic stroke in patients with AF: Dabigatran 150mg BD is superior to warfarin in preventing stroke and has a reduced risk of intracerebral hemorrhage. Total major bleeding is higher than warfarin (mostly GI bleeds) Dabigatran 110mg BD is non-inferior to warfarin in preventing stroke and has a reduced risk of bleeding, especially intracerebral hemorrhage. GI bleeding occurred in 1.12%pa vs warfarin 1.02%pa (p=0.43). Rivaroxaban 20mg daily is non-inferior to warfarin in preventing stroke and has a reduced risk of intracerebral hemorrhage. Total major bleeding is similar to warfarin. Apixaban 5mg BD is superior to warfarin in preventing stroke and has a reduced risk of intracerebral hemorrhage. Total major bleeding is lower than warfarin. Apixaban 5mg BD is superior to aspirin in preventing stroke and has similar risk of intracerebral hemorrhage and total major bleeding. Edoxaban 60mg daily is non-inferior to warfarin in preventing stroke and has a reduced risk of major bleeding & intracerebral hemorrhage. Risk-Benefit Consider absolute risk of stroke vs bleeding AND potential consequences of each Source: NPS NB no head to head comparison available Reversibility of warfarin is an illusion In intracerebral hemorrhage even prothrombinex is too slow to prevent growth Mortality is the same for warfarin ICH as NOAC ICH despite “lack of antidote” NOACs much less likely to cause ICH in the first place Antidotes in phase 3 trials – instant reversal Reversal and antidotes? Hart et al Stroke 2012 From RELY ICH rates: Warfarin 0.76%pa 150mg 0.31%pa 110mg 0.23%pa Biggest risk factor for ICH = concomitant Aspirin! Reversal and antidotes ICH rates with Xa inhibitors warfarin Xa aspirin p-value AVERROES - 0.4%pa 0.4%pa 0.69 ARISTOTLE 0.8%pa 0.33%pa <0.001 ROCKET-AF 0.7%pa 0.5%pa 0.02 RELY 0.74%pa 150mg BD 0.3%pa 110mg BD 0.23%pa (p<0.001) Xa antidote and anti-dabigatran Fabfragment antidote now in phase 3 trials major bleeding Fatal bleeding Intra-cranial bleeding Clinically relevant non-major bleeding Age discrimination - efficacy vs bleeding Dabigatran post-hoc data: Stroke Warfarin DBG 110 DBG 150 Age <75 1.43 %/yr 1.32 %/yr 0.90 %/yr Age ≥ 75 2.14 %/yr 1.89 %/yr 1.43 %/yr Extracranial Warfarin bleeding DBG 110 DBG 150 Age <75 2.44 %/yr 1.76 %/yr 1.91 %/yr Age ≥ 75 3.44 %/yr 4.10 %/yr 4.68 %/yr Intracranial Warfarin bleeding DBG 110 DBG 150 Age <75 0.14 %/yr 0.26 %/yr 0.61 %/yr Age ≥ 75 1.00 %/yr 0.37 %/yr 0.41 %/yr NB ICH lower than warfarin regardless of age Eikelboom Circulation 2011 Older patients have higher stroke risk and higher bleeding risk Does lower CrCl alter risk-benefit? Stroke/Systemic Embolism Major Bleeding Hohnloser et al Eur Heart J 2012 Does lower CrCl alter risk-benefit? APIXABAN vs WARFARIN Stroke or Systemic embolism Major Bleeding Hohnloser et al Eur Heart J 2012 Does lower CrCl alter risk-benefit? DABIGATRAN vs WARFARIN – Stroke or systemic embolism Connolly NEJM 2009 Major bleeding Hijazi Circulation 2014 Does lower CrCl alter risk-benefit? Warfarin Dabigatran 110mg Warfarin Dabigatran 110mg Warfarin Dabigatran 150mg Warfarin Dabigatran 150mg Hijazi Circulation 2014 Hijazi Circulation 2014 Does lower CrCl alter risk-benefit? Rivaroxaban vs warfarin Stroke or systemic embolism CrCl (ml/min) Major bleeding CrCl (ml/min) Patel NEJM 2011 When to commence post stroke? No good evidence Balancing risk of hemorrhagic transformation (related to infarct volume) versus recurrent embolism Warfarin generally immediate for TIA 3-6 days for moderate stroke 10-14 days for major stroke – probably similar for NOAC despite immediate action Anticoagulation after ICH?? Any such use is “off-label” Consider if high absolute risk of ischemic stroke (eg CHADS ≥4) and mitigating circumstances eg Context – trauma, high INR etc Uncontrolled hypertension (not if amyloid) Would you use Warfarin vs NOAC vs aspirin? “reversibility” vs risk of ICH vs effectiveness in preventing ischemic stroke When to start antithrombotics after ICH?? Amyloid angiopathy recurrence risk (not on anticoagulation*) ~5.4%/yr (up to 14%/yr in some studies) Hypertensive ICH recurrence risk (not on anticoagulation*) ~2%/yr Bailey Neurology 2001 Amyloid angiopathy recurrence risk: antiplatelet effect prospective cohort 104 lobar ICH patients Biffi Neurology 2010 Absolute risk of ischemic stroke un-anticoagulated: CHADS2 Annual stroke risk 0 1.9% 1 2.8% 2 4% 3 5.9% 4 8.5% 5 12.5% 6 18.2% CHADS2 C – congestive heart failure H – hypertension A – age >75 D - diabetes S2 – previous stroke/TIA (2 points) Starting anticoagulation – my practice NOACs preferred if CrCl acceptable NOACs even more dependent on adherence (short t½) All 3 agents are reasonable choices (no head to head data) If already taking Warfarin and excellent time in therapeutic range reasonable to continue – less ICH with NOAC but NNT ~200pa “warfarin is out… and aspirin is mega-out!” Hans-Christoph Diener Use the correct dose: don’t compromise efficacy Calculate Renal function = CrCl (Cockcroft-Gault, not just eGFR!) Apixaban: 5mg BD unless 2 of age>80, Cr>133μmol/L, wt<60kg 2.5mg BD Do not use if CrCl<25ml/min (27% renal clearance) Dabigatran: 150mg BD unless CrCl 30-50ml/min or age>75 110mg BD Do not use if CrCl<30ml/min (80% renal clearance) Rivaroxaban: 20mg daily unless CrCl 30-50ml/min 15mg daily Do not use if CrCl<30ml/min (35% renal clearance) Maximising safety Control hypertension Avoid concurrent antiplatelets Monitor CrCl, especially if intercurrent illness Take home messages For NVAF patients new to anticoagulation with CrCl>25ml/min why would you use warfarin? For patients “stable” on warfarin consider TTR and weigh the risk of ICH “reversibility” of warfarin after ICH is an illusion Poor renal function with CrCl>25ml/min – apixaban may be safer than warfarin Maintain tight BP control and avoid concurrent antiplatelets Don’t use aspirin for AF tPA and NOACs Known to have taken <12hr = tPA contraindicated Otherwise for dabigatran – check dilute thrombin time (DBG<40ng/mL) For apixaban <10ng/ml/rivaroxaban <100ng/ml on calibrated anti-Xa Or use endovascular therapy (faster…) Peri-operative management First ask if necessary to stop No need to “bridge” with Clexane if NOAC Time off NOAC: renal function surgical bleeding risk Peri-operative management Factor Xa Low risk = stop 24hr pre and * 48hr recommended if CrCl 30-49ml/min restart 24hr post High risk = stop 48hr pre and * 72hr recommended if CrCl 30-49ml/min restart 48hr post Apixaban: Ward 2013, Thrombosis J * Tran IMJ 2014 Peri-operative management Dabigatran: CrCl (ml/min) estimated t½ high risk standard risk >80 13hr 48hr 24hr 50-80 15hr 48-72hr 24-48hr 30-50 18hr 4 days 48-72hr Practical Guide to Pradaxa in NVAF, Boehringer Ingelheim