Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Compartmental models in epidemiology wikipedia , lookup
Non-specific effect of vaccines wikipedia , lookup
HIV and pregnancy wikipedia , lookup
Focal infection theory wikipedia , lookup
Public health genomics wikipedia , lookup
Prenatal testing wikipedia , lookup
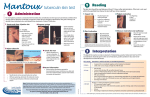
TB Testing Update Lee B. Reichman, MD, MPH Northeastern National TB Center Audio Conference History of Treatment of Latent Tuberculosis Infection For more than 3 decades, treatment of persons with latent Mycobacterium tuberculosis infection to prevent active disease has been an essential component of TB control in the US History of Treatment of Latent Tuberculosis Infection 1965: First recommended for use in the US for previously untreated TB, PPD converters, and all children <3 years with a positive tuberculin test result 1967: Recommendations broadened to include all TST + (>10 mm) and close contacts History of Treatment of Latent Tuberculosis Infection 1970: 2 deaths and 19 developed liver disease out of 2000 contacts exposed to an infectious case on Capitol Hill 1974: Development of guidelines regarding pretreatment screening and monitoring to minimize risk for hepatitis and exclusion of low-risk persons older than 35 as candidates for treatment History of Treatment of Latent Tuberculosis Infection 1983: Guidelines further revised to recommend routine clinical and laboratory monitoring for persons older than 35 or with increased risk for hepatotoxicity 1998: 2 months of RIF + PZA (2RZ) recommended for HIV+, subsequently HIV- 2000: 9 months Isoniazid decreed better than 6 2RZ decreed equal to 9 Isoniazid 2001: 2RZ deemphasized due to liver toxicity in favor of 9 month Isoniazid 2004: 4R suggested as effective advantageous regimen Targeted Tuberculin Testing and Treatment of Latent TB Infection As the rate of active TB in the United States has decreased, identification and treatment of persons with latent infection who are at high risk for active TB have become essential components of the TB elimination strategy Terminology • “Treatment of latent TB infection” replaces the terms “preventive therapy” and “chemoprophylaxis” to promote greater understanding of the concept for both patients and providers. • Targeted tuberculin testing is used to focus program activities and provider practices on groups at the highest risk for TB. Targeted Tuberculin Testing • Detects persons with LTBI who would benefit from treatment • De-emphasizes testing of groups that are not at high risk for TB • Can help reduce the waste of resources and prevent inappropriate treatment What’s New (1) Tuberculin skin testing • Emphasis on targeting persons at high risk • 5-mm induration cutoff level for organ transplant recipients and other immunosuppressed patients being treated with prednisone or TNF-α antagonists4 • Skin-test conversion defined as increase of 10 mm of induration within a 2-year period, regardless of age ____________________________________________________ MMWR August 61, 2004; 53(33): 683-686 What’s New (2) Treatment of LTBI • HIV-negative persons – INH for 9 months preferred regimen • HIV-positive persons and those with fibrotic lesions on chest x-ray (consistent with previous TB) – INH should be given for 9 months • For all persons – RIF for 4 months is an option What’s New (3) Clinical and laboratory monitoring • Routine baseline and follow-up monitoring not required except for – HIV-infected persons – Pregnant women or those in early postpartum period – Persons with chronic liver disease or who use alcohol regularly • Monthly monitoring for signs or symptoms of possible adverse effects Identifying Risk Factors That Lead to Development of TB Disease Persons at Risk for Developing TB Disease Persons at high risk for developing TB disease fall into 2 categories • Those who have been recently infected • Those with clinical conditions that increase their risk of progressing from LTBI to TB disease Recent Infection as a Risk Factor (1) Persons more likely to have been recently infected include • Close contacts to person with infectious TB • Skin test converters (within past 2 years) • Recent immigrants from TB-endemic regions of the world (within 5 years of arrival to the U.S.) Recent Infection as a Risk Factor (2) • Children 5 years with a positive TST result • Residents and employees of high-risk congregate settings (e.g., correctional facilities, homeless shelters, health care facilities) Increased Risk for Progression to TB Disease (1) Persons more likely to progress from LTBI to TB disease include • HIV-infected persons • Those with a history of prior, untreated TB or fibrotic lesions on chest radiograph Increased Risk for Progression to TB Disease (2) • Underweight or malnourished persons • Injection drug users • Those receiving TNF-α antagonists for treatment of rheumatoid arthritis or Crohn’s disease Increased Risk for Progression to TB Disease (3) • Persons with certain medical conditions such as – Silicosis – Diabetes mellitus – Chronic renal failure or on hemodialysis – Solid organ transplantation (e.g., heart, kidney) – Carcinoma of head or neck – Gastrectomy or jejunoilial bypass Risk Assessment Tools With renewed emphasis on targeted tuberculin testing, the use of a risk assessment tool, such as a questionnaire, is one way to help TB Programs direct their resources and focus their efforts Tuberculin Testing Testing for M. tuberculosis Infection Mantoux tuberculin skin test (TST) Skin test that produces delayed-type hypersensitivity reaction in persons with M. tuberculosis infection QuantiFERON® -TB test and QuantiFERON® Gold Blood test that measures and compares amount of interferon-gamma (IFN-) released by blood cells in response to antigens Mantoux Tuberculin Skin Test • Preferred method of skin testing for M. tuberculosis infection • TST is useful for – Determining how many people in a group are infected (e.g., contact investigation) – Examining persons who have symptoms of TB • Multiple puncture tests (e.g., Tine Test) are inaccurate and not recommended Administering the TST • Inject 0.1 ml of 5 TU PPD tuberculin solution intradermally on volar surface of lower arm using a 27-gauge needle • Produce a wheal 6 to 10 mm in diameter • Reading the TST (1) • Measure reaction in 48 to 72 hours • Measure induration, not erythema • Record reaction in millimeters, not “negative” or “positive” • Ensure trained health care professional measures and interprets the TST result Reading the TST (2) • Educate patient and family regarding significance of a positive TST result • Positive TST reactions can be measured accurately for up to 7 days • Negative reactions can be read accurately for only 72 hours TST Interpretation (1) 5-mm induration is interpreted as positive in • HIV-infected persons • Close contacts to an infectious TB case • Persons with chest radiographs consistent with prior untreated TB TST Interpretation (2) 5-mm induration is interpreted as positive in (cont.) • Organ transplant recipients • Other immunosuppressed patients (e.g., those taking the equivalent of >15 mg/d of prednisone for 1 month or those taking TNFα antagonists) TST Interpretation (3) 10-mm induration is interpreted as positive in • Recent immigrants • Injection drug users • Residents or employees of congregate settings • Mycobacteriology laboratory personnel TST Interpretation (4) 10-mm induration is interpreted as positive in (cont.) • Persons with clinical conditions that place them at high risk • Children < 4 years; infants, children, and adolescents exposed to adults at high-risk TST Interpretation (5) 15-mm induration is interpreted as positive in • Persons with no known risk factors for TB.* ____________________________________________________ *Although skin testing programs should be conducted only among highrisk groups, certain individuals may require TST for employment or school attendance. Diagnosis and treatment of LTBI should always be tied to risk assessment Factors that May Cause False-Positive and False-Negative Reactions to the Tuberculin Skin Test Type of Reaction Possible Cause False-positive Nontuberculous mycobacteria BCG vaccination False-negative Anergy Recent TB infection Very young age: < 8 mos. old Live-virus vaccination Overwhelming TB disease BCG – Fantasy and Fact FANTASY FACT • BCG protects against getting TB infection •BCG will not protect against becoming infected with TB • BCG provides lifetime protection against developing active TB •BCG protects against severe complications of TB disease in young children, but provides little or no protection in adolescents and adults • BCG causes the tuberculin skin test (TST) to be positive for life •BCG causes the TST to be positive for a few years and then the TST reaction becomes much weaker. Generally, no reaction is present after 5 years • In a BCG-vaccinated person, a positive TST result is most likely due to BCG •There is no way to tell whether a positive TST result is due to BCG or to TB infection • A positive TST result in a person of any age from any country is most likely due to BCG, not TB infection •A positive TST result in an adolescent or adult from a TB high-burden country is almost always due to TB infection, not BCG • There is no need for a BCG-vaccinated person with a positive TST result to be treated •Persons from countries with high TB burden are at risk of developing active TB and should be treated BCG Vaccine and TB Testing (1) • Many have a history of bacille Calmette-Guèrin (BCG) vaccination in infancy, and a blind faith in their vaccination seems to prevent them from availing themselves of treatment for latent TB infection to prevent active TB • Since the 1920's, BCG has been given to children in developing countries, including most on the current World Health Organization (WHO) list of TB "hot spots" • Approximately 100 million children receive BCG annually, and most experts agree that it is highly variable in protecting adults against TB NEJM 2002; 347:1453-1454 BCG Vaccine and TB Testing (2) • Tuberculin reactions from BCG given in infancy invariably wane within five years • No method can reliably distinguish tuberculin reactions caused by BCG from those caused by natural mycobacterial infections • "A positive reaction to tuberculin in BCG vaccinated persons indicates infection with M.tuberculosis when the person tested is at increased risk for recent infection" NEJM 2002; 347:1453-1454 Boosting • Some people with LTBI may have negative skin test reaction when tested years after infection • Initial skin test may stimulate (boost) ability to react to tuberculin • Positive reactions to subsequent tests may be misinterpreted as a new infection Two Step Testing Use two step testing for initial skin testing of adults who will be retested periodically • If first test positive, consider the person infected • If first test negative, give second test 1-3 weeks later • If second test positive, consider person infected • If second test negative, consider person uninfected The Elderly: A Special Population TB in the Elderly (1) Most commonly due to reactivation of previously dormant pulmonary foci related to TB exposure earlier in life TB in the Elderly (2) • Boosting is more common in those 55 years of age, but is unusual after the age of 75 years • Two-step method should be used whenever a TB skin test will be repeated periodically for example residents or employees of LTCF that care for the elderly TB in the Elderly (3) • Efforts to carefully select and monitor patients who may be candidates for treatment of LTBI • Current evidence favors treatment of LTBI in elderly individuals who are at increased risk for developing TB disease TB in the Elderly (4) Monitoring should include • Baseline liver function tests • Repeat LFTs to monitor hepatotoxicity • Assess monthly for signs and symptoms of liver toxicity ® QuantiFERON Tests QuantiFERON®-TB Test and QuantiFERON®-Gold Test (1) • Whole-blood test used to detect M. tuberculosis infection • Approved by the U.S. Food and Drug Administration (FDA) • Entails mixing blood samples with antigens from M. tuberculosis, M. avium complex, and controls and incubating for 16 to 24 hours QuantiFERON®-TB Test and QuantiFERON®-Gold Test (2) • Cells that recognize the antigen release interferon- • Amount of interferon released in response to tuberculin is compared to amount released in response to other antigens5 ____________________________________________________ MMWR January 31, 2003; 52 (RR-02): 15-18 and CDC Fact Sheet Document # 250103, March 2003 Comparison of QFT and TST QFT TST • In vitro test • In vivo test • Specific antigens • Single antigen • No boosting • Boosting • 1 patient visit • 2 patient visits • Minimal inter-reader variability • Inter-reader variability • Results possible in 1 day • Results in 2-3 days • Requires phlebotomy All testing activities should be accompanied by a plan for follow-up care LTBI Treatment for TST (+) Contacts n = 1725 n = 58 n = 11 Marks, Taylor, Qualls, et al: Outcomes of TB Contact Investigations, AJRCCM, Dec. 2000 n = 132 n = 721 Summary • Targeted testing = testing only those with risk factors • Treatment of LTBI is an essential TB control strategy • A decision to test is a decision to treat INFORMATION LINE 1 • 800 • 4 TB DOCS 1 • 800 • 482 • 3627 www.umdnj.edu/ntbcweb