Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
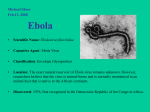
ISARIC/WHO Teleconference January 15, 2015 Treating the Host Response to Ebola Virus Disease David S. Fedson, MD [email protected] The Challenge of Managing Patients with Ebola Virus Disease in West Africa • Almost 10,000 Ebola patients are known to have died • The outbreak has been partially controlled in some regions, but the end is not in sight • Public health efforts will be essential for outbreak control • Clinical management of individual Ebola patients has been difficult (CFR 40-70%) and dangerous • “Top down” interventions that target the virus (vaccines, antivirals, antibody treatments) are experimental, in very short supply, and will not have a major impact on the management of individual patients in the foreseeable future • A “bottom up” approach using safe and inexpensive generic drugs to treat the host response of all patients with Ebola virus disease is available in West Africa today and might save lives Treating the Host Response to Ebola Virus Infection in Sierra Leone: First Steps • Op-Ed article in The New York Times on August 15th David S. Fedson and Steve M. Opal “Can Statins Help Treat Ebola” • Letter in The Journal of Infectious Diseases published online on August 25th (manuscript) and September 24th Fedson D.S. A practical treatment for patients with Ebola virus disease. J Infect Dis 2015; 211: 611-2. • Dr. Ole Martin Rordam in Trondheim, Norway read the NYT Op-Ed article, bought a supply of atorvastatin (40 mg, 4000 doses), irbesartan (150 mg, 4000 doses) and clomiphene (50 mg, 50 doses), and sent it through a colleague to Sierra Leone • Ebola patients (test-positive) have been treated by local physicians in Freetown, Port Loko, Hastings and perhaps other sites Atorvastatin and Irbesartan Treatment in Sierra Leone - 1 34 Military Hospital in Freetown – early November • • • • • • 22 test-positive patients treated with atorvastatin (40 mg/day) and irbesartan (150 mg/day) 22 test-positive patients treated with irbesartan and clomiphene (50 mg/day); only 50 doses of clomiphene had been supplied Duration of treatment not known; all patients survived One military physician was treated for 3 days and improved, but treatment was changed to an antiviral and convalescent plasma and he relapsed and died On November 11th, following review of this experience by its Expert Committee on Drug Safety, the Pharmacy Board of Sierra Leone sought written guidance on further studies of treatment (subsequent actions not known) Report of 531 patients at the Hastings Ebola Treatment Centre treated with IV fluids with 31% mortality; whether some patients received atorvastatin and irbesartan is not known Ansumana R et al. N Engl J Med 2014. Epub on December 24th. Atorvastatin and Irbesartan Treatment in Sierra Leone - 2 Port Loko Government Hospital – internal memorandum, 27/11/14 “Ten patients tested positive for EVD were commenced on the above therapy while continuing the usual protocol for treatment on 16/11/14. They showed remarkable improvement and five of them have been discharged from the Maforkie Treatment. More patients are on the management and we expect promising results.” • • • • Treatment records show 15 patients were treated orally with atorvastatin (40 mg/day), irbesartan (150 mg/day) and clomiphene (50 mg/day) for three days, and then continued on atorvastatin and irbesartan only for 3-4 more days All 15 patients survived One additional critically ill patient died after receiving only one or two doses of treatment At least ten additional patients at PLGH have been treated, but the results are not known Atorvastatin and Irbesartan Treatment in Sierra Leone - 3 Limitations • • • • Patients apparently treated consecutively, not randomized All patients received atorvastatin and irbesartan, only a few patients received a short course of clomiphene No additional details known (duration of illness before treatment initiated, severity of initial signs and symptoms, other treatments, rapidity of response to treatment) No details known on the selection of patients for treatment and characteristics of those not treated (duration of illness before admission, clinical severity, outcome) Are the clinical results significant? • • • • At least 100 patients have been treated with atorvastatin and irbesartan, with two known deaths To reduce mortality from 50% to 25% (with a significant 95% CI) - RCT 210 subjects - consecutive treatment 55 subjects A matched set case-control study could establish the effectiveness of treatment On January 8, 2015, WHO initiated a review of the treatment experience in Sierra Leone Ebola Virus Disease and Sepsis in Patients: Endothelial Dysfunction and Coagulopathy • Clinical similarities - pro-inflammatory cytokines/chemokines - lymphocyte apoptosis liver and renal abnormalities (MOF) endothelial dysfunction and coagulopathy high mortality Henley LE, Geisbert TW. Thromb Haemost 2005; 94: 254-61. McElroy AK et al. J Infect Dis 2014; 210: 558-66. Opal SM, van der Poll T. J Intern Med 2015. To be published. • Massive fluid losses internally (third spacing) and externally (diarrhea, vomiting), severe electrolyte disturbances, not yet documented in animal models • In sepsis patients, RCT showed atorvastatin reduced the development of MOF by 83% Patel J et al. Crit Care 2012; 16: R231. 7 Hamburg - Abdominal Ultrasound Exam of a Patient with Ebola Virus Disease, Day 10 LIVER normal aspect and size without local lesions, no cholestasis, all liver vessels with orthograde flow SPLEEN normal aspect and size KIDNEYS and both kidneys of normal aspect and size, no obstruction BLADDER of the urinary tract INTESTINAL pronounced edema of the stomach, small intestine TRACT and large intestinal wall. Extremely distended intestinal loops, with large amounts of intra-intestinal fluids and complete absence of peristaltic movement LYMPH NODES mesenteric lymph nodes enlarged ABDOMINAL complete collapse of the inferior vena cava VESSELS OTHER No signs of pericardial effusion, pleural effusion or ascites Kreuls B et al. N Engl J Med 2014; 371: 2394-401. Atlanta - Fluid Balance in Ebola Patient 2 Massive fluid deficits demonstrated over the course of the disease Lyon GM et al. N Engl J Med 2014; 371: 2402-9. Endothelial Barrier Dysfunction in Septic Shock and Virus Infections Opal SM et al. J Intern Med 2015. To be published. Dalrymple NA et al. Curr Opin Virol 2014; 7: 134-40. Ebola, Vascular Permeability, and its Treatment with Statins and Angiotensin Receptor Blockers In vitro mechanistic studies • Atorvastatin inhibits Rho and Rac GTPases, increases VEcadherin and preserves endothelial junction integrity Chen W et al. Am J Physiol Lung Cell Mol Physiol 2008; 295: L575-L583. Xiao H et al. PLoS One 2013; 8: e59233. Non infectious Ebola virus shed glycoprotein increases vascular permeability Escudero-Perez B et al. PLoS Pathog 2014; 10: e1004509. • Angiotensin II increases endothelial permeability, and this is blunted by angiotensin receptor blockade Bodor C et al. Am J Physiol Cell Physiol 2012; 302: C267-C276. Molecular Targets of Statins, ACE Inhibitors and ARBs in Endothelial Cells Combined treatment more effective than single agent treatment Lee HY et al. Circ J 2014; 78: 281-7. Ceriello A et al. Circulation 2005; 111: 2518-24. Statins and ARBs: Possible Cell Signaling Effects in Treating the Host Response to Ebola Virus Infection • • • • • • • • • • • • • • • • TLR4, NF-kB and AP-1; p38 MAPK and PI3/Akt (cytoprotective) pro-inflammatory TNF, IL-1b, IL-6, IL-8, MCP1, MIP1/, CCR5 anti-inflammatory IL-10, TGF- pro-resolving mediators lipoxin A4, protectin D-1, resolvin D1 HO-1 TLR signaling for PAMPs, alarmins (DAMPS) cytokines cellular adhesion molecules (VCAM-1, ICAM-1, P-selectin) HMGB1/RAGE and late mediators of inflammation tissue factor, thrombomodulin pro-thrombotic coagulopathy iNOS, eNOS stabilize cardiovascular function adipokines (adiponectin) that decrease inflammation C5a-C5aR-related increase in vascular permeability pulmonary hypertension modify macrophage function, caspase activation (inflammasomes) and autophagy and apoptosis in different cells GSH, NADPH oxidase (NOX) ROS, oxidative stress stabilize endothelial cell actin cytoskeleton and EC adherens junctions endothelial barrier integrity, vascular permeability AMPK/PGC-1 mitochondrial biogenesis, ATP Fedson DS. Antiviral Res 2013; 99: 417-35. Candidates for Treating the Host Response in Ebola Patients with Atorvastatin and Irbesartan • Atorvastatin and irbesartan are known to be safe when given to patients with acute critical illness • Treat all patients with Ebola virus disease - immediately treat all patients suspected of having EVD in ETUs and those cared for at home - continue treatment in those with laboratory-documented infection - discontinue treatment in those who are test-negative when they are not longer considered infected • Prevent complications in those who might become infected - health care workers in ETUs - caregivers of Ebola patients treated at home - community healthcare workers, surveillance staff and burial workers - other close contacts of Ebola patients Treating the Host Response to Ebola Virus Disease: Summary • • • • • Patients with Ebola virus disease in West Africa continue to experience high mortality The central pathophysiological lesion in Ebola patients is the loss of endothelial barrier integrity, primarily in the GI tract Drugs that treat the host response by restoring endothelial barrier integrity could allow patients to live longer, develop their own immune responses, and get rid of the virus Atorvastatin and irbesartan (an angiotensin receptor blocker) - restore endothelial barrier integrity - are safe, inexpensive and widely available generic drugs - dramatically reduced mortality in ~100 consecutively treated patients in Sierra Leone - these treatment results should be validated in a matched set case-control study If found to be effective, atorvastatin and irbesartan would radically alter the management of Ebola virus disease in patients and their close contacts Treating the Host Response to Ebola Virus Disease Thank you Copies of additional slides, an unpublished essay and additional articles are available on request [email protected]