Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
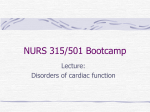
Acta Cardiol Sin 2015;31:461-463 Case Report doi: 10.6515/ACS20150511A Contrast Pooling and Layering in a Patient with Left Main Coronary Artery Occlusion and Cardiogenic Shock Tzu-Chiao Lin,1 Chin-Sheng Lin,1 Hsian-He Hsu2 and Jun-Ting Liou1 A 57-year-old male with type 2 diabetes mellitus presented to the emergency department with sudden onset of chest pain. Shock status and considerably low right arm blood pressure were detected. The patient underwent contrast-enhanced computed tomography (CT) which revealed dependent contrast pooling and layering of contrast material within the inferior vena cava. Post-processing CT angiography depicted total occlusion of the left main coronary artery. Sudden cardiac arrest developed after CT examination, and following emergency coronary angiography we confirmed the diagnosis of left main coronary artery occlusion and cardiogenic shock. Clinical physicians should recognize these CT findings of imminent cardiovascular decompensation and provide prompt medical management to prevent further patient deterioration. Key Words: Cardiogenic shock · Dependent pooling · Layering · Left main coronary artery disease INTRODUCTION partment with sudden onset of squeezing chest pain and cold sweating. Relevant past history was unremarkable except for type 2 diabetes mellitus under treatment with oral anti-diabetic agents for more than 3 years. His blood pressure was 86/54 mmHg, heart rate 64 beats per minute, respiratory rate 24 breaths per minute, and SaO2 of 93% when using ambient air. Physical examination revealed a regular heart beat without audible murmur, and crackle breathing sounds at bilateral basal lung fields. In addition, the patient had lower right arm BP (59/23 mmHg) as compared to his other limbs. A 12-lead electrocardiogram showed normal sinus rhythm with ST segment elevation at lead aVR, and ST segment depression at leads II, III, and aVF (Figure 1A). Transthoracic echocardiogram demonstrated severe generalized hypokinesia of the left ventricle with ejection fraction about 20% and mild aortic regurgitation. Due to only limited time for adequate diagnosis and further management, contrast-enhanced CT was first considered for the emergency. This imaging excluded aortic dissection but revealed dependent contrast pooling and layering of contrast material and blood within the inferior vena cava (Figure 1B, 1C). Moreover, post- Computed tomography (CT) is an important and popular diagnostic tool. Cardiogenic shock is defined as decreased cardiac output leading to circulatory failure and tissue hypoperfusion. We present a rare case of documented left main coronary artery total occlusion with characteristic CT features of imminent cardiogenic shock. CASE REPORT A 57-year-old man presented to the emergency de- Received: May 2, 2014 Accepted: May 11, 2015 1 Division of Cardiology, Department of Medicine; 2Department of Radiology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan. Address correspondence and reprint requests to: Dr. Jun-Ting Liou, Division of Cardiology, Department of Medicine, Tri-Service General Hospital, No. 325, Section 2, Cheng-Kung Road, Neihu 114, Taipei, Taiwan. Tel: 886-2-8792-7160; Fax: 886-2-6601-2656; E-mail: ljtmail @gmail.com 461 Acta Cardiol Sin 2015;31:461-463 Tzu-Chiao Lin et al. A B C D Figure 1. (A) A 12-lead electrocardiogram revealing ST segment elevation in lead aVR and ST segment depression in lead II, III, and aVF. (B) Contrast-enhanced Computed tomography (CT) demonstrating dependent venous pooling of contrast material in dependent hepatic veins (arrow) and inferior vena cava (IVC). (C) Venous pooling and layering of contrast material within superior vena cava, right atrium of heart, inferior vena cava (arrow), and other dependent venous structures (arrow head). (D) CT angiogram illustrating total occlusion of left main coronary artery (LMCA) (arrow). processing CT angiography depicted total occlusion of the left main coronary artery (LMCA) (Figure 1D). Sudden cardiac arrest occurred subsequent to the patient’s CT examination. Aggressive resuscitation efforts were applied, along with intra-aortic balloon pump counterpulsation, emergent cardiac catheterization and digital subtraction coronary angiography. This intervention and its associated procedures confirmed the diagnosis of LMCA total occlusion (Figure 2A, 2B). However, the patient expired despite temporary revascularization of LMCA by balloon dilatation. A B Figure 2. (A) Digital subtraction coronary angiogram revealing total occlusion over LMCA (arrow). (B) After emergent percutaneous coronary intervention, TIMI 1 flow over left anterior descending coronary artery and left circumflex coronary artery were noted. Abbreviations are in Figure 1. DISCUSSION shock status should receive surgery immediately. In the current report, we presented a case of LMCA disease with cardiogenic shock who was initially misdiagnosed as AAS. Moreover, we demonstrated the rare CT images of dependent venous contrast pooling as signs of documented total occlusion of LMCA, cardiogenic shock and markedly depressed cardiac output. In patients with acute chest pain and shock status, it is important and usually a diagnostic challenge to differentiate acute coronary syndrome (ACS) from acute aortic syndrome (AAS), since the treatment strategies for these two disease are completely different. In contrast to patients with ACS, who typically require primary percutaneous coronary intervention, patients with AAS and Acta Cardiol Sin 2015;31:461-463 462 CT Manifestation of Cardiogenic Shock images.2-4 Thus, dependent venous pooling implies cardiac pump dysfunction which involves a failure to propel blood against gravity. In conclusion, we demonstrated the rare CT features of a case of LMCA disease with cardiogenic shock. The contrast-enhanced CT findings of dependent venous contrast pooling and contrast-blood layering suggest signs of cardiogenic shock and carry a very poor prognosis for the patient. Clinicians should be notified immediately and provide prompt medical management to avoid a catastrophic outcome. There have been a scant few reports regarding the CT features of cardiogenic shock.1-4 The underlying lethal disease of these patients includes aortic dissection, trauma with massive bleeding, intra-abdominal infection with septic shock, and acute myocardial infarction with cardiogenic shock.1-4 Typical CT features in these shock patients demonstrated contrast collecting in the dependent portion of the superior vena cava and the inferior vena cava (IVC), forming a blood-contrast level.1 Moreover, the retrograde contrast from IVC to the right hepatic vein, which then densely opacified the right lobe liver parenchyma.1 With normal physiological flow, specific gravity has little effect on the contrast agent dynamics. However, in patients with cardiogenic shock, both arterial and venous blood flows dramatically decrease, and even stop. Contrast agents are heavier than blood and tend to accumulate in the dependent parts of the venous system. Under such circumstances, the distribution of the contrast agent depends largely on its density and specific gravity, as well as the injected volume and duration.1 Therefore, most of the injected contrast agents in these patients are found in the superior vena cava, the inferior vena cava, and the dependent parts of the body, including the organs and vessels, causing venous pooling and layering of contrast material in contrast-enhanced CT REFERENCES 1. Tsai PP, Chen JH, Huang JL, Shen WC. Dependent pooling: a contrast-enhanced sign of cardiac arrest during CT. AJR 2002;178: 1095-9. 2. Roth C, Sneider M, Bogot N, et al. Dependent venous contrast pooling and layering: a sign of imminent cardiogenic shock. AJR Am J Roentgenol 2006;186:1116-9. 3. Jana M, Gamanagatti SR, Kumar A. Case series: CT scan in cardiac arrest and imminent cardiogenic shock. Indian J Radiol Imaging 2010;20:150-3. 4. Bagheri SM, Taheri MS, Pourghorban R, Shabani M. Computed tomographic imaging features of sudden cardiac arrest and impending cardiogenic shock. J Comput Assist Tomogr 2012;36: 291-4. 463 Acta Cardiol Sin 2015;31:461-463