Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
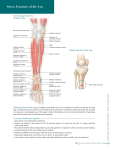
Medial Tibial Periostitis: Shin Splints Normal Leg Anatomy: Anterior View Biceps femoris tendon Patellar tendon Common peroneal nerve Insertion of sartorius muscle Tibial tuberosity Tibialis anterior muscle Deep peroneal nerve Tibia Gastrocnemius muscle Soleus muscle Extensor digitorum longus m. Medial Tibial Periostitis – Shin Splints Cross Section View Superficial peroneal nerve Peroneus longus muscle Fibula Tibia Medial tibial perisostitis Peroneus brevis muscle Inferior extensor retinaculum Peroneus tertius tendon Extensor digitorum brevis muscle Extensor digitorum longus tendon Extensor digitorum brevis tendon Extensor hallucis longus muscle Medial malleolus Tibialis anterior tendon Deep peroneal nerve Extensor hallucis brevis tendon Extensor hallucis longus tendon Tibial Periostitis or Medial Tibial Stress Syndrome (MTSS), more commonly called “shin splints,” is pain that is felt at the front of the lower leg between the knee and ankle. This shin pain occurs when the muscles pull on where they attach to the bone and is caused by overusing or overloading the lower leg. MTSS can occur from activities such as running, dancing or “stop and start” sports like basketball or tennis. It can also occur with a sudden increase in training/activity or in people with flat feet. Symptoms of shin splints include: mild swelling, pain and/or tenderness in the inside front part of the lower leg. Common Treatment Options • Rest. • Apply ice packs to the leg for 20 - 30 minutes every 3 - 4 hours for the first 2 - 3 days until the pain goes away. • Take anti-inflammatory medications such as ibuprofen or naproxen. • Modify activity, training intensity or sport until pain has subsided. Swimming and cycling are usually good options. • Stretch the muscles of the lower leg; especially the ankle and toe flexors. • Surgery is rarely required. © 2 0 1 0 L i p p i n c o t t W i l l i a m s & W i l k i n s | Wo l t e r s K l u w e r H e a l t h Superior extensor retinaculum Lateral malleolus Contact information © 2 0 1 0 L i p p i n c o t t W i l l i a m s & W i l k i n s | Wo l t e r s K l u w e r H e a l t h Notes: