Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
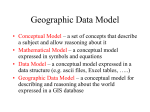
Am J Physiol Heart Circ Physiol 301: H478–H487, 2011. First published May 13, 2011; doi:10.1152/ajpheart.00314.2011. TRANSLATIONAL PHYSIOLOGY Left ventricular mechanical limitations to stroke volume in healthy humans during incremental exercise Eric J. Stöhr,1 José González-Alonso,1 and Rob Shave1,2 1 Centre for Sports Medicine and Human Performance, Brunel University, Uxbridge; and 2Cardiff School of Sport, University of Wales Institute Cardiff, Cardiff, United Kingdom Submitted 29 March 2011; accepted in final form 9 May 2011 twist; torsion; untwisting; diastole IN HEALTHY INDIVIDUALS, the increase in cardiac output at the transition from rest to exercise is achieved by a combination of both enhanced heart rate (HR) and stroke volume (SV) (18, 21, 25). Although some investigators have contested a plateau in SV during incremental exercise (14, 38), a considerable number of studies have shown that SV levels off at ⬃40 –50% of the maximal exercise capacity (18, 21, 22, 25, 26). This leveling off of SV is the result of a plateau in both end-diastolic volume (EDV) and end-systolic volume (ESV) (25). Maintained EDV and ESV suggest that LV filling and ejection do not increase further above moderate exercise intensities. However, this is surprising considering that central venous pressure Address for reprint requests and other correspondence: R. Shave, Univ. of Wales Institute Cardiff, Cyncoed Campus, Cyncoed Road, Cardiff CF23 6XD, UK. H478 and inotropic state appear to increase continuously to the point of task failure (12, 22). Thus the plateau in SV may be related to cardiac mechanical constraints in accommodating a greater EDV or further decreasing ESV. Previous studies have shown that left ventricular (LV) twist and untwisting (“LV twist mechanics”) play an important role in normal systolic and diastolic function at rest, contributing to LV ejection and filling (6, 13, 27, 28, 31). Two recent studies have further demonstrated that systolic and diastolic LV twist mechanics are significantly enhanced in healthy individuals performing low- to moderate-intensity exercise (9, 23), whereas twist and untwisting are unaltered in patients with hypertrophic cardiomyopathy during mild effort (23). Although these findings underline the importance of dynamic twist mechanics for LV function in individuals without any known cardiac disease, the normal response of LV mechanics to exercise at intensities exceeding 40% peak power has never been assessed. It is possible that the previously observed plateau in EDV and ESV despite progressive increases in central venous pressure and contractility may be reflective of an underlying limit in cardiac twist mechanics. The aim of the present study was to examine the relationships between LV twist mechanics and SV, HR, cardiac output, ESV, and EDV to gain insight into the factors underlying the plateau in SV. To determine whether the relationships would be directly caused by the exercise performed, healthy individuals were assessed during both continuous and discontinuous incremental exercise. We hypothesized that a limit in twist mechanics at submaximal exercise intensities is an important factor underlying the leveling off in SV during incremental exercise in healthy individuals. METHODS Study Population Following ethical approval from the Brunel University Research Ethics Committee, nine healthy recreationally active males (age 26 ⫾ 4 yr, height 175.1 ⫾ 4.9 cm, peak power 249 ⫾ 31 W, peak HR 173 ⫾ 14 beats/min) provided verbal and written informed consent to take part in the study. To ensure optimal echocardiographic images, participants were examined for quality of images before enrolment. This study conforms to the code of ethics of the World Medical Association (Declaration of Helsinki). Familiarization and Exercise Testing Participants attended the laboratory a total of four times with visits separated by 48 –72 h. On days 1 and 2, participants were familiarized with supine cycling (Lode, Angio 2003, Groningen, Netherlands) in the left lateral position tilted at a 45° angle [see 0363-6135/11 Copyright © 2011 the American Physiological Society http://www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Stöhr EJ, González-Alonso J, Shave R. Left ventricular mechanical limitations to stroke volume in healthy humans during incremental exercise. Am J Physiol Heart Circ Physiol 301: H478 –H487, 2011. First published May 13, 2011; doi:10.1152/ajpheart.00314.2011.— During incremental exercise, stroke volume (SV) plateaus at 40 –50% of maximal exercise capacity. In healthy individuals, left ventricular (LV) twist and untwisting (“LV twist mechanics”) contribute to the generation of SV at rest, but whether the plateau in SV during incremental exercise is related to a blunting in LV twist mechanics remains unknown. To test this hypothesis, nine healthy young males performed continuous and discontinuous incremental supine cycling exercise up to 90% peak power in a randomized order. During both exercise protocols, end-diastolic volume (EDV), end-systolic volume (ESV), and SV reached a plateau at submaximal exercise intensities while heart rate increased continuously. Similar to LV volumes, two-dimensional speckle tracking-derived LV twist and untwisting velocity increased gradually from rest (all P ⬍ 0.001) and then leveled off at submaximal intensities. During continuous exercise, LV twist mechanics were linearly related to ESV, SV, heart rate, and cardiac output (all P ⬍ 0.01) while the relationship with EDV was exponential. In diastole, the increase in apical untwisting was significantly larger than that of basal untwisting (P ⬍ 0.01), emphasizing the importance of dynamic apical function. In conclusion, during incremental exercise, the plateau in LV twist mechanics and their close relationship with SV and cardiac output indicate a mechanical limitation in maximizing LV output during high exercise intensities. However, LV twist mechanics do not appear to be the sole factor limiting LV output, since EDV reaches its maximum before the plateau in LV twist mechanics, suggesting additional limitations in diastolic filling to the heart. LV MECHANICS AND STROKE VOLUME DURING EXERCISE ing the two trials, the order of exercise stages within the discontinuous trial was also randomized. Following completion of each stage during the discontinuous trial, participants were given up to 10 min recovery in the supine position to allow HR to return to baseline. To avoid changes in hydration status between the continuous and discontinuous exercise test, participants were provided with a 4.5% glucose solution to drink ad libitum after their first trial. Throughout both exercise trials, mean arterial blood pressure (MAP) was assessed using a beat-by-beat arterial blood pressure monitoring system (FinometerPRO, FMS; Finapres Measurement Systems, Arnhem, Netherlands) and recorded continuously for off-line analysis (PowerLab; ADInstruments, Chalgrove, UK). MAP was calculated as the average blood pressure obtained from the beat-by-beat pressure waveforms during the last 2 min of each exercise stage (Chart Version 5.5.6; ADInstruments). HR was recorded continuously via the ECG inherent to the ultrasound (Vivid 7; GE Medical). Fig. 1. Systemic cardiovascular and global left ventricular (LV) function during continuous and discontinuous incremental exercise. Mean arterial pressure, heart rate (HR), and cardiac output increased continuously while end-diastolic volume (EDV), end-systolic volume (ESV), and stroke volume (SV) reached a plateau at submaximal exercise intensities. Filled and open squares represent continuous and discontinuous exercise, respectively. W, workload. Data are means ⫾ SE. #P ⬍ 0.01 between continuous and discontinuous trials (n ⫽ 9). AJP-Heart Circ Physiol • VOL 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Supplemental Video 1 (Supplemental data for this article may be found on the American Journal of Physiology: Heart and Circulatory Physiology website.)]. On day 3, each participant performed a continuous incremental exercise test to volitional fatigue from which individual peak power (Lode, Angio 2003) and peak HR (Vivid 7; GE Medical, Horton, Norway) were determined. On the experimental day, following 10 min of rest on the supine cycle ergometer, each participant performed incremental exercise to volitional fatigue. To have confidence that our results were reproducible and that the observation would be directly related to the exercise performed, each participant completed both a continuous and discontinuous exercise protocol in a randomized order separated by 1 h of rest. Exercise during the continuous and discontinuous trials was performed for 4 min at 25 ⫾ 3, 75 ⫾ 9, 125 ⫾ 15, 174 ⫾ 22, and 224 ⫾ 28 W, which equated to 10, 30, 50, 70, and 90% of the individual peak power attained during the initial continuous incremental exercise to fatigue. In addition to counterbalanc- H479 H480 LV MECHANICS AND STROKE VOLUME DURING EXERCISE Echocardiography Statistical Analysis Data are presented as means ⫾ SD unless otherwise stated. The change in blood pressure and LV function indexes during the continuous and discontinuous protocol was analyzed using repeated-measures ANOVA. Paired-samples t-test was used post hoc to detect differences between conditions; Bonferroni correction was applied to account for multiple comparisons. Comparison between the responses during the continuous and discontinuous trial was performed using two-way repeated-measures ANOVA. Relationships between variables were assessed using Pearson’s product moment correlation. Alpha was set a priori to 0.05. All statistical analyses were performed using STATISTICA (version 6; StatSoft, Tulsa, OK). Table 1. Cardiovascular responses to incremental exercise Workload, %peak power output Heart rate, beats/min Cont Discont EDV, ml Cont Discont ESV, ml Cont Discont SV, ml Cont Discont Q, l/min Cont Discont MAP, mmHg Cont Discont IVRT, ms Cont Discont Control 10% 30% 50% 70% 90% 62 ⫾ 9 63 ⫾ 7 95 ⫾ 10& 105 ⫾ 14* 112 ⫾ 17& 117 ⫾ 21* 134 ⫾ 19& 138 ⫾ 21& 159 ⫾ 18& 147 ⫾ 16*†‡ 171 ⫾ 14& 158 ⫾ 12& P ⬍ 0.001 135 ⫾ 6 128 ⫾ 10 145 ⫾ 13 138 ⫾ 10 153 ⫾ 10* 139 ⫾ 11 153 ⫾ 14* 145 ⫾ 13 153 ⫾ 11* 145 ⫾ 10* 148 ⫾ 18 150 ⫾ 11* NS 46 ⫾ 4 44 ⫾ 6 41 ⫾ 6* 37 ⫾ 8 35 ⫾ 8* 31 ⫾ 8* 28 ⫾ 8*†‡ 26 ⫾ 7*† 26 ⫾ 8*†‡ 28 ⫾ 8* 89 ⫾ 8 84 ⫾ 5 104 ⫾ 11* 101 ⫾ 12* 118 ⫾ 13*† 109 ⫾ 11* 125 ⫾ 15*† 119 ⫾ 13* 127 ⫾ 11*† 117 ⫾ 8* 124 ⫾ 14*† 122 ⫾ 9*†‡ 5.5 ⫾ 0.8 5.2 ⫾ 0.6 9.8 ⫾ 0.7* 10.7 ⫾ 2.5* 13.2 ⫾ 1.9& 12.7 ⫾ 2.5& 16.6 ⫾ 2.0& 16.3 ⫾ 2.7& 20.1 ⫾ 1.8& 17.1 ⫾ 2.0*†‡ 21.1 ⫾ 1.6*†‡$ 19.2 ⫾ 1.5*†‡$ P ⬍ 0.001 79 ⫾ 8 84 ⫾ 9 99 ⫾ 5* 98 ⫾ 8* 104 ⫾ 4* 97 ⫾ 10* 109 ⫾ 6& 110 ⫾ 12*‡ 113 ⫾ 9*†‡ 120 ⫾ 13*†‡ 121 ⫾ 10& 126 ⫾ 12*†‡$ P ⬍ 0.01 75 ⫾ 10 75 ⫾ 16 69 ⫾ 11* 67 ⫾ 12 58 ⫾ 6*† 55 ⫾ 10* 51 ⫾ 10*† 50 ⫾ 12*† 44 ⫾ 9*†‡ 45 ⫾ 12*† 44 ⫾ 11*†‡ 41 ⫾ 14*† NS 24 ⫾ 10*†‡ 28 ⫾ 8* Cont vs. discont NS NS Values are means ⫾ SD. Cont, continuous incremental exercise; Discont, discontinuous incremental exercise; IVRT, isovolumic relaxation time; Q, cardiac output; EDV, end-diastolic volume; ESV, end-systolic volume; SV, stroke volume; MAP, mean arterial pressure. *P ⬍ 0.01 compared with rest. †P ⬍ 0.01 compared with 10%. ‡P ⬍ 0.01 compared with 30%. $P ⬍ 0.01 compared with 50% exercise. &P ⬍ 0.01 compared with 70%. NS, not significant. AJP-Heart Circ Physiol • VOL 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Standard measurements. Echocardiographic images were recorded with a 1.5- to 4-MHz phased array transducer on a commercially available ultrasound system (Vivid 7; GE Medical) at baseline (rest) and during the last 2 min of each exercise stage. All images were taken by a highly experienced trained sonographer. Participants were familiarized with brief periods of end-expiratory breath-hold during exercise. Parasternal short-axis and apical four-chamber views were recorded at end-expiration, and three consecutive cardiac cycles were saved for offline analysis. Because of increasing HRs with incremental exercise, the time that participants had to perform end-expiratory breath-hold to acquire three cardiac cycles was progressively reduced. LV parasternal short-axis images on the level of the papillary muscles were analyzed for end-diastolic and end-systolic diameters. Because of the high HRs during later stages of incremental exercise, we used M-mode with its high temporal resolution (up to 2,000 frames/s; see Ref. 11) to calculate EDV, ESV, and SV according to the method by Teichholz et al. (36). Cardiac output was calculated as the product of HR and SV averaged over three cardiac cycles. Isovolumic relaxation time (IVRT) was assessed using pulsedwave tissue Doppler of the septal mitral annulus as previously described (3). LV speckle tracking twist mechanics. LV systolic and diastolic rotation were assessed from parasternal short-axis images recorded at the LV base on the level of the mitral valve and at the apex as close to the point of end-systolic luminal obliteration as possible (37), which was achieved by moving the transducer one to two intercostal spaces lower than the basal image. To ensure reproducibility of images at all stages of exercise, the position of the ultrasound transducer during baseline assessment was marked on the participant’s chest. This enabled rapid identification of a similar apical imaging window, allowing the sonographer to then visually adjust and acquire comparable cross-sectional views. Furthermore, frame rate was kept constant between all subjects and all conditions at 97 frames/s; imaging depth for both LV basal and apical short-axis views was also standardized within participants (33). A single focal point was positioned in the center of the ventricular cavity for all short-axis images. Images were analyzed off-line for two-dimensional (2-D) speckle tracking-derived basal and apical rotation and rotational velocities (EchoPAC, Version 7.0.0; GE Medical). 2-D speckle tracking was successful at low and high exercise intensities up to near maximal effort (see Supplemental Video 2). To adjust for inter- and intraindividual variability of HR, raw data were exported to a spreadsheet (Microsoft, Seattle, WA) and normalized to the percentage of systolic and diastolic duration, respectively (7). Normalization was achieved by cubic spline interpolation of systolic and diastolic data to 300 points, respectively (GraphPad Prism 5.00 for Windows, San Diego, CA). LV twist, untwisting, and the respective velocities were obtained by subtraction of basal rotation/rotation velocity data from apical rotation/ rotation velocity data. Peak untwisting velocity was determined as the greatest negative deflection following peak twisting velocity. In addition to peak values, the absolute time it took for LV twist indexes to reach their peak was determined from the frame-by-frame speckle tracking analysis and expressed in milliseconds. Comparison between temporal occurrence of mitral valve opening and peak diastolic untwisting velocity was performed to assess whether peak diastolic twist indexes occurred before, simultaneously with, or following mitral valve opening. LV MECHANICS AND STROKE VOLUME DURING EXERCISE RESULTS LV Volumes and Arterial Blood Pressure the increase in LV twist, twist velocity, and untwisting velocity reached a plateau at ⬃50% peak power and remained at this level for all subsequent exercise stages (Table 2). Compared with the discontinuous trial, twist and twisting velocity were significantly higher at 70% peak power during continuous incremental exercise (P ⱕ 0.01); however, all other twist indexes did not differ between the two protocols (P ⬎ 0.05). In both trials, the increase in diastolic apical rotation velocity from rest to 90% maximal exercise capacity was significantly higher than the increase in basal rotation velocity (P ⬍ 0.01, Fig. 3). In addition to the significant change in peak values, temporal analysis showed that peak diastolic apical rotation and peak untwisting velocity reached their peak at the same time as mitral valve opening at all exercise stages (P ⬍ 0.01) while peak LV diastolic basal rotation velocity occurred significantly after mitral valve opening at 70 and 90% maximal exercise capacity (all P ⬍ 0.01, Fig. 4). As shown in Figs. 5 and 6, during continuous exercise LV, twist mechanics correlated linearly with SV, HR, cardiac output, and ESV (P ⬍ 0.01), whereas the relationships between LV mechanics and EDV appeared to have an exponential pattern. Furthermore, during both trials, LV twist and untwisting velocity were strongly related (P ⱕ 0.01, Fig. 7). LV Twist Mechanics Peak LV systolic and diastolic basal rotation, apical rotation, twist, and the respective velocities increased significantly from rest to exercise (all P ⬍ 0.01, Fig. 2). Similar to the SV response, DISCUSSION This is the first study to examine whether the plateau in SV at submaximal exercise intensities is underpinned by Fig. 2. Graphical representation of the mean LV twist mechanics over the course of an entire cardiac cycle during continuous (A) and discontinuous (B) incremental exercise (n ⫽ 9). LV systolic and diastolic twist mechanics increased continuously up to moderate exercise intensities and leveled off thereafter. Red, blue, and black lines represent LV apex, base, and twist, respectively. Vertical lines show aortic valve closure (AVC, solid line) and mitral valve opening (MVO, broken line). Data are means ⫾ SE. Rot, rotation. For the purpose of clarity, error bars have been omitted, but values are provided in Table 2. AJP-Heart Circ Physiol • VOL 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 During the initial stages of both continuous and discontinuous incremental exercise, EDV and SV significantly increased while ESV significantly decreased compared with rest (all P ⬍ 0.01; Fig. 1). Following this initial response, EDV reached a plateau at ⬃30% peak power while ESV and SV leveled off at ⬃50% peak power (Table 1). As a result of the progressive rise in HR, cardiac output increased continuously up to 70% peak power and then also plateaued (all P ⬍ 0.01). Because of a significantly higher HR during the later stages of the continuous trial, the increase in cardiac output was also larger during the continuous protocol (both P ⬍ 0.01). In contrast, the increase in MAP was significantly lower during the later stages of the continuous trial (P ⬍ 0.01). During both continuous and discontinuous exercises, IVRT declined continuously and was not significantly different between trials (P ⬍ 0.01). Body mass was unaltered before and following both protocols (precontinuous: 70.5 ⫾ 8.3 kg; postcontinuous: 70.4 ⫾ 8.4 kg; prediscontinuous: 70.5 ⫾ 8.3 kg; postdiscontinuous: 70.2 ⫾ 8.4 kg; all P ⬎ 0.05). H481 H482 LV MECHANICS AND STROKE VOLUME DURING EXERCISE Table 2. Peak systolic and diastolic LV twist indexes at rest and during incremental exercise Workload, %peak power output Control 10% 30% 50% 70% 90% Cont vs. discont Peak (systole) 13.9 ⫾ 3.9 11.0 ⫾ 4.2 15.4 ⫾ 2.4 17.2 ⫾ 3.9 19.8 ⫾ 5.1* 20.1 ⫾ 6.3* 23.8 ⫾ 6.0*† 25.3 ⫾ 7.0* 26.8 ⫾ 4.2*†‡ 21.2 ⫾ 3.6* 24.7 ⫾ 6.9*† 22.4 ⫾ 3.1* P ⫽ 0.01 10.0 ⫾ 2.7 8.0 ⫾ 3.4 11.7 ⫾ 2.2 14.3 ⫾ 3.4* 15.4 ⫾ 4.7 16.5 ⫾ 4.3* 18.3 ⫾ 5.6*† 19.1 ⫾ 5.4* 19.5 ⫾ 3.1*†‡ 16.8 ⫾ 3.3* 18.5 ⫾ 5.2*† 15.8 ⫾ 2.8* NS ⫺4.4 ⫾ 2.3 ⫺3.6 ⫾ 2.3 ⫺4.2 ⫾ 2.0 ⫺4.2 ⫾ 2.1 ⫺6.2 ⫾ 2.3*† ⫺4.3 ⫾ 2.8*† 103 ⫾ 21 91 ⫾ 22 105 ⫾ 18 130 ⫾ 36 150 ⫾ 31*† 147 ⫾ 42* ⫺63 ⫾ 15 ⫺57 ⫾ 24 ⫺73 ⫾ 19 ⫺71 ⫾ 29 89 ⫾ 22 75 ⫾ 36 107 ⫾ 32* 131 ⫾ 28* ⫺95 ⫾ 30* ⫺74 ⫾ 29 149 ⫾ 37*† 150 ⫾ 30* ⫺6.5 ⫾ 2.6† ⫺7.2 ⫾ 3.7† 200 ⫾ 49*†‡ 208 ⫾ 43*†‡ ⫺8.0 ⫾ 2.5† ⫺5.6 ⫾ 2.2† ⫺7.8 ⫾ 3.3 ⫺7.1 ⫾ 2.5 NS 232 ⫾ 35*†‡ 193 ⫾ 38* 216 ⫾ 42*†‡ 206 ⫾ 53* ⫺141 ⫾ 32*†‡ ⫺106 ⫾ 32* ⫺142 ⫾ 36*†‡ ⫺113 ⫾ 36*† NS 199 ⫾ 45*† 178 ⫾ 53* 192 ⫾ 44*† 163 ⫾ 52* NS 93 ⫾ 41 89 ⫾ 28 122 ⫾ 44*† 93 ⫾ 34* 103 ⫾ 35 90 ⫾ 32 NS ⫺114 ⫾ 42* ⫺113 ⫾ 43*† 183 ⫾ 43*† 177 ⫾ 48* P ⫽ 0.01 Peak (diastole) Basal rot vel, degree/s Cont Discont Apical rot vel, degree/s Cont Discont Untwisting vel, degree/s Cont Discont Untwisting rate, degree/s Cont Discont 67 ⫾ 22 59 ⫾ 19 70 ⫾ 22 65 ⫾ 16 80 ⫾ 22 74 ⫾ 37 ⫺69 ⫾ 18 ⫺66 ⫾ 35 ⫺111 ⫾ 35* ⫺132 ⫾ 57* ⫺165 ⫾ 74* ⫺180 ⫾ 70* ⫺235 ⫾ 76*†‡ ⫺223 ⫾ 99* ⫺301 ⫾ 118*†‡ ⫺235 ⫾ 100*† ⫺267 ⫾ 106*†‡ ⫺254 ⫾ 97*† NS ⫺116 ⫾ 28 ⫺101 ⫾ 38 ⫺147 ⫾ 39 ⫺157 ⫾ 59 ⫺211 ⫾ 61*† ⫺218 ⫾ 96* ⫺286 ⫾ 88*† ⫺264 ⫾ 113* ⫺336 ⫾ 110*†‡ ⫺278 ⫾ 93*† ⫺300 ⫾ 101 ⫺284 ⫾ 94*† NS ⫺66 ⫾ 24 ⫺65 ⫾ 37 ⫺102 ⫾ 32* ⫺111 ⫾ 47 ⫺132 ⫾ 57* ⫺133 ⫾ 61* ⫺202 ⫾ 89*†‡ ⫺150 ⫾ 65* ⫺236 ⫾ 64*†‡ ⫺193 ⫾ 85* ⫺195 ⫾ 50*†‡ ⫺186 ⫾ 83* NS Values are means ⫾ SD. Rot, rotation; vel, velocity. *P ⬍ 0.01 compared with rest. †P ⬍ 0.01 compared with 10%. ‡P ⬍ 0.01 compared with 30%. NS, not significant. constraints in LV twist and untwisting in healthy individuals. There were five novel findings. 1) Similar to the previously observed plateau in SV, LV systolic and diastolic twist mechanics also reached an upper limit at moderate exercise intensities and remained at this level thereafter. 2) The change in LV twist mechanics during incremental exercise correlated with ESV, SV, HR, and cardiac output. 3) At all exercise intensities, enhanced peak LV untwisting velocity was Fig. 3. Peak diastolic rotation velocities at rest and during continuous (A) and discontinuous (B) incremental exercise. Peak diastolic apical rotation velocity was significantly higher at all exercise intensities compared with peak diastolic basal rotation velocity. Consequently, the increase in LV untwisting velocity was almost solely meditated by enhanced apical untwisting. Data are means ⫾ SE. For clarity, all data are expressed as positive values. *P ⬍ 0.01 compared with apical diastolic velocity (n ⫽ 9). AJP-Heart Circ Physiol • VOL 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Twist, degrees Cont Discont Apical rotation, degrees Cont Discont Basal rotation, degrees Cont Discont Twist vel, degree/s Cont Discont Basal rot vel, degree/s Cont Discont Apical rot vel, degree/s Cont Discont LV MECHANICS AND STROKE VOLUME DURING EXERCISE the result of faster apical than basal untwisting. 4) Peak LV untwisting velocity occurred before or simultaneously with mitral valve opening at all exercise intensities. 5) There were little differences in the response of LV twist mechanics between discontinuous and continuous incremental exercise. Together, the findings suggest that, in healthy individuals, maximal systolic and diastolic LV twist mechanics are reached at submaximal exercise intensities. Their close relationship with SV and cardiac output may indicate that a limit in rotational mechanics during moderate- to high-intensity exercise possibly contributes to the plateau in SV. However, the plateau in EDV before the leveling off of LV twist mechanics further suggests that the ability to maximize LV filling may not be related to LV twist mechanics but to peripheral or cardiac structural factors. LV Twist Mechanics and SV In the present study, the changes in EDV, ESV, and SV during continuous and discontinuous incremental exercise were similar AJP-Heart Circ Physiol • VOL to those reported by previous studies, showing an initial increase followed by a plateau at moderate exercise intensities (4, 18, 22, 25). The present data further support the concept of a limit in cardiac function at submaximal exercise intensities by showing that, during both continuous and discontinuous incremental exercise, LV systolic and diastolic twist velocities also reach their peak at moderate exercise intensities. In previous studies, central venous pressure has been shown to increase continuously during incremental exercise up to maximal oxygen consumption (12, 18, 22). Thus, the presently observed plateau in EDV may, therefore, have been related to an inability of the LV to further improve diastolic filling above moderate exercise intensities. During continuous incremental exercise, this does not, however, appear to be related to diastolic untwisting, since diastolic untwisting increased further when maximal EDV had been attained. The mechanisms for the linear increase in EDV during discontinuous exercise and the plateau in EDV during continuous exercise in this study are not clear. Previous studies have shown conflicting EDV responses to incremental exercise, possibly related to differences in training status or posture (supine vs. upright exercise) (14, 25, 38). In relation to this, it must be noted that the present results were obtained during supine cycling exercise and that altered hemodynamics during upright exercise may be associated with different LV twist mechanics. Additionally, it has been shown that greater myocardial compliance plays an important role in the generation of a large EDV at a given filling pressure (20). Maximal LV diastolic expansion may be limited by pericardial constraint (10), especially during high levels of exercise (5). During incremental exercise, the plateau in EDV may thus be caused by the pericardium constraining end-diastolic distension and also reduced filling time due to elevated HRs rather than a limitation in diastolic untwisting performance. While the plateau in EDV did not appear to be directly related to LV mechanics, the plateau in twist and untwisting at high to severe exercise intensities likely contributed to the leveling off of SV, which is supported by the strong correlation between these indexes. In contrast to the curvilinear relationship between twist mechanics and EDV, the strong linear correlation between twist mechanics and ESV is suggestive of a limit in end-systolic function. Previous studies have demonstrated that sympathetic stimulation enhances LV twist mechanics (8, 16) and that, during incremental exercise, sympathetic activity increases progressively up to the point of volitional fatigue (12). Accordingly, it may have been expected that LV twist should also have increased in a similar fashion. Similar to diastolic distensibility, the lack of a continuous increase in LV twist beyond moderate exercise intensities may be indicative of a mechanical constraint during moderate to high levels of exercise. Maximal endsystolic tissue compression may have caused the plateau in peak systolic basal and apical rotation. An inability to twist further during systole would in turn impact diastolic untwisting (15, 17). Although theses hypotheses require further examination, it is plausible that, in the intact human heart during moderate- to high-intensity exercise, the pericardium and tissue compression properties may limit both LV systolic and diastolic twist mechanics, which would consequently contribute to the plateau in SV. Another factor that may have influenced the observed plateau in LV twist mechanics during incremental exercise is the exerciseinduced elevation in arterial blood pressure. In the present study, 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Fig. 4. Time-to-peak diastolic mechanics in relation to the time to MVO. In parallel to the significant reduction in the time to MVO with increasing exercise intensity, time-to-peak LV diastolic apical rotation velocity and untwisting velocity was also shortened, and peaks were reached at the moment of MVO. In contrast, time-to-peak diastolic basal rotation velocity did not shorten continuously and its peak occurred significantly later than MVO at high to severe exercise intensities. Data are means ⫾ SE. *P ⬍ 0.01 compared with time to MVO for base and apex (n ⫽ 9). H483 H484 LV MECHANICS AND STROKE VOLUME DURING EXERCISE although absolute differences were small, MAP was significantly higher during the discontinuous protocol compared with the continuous trial. Conversely, LV twist was significantly lower during the discontinuous protocol. These data are in accordance with earlier findings showing that increased afterload reduces peak LV systolic twist (8). Thus enhanced arterial blood pressure may offset the positive inotropic effect caused by augmented sympa- thetic activity during exercise intensities exceeding 50% maximal capacity and thereby limit the increase in LV twist. Because the energy required for active diastolic untwisting is stored during systole (15, 17), the increase in arterial blood pressure may also indirectly attenuate the increase in LV untwisting velocity. This would explain the strong relationship between systolic twist and diastolic untwisting velocity observed in the present investigation. Fig. 6. Relationships between LV twist mechanics and EDV and ESV during continuous () and discontinuous (Œ) incremental exercise (n ⫽ 9). Although the relationships with ESV were clearly linear, the relationships between LV twist mechanics and EDV during continuous incremental exercise were not significant and appeared more exponential, suggesting that the early plateau in SV is the result of reduced filling that may not be related to cardiac systolic or diastolic mechanics. The y-axes for untwisting velocity are inversed to reflect the increase in untwisting velocity. Data are means ⫾ SE. AJP-Heart Circ Physiol • VOL 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Fig. 5. Relationships between LV twist mechanics and SV, HR, and cardiac output during continuous () and discontinuous (Œ) incremental exercise (n ⫽ 9). The increase in LV twist mechanics correlated significantly with the change in SV, HR, and cardiac output during both continuous and discontinuous incremental exercise. The y-axes for untwisting velocity are inversed to reflect the increase in untwisting velocity. Data are means ⫾ SE. LV MECHANICS AND STROKE VOLUME DURING EXERCISE In addition, Takeuchi and Lang (35) have reported a reduced peak LV untwisting velocity in arterial hypertension at rest, further suggesting an impact of elevated arterial blood pressure on LV twist mechanics. However, in contrast to the present data, Takeuchi and Lang (35) also reported a delay in peak LV untwisting. Our study shows that, during exercise in healthy individuals, despite extensive shortening of the cardiac cycle, peak LV untwisting occurs simultaneously with mitral valve opening at all exercise intensities. Therefore, a delay in peak LV untwisting velocity beyond mitral valve opening during exercise is likely indicative of cardiac dysfunction. Implications for Pathological and Physiological Adaptations Uncoupling of Basal and Apical Twist Mechanics During Incremental Exercise To establish an intraventricular pressure gradient that maximizes LV suction for diastolic filling, pressure at the LV apex must be lower than at the base. Accordingly, during exercise, greater apical untwisting compared with basal untwisting is beneficial for LV filling. Indeed, Doucende et al. (9) showed that the increase in apical untwisting during incremental exercise up to ⬃40% maximal exercise capacity was significantly higher than the increase in basal untwisting. Our data extend these findings by showing that this uncoupling increases more as exercise intensity increases to near maximal levels. This finding underlines the importance of an apical untwisting reserve to meet an enhanced cardiovascular demand in healthy individuals, which may be absent in cardiac disease (23). Furthermore, the previous and present data indicate that, during exercise, a differential response in LV rotation at the base and the apex is normal. Similarly, Akagawa et al. (2) observed a greater increase in apical subendocardial rotation than basal subendocardial rotation following dobutamine infusion in healthy individuals at rest. Some authors have proposed that this response may be caused by region-specific adrenoreceptor sensitivity (24). In this regard, data are available showing that electrical activation at the apex persists longer than at the base (29), which may result in an enhanced Ca2⫹ release and a faster reuptake in apical myocytes. Moreover, we have previously shown that basal rotation predominates over apical rotation during heat stress, a condition that is characterized by a reduction in EDV (34). In contrast, the greater apical rotation during incremental exercise in the present study is likely AJP-Heart Circ Physiol • VOL related to the increase in EDV, as has recently been shown using saline infusion (39). Thus enhanced venous return from the exercising muscles and the resultant increased EDV may have contributed to a change in myofiber alignment and increased LV twist and untwisting in a mechanically more efficient manner (1). Collectively, the present data suggest that the LV apex, in contrast to the base, has a greater “reserve” to respond to exercise. By implication, it follows that the lower potential of the LV base to respond may represent a key factor in the limitation of overall LV twist mechanics to increase beyond moderate exercise intensities. Similar to the observed difference in peak basal and apical rotation, the time taken for diastolic rotation velocities to reach their peak also differed between the base and the apex at higher exercise intensities. Figure 4 shows that, during continuous incremental exercise at 70 and 90% of peak power, peak LV diastolic basal rotation velocity occurred after mitral valve opening, whereas peak apical untwisting still occurred before or simultaneously with the start of early LV filling. Because both peak apical and basal diastolic untwisting plateau at these exercise intensities, it is possible that the higher peak basal untwisting later in diastole is reflective of an enhanced atrial contribution to filling action rather than a reduction in basal function. This agrees with the previous observation of a relationship between peak diastolic basal rotation velocity and early filling velocity during moderateintensity exercise (9). The functional significance of this association during exercise and other conditions of altered hemodynamics and inotropic state is, however, currently not clear and requires further study. In recent years, the number of clinical trials examining LV twist mechanics in acute and chronic pathology has risen steadily (13, 30, 32), yet the normal response of LV twist mechanics to stress in healthy individuals is still poorly understood. In the clinical and athletic environment, exercise tests are frequently used to expose cardiovascular abnormalities and establish physiological performance. The present study provides insight into the normal response of LV twist mechanics during incremental exercise to near maximal exercise capacity. Failure of LV twist mechanics to progressively increase up to moderate relative exercise intensities, peak LV untwisting velocity occurring markedly following mitral valve opening, and apical mechanics not increasing to a greater extent than basal rotation during the course of a diagnostic exercise test may all reflect underlying pathology. Equally, highly trained individuals that have a higher SV at rest and during exercise may display a different response in LV twist mechanics reflecting chronic myocardial adaptations to exercise training. Despite some small differences between trials, the present investigation also demonstrates that LV twist and untwisting are very similar whether incremental exercise is performed continuously or discontinuously. The option to employ a discontinuous protocol, which drastically reduces the time that individuals are exposed to acute cardiovascular stress, may be an important advantage in some populations and conditions. Technical Considerations and Limitations At present, the assessment of LV twist mechanics with 2-D speckle tracking ultrasound entails some inherent methodological 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 Fig. 7. Relationship between LV twist and untwisting velocity during continuous () and discontinuous (Œ) incremental exercise (n ⫽ 9). Systolic twist and diastolic untwisting velocity were closely related during both continuous and discontinuous incremental exercise, suggesting a strong interdependence between systolic and diastolic function in healthy individuals. The y-axis is inversed to reflect the increasing untwisting velocity. Data are means ⫾ SE. H485 H486 LV MECHANICS AND STROKE VOLUME DURING EXERCISE ACKNOWLEDGMENTS We thank all participants for their commitment throughout the study. We also thank Emilie Timlin for excellent assistance during data collection. DISCLOSURES None. REFERENCES 1. Adhyapak SM, Parachuri VR. Architecture of the left ventricle: insights for optimal surgical ventricular restoration. Heart Fail Rev 15: 73–83, 2010. AJP-Heart Circ Physiol • VOL 2. Akagawa E, Murata K, Tanaka N, Yamada H, Miura T, Kunichika H, Wada Y, Hadano Y, Tanaka T, Nose Y, Yasumoto K, Kono M, Matsuzaki M. Augmentation of left ventricular apical endocardial rotation with inotropic stimulation contributes to increased left ventricular torsion and radial strain in normal subjects: quantitative assessment utilizing a novel automated tissue tracking technique. Circ J 71: 661–668, 2007. 3. Alam M, Wardell J, Andersson E, Samad BA, Nordlander R. Characteristics of mitral and tricuspid annular velocities determined by pulsed wave Doppler tissue imaging in healthy subjects. J Am Soc Echocardiogr 12: 618 –628, 1999. 4. Astrand PO, Cuddy TE, Saltin B, Stenberg J. Cardiac Output during Submaximal and Maximal Work. J Appl Physiol 19: 268 –274, 1964. 5. Belenkie I, Smith ER, Tyberg JV. Ventricular interaction: from bench to bedside. Ann Med 33: 236 –241, 2001. 6. Buckberg G, Hoffman JI, Mahajan A, Saleh S, Coghlan C. Cardiac mechanics revisited: the relationship of cardiac architecture to ventricular function. Circulation 118: 2571–2587, 2008. 7. Burns AT, La Gerche A, Prior DL, Macisaac AI. Left ventricular untwisting is an important determinant of early diastolic function. JACC Cardiovasc Imaging 2: 709 –716, 2009. 8. Dong SJ, Hees PS, Huang WM, Buffer SA ,Jr, Weiss JL, Shapiro EP. Independent effects of preload, afterload, and contractility on left ventricular torsion. Am J Physiol Heart Circ Physiol 277: H1053–H1060, 1999. 9. Doucende G, Schuster I, Rupp T, Startun A, Dauzat M, Obert P, Nottin S. Kinetics of left ventricular strains and torsion during incremental exercise in healthy subjects: the key role of torsional mechanics for systolic-diastolic coupling. Circ Cardiovasc Imaging 3: 586 –594, 2010. 10. Esch BT, Bredin SS, Haykowsky MJ, Scott JM, Warburton DE. The potential role of the pericardium on diastolic filling in endurance-trained athletes under conditions of physiological stress. Appl Physiol Nutr Metab 32: 311–317, 2007. 11. Feigenbaum H. Role of M-mode technique in today’s echocardiography. J Am Soc Echocardiogr 23: 240 –257, 2010. 12. Galbo H, Holst JJ, Christensen NJ. Glucagon and plasma catecholamine responses to graded and prolonged exercise in man. J Appl Physiol 38: 70 –76, 1975. 13. Geyer H, Caracciolo G, Abe H, Wilansky S, Carerj S, Gentile F, Nesser HJ, Khandheria B, Narula J, Sengupta PP. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr 23: 351–369, 2010. 14. Gledhill N, Cox D, Jamnik R. Endurance athletes’ stroke volume does not plateau: major advantage is diastolic function. Med Sci Sports Exerc 26: 1116 –1121, 1994. 15. Granzier HL, Labeit S. The giant protein titin: a major player in myocardial mechanics, signaling, and disease. Circ Res 94: 284 –295, 2004. 16. Helle-Valle T, Crosby J, Edvardsen T, Lyseggen E, Amundsen BH, Smith HJ, Rosen BD, Lima JA, Torp H, Ihlen H, Smiseth OA. New noninvasive method for assessment of left ventricular rotation: speckle tracking echocardiography. Circulation 112: 3149 –3156, 2005. 17. Helmes M, Lim CC, Liao R, Bharti A, Cui L, Sawyer DB. Titin determines the Frank-Starling relation in early diastole. J Gen Physiol 121: 97–110, 2003. 18. Higginbotham MB, Morris KG, Williams RS, McHale PA, Coleman RE, Cobb FR. Regulation of stroke volume during submaximal and maximal upright exercise in normal man. Circ Res 58: 281–291, 1986. 19. Kronik G, Slany J, Mosslacher H. Comparative value of eight M-mode echocardiographic formulas for determining left ventricular stroke volume. A correlative study with thermodilution and left ventricular singleplane cineangiography. Circulation 60: 1308 –1316, 1979. 20. Levine BD, Lane LD, Buckey JC, Friedman DB, Blomqvist CG. Left ventricular pressure-volume and Frank-Starling relations in endurance athletes. Implications for orthostatic tolerance and exercise performance. Circulation 84: 1016 –1023, 1991. 21. Mortensen SP, Damsgaard R, Dawson EA, Secher NH, GonzalezAlonso J. Restrictions in systemic and locomotor skeletal muscle perfusion, oxygen supply and VO2 during high-intensity whole-body exercise in humans. J Physiol 586: 2621–2635, 2008. 22. Mortensen SP, Dawson EA, Yoshiga CC, Dalsgaard MK, Damsgaard R, Secher NH, Gonzalez-Alonso J. Limitations to systemic and locomotor limb muscle oxygen delivery and uptake during maximal exercise in humans. J Physiol 566: 273–285, 2005. 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 limitations, mostly pertaining to image quality and through-plane motion of myocardial tissue. While through-plane motion cannot be avoided, it appears to have relatively little impact on tracking of myocardial tissue during incremental exercise, since tracking in the present study was successful in ⬎90% of myocardial segments, indicated by the tracking score provided by the software and confirmed by visual inspection. This successful tracking was likely related to the assessment of echocardiographic image quality in participants before enrolment and the standardization of image acquisition. To ensure accuracy and comparability of data, image acquisition must take into account frame rates (16), imaging depth (33), and the level of the apical short-axis view (37). In this study, a constant frame rate of 97 frames/s between all participants and all conditions was applied. Furthermore, imaging depth within the basal and apical short-axis views was also standardized, and the apical short-axis level was chosen as caudal as possible to estimate the largest “true” LV twist. Despite pronounced differences in myocardial velocities, the pattern of response in apical rotation (high rotational velocity) and basal rotation (low rotational velocity) was very similar in systole and diastole during both trials, which suggests that the observed change during exercise is physiological in nature. Despite the stringent standardization, speckle tracking values may be slightly underestimated because of elevated HRs at higher exercise intensities, although this error was probably minimized by applying cubic spline interpolation and averaging data over three cardiac cycles. The much lower temporal resolution inherent to magnetic resonance imaging and three-dimensional ultrasound modalities would likely result in a greater error in the assessment of LV twist indexes, whereas the present study demonstrates that the assessment of LV twist mechanics with 2-D speckle tracking echocardiography during incremental exercise up to high exercise intensities is feasible. The authors acknowledge that the assessment of LV volumes using the linear Teichholz method is not the current gold standard in echocardiography. However, the Teichholz method was chosen because of the limited amount of time available for image acquisition during each stage of exercise. Moreover, the Teichholz method has been shown to provide accurate estimation of LV volumes in individuals without wall motion abnormalities (19). In conclusion, during incremental exercise, the plateau in LV twist mechanics and their close relationship with SV and cardiac output indicate a mechanical limitation in maximizing LV output during high exercise intensities. However, LV twist mechanics do not appear to be the sole factor responsible for the plateau in SV, since EDV reaches its maximum before the plateau in LV twist mechanics. LV MECHANICS AND STROKE VOLUME DURING EXERCISE AJP-Heart Circ Physiol • VOL 33. Sivesgaard K, Christensen SD, Nygaard H, Hasenkam JM, Sloth E. Speckle tracking ultrasound is independent of insonation angle and gain: an in vitro investigation of agreement with sonomicrometry. J Am Soc Echocardiogr 22: 852–858, 2009. 34. Stöhr EJ, González-Alonso J, Pearson J, Low DA, Ali L, Barker H, Shave R. Effects of graded heat stress on global left ventricular function and twist mechanics at rest and during exercise in healthy humans. Exp Physiol 96: 114 –124, 2011. 35. Takeuchi M, Lang RM. Reduced and delayed untwisting of the left ventricle in patients with hypertension and left ventricular hypertrophy: a study using two-dimensional speckle tracking imaging: reply. Eur Heart J 29: 825– 826, 2008. 36. Teichholz LE, Kreulen T, Herman MV, Gorlin R. Problems in echocardiographic volume determinations: echocardiographic-angiographic correlations in the presence of absence of asynergy. Am J Cardiol 37: 7–11, 1976. 37. van Dalen BM, Vletter WB, Soliman OI, ten Cate FJ, Geleijnse ML. Importance of transducer position in the assessment of apical rotation by speckle tracking echocardiography. J Am Soc Echocardiogr 21: 895–898, 2008. 38. Warburton DE, Haykowsky MJ, Quinney HA, Blackmore D, Teo KK, Humen DP. Myocardial response to incremental exercise in endurancetrained athletes: influence of heart rate, contractility and the Frank-Starling effect. Exp Physiol 87: 613–622, 2002. 39. Weiner RB, Weyman AE, Khan AM, Reingold JS, Chen-Tournoux AA, Scherrer-Crosbie M, Picard MH, Wang TJ, Baggish AL. Preload dependency of left ventricular torsion: the impact of normal saline infusion. Circ Cardiovasc Imaging 3: 672–678, 2010. 301 • AUGUST 2011 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.5 on May 4, 2017 23. Notomi Y, Martin-Miklovic MG, Oryszak SJ, Shiota T, Deserranno D, Popovic ZB, Garcia MJ, Greenberg NL, Thomas JD. Enhanced ventricular untwisting during exercise: a mechanistic manifestation of elastic recoil described by Doppler tissue imaging. Circulation 113: 2524 –2533, 2006. 24. Nottin S, Doucende G, Schuster-Beck I, Dauzat M, Obert P. Alteration in left ventricular normal and shear strains evaluated by 2D-strain echocardiography in the athlete’s heart. J Physiol 586: 4721–4733, 2008. 25. Poliner LR, Dehmer GJ, Lewis SE, Parkey RW, Blomqvist CG, Willerson JT. Left ventricular performance in normal subjects: a comparison of the responses to exercise in the upright and supine positions. Circulation 62: 528 –534, 1980. 26. Rowland T. Endurance athletes’ stroke volume response to progressive exercise: a critical review. Sports Med 39: 687–695, 2009. 27. Russel IK, Gotte MJ, Bronzwaer JG, Knaapen P, Paulus WJ, van Rossum AC. Left ventricular torsion: an expanding role in the analysis of myocardial dysfunction. JACC Cardiovasc Imaging 2: 648 –655, 2009. 28. Sallin EA. Fiber orientation and ejection fraction in the human left ventricle. Biophys J 9: 954 –964, 1969. 29. Sengupta PP, Khandheria BK, Korinek J, Wang J, Jahangir A, Seward JB, Belohlavek M. Apex-to-base dispersion in regional timing of left ventricular shortening and lengthening. J Am Coll Cardiol 47: 163–172, 2006. 30. Sengupta PP, Khandheria BK, Narula J. Twist and untwist mechanics of the left ventricle. Heart Fail Clin 4: 315–324, 2008. 31. Sengupta PP, Korinek J, Belohlavek M, Narula J, Vannan MA, Jahangir A, Khandheria BK. Left ventricular structure and function: basic science for cardiac imaging. J Am Coll Cardiol 48: 1988 –2001, 2006. 32. Shaw SM, Fox DJ, Williams SG. The development of left ventricular torsion and its clinical relevance. Int J Cardiol 130: 319 –325, 2008. H487