Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
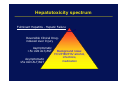
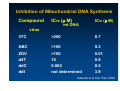
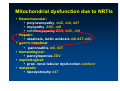
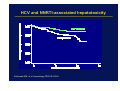
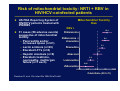
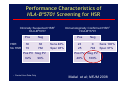
Epatotossicità da farmaci antiretrovirali: ruolo della farmacocinetica e della patologia epatica sottostante Raffaele Bruno Università degli studi di Pavia Liver injury in HIV-infected patients Opportunistic diseases HCV treatment HIV treatment NRTIs, NNRTIs, PIs; OI Rx Immune reconstitution Fatty Liver Disease Hepatitis viruses Alcohol abuse/IVDU Preexisting diseases Incidence/ 100 persons Liver toxicity is the most common severe adverse event in the HAART era Coinfection with hepatitis B or C associated with 4.15 (95% CI 2.26–7.60) hazard ratio of Grade 4 liver toxicity Reisler RB, et al. J Acquir Immune Defic Syndr 2003;34:379–86 How is hepatotoxicity defined? ALT or AST level (number of times ULN) Grade 4 toxicity 10 “Severe hepatotoxicity” Grade 3 toxicity 5 Grade 1 or 2 toxicity ULN → 1 Normal 0 Hepatotoxicity spectrum Fulminant Hepatitis - Hepatic Failure Reversible Clinical Druginduced Liver Injury Asymptomatic >5x ULN ALT/AST Asymptomatic ≤5x ULN ALT/AST Background noise: HCV/HBV/HIV alcohol, infections, medication Liver Disease and Antiretroviral Therapy - Patterns of liver injury z In case series of patients with HIV infection, the prevalence of liver enzyme abnormalities is: – 40%-70% for elevations in ALT, – 20%-40% for elevated alkaline phosphatase, – 0%-10% for increased bilirubin. Bruno et. Al. Am J Gastroenterol 2002 Liver Disease and Antiretroviral Therapy Patterns of Hepatic Injury Cholestatic Mixed Hepatocellular Alanine aminotransferase (ALT) + ++ +++ Aspartate aminotransferase (AST) + ++ +++ Alkaline phosphatase +++ ++ + Gamma glutamyl transpeptidase (GGT) +++ ++ + Liver Disease and Antiretroviral Therapy Probable Mechanisms of Antiretroviral-Induced Hepatotoxicity Drug Class Mechanism Manifestations NRTIs Impaired mitochondrial polymerase gamma function Lactic acidosis, steatosis ? Inhibition of retinoic binding protein Hepatocellular injury, steatosis PIs UDP-glucuronyl NNRTIs ? Impaired transferase competition mitochondrial polymerase gamma ? Immune-mediated hypersensitivity Unconjugated hyperbilirubinemia Lactic acidosis, steatosis Eosinophilic hepatic injury NRTI-related hepatotoxicity z Syndrome of mitochondrial toxicity – Mitochondria have their own DNA (mtDNA) that encodes 13% of mitochondrial proteins – mtDNA is replicated by DNA polymerase γ • Differs from nuclear DNA z NRTIs inhibit DNA polymerase γ – Mitochondrial dysfunction – Cellular toxicity z High-risk drugs – Stavudine, didanosine, zalcitabine z Low-risk drugs – Abacavir, zidovudine, lamivudine, tenofovir 100 11 9 3.6 10 13 1 0.1 0.01 0.01 0.04 0.02 Martin JL, et al. Antimicrob Agents Chemother 1994;38:2743-9 FI A U in e Za l ci ta b ne an os i id D St av id in e ud in e iv La m ov ud in e Zi d ba ca vi r 0.001 A Relative Potency of Inhibition* NRTIs: Inhibition of DNA polymerase γ Effect of NRTIs on mtDNA Content in Liver and Muscle Cells B: Skeletal Muscle Cells Relative mtDNA content (%) A: HepG2 Liver Cells 140 120 3TC Tenofovir 100 Abacavir 80 ZDV 60 d4T 40 20 ddC A 140 Abacavir 120 Tenofovir 3TC ZDV 100 80 60 d4T 40 ddI 20 0 ddC ddI B 0 0.1 1 10 100 1000 NRTI concentration (µmol/L) 0.1 1 10 100 1000 NRTI concentration (µmol/L) Birkus G, et al. Antimicrob Agents Chemother. 2002;46:716-723 Mitochondria Mitochondrion Cell z Energy power-houses z Have their own DNA z Mitochondrial DNA is replicated by a separate enzyme to nuclear DNA Polymerase γ mtDNA mtDNA mtDNA encoded protein function mitochondrion Polymerase γ NRTI nDNA encoded protein mtDNA dysfunction Inhibition of Mitochondrial DNA Synthesis Compound IC50 (µ M) IC50 (µ M) mt DNA virus 3TC >200 0.7 ABC >100 5.3 ZDV >100 0.01 d4T 10 0.9 ddC 0.002 0.5 ddI not determined 3.9 Kakuda et al Clin Ther 2000 Segregation of mitochondria during cell division Normal Mitochondria Dysfunctional Mitochondria Threshold 70% mutant 80% mutant DISEASE 60% mutant NORMAL Progenitor cell showing heteroplasmy of mitochondria At cell division, each daughter cell gets the same nDNA, but varying mtDNA 40% mutant NORMAL 100% NORMAL Mitochondrial dysfunction due to NRTIs y Neuromuscular: y polyneuropathy ddC, ddI, d4T y myopathy ZDV, ddI y cardiomyopathy ZDV, ddC, ddI y Hepatic: y steatosis, lactic acidosis ddI,d4T,ddC y gastro-intestinal: y pancreatitis ddI, d4T y hematological: y pancytopenias ZDV y nephrological: y prox. renal tubular dysfunction adefovir y metabolic y lipodystrophy d4T Energy production in mitochondria glucose pyruvate + NADH FFA cytosol triglycerides Resp chain Acetyl CoA NADH TCA cycle CO2 + H2O NAD+ ketone bodies NAD+ mitochondrion Lactic acidosis glucose pyruvate + NADH FFA cytosol lactate + NAD+ triglycerides Resp chain Acetyl CoA NADH TCA cycle CO2 + H2O NAD+ ketone bodies NAD+ mitochondrion From Hyperlactatemia to Acidosis Source: Medscape NRTI-based liver toxicity: Clinical presentation z Non-specific symptoms – Abdominal pain, vomiting, anorexia, pain (right upper quadrant), weight loss z Hepatomegaly z Mixed cholestatic/hepatocellular pattern of liver enzymes z Evidence of extrahepatic mitochondrial toxicity – Amylase/lipase, CPK, lactate, metabolic acidosis, loss of bicarbonate Falco et al. Clin Infect Dis 2002 HCV and NNRTI-associated hepatotoxicity Sulkowski MS, et al. Hepatology 2002;35:182-9 Risk of mitochondrial toxicity: NRTI + RBV in HIV/HCV-coinfected patients z US FDA Reporting System of Mitochondrial Toxicity HIV/HCV patients treated with IFN/RBV Risk RBV + z 31 cases (58 adverse events) suggestive of mitochondrial toxicity – Pancreatitis and/or increased lipase (n=21) – Lactic acidosis (n=20) – Elevated LFTs (n=8) – Hepatic steatosis (n=6) – Elevated creatinine, neuropathy, multiorgan failure (n=1 each) 12.4 Didanosine Didanosine + stavudine 8.0 3.3 Stavudine 1.1 Abacavir 0.2 Lamivudine 0.06 Zidovudine 0.01 0.1 1.0 10 Odds Ratio (95% CI) Fleischer R, et al. Clin Infect Dis 2004;38:e79-e80 100 Interactions between Mito and CYPs 450 CYPs MITO ROS Lipid peroxidation Fat deposits Mitochondrial disfunction 1 TNF- α 2 3 ROS Lipid Depletion of Peroxidation antioxidans 4 FAT Vicious cycles involving ROS and Mitochondria From ROS to steatohepatitis fibrosis ROS Lipid peroxidation products Cytokines Cell killing (IL-2, IFN-γ ,TNF-α, TGF-β, PDGF) TGF-β Activation Apoptosis Kupffer cell Hepatocytes Hepatic stellate cells FIBROSIS Some ARV Pharmacogenetic Variants z Abacavir HSR (HLA-B*5701)white > black z Efavirenz PK (CYP2B6) z z z z black > white Nevirapine LFTs (ABCB1) black > white Atazanavir jaundice (UGT) white > black Atazanavir PK (PXR?) white > black Nelfinavir (CYP2C19) Asian > black, white To date, every genetic variant that affects HIV disease progression, ARV pharmacokinetics, efficacy, or toxicity differs considerably in frequency depending on geographic region of ancestry. From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Associations Between Allelic Variants and HIV Treatment Response Drug z Abacavir Phenotype Gene Hypersensitivity HLA-B*5701 Lancet 2002:359,727 & 1121; PNAS 2004:101,4180 z Indinavir Jaundice UGT-1A1 Atazanavir PNAS 2001:98,12671; ICAAC 2002; JID 2005;192,1381 z NRTI Lipoatrophy TNF-α promoter, HFE AIDS 2002:16,2013; AIDS 2003:17,121; JID 2008:197, 858 z Nevirapine Hypersensitivity HLA-DRB1*0101, -Cw8, -B3505 Hepatotoxicity ABCB1 Pharmacokinetics CYP2B6 AIDS 2005:19,97; Pharmacogenet Genom 2005;15,1; Clin Inf Dis 2006;43,779 & 783; AIDS 2006:20,1621; AIDS 2007;21,264; Pharmacogenet Genom 2009;19,139 From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Genetic Associations (continued) Drug z Efavirenz Phenotype Slide 28 Gene CNS effects, Pharmacokinetics CYP2B6 ABCB1, CYP2A6 Viral response, Resistance Lancet 2002;359:30; AIDS 2004;18:2391; Pharmacogenet Genom 2005;15:1; JID 2005;192:1931; CID 2006;42:401; CROI 2008; JID 2009;199:872 z Nelfinavir Viral response, Pharmacokinetics CYP2C19 JID 2005;192:1931 z PIs Dyslipidemia APOC, RETN JID 2005;191:1419; PLoS Med 2006;3:e52; AIDS 2008;22:1561. z NRTIs Peripheral neuropathy AIDS 2005;19:1341, AIDS 2006;20:1503 z HAART CD4 recovery JID 2006;194:1098 From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Mitochondrial haplogroup T, HFE Proliferation & apoptosis Genetic Associations (continued) Drug z Tenofovir Slide 29 Phenotype Gene Renal toxicity MRP2 (ABCC2) JID 2006;94:1481 z Others… z ? z ? z ? z ? z ? z ? z ? From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Slide 30 Approved Studies with ACTG Human DNA from US (A5128) Project Papers NWCS 213 – efavirenz, nelfinavir PK & response ◄ 2 NWCS 214 – efavirenz CNS toxicity and PK ◄ 2 NWCS 215 – T cell turnover rates ◄ 1 NWCS 224 – metabolic complications 1 NWCS 233 – CD4 increase on ART ◄ 1 NWCS 237 – metabolic complications * NWCS 238 – peripheral neuropathy ◄ 3 NWCS 239 – efavirenz resistance after Rx interruption ◄ 1 NWCS 243 – HLA and viral evolution * NWCS 248 – efavirenz & lopinavir PK 1 NWCS 253 – efavirenz response ◄ NWCS 254 – efavirenz response ◄ NWCS 256 – peripheral neuropathy ◄ NWCS 259 – metabolic complications NWCS 262 – innate immunity and responses to ART NWCS 266 – treatment responses to ART NWCS 268 – efavirenz PK ◄ NWCS 273 – peripheral neuropathy ◄ NWCS 275 – pharmacogenomics of HIV therapy ◄ NWCS 279 – immune control NWCS 280 – lipoatrophy ◄ From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. NWCS 291 – tenofovir renal toxicity ◄ DNA banked on >10,000 individuals Slide 31 Abacavir hypersensitivity & HLA-B*5701 From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Frequency of HLA-B*5701 Slide 32 W. EUROPE 5-7% US Caucasian ~8% US Asian ~1% MEDITERRANEAN UK 1-2% ~8% MIDDLE EAST 1-2% (NB 5-7% Ashkenazi Jews) INDIA 5-20% CHINA 0% (NB 2.5% N.E. provinces) US AfricanAmerican ~2.5% JAPAN 0% US Hispanic ~2% AUSTRALIA ~8% THAILAND 4-10%* S. AMERICAN Caucasian 5-7% Subsaharan AFRICA <1% *THAILAND B*57 carriage: Urban Bangkok 3.6% Thai Dai Lue (NE Thai) ~11% Southern Thai Muslim 3% Nolan et al J HIV Ther 2003;8:36 From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. “PREDICT” Double-Blind Study Design ABC-containing regimen HSR monitoring according to Standard of Care1 (control arm) ABC-naïve subjects Randomise (1:1) ABC-containing regimen HSR monitoring according to Standard of Care plus HLA-B*5701 screening2 (screening arm) • 6-Week Observation Period 1. retrospective high resolution typing 2. prospective high resolution typing HLA-B*5701 positive subjects excluded HLA-B*5701 negative subjects continued Mallal et al; NEJM 2008. Performance Characteristics of HLA-B*5701 Screening for HSR Clinically Suspected HSR1 HLA-B*5701 HSR No HSR Pos Neg 30 19 36 762 Pos PV Neg PV 62% 1 Control Arm Data Only 96% Sens 46% Spec 98% Immunologically Confirmed HSR1 HLA-B*5701 Pos Neg 23 25 0 794 Sens 100% Spec 97% Pos PV Neg PV 48% 100% Mallal et al; NEJM 2008 DHHS Panel Guidelines (12/07) (http://aidsinfo.nih.gov) “The Panel recommends HLA-B*5701 testing prior to initiating abacavir therapy... HLA-B*5701-positive patients positive status should be recorded as an abacavir allergy in the patient’s medical record….” should not be prescribed abacavir…, From DH Haas, MD, at San Francisco, CA: April 20, 2009, IAS–USA. Why TDM in HIV therapy? Adapted from Acosta EP, et al AIDS Res Human Retro 2002 ART and the liver: Conclusions z Liver-related morbidity and mortality are assuming an increasing importance in HIV care z Each class of antiretroviral agents may be associated with hepatic toxicity z Viral hepatitis co-infection increases the risk of drug- induced liver injury; all co-infected patients must be monitored carefully z Data suggest that treatment of HIV slows progression of fibrosis and reduces liver-related mortality