Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
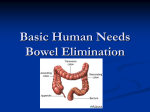
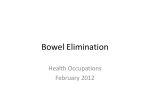
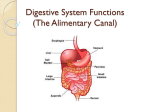
Bowel Elimination Susan L. Maiocco MSN, RN, APN, C A&P • Large intestine – – – – – – Primary organ of bowel elimination Extends from ileocecal valve to anus 5’ in length (adult) 3” width at widest to 1” narrowest Diameter decreases from cecum to anus Functions • Absorption of water • Formation of feces • Expulsion of feces A&P • Waste products of digestion (chyme) move from small intestine through ileocecal valve to cecum. • Large intestine absorns 800-1000mL of liquid daily – Passes to slow-hard stools – Too rapid-watery • • • • Ascending colon Transverse colon Descending colon Sigmoid colon Definitions • Feces – Solid waste products that have reached the distal end of the colon – Ready for excretion • Stool – Feces that have been excreted • Peristalsis – Contractions of the muscles of the intestine – Moves waste products through length of intestine continuously • Hemorrhoids – Abnormally distended veins in rectum • Defecation – Process of bowel elimination • Anus – Opening at end of anal canal A&P • ANS – Innervates muscles of colon – PSN • Stimulates movement – Sympathetic • Inhibits movement – These 2 systems function antagonistically • Mass peristalsis occurs 1-4 times/24 hours after food has been ingested promoting urge to defecate • After passing through sigmoid colon, waste products enter rectum • Stopped from exiting by anal sphincters Defecation • Emptying of the large intestine • External sphincter – Voluntary control • Parasympathetic stimulation – Internal anal sphincter relaxes – Colon contracts – Fecal mass enters rectum – Rectum distends stimulating defecation reflex • Valsalva Maneuver – Bearing down – Contraindicated in cardiac patients • Increases pressure in abdominal and thoracic cavities, decreasing cardiac output • When bearing down ceases, pressure lessened, larger than normal amount of blood flow to heart-elevates BP Factors Affecting Bowel Elimination • Developmental Considerations – Older Adult • Constipation • Daily Patterns • Food/Fluid • Activity/Muscle tone – Regular exercise improves GI motility and muscle tone • • • • Lifestyle Psychological variables Pathologic conditions Medications Nursing Process • Assessment – History – Physical Exam • Inspection, Auscultation, Percussion,Palpation • Anus/Rectum – Superficial exam – Rectal » Left Sims position • Stool characteristics Diagnostic Studies • Stool collection – Patient should void first • • • • • • – Occult blood EGD – Esophagus, stomach, upper duodenum Colonoscopy – Rectal, colon, distal small bowel Sigmoidoscopy – Distal sigmoid colon, rectum, anal canal UGI/Small Bowel Series – Barium swallow-esophagus, stomach, small intestine Barium EnemaAbdominal US – Large intestine MRI – Detailed anatomic views • CT Scan Enemas • Removes feces from colon – Relieves constipation – Prevents involuntary escape of fecal material during surgery – Promotes visualization of the intestinal tract by radiographic or instrument examination – Helps establish regular bowel function Enemas • Cleansing – 500-1000mL – Hypotonic (tap water)-distends intestine, increases periatalis, softens stools – Isotonic (normal saline)-distends intestine, increases periatalis, softens stools – Hypertonic-distends intestine; rritates intestinal mucosa • Commercial • Small volume • Retention – Oil-lubricates; should be retained for 30 minutes – Carminative-expels gas; milk/molasses; MgSO4, glycerin, water – Medicated – Antihelminthic-destroyes parasites – Nutritive • Return flow-expels flatus – 100-200 mL; repeated 5-6 times Emptying the Colon of Feces • Rectal suppositories • Oral intestinal lavage – GoLYTELY – 1-6 hours for clear return • Digital removal of stool – Fecal Impaction • Prolonged retention or accumulation of fecal material that forms hardened mass • Liquid feces seepage with no passage of normal stool is sign of impaction Bowel Incontinence • Inability of the anal sphincter to control the discharge of fecal and gaseous material • Rectal Indwelling catheter • Fecal incontinence pouch Bowel Training Program • Purpose – Manipulate factors within a persons control to produce the elimination of a soft, formed stool at regular intervals without a laxative • • • • Food/fluid intake Exercise Time Establishes regular pattern of defecation Nasogastric Tube • Decompress or drain the stomach of fluid or unwanted stomach contents and when conditions are present in which peristalsis is absent – Paralytic ileus – Intestinal obstruction • Allow GI tract to rest and heal after surgery • Monitor GI bleeding • Lavage Bowel Diversions • Ostomy – Opening in abdominal wall for fecal elimination • Stoma – Intestinal mucosa brought out to abdominal wall – Ilieostomy • Allows liquid fecal content from the ileum to be eliminated through the stoma – Colostomy • Permits formed feces in the colon to exit through the stoma Ostomies Bowel Resection & Colostomy Ostomy Care • Keep the patient as free of odors as possible • Inspect stoma regularly – Color should be dark pink/red • Note size of stoma – Protrudes ½- 1” – Stabilizes 6-8 weeks • • • • Skin care Intake/Output Change appliance Irrigate prn/order Patient Education • • • • • • Community resources are available for assistance. Initially encourage patients to avoid foods high in fiber. Avoid foods that cause diarrhea or flatus. Drink two quarts of water daily. Teach about medications. Teach about odor control (intake of dark green vegetables). • Resume normal activity including work and sexual relations.