Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
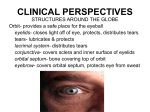
Chapter 7: The Eyelids and the Lacrimal System Updated August 2008 I. Structure and Function of the Eyelids A) Tarsal plates provide structural rigidity for the eyelids 1. tarsal plates- in upper and lower eyelids 2. tarsal portion- the part of the upper or lower lids that contain the tarsal plates 3. septal portion- in front of the orbital septum i. superior: part of the lid from the top of the superior tarsal plate to the orbital rim ii. inferior: part of the lid from the bottom of the inferior plate to the orbital rim 4. palpebral furrows i. superior and inferior ii. folds in the skin of the lid that mark the division between the tarsal and septal portions of the lid B) The tarsal plates are made of meibomian glands embedded in dense connective tissue 1. tarsal (meibomian) glands i. one individual gland looks like a “grapevine” with a central branch and bunches of grapes along the central branch ii. “central branch” = central collecting duct iii. “bunches of grapes” = secretory lobules made of clusters of secretory cells iv. secretes lipids (oily secretion) to coat the lid margins and form thin lipid layer on top of tear film 2. COMMON Pathologies (a) internal hordeolum - acute infection of tarsal gland that causes the gland’s duct to become clogged, produces swelling on inner side of lid- usually near the lid margin (b) chalazion - abnormal accumulation of cells within the tarsal glands, produces prominent bulge on inner and outer lid surface C) Contraction of muscles inserting onto or near the edges of the tarsal plates OPEN the palpebral fissure (opens the eyelids) 1. levator (palpebrae superioris) i. striated muscle ii. contraction elevates upper eyelid iii. origin: apex of orbit on sphenoid bone iv. insertion: not on bone- muscular portion ends behind orbital margin and expands into the connecting tendon called the levator aponeurosis v. innervated by occulomotor nerve SPECIAL NAME For the connecting Tendon (levator aponeurosis) broad, flat tendon expands entire width of upper lid insertion: anterior edge of superior tarsal plate and orbicularis muscle in front of tarsal plate 2. superior tarsal muscle (of Müller) i. smooth muscle ii. contraction elevates upper eyelid iii. located behind levator aponeurosis and extends to upper edge of superior tarsal plate iv. no origin or insertion on bone- located within the levator v. innervation: sympathetic nervous system 3. inferior tarsal muscle (of Müller) i. smooth muscle VS 112 Ocular Anatomy UAB School of Optometry Page 1 of 8 ii. iii. contraction depresses lower eyelid extends from bottom edge of inferior tarsal plate to connective tissue surrounding inferior oblique and inferior rectus muscles iv. no origin or insertion on bone v. innervation: sympathetic nervous system 4. superior transverse ligament (Whitnall’s ligament) i. connective tissue sling that supports levator ii. extends between junction of levator muscle and levator aponeurosis from posterior edge of lacrimal fossa (lateral) to trochlea (medial) 5. ptosis i. drooping of upper lid ii. caused by loss of tone in levator or superior tarsal muscle D) Contraction of orbicularis muscle CLOSES the palpebral fissure 1. orbicularis oculi i. extends over entire orbital opening and beyond the orbital margins onto the face ii. origin and insertion in connective tissue iii. pretarsal portion- in front of (anterior to) tarsal plates iv. preseptal portion- edge of tarsal plate to orbital margin v. palpebral portion- pretarsal and preseptal portions vi. orbital portion- past orbital rim onto brow and cheek regions of face vii. marginal/ciliary portion (muscle of Riolan)- adjacent to lid margin viii. innervation: facial nerve 2. medial palpebral ligament i. actually a tendon because connects muscle to bone- aka medial canthal tendon ii. attaches orbicularis on medial orbit to frontal process of maxilla 3. lateral palpebral ligament i. like medial palpebral ligament, actually a tendon because connects muscle to bone- aka lateral canthal tendon ii. attaches orbicularis on lateral orbit to zygomatic bone on lateral orbital (Whitnall’s) tubercle 4. lateral palpebral raphe- horizontal line formed by interlaced ends of fiber bundles from upper and lower lids at lateral palpebral ligament E) Blinking is a reflex response or a regular, spontaneous action 1. Caused by relaxation and inhibition of levator followed by contraction of orbicularis i. Involves only the palpebral portions of the orbicularis 2. Bell’s phenomenon i. Rotation of eye up and out during voluntary lid closure ii. Uncertain significance – may or may not be diagnostic of pathology iii. “Bell's phenomenon is a normal defence reflex present in about 75% of the population, resulting in elevation of the globes when blinking or when threatened (try touching your cornea with your finger, for example). It becomes noticeable only when the orbicularis muscle becomes weak as in, for example, bilateral facial palsy associated with the GuillainBarré syndrome. It is, however, present behind forcibly closed lids in most healthy people and should not be regarded as a pathognomonic sign.” From British Medical Journal Oct 2001. 3. Reflex blinks i. Caused by sensory stimuli ii. Upper lid closes palpebral fissure completely VS 112 Ocular Anatomy UAB School of Optometry Page 2 of 8 iii. Fast- 150-200 ms 4. Spontaneous blinks i. Occur every few seconds ii. Upper lid does not close palpebral fissure completely iii. Upper lid moves slower than reflex blinks- 250-300 ms iv. Move tears across the cornea 1. Vertical lid movement- upper lid lowers and moves tears vertically 2. Horizontal lid movement- lower lid shifts medially and moves tears horizontally F) Overaction of the orbicularis may appear as blepharospasm or as entropion 1. blepharospasm i. uncontrollable, forceful, involuntary closure of lids ii. treatment 1. eliminate source of irritation in facial nerve 2. block release of neurotransmitter at neuromuscular junction a. ex. Botulinum A toxin- blocks release of synaptic vesicles at terminal end of axon, therefore reduces acetylcholine in synaptic cleft; lasts several months 2. entropion i. inward rotation of lid margins ii. brings lashes in contact with cornea- painful and causes abrasion of cornea, which can lead to further infection iii. most commonly caused by sustained contraction of preseptal portion of orbicularis G) Paresis (weakness) of the orbicularis produces ectropion and epiphora 1. ectropion i. chronic eversion of lower lid ii. consequences 1. improper movement of tears 2. dessication of cornea 3. epiphora 2. epiphora i. accumulation of tears, which spill over lid margin onto face ii. causes ulceration of skin tissue under eye H) Eyelashes and associated glands 1. cilia i. eyelashes ii. protective 2. glands of Zeis i. small within eyelid ii. produce oil secretion to coat lashes and help with catching dust iii. external hordeolum (stye) 1. infected gland of Zeis 2. bulge on outer surface of lid 3. spontaneous recovery or antibiotic 3. glands of Moll i. sweat glands of eyelid VS 112 Ocular Anatomy UAB School of Optometry Page 3 of 8 ii. ducts empty onto lid margins external to cilia I) The skin on the lids is continuous with the conjunctiva that lines the posterior surface of the lids and covers the anterior surface of the sclera 1. conjunctiva i. tissue with nonkeratinized epithelium overlying connective tissue substrate/stroma ii. analogous to epidermis and dermis of skin 2. palpebral conjunctiva i. lines posterior surface of eyelid ii. reflects back to cover anterior sclera and cornea 3. fornix conjunctiva i. fold behind each lid ii. prevents objects, such as contacts, from getting into back of the eye 4. bulbar and limbal conjuctiva- covers anterior part of eye ball 5. goblet cells i. mucus-secreting apocrine glands interspersed between epithelial cells of conjunctiva ii. greatest density in fornix iii. secretes bottom mucin layer of tear film J) Orbital Septum 1. continuous, flexible connective tissue sheet that extends from the orbital rim to the tarsal plates – lateral edge is described differently in various anatomy and oculoplastic articles and books as Either attached to the edge of the margin OR fused with the lateral palpebral ligament (LPL) and attached to the lateral orbital tubercle (Whitnall’s). The LPL is a rather weak flimsy structure. 2. keeps in orbital fat 3. effectiveness is function of heredity and decreases with age 4. blepharochalasis- bulging of upper lid from orbital fat pushing through weakened orbital septum 5. dermatochalasis- folding and bulging of excess skin on lid surface K) Palpebral fissure variations between sexes, races, and individuals 1. plica semilunaris i. lies in medial canthus ii. crescent, moon-shaped bulge of conjunctiva iii. vestigial iv. contains small glands 2. lacrimal caruncle i. lies in medial canthus ii. small tissue bulge on top of plica semilunaris iii. vestigial iv. contains small glands and fine cilia 3. epicanthal fold (epicanthus) i. fold of skin that covers plica semilunaris and lacrimal caruncle until late in gestation ii. retained in Asians/generally lost in Caucasians and African Americans L) “The Big Picture” 1. Septal portion of upper lid (tissues from outside to inside) VS 112 Ocular Anatomy UAB School of Optometry Page 4 of 8 Thin epidermis → dermis → orbicularis → loose connective tissue → orbital septum → levator aponeurosis → superior tarsal muscle → palpebral conjunctiva 2. Tarsal portion of upper lid i. Thin epidermis → dermis → orbicularis → connective tissue and end of levator aponeurosis → tarsal plate → palpebral conjunctiva 3. Septal and tarsal portions of lower lids the same except no levator aponeurosis i. II. Tear Supply and Drainage A. Most of the tear fluid is supplied by the main lacrimal gland 1. The lacrimal gland is located in the upper lateral portion of the orbit 2. It is partially divided by the levator aponeurosis into two connected lobes; a larger lobe lying next to the frontal bone in the lacrimal fossa and a smaller palpebra lobe 3. The gland consists of acini (lobules of secretory clusters) 4. Several cell types are present in the secretory clusters, including myoepithelial cells and lymphocytes with occuluding junctions and nerve terminals. 5. The lacrimal gland produces 1μL per minute or 1.5mL per day B. Secretion by the lacrimal gland is regulated by autonomic inputs operating through a second messenger system 1. Secretion of the lacrimal gland appears to be affected by the release from the parasympathetic axon terminals including acetylcholine, neuromodulatory peptides (VIP). 2. The secretory cells membranes have G-protein linked receptors. 3. The G-protein can be considered as a messenger, whose activation prompts it to seek out and activate intracellular enzymes systems involved in the production of secretory products of the cell C. The composition of the lacrimal gland secretion varies with the secretion rate 1. Most of the proteins produced by the lacrimal gland cells are regulated proteins who are not secreted as they are formed but are stored in the vesicles 2. Constitutive proteins are not subject to external regulation and their rates of production and secretion are intrinsic to the cell D. Dry eye may result from a decreased amount of tears, abnormal tear composition, or both 1. Dry eye (loss of eye moisture) refers to a variety of disorders of the ocular tears experienced as sensations of dryness of the eyes, discomfort, or presence of a foreign object. 2. Numerous potential causes i. Lower aqueous tear production ii. Break up of tear fluid due to improper mix of mucus (goblet contribution), or oil layer (inadequate production of meibomian glands) 3. Severe discomfort due to exposure of nerve endings of cornea 4. Poor vision due to surface irregularities. 5. Keratoconjunctivitis sicca, the most common form of dry eye, is due to a decreased aqueous component in tears. 6. Secretion by the lacrimal gland declines with age; dry eye is more common in older women. 7. An aggressive method for treating dry eye requires blocking normal tear drainage. This involves blocking the puncta so that the reduced supply of tears is not drained VS 112 Ocular Anatomy UAB School of Optometry Page 5 of 8 away so quickly. The inferior punctum can be blocked with a removable silicon plug. E. Tears are drained off at the medial canthus and deposited in the nasal cavity. 1. Tears enter the puncta on the upper and lower lid margins, flowing through the canaliculi to the lacrimal sac. 2. The initial course of the canaliculi from the puncta is vertical, for about 2 mm, to the expanded regions (the ampullae), from which the canaliculi run horizontally to the sac. 3. Tears in the lacrimal sac drain down through the nasolacrimal duct into the nasal cavity. 4. In summary, there are two tubes (the canaliculi) bringing tears away from the lid margins, lacrimal sac collecting the tears, and the nasolacrimal duct depositing the collected tears into the nasal cavity. 5. A flap of tissue at the nasal end of the duct, the valve of Hasner, may prevent the movement of fluid and air from the nasal cavity to the drainage system. Hasner’s valve usually allows free flow of tears from the nasolacrimal duct into the nasal cavity. However, when pressure builds up in the nasal cavity during sneezing or coughing, the pressure differential between the nasolacrimal duct and nasal cavity pushes the free end of Hasner’s valve laterally so that it covers the end of the duct and prevents entry of the nasal contents into the duct (prevents backflow of nasal mucus into lacrimal sac). F. Pressure gradients created by contraction of the orbicularis during blinks move tears through the canaliculi into the lacrimal sac 1. The lacrimal sac lies next to the rigid bone of its fossa and just behind the strong medial palpebral ligament 2. Contraction of the tarsal and lacrimal (Horner’s muscle) portions of the orbicularis should compress the sac; relaxation of the muscles should permit the sac to expand 3. Drainage during blinks – blinking results in contracting and squeezing facilitating tear drainage. Stages of mechanical facilitation of tear fluid removal by blinking: i. Prior to a blink the drainage system is fully open and no pressure gradient exists within the system. ii. During the lid-closing phase of the blink, the puncta meet and close, and the canaliculi ad the lacrimal sac are compressed by contraction of the tarsal and lacrimal portions of the orbicularis. This compression produces positive pressure that move tears into the nasolacrimal duct to the nasal cavity. iii. As the lids reopen, the canaliculi and lacrimal sac expand before the puncta open, creating negative pressure within the system. This negative pressure sucks tears through the puncta into the canaliculi and lacrimal sac when the puncta separate as the lids continue to open. iv. As the blink ends, the puncta reopens and fluid flows into the puncta and canaliculi. III. Formation of the Eyelids and the Lacrimal System A. The eyelids first appear as folds in the surface ectoderm, which gives rise to the lid glands 1. During the first 7 weeks of gestation, the lids appear as small folds in the surface ectoderm; the folds become more pronounced during the next week, and mesoderm moves into the interior of the folds. VS 112 Ocular Anatomy UAB School of Optometry Page 6 of 8 2. The upper and lower lid margins meet and fuse during the eighth week. 3. The eyelash follicles and glands bud from the surface ectoderm, with the follicles appearing first, at about 9 weeks, followed by Moll’s glands, the tarsal glands, and Zeis’s glands 4. The eyelashes protrude from the follicles during the sixth month, and adhesions between the lid margins begin to breakdown B. The lacrimal gland and the lacrimal drainage system derive from surface ectoderm, either as several separate groups of cells or as a single, continuous column of cells. C. Most developmental anomalies of eyelids and lacrimal system are problems in lid position or blockage of the drainage channels D. Anomalous innervation can produce eyelid movement linked to contraction of the muscles in the jaw. 1. In some individuals, movements of the mandible when chewing are associated with rapid movement of one eyelid. This phenomenon, Marcus Gunn’s syndrome, also called jaw-winking, is most noticeable in infants; it may persist into adulthood, but often with diminished intensity. 2. The phenomenon is normally unilateral and accompanied by ptosis on the affected side. 3. Marcus Gunn’s syndrome is explained by an anomalous pattern of innervation affecting the levator and the pterygoid muscles of the mandible. BLOOD SUPPLY: Facial & Maxillary Arteries (off External Carotid Artery) Facial Artery: Angular Artery = branch off Facial Artery that helps supply the Palpebral Arcades. Maxillary Artery: Infraorbital Artery = branch off the Maxillary Artery that helps supply the Palpebral Arcades. Enters the orbit via Inferior Orbital Fissure. Exits the orbit via Infraorbital Canal – will supply blood to cheeks. Ophthalmic Artery (off of Internal Carotid Artery) Supraorbital Artery = one of terminal branches of Ophthalmic Artery. Runs above the eye & passes thru Supraorbital Notch (or Foramen). Supplies the skin and muscles of the upper eyelid, brow & forehead. Dorsal Nasal Artery = one of terminal branches of Ophthalmic Artery. Runs below the trochlea to exit orbit. (a.k.a. Infratrochlear artery) Supplies the eyelid, Lacrimal Sac (including Horner’s Muscle), and the skin and muscle along the nose. Anasthamoses with Angular Artery Medial Palpebral Artery = may be a branch off Ophthalmic Artery or Dorsal Nasal Artery. Supplies blood to the eyelids. At the eyelids – all arteries split up & anasthamose with one another to form the Palpebral Arcades. This will include Medial Palpebral Artery & Lateral Palpebral Artery and Lacrimal Artery. VS 112 Ocular Anatomy UAB School of Optometry Page 7 of 8 Eyelids are also supplied by External Carotid Artery (Facial & Maxillary Artery) branches = Facial Artery & Infraorbital Artery. Lacrimal Artery = one of largest branches off Ophthalmic Artery. Supplies the Lacrimal Gland, Lateral Rectus Muscle, and skin and muscles of upper brow. Gives rise to Lateral Palpebral Artery (which supplies the eyelids). Run through orbit (at Lacrimal Fossa) Lacrimal Gland. VS 112 Ocular Anatomy UAB School of Optometry Page 8 of 8