Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Orphan drug wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
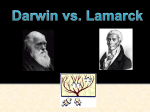
0022-3565/02/3012-698 –704$7.00 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS Copyright © 2002 by The American Society for Pharmacology and Experimental Therapeutics JPET 301:698–704, 2002 Vol. 301, No. 2 4630/981643 Printed in U.S.A. Relative Reinforcing Effects of Three Opioids with Different Durations of Action M. C. KO, J. TERNER, S. HURSH, J. H. WOODS, and G. WINGER Departments of Pharmacology and Psychology, University of Michigan, Ann Arbor, Michigan (M.C.K., J.T., J.H.W., G.W.); Science Applications International, Joppa, Maryland (S.H.); and Johns Hopkins University School of Medicine, Baltimore, Maryland (S.H.) Received October 9, 2001; accepted February 6, 2002 This article is available online at http://jpet.aspetjournals.org Relatively little is known about what properties of drugs of abuse contribute to their reinforcing effects. It is generally acknowledged, however, that stimuli function better as reinforcers if there is relatively little delay between the response and reinforcer delivery (Renner, 1964; de Villiers, 1977). There is some evidence to support the notion that drugs that have fast onsets of action are stronger reinforcers than drugs that have slow onsets of action. Balster and Schuster (1973) and Panlilio et al. (1998), for example, reported that lower rates of behavior were maintained by cocaine when it was delivered slowly compared with more rapid administration. We have found that ketamine, an NMDA antagonist with a rapid onset of action, is as strong a reinforcer as phencyclidine, an NMDA antagonist with a somewhat less rapid onset of action, but much stronger as a reinforcer than dizocilpine, an NMDA antagonist with a slow onset of action (Winger et al., 2002). These latter three drugs vary in their durations as well as their onsets of action, and the contribution of duration of action to the relative reinforcing effects of drugs of abuse is not well documented. Panlilio and Schindler (2000) are among the few who have compared behavior maintained by shorter and longer acting drugs. They found that the ultrashort-acting opioid remifentanil served as a reinforcer when delivered intravenously to rats and that it maintained breakpoints under progressive ratio schedules that were not markedly different from resulting in drug administration was increased from one session to the next. Comparisons were made of the behavioral economic variables Pmax and area under the demand curve (Omax). Remifentanil maintained higher rates of responding than did alfentanil, and alfentanil maintained higher rates of responding than did fentanyl. When normalized demand functions were compared, however, the drugs did not differ significantly from each other in terms of Pmax or Omax. These data agree with those of others who have suggested that duration of action is not an important contributor to drugs’ reinforcing strength. those maintained by the longer-acting opioid heroin. They concluded that duration of action was independent of the ability to serve as a reinforcer. Drugs that act at the -opioid receptor are a natural choice for experimental procedures designed to evaluate the role of duration of drug action on reinforcing strength. There are several -opioid agonists that vary almost exclusively in their pharmacokinetics. Fentanyl is a fairly long-acting -opioid agonist, alfentanil has a nearly identical profile of activity but with a shorter duration of action, and remifentanil is an ultrashort-acting -opioid agonist, useful in surgical procedures in which it can be administered by constant infusion (Glass et al., 1999; Rosow, 1999). What is not certain is whether these three drugs have similar onsets of action after i.v. administration, a property that is critical if duration of action is to be isolated as a variable affecting reinforcing effect. In the current study, the onsets and durations of action of fentanyl, alfentanil, and remifentanil were determined and compared using measures of their ability to suppress respiration and to produce antinociception after their intravenous delivery. Their relative reinforcing effects were then evaluated using normalized demand function analysis as described by Hursh and Winger (1995). Materials and Methods Subjects This study was supported by U.S. Public Health Service Grant DA-00254 (to J.H.W.). Eleven adult male and female rhesus monkeys (Macaca mulatta) with body weights ranging between 5.4 and 12.8 kg were used. They ABBREVIATIONS: NMDA, N-methyl-D-aspartate; Ve, minute volume of respiration; MPE, maximum possible effect; inj, injection. 698 Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 ABSTRACT The role of duration of action on the relative reinforcing effects of three opioid drugs (fentanyl, alfentanil, and remifentanil) was evaluated. Duration and onset of action were determined using measures of respiratory depression and antinociception after i.v. administration. Effects on minute volume of respiration indicated that each of the three opioids had immediate onsets of action after i.v. administration. Fentanyl’s duration of suppression of respiration and antinociception was longer than that of alfentanil, which was longer than that of remifentanil. Reinforcing strength was measured in i.v. self-administration studies in which the fixed ratio Duration of Action and Opioid Reinforcement were housed individually with free access to water and were fed approximately 25 to 30 biscuits (Purina Monkey Chow; Ralston Purina, St. Louis, MO) and fresh fruit daily. The animals were maintained on a 12-h light/dark cycle. The monkeys were housed in facilities accredited by the American Association for the Accreditation of Laboratory Animal Care, and the studies were conducted in accordance to the Guide for the Care and Use of Laboratory Animals as adopted and promulgated by the National Institutes of Health (National Academy Press, Washington DC, revised 1996). Experimental Procedures and Designs levers were three stimulus lights: a red light on the right indicated drug availability, a green light in the center indicated an intravenous infusion, but a third light was not used in this experiment. The monkeys all had a history of i.v. alfentanil self-administration. They had initially been adapted to wearing a Teflon mesh jacket attached to a flexible steel tether (Lomir Biomedical, Malone, NY). Aseptic surgical techniques were then used to implant a silicone catheter into one of eight major veins (external or internal jugular, femoral, or brachial veins). The proximal end of the catheter was inserted close to the heart, and the distal end was run subcutaneously from the incision site toward the monkey’s back, exiting at the midscapular region. The catheter traveled through the tether to the back of the cage where it connected to a swivel. On the outside rear of the cage, a second section of silicone tubing connected to the back of the swivel, and attached to a filter (Gilman Scientific, Ann Arbor, MI) before connecting to an infusion pump (model MHRK 55; Watson-Marlow Co., Falmouth, UK). The experiments were controlled by IBM computers, programmed with software from MED Associates (St. Albans, VT). These were located in a room adjacent to the room in which the animals were housed and tested. Two experimental sessions were scheduled each day, one beginning at approximately 10:00 AM and the second beginning at approximately 4:00 PM. Each session was 130 min in duration, signaled by the onset of the red stimulus light. The schedule of drug availability started at fixed ratio 10, time-out 10 s. Thus, 10 responses on the lever under the red light turned off the red light and turned on the green light and the infusion pump. Once the infusion was completed, all lights were extinguished for 10 s, and responses had no programmed consequences. The red light was illuminated again. After several sessions of drug and saline availability on this schedule, only drug was made available, and the fixed ratio (i.e., the ratio between the number of responses and reinforcer delivery) was increased on each consecutive session from 10 to 32 to 100 to 320 to 1000. The animal was then returned to the fixed ratio 10 time-out 10 schedule, and drug availability was again alternated with saline availability for several sessions. The incrementing fixed ratio procedure was then implemented again. Each dose of each drug was tested in the incrementing fixed ratio procedure twice in each monkey. Data Analysis Respiration. Individual Ve values obtained in each test session were expressed as percentage of control of the respective parameters collected before drug administration. The volume was calculated once per minute. For the sake of clarity, the values are plotted once every 5 min (Fig. 1). Mean and S.E.M. values were calculated. These data were analyzed by a two-way analysis of variance followed by the Newman-Keuls test for multiple comparisons. In particular, the values obtained at the time points of 1, 5, 15, 30, 45, and 60 min after injection were compared among groups. Antinociception. Individual tail-withdrawal latencies were converted to percentage of maximum possible effect (MPE) by the following formula: %MPE ⫽ [(test latency ⫺ control latency)/(cutoff latency 20 s ⫺ control latency)] ⫻ 100. Comparisons were made for the same monkeys across experimental conditions. Data were analyzed by a two-way analysis of variance followed by the NewmanKeuls test for multiple comparisons. Self-Administration. Rates of responding were calculated as the number of responses made in a session while the red light was illuminated, divided by the number of seconds that the red light was illuminated. Drug consumption was calculated as the number of injections taken in a session multiplied by the dose of drug per injection. The data from each animal were averaged over the two sessions at each fixed ratio value for each drug and dose. These means were then averaged over the three animals to produce the results that are shown in Fig. 3. Measures of reinforcing strength were indicated by two variables, Pmax and Omax, that are traditionally obtained from the demand curves. Demand curves describe the relation between consumption Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 Respiration. Four rhesus monkeys, two males and two females, served as subjects in this part of the study. The apparatus used was similar to that described previously (Howell et al., 1988; France and Woods, 1990; Butelman et al., 1993). The monkey was seated in a restraint chair that was placed in a ventilated, sound-attenuating chamber. A helmet was placed over the monkey’s head and sealed around its neck by two closely fitting latex shields. Gas (air) flowed into the helmet and was pumped out at a rate of 8 l/min. The monkeys’ breathing produced changes in pressure inside the helmet that were measured with a pressure transducer connected to a polygraph (Grass model 7); the data were recorded on a polygraph trace and in a microprocessor (IBM PC jr.) via an analog-to-digital converter. The apparatus was calibrated routinely with known quantities of air. Before the test session, a catheter (Angiocath 24-gauge/19 mm; BD Biosciences, Franklin Lakes, NJ) was inserted in the monkey’s saphenous vein. Each opioid was given intravenously at the start of the recording session. Four doses of fentanyl (0.0032– 0.032 mg/kg and vehicle), four doses of alfentanil (0.0032– 0.032 mg/kg and vehicle), and two doses of remifentanil (0.0032– 0.0056 mg/kg and vehicle) were administered on separate sessions. Doses were increased until at least a 50% decrease in the baseline value was produced. Each dose was tested two times in each monkey. Test sessions were conducted twice per week with a minimum 72-h interval between drug exposures. Experimental sessions consisted of 60 min of exposure to air. Respiratory parameters were recorded continuously during sessions. Frequency, the number of inspirations per minute, was directly determined. Minute volume (Ve), the number of liters of air inspired per minute, was calculated from integration of the polygraph tracing. Because, as has been shown previously (Paronis and Woods, 1997; Kishioka et al., 2000), Ve was the most sensitive measure of drug effect, the effects of the three opioids on Ve measured during air breathing are presented herein. Antinociception. Four rhesus monkeys, one male and three females, served as subjects in this part of the study. The warm water (50°C) tail-withdrawal procedure used in this study to evaluate antinociception was similar to that described by Dykstra and Woods (1986). Monkeys were seated in primate restraint chairs, and the lower part of their shaved tails (approximately 15 cm) was immersed in a thermos flask containing water maintained at either 40, 50, or 55°C. Tail-withdrawal latencies were timed manually using a microprocessor (IBM PC) via a hand-held push-button switch. Monkeys were tested one to two times at three temperatures in a random order. If the monkeys did not remove their tails from the flask within 20 s (cutoff), the flask was removed, and a maximum time of 20 s was recorded. Sessions began with control determinations at each temperature. Each opioid was administered intravenously through a saphenous vein from either side of the lower legs. Subsequent tailwithdrawal latencies were determined at 5, 15, 30, 45, 60, and 90 min after injection. A single dosing procedure was used in all test sessions, which were conducted twice per week with a 72-h interval. Self-Administration. Three individually housed adult rhesus monkeys, two males and one female, were subjects in this experiment. They were housed in stainless steel cages (83.3 ⫻ 76.2 ⫻ 91.4 cm in depth). Each cage was equipped with a lever panel with two response levers located on the right-hand side of the cage. Above the 699 700 Ko et al. accounted for by the curve fit (R2). These were returned to the Excel spreadsheet, where Pmax and Omax were calculated. Response output functions were determined as well. These demonstrated the relation between the total number of responses in a given session and the price. In these functions, the Pmax is represented as the highest point on the curve, and Omax is represented by the total number of responses at Pmax. The response output functions for the three drugs were established using the formula Y ⫽ log(100) ⫹ ((B ⫹ 1)) ⫺ (Aⴱ(10∧X)) 䡠 log(e), where Y is log responses and X is log P. Initial values were the same as those for the demand function. Statistical comparison among the Pmax and Omax values were made with a repeated measures analysis of variance. Drugs. Fentanyl HCl, alfentanil HCl (National Institute on Drug Abuse, Bethesda, MD), and remifentanil (GlaxoWellcome, Research Triangle Park, NC) were dissolved in sterile water for the respiration and analgesia studies, and in sterile saline for the self-administration studies. For systemic administration in both respiration and antinociception assays, each compound was administered intravenously at a volume of 0.1 ml/kg. Fig. 1. Effects of fentanyl (top), alfentanil (middle), and remifentanil (bottom) on Ve over time. Abscissae: time in minutes after the i.v. administration of each opioid. Ordinates: minute volume as percentage of nondrug control. Data points are the means (⫾S.E.M.) for four monkeys. (total drug intake per session) and price (fixed ratio value divided by dose in mg/kg/inj). Pmax is a measure of the elasticity of the demand function, indicating how quickly reinforced behavior decreases as the price of the reinforcer is increased. Omax reflects the amount of behavior that the reinforcer maintains. Because the three opioids could vary in their potency as reinforcers, direct comparisons of their consumption versus fixed ratio would be confounded by these potency differences. We therefore used a normalization procedure described by Hursh and Winger (1995) to generate the demand curves. This procedure sets the consumption of each of the drugs at the lowest price (highest dose at the lowest fixed ratio) to the same normalized value of 100, and compares the elasticity and Omax values of the curves that have the same origin. Normalized demand curves were constructed after determination of the values of normalized dose or 100/number of reinforcers earned at the lowest price (q), normalized price: fixed ratio/q (P), and normalized consumption: number of reinforcers per session at each fixed ratio 䡠 q) (Q). Log P and log Q were calculated in an Excel spreadsheet from the consumption data for each dose, averaged across monkeys. This information was graphed in GraphPad Prism (GraphPad Software, San Diego, CA) by using nonlinear curve fitting and the formula Y ⫽ log(100) ⫹ B(X) ⫺ (A 䡠 (10∧X)) 䡠 log(e), where Y is log Q and X is log P. Initial values were set to a ⫽ ⫺0.05 and b ⫽ 0.004. Prism returned values for b (initial slope), a (acceleration), and variance Respiration. The effects of fentanyl, alfentanil, and remifentanil on Ve, measured immediately after and for 60 min after intravenous administration, are shown in Fig. 1. Effective doses of each drug depressed respiration as quickly as measurements could be taken (at 1 min). Fentanyl produced a dose-related depression of Ve that was 43 ⫾ 6% of control at a dose of 0.032 mg/kg [F(4,28) ⫽ 20.1; p ⬍ 0.01] at 1 min and recovered to 65 ⫾ 5% of control at the 60-min measurement period (p ⬍ 0.01). Alfentanil also produced a dose-related suppression of Ve to a maximum of 32 ⫾ 4% of control [F(4,28) ⫽ 18.8; p ⬍ 0.01] at 1 min. Alfentanil was equipotent with fentanyl, also producing the maximum response at a dose of 0.032 mg/kg (p ⬍ 0.01). Alfentanil’s action on minute volume had returned to control levels by approximately 30 min after intravenous administration of 0.032 mg/kg (p ⬍ 0.01). Remifentanil was also effective in suppressing Ve. Although a dose of 0.0032 mg/kg had little effect on Ve, a dose of 0.0056 mg/kg produced a 47 ⫾ 7% reduction in Ve (p ⬍ 0.01) at 1 min; the animals were breathing at a normal volume within 10 min of drug administration [F(5,35) ⫽ 6.9; p ⬍ 0.01]. Antinociception. The antinociceptive effects of fentanyl, alfentanil, and remifentanil measured in 50°C water are shown in Fig. 2. There was no change in the response to 40°C water, and the effects using 55°C water were much the same as those shown herein with 50°C water. Each of the opioids produced dose-dependent thermal antinociception at this temperature. Fentanyl and alfentanil were equipotent and equieffective. At a dose of 0.032 mg/kg, both drugs produced respiratory arrest in two monkeys, which was reversed by an opioid antagonist (data not shown). At smaller doses (0.018 and 0.01 mg/kg) the antinociceptive effects of these drugs and their durations of action were dose-dependent (fentanyl [F(3,9) ⫽ 59.7; p ⬍ 0.01] and alfentanil [F(3,9) ⫽ 140.9; p ⬍ 0.01]. In particular, 0.018 mg/kg fentanyl produced significant antinociception that lasted for 60 min (p ⬍ 0.01). The antinociception produced by alfentanil at this dose lasted for approximately 15 min (p ⬍ 0.01). Remifentanil produced thermal antinociception only at a dose of 0.0056 mg/kg, and this maximal effect was very transient, lasting less than 15 min. Significant differences in antinociceptive effects be- Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 Results Duration of Action and Opioid Reinforcement 701 Fig. 2. Effects of fentanyl (top), alfentanil (middle), and remifentanil (bottom) on thermal analgesia by using 50°C water. Abscissae: time in minutes after the i.v. administration of each opioid. Ordinates: latency to withdraw the tail, as a percentage of the maximum possible effect. Data points are the means (⫾S.E.M.) for four monkeys. tween the dose and vehicle condition are shown at corresponding time points in Fig. 2. Self-Administration. The average rates of responding maintained by each of the three opioids, and the session intakes resulting from the injection-contingent responding are shown in Fig. 3, left. The fastest rates of responding were produced by remifentanil, with a dose of 0.0001 mg/kg/inj producing an average maximum rate of 1.9 responses/s at fixed ratio 32. Alfentanil maintained the next fastest rate of 1.32 responses/s at fixed ratio 32. Fentanyl maintained the slowest rates, with a maximum rate of 0.94 responses/s at a dose of 0.001 mg/kg/inj and fixed ratio 1000. In general, rates of responding increased as the fixed ratio value was increased up to a maximum, and then decreased with further increases in fixed ratio value, producing an inverted U-shaped function of response rate against fixed ratio value. For the largest dose of fentanyl, rates increased monotonically across the fixed ratio values, although downturns would certainly have been observed at higher ratio values. Typically, as the dose of each opioid was increased, the fixed ratio at which the maximum rate of responding oc- Discussion The effects of these three -opioids on respiration and antinociception assays confirm in rhesus monkeys what is commonly held in clinical practice: fentanyl was longer acting than alfentanil, which was longer acting than remifentanil (Scholz et al., 1996; Rosow, 1999; Gesztesi et al., 2000). In addition, fentanyl and alfentanil were nearly equally potent, and remifentanil was approximately 6 times more potent. After intravenous administration, each of these opioids had immediate onsets of action and a qualitatively similar ability to suppress respiration and to produce antinociception. These observations are consistent with the pharmacological profiles of -opioid full agonists (Niemegeers and Janssen, 1981; James et al., 1991; Glass et al., 1993; Willens and Myslinski, 1993; Emmerson et al., 1996). In measures of reinforcing effects, the same order of potency was seen as in measures of respiration and antinociception: fentanyl and alfentanil were nearly equipotent and remifentanil was 10 times more potent. The inverted Ushaped curves that developed as fixed ratio values were increased across each dose of drug have been observed in other studies in which fixed ratio values are increased systematically (Lemaire and Meisch, 1985; Winger, 1993). The relatively low rates of responding that occurred with small ratio values was likely to be due to accumulation of drug and consequent drug-induced suppression of ongoing rates of re- Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 curred increased as well. Thus, with fentanyl, a dose of 0.0001 mg/kg/inj maintained peak response rates at fixed ratio 32, a dose of 0.0003 mg/kg/inj maintained peak response rates at fixed ratio 100, and a dose of 0.001 mg/kg/inj maintained peak response rates at fixed ratio 1000; the rates maintained by this largest dose could have increased if higher ratios had been evaluated. Similarly, with alfentanil the smallest dose of 0.0003 mg/kg/inj maintained peak response rates at fixed ratio 32, the intermediate dose of 0.001 mg/kg/inj maintained peak response rates at fixed ratio 100, and the largest dose of 0.003 mg/kg/inj maintained peak response rates at fixed ratio 320. The one exception was remifentanil for which the two smaller doses both produced peak response rates at a fixed ratio 32, and the largest dose maintained peak response rates at fixed ratio 320. The number of injections and the amount of drug consumed decreased monotonically as the fixed ratio value increased (Fig. 3, right). The larger the dose per injection, the greater the total session consumption across fixed ratio values. The demand and response-output functions are shown for individual animals in Fig. 4. Typical demand functions developed in which consumption was maintained across low price increases, and decreased as price became larger (Fig. 4, left). The goodness of fit for the demand curves to the averaged data was excellent; R2 values were 0.98 for alfentanil and remifentanil and 0.93 for fentanyl. The Pmax and Omax values, obtained using averages across monkeys, are shown in the figure and were, respectively, 528 and 13,145 for remifentanil, 365 and 9953 for alfentanil, and 383 and 6888 for fentanyl. There were no statistically significant differences among either the Pmax or Omax values, indicating that these three opioids did not differ significantly in their reinforcing effectiveness. 702 Ko et al. sponding. Drug accumulation was greater at small ratio values because these small values resulted in shorter interinjection times. As the ratio was increased, interinjection times increased, drug accumulation was reduced, and rates rose as a consequence. The relatively low rates of responding that occurred at higher ratio values were likely due to an entirely different mechanism, one of more relevance to the comparison of relatively reinforcing strength: these low rates are presumed to be a function of the inability of the drug to maintain responding as the amount of behavior necessary to obtain the drug was increased. Larger doses of drug were more resistant to the ratio increases, indicating that larger doses functioned better as reinforcers than smaller doses. Despite the increases in rates that accompanied initial increases in fixed ratio values, there was a monotonic decrease in total session consumption for all drugs as the fixed ratio values increased. In addition, the total consumption was consistently greater as the dose per injection of each of the drugs increased. The demand functions generated indicated that consumption of these drugs was defended as price (ratio/dose) was initially increased. Eventually, however, a price was reached at which drug intake began to decrease. This price at which the demand curve changed from relatively inelas- tic to relatively elastic (slope of the curve ⫽ ⫺1) is known as the Pmax and reflected the amount of behavior the monkeys were willing to expend to obtain the drugs as the price increased. The Pmax values, normalized to account for differences in potency among the drugs, did not differentiate the drugs, indicating that these opioids did not differ in their ability to maintain behavior in the face of increasing response requirements. A second measure of reinforcing effectiveness is Omax, the total responses at Pmax. The Omax reflected the total amount of behavior the animals were willing to expend to obtain the drugs. Normalized Omax values also did not differ significantly among the three opioids, supporting the notion that the drugs did not differ in their reinforcing effectiveness. Therefore, insofar as reinforcing strength after i.v. delivery plays a role in drug abuse potential in humans, these drugs should not be expected to have different abuse potentials. The relation between the measures of Pmax and Omax is not yet well defined. Bickel et al. (2000) recently described reinforcing effectiveness as being heterogenous, with Pmax and Omax each contributing separately to the concept. Our previous data (Hursh and Winger, 1995) suggested that these two indices may vary independently. Why a particular reinforcer might, for example, resist increases in price but not produce Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 Fig. 3. Rates of responding (left) and consumption (right) of the three opioids, as a function of fixed ratio values. Data for rates of responding are shown as responses per second for fentanyl (top), alfentanil (middle), and remifentanil (bottom). Abscissae: number of lever-press responses during the red stimulus light condition. Ordinates: number of responses required for delivery of each reinforcer. Data for consumption are shown as milligrams per kilogram per session (abscissae) for the drugs as a function of the fixed ratio value (ordinates). Data points are the means (⫾S.E.M.) for three monkeys. Duration of Action and Opioid Reinforcement 703 large amounts of behavior relative to another reinforcer remains unknown. Fortunately, for the three drugs evaluated herein, the differences among the Pmax and Omax values were small and not significant, presenting consistent evidence that these drugs do not differ in their reinforcing effectiveness. In conclusion, remifentanil, alfentanil, and fentanyl had similar rapid rates of onset of action, and differed exclusively in their potencies and durations of action. Despite the fact that, compared with alfentanil, remifentanil maintained relatively higher rates of responding, and fentanyl maintained relatively lower rates of responding, none these drugs differed greatly in their elasticities or total response outputs, indicating similar apparent reinforcing strengths. Although it must be kept in mind that only three drugs were studied, and that these drugs had durations of action that spanned a relatively narrow range (15– 60 min), the data support the report of Panlilio and Schindler (2000) that duration of action does not appear to play an important role in determining the reinforcing strength of drugs that are otherwise the same with respect to onset of action and quality of effect. Acknowledgments We thank Debbie Huntzinger, Laurie McDowell, Mark Johnson, Michael Song, and John Busenbark for excellent technical assistance. References Balster RL and Schuster CR (1973) Fixed-interval schedule of cocaine reinforcement: effect of dose and infusion duration. J Exp Anal Behav 20:119 –129. Bickel WK, Marsch LA, and Carroll ME (2000) Deconstructing relative reinforcing efficacy and situating the measures of pharmacological reinforcement with behavioral economics: a theoretical proposal. Psychopharmacology 153:44 –56. Butelman ER, France CP, and Woods JH (1993) Apparent pA2 analysis on the respiratory depressant effects of alfentanil, etonitazene, ethylketocyclazocine (EKC) and Mr2033 in rhesus monkeys. J Pharmacol Exp Ther 264:145–151. de Villiers P (1977) Choice in concurrent schedules and a quantitative formulation of the law of effect, in Handbook of Operant Behavior (Honig WK and Staddon JER eds) pp 233–287, Prentice-Hall, Englewood Cliffs, NJ. Dykstra LA and Woods JH (1986) A tail withdrawal procedure for assessing analgesic activity in rhesus monkeys. J Pharmacol Methods 15:263–269. Emmerson PJ, Clark MJ, Mansour A, Akil H, Woods JH, and Medzihradsky F (1996) Characterization of opioid agonist efficacy in a C6 glioma cell line expressing the opioid receptor. J Pharmacol Exp Ther 278:1121–1127. France CP and Woods JH (1990) Respiratory effects of receptor-selective opioids in rhesus monkey, in The International Narcotics Research Conference (INRC) ‘89 (Quirion R, Jhamanda K, and Gianoulakis C eds) pp 295–298, A. R. Liss, New York. Gesztesi Z, Rego MM, and White PF (2000) The comparative effectiveness of fentanyl and its newer analogs during extracorporeal shock wave lithotripsy under monitored anesthesia care. Anesth Analg 90:567–570. Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017 Fig. 4. Demand curves (left) and response output functions (right) for the individual opioids. Left abscissae: log of the normalized price; left ordinates: log of the normalized consumption. Right abscissae: log of the normalized price; right ordinates: log of the total responses. Data points are the averages for each of the three individual monkeys at each of the three tested doses. The Pmax and Omax data (left) were determined using the averaged values for the demand functions. 704 Ko et al. Glass PS, Gan TJ, and Howell S (1999) A review of the pharmacokinetics and pharmacodynamics of remifentanil. Anesth Analg 89:S7–S14. Glass PS, Hardman D, Kamiyama Y, Quill TJ, Marton G, Donn KH, Grosse CM, and Hermann D (1993) Preliminary pharmacokinetics and pharmacodynamics of an ultra-short-acting opioid: remifentanil (GI87084B). Anesth Analg 77:1031–1040. Howell LL, Bergman J, and Morse WH (1988) Effects of levorphanol and several kappa-selective opioids on respiration and behavior in rhesus monkeys. J Pharmacol Exp Ther 245:354 –372. Hursh SR and Winger G (1995) Normalized demand for drugs and other reinforcers. J Exp Anal Behav 64:373–384. James MK, Feldman PL, Schuster SV, Bilotta JM, Brackeen MF, and Leighton HJ (1991) Opioid receptor activity of GI 87084B, a novel ultra-short acting analgesic, in isolated tissues. J Pharmacol Exp Ther 259:712–718. Kishioka S, Paronis CA, Lewis JW, and Woods JH (2000) Buprenorphine and methoclocinnamox: agonist and antagonist effects on respiratory function in rhesus monkeys. Eur J Pharmacol 391:289 –297. Lemaire GA and Meisch RA (1985) Oral drug self-administration in rhesus monkeys: interactions between drug amount and fixed ratio size. J Exp Anal Behav 44:377– 389. Niemegeers CJE and Janssen PAJ (1981) Alfentanil (R39209), a particularly shortacting morphine-like narcotic for intravenous use in anesthesia. Drug Dev Res 1:83– 88. Panlilio LV, Goldberg SR, Gilman JP, Jufer R, Cone EJ, and Schindler CW (1998) Effects of delivery rate and non-contingent infusions of cocaine on cocaine selfadministration in rhesus monkeys. Psychopharmacology 137:253–258. Panlilio LV and Schindler CW (2000) Self-administration of remifentanil, an ultrashort acting opioid, under continuous and progressive ratio schedules of reinforcement in rats. Psychopharmacology 150:61– 66. Paronis CA and Woods JH (1997) Ventilation in morphine-maintained rhesus monkeys. II: Tolerance to the antinociceptive but not the ventilatory effects of morphine. J Pharmacol Exp Ther 282:355–362. Renner KE (1964) Delay of reinforcement: a historical review. Psychol Bull 61:341– 361. Rosow CE (1999) An overview of remifentanil. Anesth Analg 89:S1–S3. Scholz J, Steinfath M, and Schulz M (1996) Clinical pharmacokinetics of alfentanil, fentanyl and sufentanil. An update. Clin Pharmacokinet 31:275–292. Willens JS and Myslinski NR (1993) Pharmacodynamics, pharmacokinetics, and clinical uses of fentanyl, sufentanil, and alfentanil. Heart Lung 22:239 –251. Winger G (1993) Fixed ratio and time out changes on behavior maintained by cocaine or methohexital in rhesus monkeys. 1. Comparison of reinforcing strength. Exp Clin Psychopharmacol 1:142–153. Winger G, Hursh SR, Casey KL, and Woods JH (2002) Relative reinforcing effects of three NMDA antagonists with different onsets of action. J Pharmacol Exp Ther 301:690 – 697. Address correspondence to: Dr. Gail Winger, Department of Pharmacology, University of Michigan Medical School, 1301 MSRB III, Ann Arbor, MI 481090632. E-mail: [email protected] Downloaded from jpet.aspetjournals.org at ASPET Journals on May 4, 2017