Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
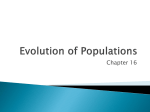
Original Article Cardiorespiratory Fitness, Body Mass Index, and Heart Failure Mortality in Men Cooper Center Longitudinal Study Stephen W. Farrell, PhD; Carrie E. Finley, MS; Nina B. Radford, MD; William L. Haskell, PhD Background—We evaluated the individual and joint associations among cardiorespiratory fitness (CRF), body mass index, and heart failure (HF) mortality, as well as the additive effect of an increasing number of cardiovascular risk factors on HF mortality in fit versus unfit men. Methods and Results—A total of 44 674 men without a history of cardiovascular disease underwent a baseline examination between 1971 and 2010. Measures included body mass index and CRF quantified as duration of maximal treadmill exercise testing. Participants were divided into age-specific low, moderate, and high CRF categories. Hazard ratios were computed with Cox regression analysis. During a mean follow-up of 19.8±10.4 years, 153 HF deaths occurred. Adjusted hazard ratios across high, moderate, and low CRF categories were 1.0, 1.63, and 3.97, respectively, whereas those of normal, overweight, and obese body mass index categories were 1.0, 1.56, and 3.71, respectively (P for trend <0.0001 for each). When grouped into categories of fit and unfit (upper 80% and lower 20% of CRF distribution, respectively), hazard ratios were significantly lower in fit compared with unfit men in normal and overweight body mass index strata (P<0.002) but not in obese men. Within men matched for the same number of HF risk factors, fit men had significantly lower HF mortality than unfit men (P≤0.02). Conclusions—Higher baseline CRF is associated with lower HF mortality risk in men, regardless of the number of HF risk factors present. Men should be counseled on physical activity with the goal of achieving at least a moderate level of CRF, thereby presumably decreasing their risk of HF mortality. (Circ Heart Fail. 2013;6:898-905.) Key Words: body mass index ■ heart failure H eart failure (HF) is a common cause of mortality in older US adults, accounting for 292 214 deaths where HF is listed as a primary or secondary cause and for 58 933 deaths where it is listed as the underlying cause of death.1 For individuals aged ≥65 years, HF is the most frequent cause of hospitalization, and it is estimated that 6 million Americans are living with HF. In addition to its physical and psychological toll, HF also places a significant economic burden on the society. The estimated direct and indirect cost of HF in the United States is $37.2 billion in 2009.1 ■ physical fitness our knowledge, there are no reported data relating an objective measure of CRF with HF mortality. Although there has been an important recent report on the joint exposures of multiple adiposity measures, physical activity, and incidence of HF,14 there are no reported data on the joint exposures of CRF and body mass index (BMI) with subsequent HF mortality. Because overweight and obesity, as well as physical inactivity, are highly prevalent in the US population,17,18 we think it is important to examine these issues. Thus, the primary purpose of our investigation is to examine the individual and joint associations among CRF, BMI, and HF mortality in a large cohort of men in the Cooper Center Longitudinal Study (CCLS). A secondary purpose is to examine the additive effect of an increasing number of risk factors on HF mortality in fit versus unfit men. Clinical Perspective on p 905 Well-established risk factors for HF include age, hypertension, tobacco use, diabetes mellitus, obesity, high alcohol intake, previous myocardial infarction, sleep apnea,2 and valve disease.3–6 Although many studies have examined the association between physical activity and cardiovascular disease (CVD) mortality,7–12 much less is known about the association between physical activity and HF mortality. Studies that have examined this association relied exclusively on self-reported physical activity patterns,13–15 which are only moderately correlated with objective measures of cardiorespiratory fitness (CRF).16 To Methods Study Participants and Measurements The CCLS is an updated continuation of the Aerobics Center Longitudinal Study (ACLS)19 and includes additional clinical variables, an expanded biobank, and mortality data collected through 2010. Participants in the present study included 44 674 men without a personal history of CVD who completed a baseline comprehensive medical examination at the Cooper Clinic in Dallas, TX, during Received July 30, 2012; accepted July 10, 2013. From the Education Department (S.W.F.), and Research Department (C.E.F.), The Cooper Institute, Dallas, TX; Cardiovascular Medicine Department, The Cooper Clinic, Dallas, TX (N.B.R.); and Department of Medicine, Stanford University, Palo Alto, CA (W.L.H.). Correspondence to Stephen W. Farrell, PhD, The Cooper Institute, 12330 Preston Rd, Dallas, TX 75230. E-mail [email protected] © 2013 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 898 DOI: 10.1161/CIRCHEARTFAILURE.112.000088 Farrell et al Fitness, BMI, Heart Failure Mortality 899 1971–2010. All participants were US residents, and the majority (≈90%) were white and from middle-to-upper socioeconomic strata. After receiving written informed consent from each participant, a clinical evaluation was performed and included an examination by a physician, fasting blood chemistry assessment, personal and family health history, anthropometry, resting blood pressure and ECG, and a maximal graded treadmill exercise test. A standard physician’s scale and stadiometer were used to measure weight and height. BMI was calculated as weight in kilograms divided by height in meters squared. We categorized men as normal weight (BMI, 18.5–24.9 kg/m2), overweight (BMI, 25.0–29.9 kg/m2), or obese (BMI ≥30 kg/m2). CRF was quantified as the duration of a maximal treadmill exercise test using a modified Balke protocol20 as described elsewhere. Exercise duration from this protocol correlated highly (r=0.92) with directly measured maximal oxygen uptake in men.21 All participants were encouraged to provide a maximal effort, and those that did not achieve ≥85% of age-predicted maximal heart rate (n=1697) were excluded from the analyses. We felt it was important to exclude these men to avoid CRF misclassification and because some men in this group may have had subclinical disease, which may have prevented them from achieving a maximal test. To standardize exercise test performance, we computed maximal metabolic equivalent (MET; 1 MET=3.5 mL O2 uptake/kg body weight per minute) levels of CRF based on the final treadmill speed and grade.22 Trained Cooper Clinic technicians analyzed blood chemistry using automated techniques following standardized procedures. This laboratory participates in and meets quality control standards of the Centers for Disease Control and Prevention Lipid Standardization Program. The CCLS undergoes annual review and approval by the Institutional Review Board of The Cooper Institute. Men with previously diagnosed HF, myocardial infarction, stroke, or cancer (n=5945), as well as men with a BMI <18.5 kg/m2 (n=82) and men with <1 year (n=670) of follow-up, were excluded from analyses. Following these exclusions, the resultant sample size of the cohort was 44 674. Mortality Surveillance The National Death Index was used to ascertain vital status. The National Death Index has a sensitivity of 96% and a specificity of 100% for determining deaths in the general population.23 Once we identified possible decedents, Departments of Vital Statistics in the appropriate states were contacted, and official copies of death certificates were requested. We compared information on the death certificates with clinical records to confirm that the death certificate matched the individual. A nosologist coded the underlying and contributing causes of death according to the International Classification of Diseases, Ninth and Tenth Editions, Revised. Statistical Analyses We followed study participants for mortality from the date of their baseline examination to the date of death for decedents or to December 31, 2010, for survivors. We computed man-years of exposure as the sum of follow-up time among decedents and survivors. There were 153 HF deaths identified during an average of 19.8±10.4 years of follow-up and 883 870 man-years of exposure. Cox proportional hazards regression analysis was used to estimate hazard ratios (HRs) and 95% confidence intervals of HF mortality according to exposure categories. HRs were used instead of odds ratios because HRs are used in cohort studies to express the relative effect of a variable on the risk of an event over time. In our primary analysis, BMI was grouped as described previously. CRF was grouped as low fit (lowest 20%), moderate fit (next 40%), and high fit (highest 40%) according to age-standardized normative data based on maximal treadmill exercise test duration as described elsewhere.19 Multivariate analyses included age (years), examination year, smoking status (never, past, current), resting systolic blood pressure, BMI (where applicable), presence of diabetes mellitus, and family history of CVD. These 7 factors will henceforth be referred to as covariables. Tests of linear trends in mortality rates and risk estimates across exposure categories were computed using ordinal scoring. We also examined the joint exposures of BMI and CRF with HF mortality. In these analyses, BMI exposure groups were based on those previously described. CRF was grouped as fit and unfit based on the upper 80% and the lower 20% of the age-standardized CRF distribution, as previously reported in the CCLS.24 Next, comparisons of HF mortality between fit and unfit men were performed within groups of men, with 0, 1, or ≥2 risk factors. Finally, we examined the HRs for each of the individual HF risk factors, with the low-risk group (normal resting blood pressure and no personal history of hypertension, current nonsmoker, no personal history of diabetes mellitus, BMI <30 kg/m2, fit, and no family history of CVD) as the referent and using dichotomies for all comparisons. We assessed interaction among exposure groups using likelihood ratio tests of nested models. All P values are 2-sided, and P<0.05 was considered statistically significant. Results Of the 1486 total CVD deaths in the cohort, 153 (10.2%) were from HF. Baseline characteristics of the overall cohort according to vital status are presented in Table 1. On average, decedents were significantly older (49.8 versus 43.4 years), had higher BMI (27.8 versus 26.7 kg/m2), lower CRF (9.6 versus 11.7 METs), higher resting systolic (131.0 versus 121.6 mm Hg) and diastolic (86.5 versus 81.5 mm Hg) blood pressure, and higher total cholesterol (223.2 versus 206.9 mg/dL), triglyceride (179.5 versus 137.5 mg/dL), and blood glucose (111.1 versus 99.8 mg/dL) values than survivors. In addition, decedents had a higher prevalence of smoking than survivors (24.8% versus 17.4%), as well as a higher prevalence of diabetes mellitus (6.5% versus 1.8%) and hypertension (32.0% versus 14.4%; P<0.01 for all comparisons). Baseline characteristics of the cohort across CRF categories are presented in Table 2. Other than alcohol intake and family history of CVD, which were similar across categories of CRF, each of the baseline characteristics was significantly associated with categories of CRF. More specifically, higher levels of CRF were strongly associated with more favorable risk status (P for trend <0.0001 for each characteristic). Adjusted HRs for HF mortality according to exposures group are presented in Table 3. There was a significant inverse trend in HF mortality across CRF categories (HRs=1.0, 1.63, and 3.97 for high-, moderate-, and low-fit men, respectively; P for trend <0.0001). The trend was only slightly attenuated (P<0.0001) after adjustment for BMI (results not shown). As also shown in Table 3, there was a significant positive trend in HF mortality across incremental BMI categories (HRs=1.0, 1.56, and 3.71 for normal weight, overweight, and obese men, respectively; P for trend <0.0001). The trend was only slightly attenuated (P<0.003) after adjustment for CRF (results not shown). To place our findings into a more clinically relevant perspective, we jointly regressed HF mortality rates on BMI and CRF exposures grouped according to standardized definitions (Figure 1). HRs across incremental BMI categories of normal weight, overweight, and obese men were higher in unfit (3.96, 3.64, and 6.11, respectively) than fit (1.0, 1.72, and 4.47, respectively) men. However, these differences reached statistical significance in the normal weight and overweight BMI categories only (P<0.002). We next examined HF mortality in fit versus unfit men within groups having none (referent) or any 1 or ≥2 risk 900 Circ Heart Fail September 2013 Table 1. Baseline Characteristics of 44 674 Men in the Cooper Center Longitudinal Study During 1971–2010 All (N=44 674) Survivors (n=44 521) HF Decedents (n=153) Age, y 43.4±9.2 43.4±9.2 49.8±9.0 BMI, kg/m2 26.7±3.9 26.7±3.9 27.8±4.0 Cardiorespiratory fitness level, METs 11.6±2.4 11.7±2.4 9.6±2.0 Resting heart rate 61.2±10.7 61.2±10.7 64.0±12.0 Systolic blood pressure, mm Hg 121.6±13.0 121.6±13.0 131.0±18.2 Diastolic blood pressure, mm Hg 81.5±9.6 81.5±9.5 86.5±11.9 206.9±40.0 206.9±40.0 223.2±39.4 Cholesterol, mg/dL HDL, mg/dL 46.2±12.0 (n missing=9137) 46.2±12.0 (n missing=9060) 41.7±11.3 (n missing=77) LDL, mg/dL 132.4±35.3 (n missing=9978) 132.3±35.3 (n missing=9895) 147.5±35.5 (n missing=84) 137.6±113.1 137.5±112.8 99.8±16.9 99.8±16.8 111.1±33.8 8.4±10.6 (n missing=3976) 8.4±10.6 (n missing=3961) 7.8±9.2 (n missing=15) Nonsmoker 25 495 (57.1) 25 436 (57.1) 59 (38.6) Former smoker 11 380 (25.5) 11 324 (25.4) 56 (36.6) Current smoker 7799 (17.5) 7761 (17.4) 38 (24.8) Triglycerides, mg/dL Glucose, mg/dL Alcohol, drinks/wk 179.5±173.7 Smoking, n (%) Personal history of diabetes mellitus, % Personal history of hypertension, % Family history of CVD, % Follow-up, y 802 (1.8) 792 (1.8) 10 (6.5) 6457 (14.5) 6408 (14.4) 49 (32.0) 19 792 (44.3) 19 719 (44.3) 73 (47.7) 19.8±10.4 19.8±10.3 23.0±9.0 Unless otherwise specified, data are means±SD. BMI indicates body mass index; CVD, cardiovascular disease; HDL, high-density lipoprotein; HF, heart failure; LDL, low-density lipoprotein; METs, 1 metabolic equivalent=3.5 mL O2 uptake/kg body weight per minute. factors (Figure 2). Within each of these 3 groups, fit men had significantly lower HF mortality than unfit men (P<0.02). In Figure 3, we show the age-adjusted and examination year–adjusted HRs for HF mortality using each individual HF risk factor. HRs for obese (3.29, 2.3–4.7) and unfit (3.37, 2.4–4.7) men were similar and were the highest of all risk factors examined. Discussion To our knowledge, this is the first study using objective measures of both CRF and BMI examining the individual and joint associations among CRF, BMI, and HF mortality in men, as well as examining HF mortality in fit versus unfit men with a varying number of risk factors. CRF was strongly and inversely associated with HF mortality. Compared with men with high CRF, moderate-fit and low-fit men were 1.63 and 3.97× more likely to die from HF, respectively, after adjusting for potential confounding variables during an average follow-up of 19.8 years. BMI was also independently and significantly associated with HF mortality. Importantly, mortality rates were lower in fit than unfit men within each BMI strata, particularly within the normal weight and overweight groups. These findings suggest that among men with no personal history of CVD at baseline, measurement of both CRF and BMI may be preferable to measurement of BMI only for assessing risk of future HF mortality. As mentioned, a moderate-to-high level of CRF did not provide as much protection from HF mortality in obese men compared with normal weight and overweight men. On exploring this finding further, we determined that the average MET level for fit–obese men (11.0±1.2) was lower than that in fi t–overweight (12.0±1.7) and fit–normal weight men (13.2±2.2; P for trend <0.0001). Thus, in the obese group, the level of CRF in moderate- to high-fit men may not be sufficiently greater than that in unfit men to provide cardioprotective benefit in HF mortality. An additional novel finding was the marked difference in HF mortality between fit and unfit men with the same number of HF risk factors. HRs for fit men with 0, any 1, or ≥2 risk factors were substantially lower than those in unfit men with the same number of risk factors. For example, among men with ≥2 risk factors, HRs for fit versus unfit were 3.01 and 7.27, respectively (P=0.0002). Thus, a moderate-to-high level of CRF seems to offer substantial protection against HF mortality, irrespective of the number of traditional HF risk factors present. Our findings are consistent with other CCLS articles that have shown that relative to low-fit individuals, attaining a moderate-to-high level of CRF attenuates mortality risk in obese individuals,25 hypertensives,26 type 2 diabetes mellitus individuals,27 and smokers.28 We were also able to compare the relative strength of each risk factor on HF mortality. Low CRF (unfit) and obesity emerged as the 2 strongest risk factors, with HRs of 3.37 and 3.29, respectively (P<0.0001 for each). As previously mentioned, there are few studies in the literature that have examined the relationships among physical activity, adiposity, and HF incidence. In a recent study of 28 842 Finnish men with a mean follow-up of 18.4 years, Hu et al14 reported an inverse association between physical activity and the incidence of HF, as well as a direct association between various adiposity measures and incidence of HF. Joint associations revealed a Farrell et al Fitness, BMI, Heart Failure Mortality 901 Table 2. Baseline Characteristics of 44 674 Men Across Different Categories of Cardiorespiratory Fitness in the Cooper Center Longitudinal Study During 1971–2010 Low Fitness (n=9120) Moderate Fitness (n=17 775) High Fitness (n=17 779) P for Trend Age, y 44.0±9.2 43.6±9.2 42. 9±9.1 <0.0001 BMI, kg/m2 29.7±5.1 26.9±3.2 25.0±2.6 <0.0001 Cardiorespiratory fitness level, METs 8.7±1.1 10.9±0.9 13.8±1.8 <0.0001 Resting heart rate 67.7±10.6 62.6±9.6 56.4±9.5 <0.0001 Systolic blood pressure, mm Hg 124.7±13.8 121.5±12.8 120.1±12.6 <0.0001 Diastolic blood pressure, mm Hg 84.2±9.9 81.9±9.5 79.7±9.0 <0.0001 215.9±42.1 210.0±40.1 199.1±37.3 <0.0001 HDL, mg/dL Cholesterol, mg/dL 41.1±10.5 (n missing=2486) 44.5±11.0 (n missing=2879) 49.9±12.3 (n missing=1956) <0.0001 LDL, mg/dL 136.9±37.5 (n missing=2790) 135.6±35.5 (n missing=3199) 127.6±33.6 (n missing=2057) <0.0001 Triglycerides, mg/dL 184.7±157.2 144.9±109.4 105.5±71.6 <0.0001 Glucose, mg/dL 104.6±24.6 99.8±16.4 97.3±11.0 <0.0001 8.3±11.0 8.4±10.7 8.3±10.4 0.50 Nonsmoker 4215 (46.2) 9971 (56.1) 11 309 (63.6) <0.0001 Former smoker 2272 (24.9) 4449 (25.0) 4659 (22.2) Current smoker 2633 (28.9) 3355 (18.9) 1811 (10.2) 371 (4.1) 300 (1.7) 131 (0.7) <0.0001 Personal history of hypertension, % 2133 (23.4) 2623 (14.8) 1701 (9.6) <0.0001 Family history of CVD, % 3918 (43.0) 7882 (44.3) 7992 (45.0) 0.03 Follow-up, y 21.2±11.1 19.9±10.6 19.0±9.6 <0.0001 Alcohol, drinks/wk Smoking, n (%) Personal history of diabetes mellitus, % Unless otherwise specified, data are means±SD. BMI indicates body mass index; CVD, cardiovascular disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; METs, 1 metabolic equivalent=3.5 mL O2 uptake/kg body weight per minute. protective effect of physical activity across all levels of BMI. For 21 094 male participants in the Physicians Health Study, a strong positive association was reported between BMI and HF incidence, and a strong inverse association was found between vigorous physical activity and HF incidence.13 More specifically, each 1 kg/m2 increase in BMI was associated with an 11% increase in HF incidence, and men who reported vigorous physical activity 5 to 7 days per week were 27% less likely to develop HF compared with men who reported that they rarely or never performed vigorous activity. Within each category of BMI, risk of HF incidence was reduced in men who reported vigorous physical activity. In this same study, the effects of BMI and vigorous activity on HF mortality were shown to be similar to their effects on HF incidence. There are many possible mechanisms by which moderateto-high CRF may be protective against HF mortality. As early as 1972, cross-sectional analyses by Bjorntorp showed that fit middle-aged men had significantly lower insulin responses to a glucose challenge than their unfit peers.29 Numerous training and prospective studies performed since that time have shown that moderate-to-high levels of physical activity are associated with improved insulin sensitivity,30 which in turn Table 3. Adjusted* HRs (95% CIs) for Heart Failure Mortality Across Cardiorespiratory Fitness and BMI Categories in 44 674 Men Who Were Followed for an Average of 19.8±10.4 Years in the Cooper Center Longitudinal Study During 1971–2010 CRF Category Total, n High (Quintile 4–5) Moderate (Quintile 2–3) Low (Quintile) 1 9120 17 779 17 775 HF deaths, n 21 47 85 HR 1.0 1.63 3.97 1.0–2.7 2.4–6.5 Normal Weight Overweight Obese 18.5–24.9 25.0–29.9 ≥30 16 043 21 387 7244 95% CI BMI category, kg/m2 Total, n HF deaths, n 38 74 41 HR 1.0 1.56 3.71 1.1–2.3 2.4–5.8 95% CI P Trend <0.0001 <0.0001 BMI indicates body mass index; CI, confidence intervals; CRF, cardiorespiratory fitness; HF, heart failure; and HR, hazard ratio. *Adjusted for age, examination year, systolic blood pressure, smoking status, family history of cardiovascular disease, and diabetes mellitus. 902 Circ Heart Fail September 2013 NS 6.11 (3.5-10.7) 7.0 HR for HF Mortality 6.0 4.47 (2.1-9.4) 5.0 3.96* (2.1-7.6) 4.0 3.64* (2.1-6.2) Unfit 3.0 2.0 1.0 1.72 (1.0-2.9) Unfit (n=1463) 1.0 Fit (n=17,435) Fit (n=14,580) Normal Weight (18.5-24.9) (n=3705) Fit (n=3539) Unfit (n=3952) Overweight (25.0-29.9) Figure 1. Joint association of cardiorespiratory fitness and body mass index (BMI) in men with adjusted* rates of heart failure (HF) mortality in the Cooper Center Longitudinal Study during 1971–2010. *Adjusted for age, exam year, resting systolic blood pressure, smoking status, family history of cardiovascular disease, and diabetes mellitus. Numbers on top of boxes represent hazard ratios (HRs; 95% confidence interval [CI]). NS indicates nonsignificant. Obese (≥30) BMI (kg/m2) reduces the incidence of type 2 diabetes mellitus31 and metabolic syndrome.32 Furthermore, mortality among individuals with type 2 diabetes mellitus33 and metabolic syndrome34 is significantly lower across increasing levels of CRF. In both cross-sectional35 and prospective studies, moderate-to-high levels of CRF are shown to be associated with more favorable blood lipid profiles,36 decreased resting blood pressure,37 and decreased mortality among those with hypertension,26 as well as a decreased likelihood of developing hypertension.38 In addition to exerting favorable effects on HF risk factors, there is cross-sectional and prospective evidence that exercise training is associated with beneficial structural and functional changes in the myocardium. Levy et al39 found that a progressive 6-month aerobic training program significantly increased end-diastolic volume, absolute peak filling rate, and peak early or single peak diastolic filling rate at rest and during exercise at all matched heart rates in younger (n=17) and older (n=14) men. In cross-sectional analyses, Seals et al40 found that endurance-trained older men had significantly better left ventricular (LV) systolic function than sedentary controls. More specifically, the trained men had greater LV end-diastolic volume at rest and during peak exercise, as well as greater LV exercise reserve (defined as the change in ejection fraction between rest and exercise). In addition, a greater decrease in end-systolic volume was shown in the trained men during exercise than the controls, despite similar increases in systolic blood pressure in the 2 groups. LV fractional shortening was also higher during peak exercise in the trained group. Because the LV wall thickness-to-radius ratio did not differ between the 2 groups, these findings indicated a pattern of volumeoverload LV hypertrophy in the trained men. In a cross-sectional study comparing long-distance runners with sedentary controls, Haskell et al41 found a >2-fold greater vasodilatory capacity of the coronary arteries in the running group than in 7.27*** (4.1-12.8) 7.0 HR for HF Mortality 6.0 5.0 3.77** (2.0-7.0) 4.0 3.01 (1.6-5.6) 2.54* (1.2-5.6) 3.0 Unfit n=4883 2.0 1.0 1.0 Unfit Fit n=11,236 0 n=1326 1.13 (0.6-4.7) Unfit n=2911 Fit n=8888 Fit n=15,433 Any 1 Any 2 or more Number of Risk Factors Figure 2. Adjusted* hazard ratios (HRs) for heart failure (HF) mortality in fit and unfit men based on the number of risk factors in the Cooper Center Longitudinal Study during 1971–2010. *Adjusted for age and exam year. Numbers on top of boxes represent HRs (95% confidence interval [CI]). Risk factors include elevated resting blood pressure (≥140/90 mm Hg) or personal history of hypertension, current smoking, personal history of diabetes mellitus, obesity (body mass index ≥30 kg/m2), and family history of cardiovascular disease.*P=0.02 compared with fit. **P<0.0001 compared with fit. ***P=0.0002 compared with fit. Farrell et al Fitness, BMI, Heart Failure Mortality 903 5.0 HR for HF Mortality 4.0 3.0 2.0 3.29* (2.3-4.7) 3.37* (2.4-4.7) 41 85 2.39* (1.7-3.3) 85 1.71** (1.2 -2.5) NS 1.72 (0.9-3.3) 1.64** (1.2-2.3) 38 10 1.0 Hypertension (n=14,028) Current Smoking (n=7799) Diabetes (n=802) 73 BMI≥30 kg/m2 (n=7244) Unfit (n=9120) Figure 3. Adjusted* hazard ratios (HRs) for heart failure (HF) mortality in men based on the presence of individual risk factors in the Cooper Center Longitudinal Study during 1971–2010. *Adjusted for age and exam year. All comparisons are dichotomies with the referent category being the group who does not have the risk factor. Numbers on top of boxes represent HRs (95% confidence interval [CI]). Numbers in boxes represent HF deaths. *P<0.0001. **P<0.005. BMI indicates body mass index; CVD, cardiovascular disease; and NS, nonsignificant. Family History of CVD (n=19,792) Heart Failure Risk Factor controls during nitroglycerin administration. More recently, greater coronary vasodilation in response to nitroglycerin was shown in a more representative population (physically active older individuals versus less active older individuals). Both daily volume and intensity of activity were significantly correlated to vasodilation.42 These findings remained significant after adjustment for several potential confounders. Fujimoto et al43 examined the effects of a 1-year progressive jogging program on myocardial function in 9 sedentary men and women with a mean age of 70 years. After training, volume-overload LV hypertrophy was shown. Although aerobic power, total aortic compliance, and arterial elastance were significantly improved by training, there was no change in LV stiffness. The authors speculated that the lack of improvement in LV stiffness may have been because of either the age at which the exercise program was initiated or an insufficient duration of training. An important point to consider when interpreting the joint associations of CRF and BMI with HF mortality is the method in which CRF was grouped for this analysis. Currently, there is no widely accepted method of defining CRF levels for use in clinical or public health research. In the CCLS, we standardized the definition of low fitness (unfit) according to the bottom 20% of the age-standardized distribution of maximal exercise duration within the overall CCLS population, with individuals in the remaining 80% of the distribution considered to be fit.19 By our definition, it would thus seem that even modest levels of CRF are associated with lower risk of HF mortality. For example, a 50- to 59-year-old man would need to achieve a maximal MET level of ≥8.9 to qualify for the fit category. This is equivalent to covering ≈1.2 miles in the Cooper 12-minute run-walk test44 or achieving a treadmill time of ≈8.5 minutes on a standard Bruce treadmill test.22 This level of CRF can be achieved by many, perhaps even most, apparently healthy adults through moderate amounts and intensities of aerobic physical activity such as brisk walking.45 Among the strengths of the current study are a large and well-characterized cohort of men, the use of objective measures for CRF and BMI, and an extensive follow-up. Although BMI is a proxy measure of body fatness, it was significantly correlated with percent body fat in the subset of the cohort for whom percent body fat was measured (n=39 971; r=0.68; data not shown). To decrease the possibility that pre-existing disease was present at baseline, men with a BMI <18.5 kg/m2, those who were not able to achieve ≥85% of predicted maximal heart rate, and men with <1 year of follow-up were excluded from analyses. Restricting our analyses to men with ≥3 years of follow-up (n=42 764) did not materially change the strength or patterns of these associations (data not shown), making us more confident that subclinical HF was not a cause of low CRF and subsequent greater HF mortality in the low-fit group. We were also able to adjust for a large number of potentially confounding variables in the multivariate analyses. This study has limitations. The cohort consists of only men who are primarily white and from middle-to-upper socioeconomic strata; therefore, our findings must be cautiously interpreted when generalizing to other populations. This same limitation strengthens the internal validity of our findings by reducing potential confounding by these variables. Furthermore, median levels of CRF in CCLS men are similar to median values obtained on a representative sample of US men.46 We also point out that the overall prevalence of metabolic syndrome among men in the CCLS cohort between 1979 and 2010 is ≈25%, which is similar to the prevalence that has been reported among NHANES (National Health and Nutrition Examination Survey) men in recent years.47 These findings suggest that Cooper Clinic men have similar risk profiles compared with other US men. Using CRF and BMI exposures as categorical rather than continuous variables could also be viewed as a potential limitation. We chose the latter approach because we feel that the use of clinically established cut points is more understandable and useful for healthcare professionals. Because a relatively large number of decedents in the cohort did not have a waist circumference measurement (n=78), we were unable to evaluate the effects of central adiposity on mortality risk. We are reporting only baseline data on adiposity exposures and CRF. It is 904 Circ Heart Fail September 2013 possible that changes in these exposures may have occurred during the follow-up period, which in turn may have influenced our results. An additional limitation includes the absence of more extensive information on smoking habits, such as number of pack-years. The relatively low number of obese men (n=7244; 16%) in the cohort may have limited our ability to detect a significant difference in mortality between fit and unfit obese men. Because the Cooper Clinic did not begin to measure high-density lipoprotein and low-density lipoprotein cholesterol until 1978, we have missing data for these variables in Table 1. We do not have information regarding the presence or absence of sleep apnea in the cohort. Because high alcohol intake (>21 drinks/week) was not significantly associated with HF mortality in our cohort and because a substantial number of men (n=7952) had missing data for the alcohol intake question, we did not include this variable in our multivariate analyses. However, by including men in the analyses who were missing the alcohol intake variable, we were able to increase our number of HF deaths. Finally, we were unable to evaluate medication use or dietary factors in this cohort. In summary, the inverse relationship between baseline CRF and HF mortality in men is quite strong and is materially unaffected by adjustment for BMI and other potential confounders. Within each category of BMI, HF mortality was lower in fit compared with unfit men. Irrespective of the number of risk factors present, fit men had substantially lower HF mortality than unfit men. When examining the individual strength of each risk factor on HF mortality, low CRF (unfit) and obesity functioned as the strongest risk factors. Regardless of the number of HF risk factors present, clinicians are encouraged to counsel their male patients to increase their levels of physical activity with the goal of achieving at least a moderate level of CRF, thereby presumably decreasing their risk of HF mortality. Acknowledgments We thank Kenneth H. Cooper, MD, MPH, for establishing the Cooper Center Longitudinal Study, The Cooper Institute for data management, and Melba Morrow for editorial assistance. Disclosures None. References 1. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. 2. Vijayan VK. Morbidities associated with obstructive sleep apnea. Expert Rev Respir Med. 2012;6:557–566. 3. He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch Intern Med. 2001;161:996–1002. 4. Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, Kannel WB, Vasan RS. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305–313. 5. Chen YT, Vaccarino V, Williams CS, Butler J, Berkman LF, Krumholz HM. Risk factors for heart failure in the elderly: a prospective community-based study. Am J Med. 1999;106:605–612. 6.Johansson S, Wallander MA, Ruigómez A, García Rodríguez LA. Incidence of newly diagnosed heart failure in UK general practice. Eur J Heart Fail. 2001;3:225–231. 7. Savela S, Koistinen P, Tilvis RS, Strandberg AY, Pitkälä KH, Salomaa VV, Miettinen TA, Strandberg TE. Leisure-time physical activity, cardiovascular risk factors and mortality during a 34-year follow-up in men. Eur J Epidemiol. 2010;25:619–625. 8. Khaw KT, Jakes R, Bingham S, Welch A, Luben R, Day N, Wareham N. Work and leisure time physical activity assessed using a simple, pragmatic, validated questionnaire and incident cardiovascular disease and all-cause mortality in men and women: The European Prospective Investigation into Cancer in Norfolk prospective population study. Int J Epidemiol. 2006;35:1034–1043. 9. Nocon M, Hiemann T, Müller-Riemenschneider F, Thalau F, Roll S, Willich SN. Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta-analysis. Eur J Cardiovasc Prev Rehabil. 2008;15:239–246. 10. Apullan FJ, Bourassa MG, Tardif JC, Fortier A, Gayda M, Nigam A. Usefulness of self-reported leisure-time physical activity to predict longterm survival in patients with coronary heart disease. Am J Cardiol. 2008;102:375–379. 11. Tanasescu M, Leitzmann MF, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Exercise type and intensity in relation to coronary heart disease in men. JAMA. 2002;288:1994–2000. 12. Rosengren A, Wilhelmsen L. Physical activity protects against coronary death and deaths from all causes in middle-aged men. Evidence from a 20-year follow-up of the primary prevention study in Göteborg. Ann Epidemiol. 1997;7:69–75. 13. Kenchaiah S, Sesso HD, Gaziano JM. Body mass index and vigorous physical activity and the risk of heart failure among men. Circulation. 2009;119:44–52. 14. Hu G, Tuomilehto J, Silventoinen K, Barengo NC, Peltonen M, Jousilahti P. The effects of physical activity and body mass index on cardiovascular, cancer and all-cause mortality among 47 212 middle-aged Finnish men and women. Int J Obes (Lond). 2005;29:894–902. 15. Wang Y, Hu G. Individual and joint associations of obesity and physical activity on the risk of heart failure. Congest Heart Fail. 2010;16: 292–299. 16. van Poppel MN, Chinapaw MJ, Mokkink LB, van Mechelen W, Terwee CB. Physical activity questionnaires for adults: a systematic review of measurement properties. Sports Med. 2010;40:565–600. 17. Kruger J, Ham SA, Sanker S. Physical inactivity during leisure time among older adults–Behavioral Risk Factor Surveillance System, 2005. J Aging Phys Act. 2008;16:280–291. 18. Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 19992004. JAMA. 2006;295:1549–1555. 19. Blair SN, Kohl HW 3rd, Paffenbarger RS Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989;262:2395–2401. 20. Balke B, Ware RW. An experimental study of physical fitness of Air Force personnel. U S Armed Forces Med J. 1959;10:675–688. 21. Pollock ML, Bohannon RL, Cooper KH, Ayres JJ, Ward A, White SR, Linnerud AC. A comparative analysis of four protocols for maximal treadmill stress testing. Am Heart J. 1976;92:39–46. 22. American College of Sports Medicine. Guidelines for Exercise Testing and Prescription. Philadelphia, PA: Lippincott, Williams & Wilkins; 2009. 23. Stampfer MJ, Willett WC, Speizer FE, Dysert DC, Lipnick R, Rosner B, Hennekens CH. Test of the National Death Index. Am J Epidemiol. 1984;119:837–839. 24. Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr. 1999;69:373–380. 25.Farrell SW, Cortese GM, LaMonte MJ, Blair SN. Cardiorespiratory fitness, different measures of adiposity, and cancer mortality in men. Obesity (Silver Spring). 2007;15:3140–3149. 26. Church TS, Kampert JB, Gibbons LW, Barlow CE, Blair SN. Usefulness of cardiorespiratory fitness as a predictor of all-cause and cardiovascular disease mortality in men with systemic hypertension. Am J Cardiol. 2001;88:651–656. 27. Church TS, Cheng YJ, Earnest CP, Barlow CE, Gibbons LW, Priest EL, Blair SN. Exercise capacity and body composition as predictors of mortality among men with diabetes. Diabetes Care. 2004;27:83–88. 28. Lee CD, Blair SN. Cardiorespiratory fitness and smoking-related and total cancer mortality in men. Med Sci Sports Exerc. 2002;34:735–739. Farrell et al Fitness, BMI, Heart Failure Mortality 905 29. Björntorp P, Fahlén M, Grimby G, Gustafson A, Holm J, Renström P, Scherstén T. Carbohydrate and lipid metabolism in middle-aged, physically well-trained men. Metabolism. 1972;21:1037–1044. 30.Colberg SR, Albright AL, Blissmer BJ, Braun B, Chasan-Taber L, Fernhall B, Regensteiner JG, Rubin RR, Sigal RJ; American College of Sports Medicine; American Diabetes Association. Exercise and type 2 diabetes: American College of Sports Medicine and the American Diabetes Association: joint position statement. Exercise and type 2 diabetes. Med Sci Sports Exerc. 2010;42:2282–2303. 31. Wei M, Gibbons LW, Mitchell TL, Kampert JB, Lee CD, Blair SN. The association between cardiorespiratory fitness and impaired fasting glucose and type 2 diabetes mellitus in men. Ann Intern Med. 1999;130:89–96. 32.LaMonte MJ, Barlow CE, Jurca R, Kampert JB, Church TS, Blair SN. Cardiorespiratory fitness is inversely associated with the incidence of metabolic syndrome: a prospective study of men and women. Circulation. 2005;112:505–512. 33. Wei M, Gibbons LW, Kampert JB, Nichaman MZ, Blair SN. Low cardiorespiratory fitness and physical inactivity as predictors of mortality in men with type 2 diabetes. Ann Intern Med. 2000;132:605–611. 34. Katzmarzyk PT, Church TS, Janssen I, Ross R, Blair SN. Metabolic syndrome, obesity, and mortality: impact of cardiorespiratory fitness. Diabetes Care. 2005;28:391–397. 35. Cooper KH, Pollock ML, Martin RP, White SR, Linnerud AC, Jackson A. Physical fitness levels vs selected coronary risk factors. A cross-sectional study. JAMA. 1976;236:166–169. 36. Durstine JL, Haskell WL. Effects of exercise training on plasma lipids and lipoproteins. Exerc Sport Sci Rev. 1994;22:477–521. 37. American College of Sports Medicine. Position Stand. Physical activity, physical fitness, and hypertension. Med Sci Sports Exerc. 1993;25:i–x. 38. Blair SN, Goodyear NN, Gibbons LW, Cooper KH. Physical fitness and incidence of hypertension in healthy normotensive men and women. JAMA. 1984;252:487–490. 39.Levy WC, Cerqueira MD, Abrass IB, Schwartz RS, Stratton JR. Endurance exercise training augments diastolic filling at rest and during exercise in healthy young and older men. Circulation. 1993;88: 116–126. 40. Seals DR, Hagberg JM, Spina RJ, Rogers MA, Schechtman KB, Ehsani AA. Enhanced left ventricular performance in endurance trained older men. Circulation. 1994;89:198–205. 41. Haskell WL, Sims C, Myll J, Bortz WM, St Goar FG, Alderman EL. Coronary artery size and dilating capacity in ultradistance runners. Circulation. 1993;87:1076–1082. 42.Nguyen PK, Terashima M, Fair JM, Varady A, Taylor-Piliae RE, Iribarren C, Go AS, Haskell WL, Hlatky MA, Fortmann SP, McConnell MV. Physical activity in older subjects is associated with increased coronary vasodilation: the ADVANCE study. J Am Coll Cardiol Cardiovasc Imaging. 2011;4:622–629. 43. Fujimoto N, Prasad A, Hastings JL, Arbab-Zadeh A, Bhella PS, Shibata S, Palmer D, Levine BD. Cardiovascular effects of 1 year of progressive and vigorous exercise training in previously sedentary individuals older than 65 years of age. Circulation. 2010;122:1797–1805. 44. Cooper KH. A means of assessing maximal oxygen intake. Correlation between field and treadmill testing. JAMA. 1968;203:201–204. 45. Stofan JR, DiPietro L, Davis D, Kohl HW 3rd, Blair SN. Physical activity patterns associated with cardiorespiratory fitness and reduced mortality: the Aerobics Center Longitudinal Study. Am J Public Health. 1998;88:1807–1813. 46. Wang CY, Haskell WL, Farrell SW, Lamonte MJ, Blair SN, Curtin LR, Hughes JP, Burt VL. Cardiorespiratory fitness levels among US adults 20-49 years of age: findings from the 1999-2004 National Health and Nutrition Examination Survey. Am J Epidemiol. 2010;171:426–435. 47. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287:356–359. CLINICAL PERSPECTIVE To our knowledge, there are no reported data relating an objective measure of cardiorespiratory fitness with subsequent heart failure (HF) mortality. In this article, we report on 44 674 apparently healthy men who underwent a baseline examination at the Cooper Clinic between 1971 and 2010. Cardiorespiratory fitness was measured via a maximal treadmill stress test. Participants were followed for ≈20 years, during which there were 153 deaths from HF. Adjusted hazard ratios across high, moderate, and low cardiorespiratory fitness categories were 1.0, 1.63, and 3.97, respectively, showing for the first time that baseline cardiorespiratory fitness is an important determinant of subsequent HF mortality. In addition, HF mortality rates were lower in fit than in unfit men within each body mass index strata, particularly within the normal weight and overweight groups. An additional novel finding in our data was the marked difference in HF mortality between fit and unfit men with the same number of traditional HF risk factors. Importantly, the level of fitness at which the risk of HF mortality is lower seems to be modest. Thus, patients who can meet current public health guidelines for physical activity (≥150 minutes per week of moderate intensity aerobic exercise) are likely to be at substantially lower risk with regard to future HF mortality. This is especially true if they are also able to control other HF risk factors such as obesity, hypertension, smoking, and diabetes mellitus.