Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
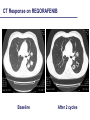
Mario Scartozzi Clinica di Oncologia Medica Ancona HIGHLIGHTS IN COLORECTAL CANCER MANAGEMENT TREATMENT OF METASTATIC DISEASE Bittoni, Giampieri et al, CROH 2012 Colon Cancer: what we already know – Chemotherapy has determined a relevant improvement in survival in the last 15 years: from 6 to 18 months – Probably FOLFOX = FOLFIRI and XELOX=FOLFOX (XELIRI has PHYLOSOPHICAL problems with toxicity) – Concept of all three drugs – Some patients with stage IV disease can be cured by an interdisciplinary approach Colon Cancer: what we already know – Chemotherapy has determined a relevant improvement in survival in the last 15 years: from 6 to 18 months – Probably FOLFOX = FOLFIRI and XELOX=FOLFOX (XELIRI has PHYLOSOPHICAL problems with toxicity) – Concept of all three drugs – Some patients with stage IV disease can be cured by an interdisciplinary approach Not all liver metastases are created equal Bittoni, Giampieri et al, CROH 2012 Multimodality Management of CRC Liver Metastases – Neoadjuvant chemotherapy • Resectable liver metastases: – Facilitate surgery – Obtain predictive and prognostic information – Early systemic therapy for poor-prognosis pts – Conversion chemotherapy • Unresectable liver metastases: – Allow R0 resection via downsizing – Postoperative (adjuvant) chemotherapy • Hepatic arterial infusion (HAI) • Systemic treatment Colon Cancer: NOT all liver metastases are created equal BIOLOGICALLY CHALLANGING Colon Cancer: MULTIMODALITY management – Neoadjuvant chemotherapy • Resectable liver metastases: – Facilitate surgery – Obtain predictive and prognostic information – Early systemic therapy for poor-prognosis pts – Conversion chemotherapy • Unresectable liver metastases: – Allow R0 resection via downsizing – Postoperative (adjuvant) chemotherapy Colon Cancer: MULTIMODALITY management – Neoadjuvant chemotherapy • Resectable liver metastases: – Facilitate surgery – Obtain predictive and prognostic information – Early systemic therapy for poor-prognosis pts – Conversion chemotherapy • Unresectable liver metastases: – Allow R0 resection via downsizing – Postoperative (adjuvant) chemotherapy Colon Cancer: EORTC 40983 (the EPOC trial) FOLFOX4 for 6 cycles (12 wks) (n = 182) • • • • R • • for 6 cycles (12 wks) 364 patients randomized Potentially resectable (≤ 4 liver metastases) Goal: Improve PFS Interim objective: Evaluate tumor response to perioperative CT Perioperative CT (n = 182) – – Surgery FOLFOX4 Surgery 159 (87.3%) underwent surgery 151 (83.0%) resected Surgery (n=182) – – 170 (93.4%) underwent surgery 152 (83.0%) resected (n = 182) Nordlinger B, et al. Lancet 2008 Efficacy Results No. pts CT No. pts Surgery % absolute difference in 3-year PFS Hazard ratio (confidence interval) All patients 182 182 +7.2% (28.1% to 35.4%) 0.79 (0.62-1.02) 0.058 All eligible patients 171 171 +8.1% (28.1% to 36.2%) 0.77 (0.60-1.00) 0.041 All resected patients 151 152 +9.2% (33.2% to 42.4%) 0.73 (0.55-0.97) 0.025 p Value MOSAIC: 3-yr DFS for stage III: +7.2% Adapted from Nordlinger B, et al. Lancet 2008;371(9617):1007-16. 2012 Nordlinger et al Surgery Chemotherapy Biologicals: How Do They Fit Into This Strategy? Colon Cancer: PFS in BEVACIZUMAB trials Wagner et al. Cochrane Review ‘09 Colon Cancer: PFS in anti-EGFR trials Loupakis, Bria E et al. Cancer 2011 BEVACIZUMAB: PFS on TREATMENT! Saltz, et al. ASCO GI 2007 Colon Cancer: NOT all liver metastases are created equal TECHNICALLY CHALLANGING Colon Cancer: MULTIMODALITY management – Neoadjuvant chemotherapy • Resectable liver metastases: – Facilitate surgery – Obtain predictive and prognostic information – Early systemic therapy for poor-prognosis pts – Conversion chemotherapy • Unresectable liver metastases: – Allow R0 resection via downsizing – Postoperative (adjuvant) chemotherapy Colon Cancer: MULTIMODALITY management – Neoadjuvant chemotherapy • Resectable liver metastases: – Facilitate surgery – Obtain predictive and prognostic information – Early systemic therapy for poor-prognosis pts – Conversion chemotherapy • Unresectable liver metastases: – Allow R0 resection via downsizing – Postoperative (adjuvant) chemotherapy What Do We Expect from Ideal Conversion Chemo? •High (anatomical) response rate – RR = goal of therapy in stage IV CRC only for • Conversion therapy • Patients with significant tumor-related symptoms •Good toxicity profile – No hepatotoxicity – No interference with surgery – No interference with liver regeneration Conversion Therapy: Liver Toxicities – 5-FU: hepatic steatosis, associated with increased postoperative morbidity - yellow liver – Irinotecan: non-alcoholic steatohepatitis (especially in obese patients), can affect hepatic reserve and increase morbidity and mortality after hepatectomy - orange liver – Oxaliplatin: hepatic sinusoidal obstruction syndrome, does not appear to be associated with increased risk of perioperative death - blue liver – Both response rate and toxicity should be considered when selecting preoperative CT in patients with colorectal liver metastases Adapted from Zorzi D, et al. Br J Surg 2007;94:274-86. Colon Cancer: Rate of Liver Resections/RR Rate of liver resection following CT Data from studies/retrospective analyses with “selected pts”, only liver MTS (r=0.96) (p=0.002) Selected pts (liver mets) △ ▲ Not selected pts Data from studies/retrospective analyses with “non selected pts” (r=0.74) (p<0.001), solid line Not selected pts: only phase III trials (r=0,67) (p=0.024), dashed line Folprecht et al. Ann Oncol ‘05 FOLFIRI vs FOLFOXIRI: RESULTS FOLFIRI FOLFOXIRI 122 pts 122 pts Confirmed RR 34% 60% <0.0001 R0 surgery (all pts) 6% 15% 0.033 R0 surgery (liver only) 12% 36% 0.017 mPFS (months) 6.8 9.8 <0.001 mOS (months) 16.7 23.4 0.026 P value Falcone A, JCO ‘07 & Masi JNCI’10 Cetuximab: CELIM & RR & R0 resection (LLD) Folprecht et al. Lancet Oncology 2010 Cetuximab: CELIM & RR & R0 resection (LLD) Folprecht et al. Lancet Oncology 2010 Colon Cancer: Rate of Liver Resections/RR Rate of liver resection following CT Data from studies/retrospective analyses with “selected pts”, only liver MTS (r=0.96) (p=0.002) K-RAS wt △ ▲ Not selected pts Data from studies/retrospective analyses with “non selected pts” (r=0.74) (p<0.001), solid line Not selected pts: only phase III trials (r=0,67) (p=0.024), dashed line Folprecht et al. Ann Oncol ‘05 Colon Cancer: Rate of Liver Resections/RR Rate of liver resection following CT Selected pts (liver mets) Data from studies/retrospective analyses with “selected pts”, only liver MTS (r=0.96) (p=0.002) K-RAS wt △ K-RAS mt Not selected pts ▲ Data from studies/retrospective analyses with “non selected pts” (r=0.74) (p<0.001), solid line Not selected pts: only phase III trials (r=0,67) (p=0.024), dashed line Folprecht et al. Ann Oncol ‘05 Cetuximab: CELIM & RR & R0 resection (LLD) Folprecht et al. Lancet Oncology 2010 Colon Cancer: Rate of Liver Resections/RR Rate of liver resection following CT Selected pts (liver mets) Data from studies/retrospective analyses with “selected pts”, only liver MTS (r=0.96) (p=0.002) K-RAS wt K-RAS mt △ ▲ Not selected pts Data from studies/retrospective analyses with “non selected pts” (r=0.74) (p<0.001), solid line Not selected pts: only phase III trials (r=0,67) (p=0.024), dashed line Folprecht et al. Ann Oncol ‘05 Response Rate in anti-EGFR trials Loupakis F, Bria E et al. Cancer 2011 Response Rate in BEVACIZUMAB trials Wagner et al. Cochrane Review ‘09 CT Morphology vs RECIST A - Pretreatment B - Posttreatment C - Pretreatment D - Posttreatment CT Morphology vs Response on BEV RECIST to Determine 234 pts with CRC liver mets treated with chemo + BEV − 50 pts underwent hepatic resection Three blinded radiologists evaluated response of liver mets according to − Standard RECIST criteria − Novel CT morphology criteria Computer Tomographic Tumor Characteristics Morphology group Overall Attenuation Tumor-Liver Interface Pheripheral Rim of Enhancement 3 Heterogeneous III defined May be present 2 Mixed Variable If initially present, partially resolved 1 Homogeneous and hypoattenuating Sharp If initially present, completely resolved Adapted from Chun YS, et al. JAMA 2009;302(21):2338-44. Response Evaluation: Morphology vs. RECIST Patients with unresectable tumor Morphologic response criteria RECIST 1.0 0.8 Proportion surviving Proportion surviving 1.0 0.6 0.4 0.2 0.8 0.6 0.4 0.2 Log-rank p=0.009 Log-rank p=0.45 0.0 0.0 0 10 20 30 40 50 60 0 10 20 Months 30 40 50 60 Months No. at risk Responders 30 30 26 16 6 2 35 34 25 14 3 0 Ronresponder 52 49 25 14 4 1 47 45 26 16 7 3 Adapted from Chun YS, et al. JAMA 2009;302(21):2338-44. Colon Cancer: NEVER (NEVER!) resectable Bad, Bad luck….. Phase III randomized trials: gains in activity and efficacy in 1st line therapy N° of patients RR PFS OS Hurwitz 402 45 vs 35 10.6 vs 6.2 20.3 vs 15.6 No16966 700 38 vs 38 9.4 vs 8 nr Crystal 599 58 vs 40 9.9 vs 8.7 23.5 vs 20 COIN 2445 64 vs 57 8.6 vs 8.6 17 vs 17.9 Nordic 566 47 vs 46 7.9 vs 8.7 19.7 vs 20.3 656 55 vs 48 9.6 vs 8 Ne vs 18.8 Bevacizumab Cetuximab Panitumumab Prime Overall Survival in BEVACIZUMAB trials Wagner et al. Cochrane Review ‘09 Overall Survival in anti-EGFRs trials Loupakis, Bria E et al. Cancer 2011 Phase III randomized trials: gains in activity and efficacy in 2nd line therapy N° of patients RR PFS OS 829 22.7 vs 8.6 7.3 vs 4.7 12.9 vs 10.8 1298 16.4 vs 4.2 4 vs 2.6 10.7 vs 10 597 35 vs 15 5.9 vs 3.9 14.5 vs 12.5 Bevacizumab Giantonio Cetuximab EPIC Panitumumab Peeters Amado JCO 2008 Amado JCO 2008 PFS/DFS for EGFR inhibitors improves across lines of therapy in KRAS wild-type patients 1.2 0.8 Slide Courtesy of A Grothey Adjuvant First line Second line CO.179 Amado8 Study 1817 EPIC6 CRYSTAL5 0 PRIME4 0.2 COIN3 0.4 NORDIC VII2 0.6 N01471 Hazard ratio 1.0 Salvage (single agent) 1. Alberts, et al. JAMA 2012; 2. Tveit, et al. JCO 2012; 3. Maughan, et al. Lancet 2011 4. Douillard, et al. ASCO 2011; 5. Van Cutsem, et al. JCO 2011; 6. Langer, et al. ESMO 2008 7. Sobrero, et al. ASCO GI 2012; 8. Amado, et al. JCO 2008; 9. Karapetis, et al. NEJM 2008 2012 Arnold D, et Al 2012 Arnold D, et Al 2012 Arnold D, et Al 2012 Arnold D, et Al AFLIBERCEPT 2012 Allegra C, et Al 2012 Allegra C, et Al 2012 Allegra C, et Al GI 2009 Kopetz S et AL 2012 Van Cutsem E, et al 2012 Van Cutsem E, et al 2012 Van Cutsem E, et al 2012 Van Cutsem E, et al 2012 Van Cutsem E, et al CT Response on REGORAFENIB Baseline After 2 cycles Bittoni, Giampieri et al, CROH 2012 Bittoni, Giampieri et al, CROH 2012