Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
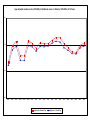
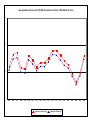
I° FORUM ONCOLOGICA PEDIATRICA DO RIO June 13-15, 2011 The Childhood Cancer System in Ontario An Evolution 1983 - 2011 Mark L. Greenberg, OC, MB, ChB, FRCPC POGO Chair in Childhood Cancer Control, University of Toronto Medical Director, Pediatric Oncology Group of Ontario (POGO) Senior Oncologist, The Hospital for Sick Children, Toronto Outline • Why is a system necessary • The health care context and the challenge in Ontario • What is POGO and the Ontario childhood cancer control system • What have we achieved • The role of data collection, curating and analysis • Is it applicable elsewhere • What have we learned o About the culture o About the process o About the benefits Size Counts! Childhood Cancer = Only 1-2% of cancer incidence PYLL in Childhood Leading causes Of PYLL among children 0-19 Canada 2000 Second biggest killer 1 -14 Breast Childhood Cancer Hodgkin’s Disease Testis Uterus Corpus Oral Cavity Colorectal Uterus Cervix Bladder Non-Hodgkin’s Lymphomas Kidney Lung Ovary Brain Leukemia Melanoma Bleyer, WA CA 40:355-367 Stomach Multiple Myeloma Esophagus Pancreas Prostate 0 400,000 800,000 Years of Life Saved Canadian Health System Healthcare in Canada • • Federal law defines single payer universal health care Delivery is a provincial jurisdiction • Physicians compensated by billing provincial government or in Academic settings by Alternative Payment Plan • Non physician salaries come via a hospital global budget OR for some programs via POGO Childhood Cancer in Ontario The Challenge . . . Average Annual Number of Childhood Cancer Cases, 0-18 Years, Treated in POGO Centres by LHIN of Residence: 2003-2008 L12 15 L11 39 L9 45 L8 53 L5 29 L3 22 L2 26 L1 16 Source: POGONIS L10 16 L7 31 L4 47 L6 37 L13 15 L14 * Pediatric Cancer in Ontario EVERY YEAR About ~ 500 children are newly diagnosed 4000 are in active treatment/early follow up • Cure rate ~ 80% • About 100 children die The Cancer Control Continuum Prevention Screening Diagnosis Treatment Supportive Care Why Did We Need a POGO? Five individual hospitals competing for resources and providing unequal services Childhood cancer overlooked for years o Its unique planning imperatives were not understood SYSTEM” required to allow oIndividuals to look beyond their institutional interests oAll health care providers to help shape the future system o Equity of access, to excellent state-of-the-art treatment oPlanning for expanded diagnostic and treatment options oEngagement of policy/decision makers re: resources Ministry of Health Funding, Pre-1994 ADULT ONCOLOGY CARE PEDIATRIC ONCOLOGY CARE HOW TO people WHAT TO people The DATA HOW TO people WHAT TO people Critical Considerations for Planning • Small numbers widely spread • Small volume, high tech, high intensity specialty • Treatment provided under protocols developed from clinical trials and complimentary practice guidelines • Specialist tertiary expertise is the core of the system o Requires – Comparably resourced centres of expertise – Cross referral and devolution where possible • Obligation/responsibility for care does not end when treatment ends Planning Requires Rationalization of services and centres of excellence Regional co-ordination and planning Easy movement among tertiary/quaternary services Access to pediatric sub-specialties Team-based, multi-disciplinary care Long-term follow-up Excellent data for provincial surveillance/planning COLLABORATION, COLLABORATION, COLLABORATION The POGO Collaboration A Childhood Cancer Control System POGO Partner Programs Tertiary Centres Satellite Centres CH-LHSC London AfterCare Clinic WRH Windsor MCH-HHS Hamilton CHEO Ottawa SRH Sudbury OSMH Orillia SickKids Toronto CHEO Ottawa CH-LHSC London TOHRCC Ottawa SRHC Newmarket GRH Kitchener SickKids Toronto KGH Kingston MCH-HHC Hamilton CVH Mississauga PMH Toronto RVHS Toronto East KGH/KRCC Kingston What is POGO? • Stable (28 years) legally incorporated not-for-profit body o Registered charitable status • Supra-institutional • Fixed staff with primary allegiance to provincial vision • Funded by Ministry of Health and Long-term Care o Other ministries secondarily – – o o Education Child and Youth Services Research grants Philanthropy – for initiatives not appropriate for government funding What is POGO? • Medical Director who holds endowed academic chair o o Cross-appointed at several constituent institutions Primary appointment at POGO • Fulltime Executive Director • Board representative of o Senior staff of all centres and all disciplines – o Charged by law as trustees to have the aims and objects of POGO as their prime responsibility when wearing POGO hat External members with specific expertise – – – – Finance Governance Human resources Health policy What are POGO’s Roles? • Co-ordinate and improve childhood cancer system • Advise Ministry on childhood cancer policy • Select, standardize, collect and analyze provincial data to support policy and service planning • Ensure strategic and equitable allocation of health care resources • Identify growth areas, gaps o Develop, cost and recommend solutions/strategies • Develop evidence driven, consensus-based standards and guidelines What are POGO’s Roles? • Catalyze support for needed programs based on evidence and data • Oversee and support implementation of province-wide programs via partner institutions o o o Guidelines (re) development Ongoing professional education Standardized, aggregate data analyzed to report service output, demographics, etc. • Research in defined spectrum • Education & knowledge transfer and exchange (KTE) At the Interface of Ontario’s Childhood Cancer Organizations, POGO is Optimally Placed to have the Greatest Impact for the Largest Number Childhood Cancer Community Partners CCS, Research Organizations Government (Provincial, Federal) Universities Private Sector Hospitals Provincial Pediatric Oncology System Integrated System of Care Mechanism for Evaluation/Research Parental/Family Services & Shield AfterCare Clinics Tertiary/Quaternary Network Financial assistance Interlink Satellite Network • • • • POGO Research Unit Epidemiology Health Services Economics Status of Survivors/Quality of Life • • • • • • • POGONIS Incidence Disease Markers Treatment Details Psychosocial Data Patient Outcomes AfterCare Database Service Planning Annual workload- and service deliveryreporting by Tertiary, Satellite, AfterCare Partners, and Interlink Education planning Shifting Staff to Patient Ratios POGONIS Data Content Overview General Profiles • Demographics – Patient/Family • Sociographics – Patient/Family • Psychographics – Patient/Family Death Record Disease Diagnoses Status Markers Medical Treatments • POGO Centres • Satellite Programs • Other/Non-POGO Late Effects Health Service Utilization Data Surveillance Activity • Population profile • Service delivery demand/volumes • Incidence, treatment, and outcome trends analyses • System performance measures o Process o Outcomes o Efficiency/effectiveness Age adjusted incidence rate (/100,000) of childhood cancer in Ontario, 1985-2004, 0-14 Years 16 14 12 10 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 Adjusted to Ontario Pop 1995 1996 1997 1998 Adjusted to World Pop 1999 2000 2001 2002 2003 2004 Age adjusted incidence rate (/100,000) of leukemia in Ontario, 1985-2004, 0-14 Years 6 5 4 3 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 Adjusted to Ontario Pop 1995 1996 1997 1998 Adjusted to World Pop 1999 2000 2001 2002 2003 2004 Provincial Childhood Cancer Cases & Service Volumes Five-Year Average Annual Pediatric Oncology Cases in Ontario New Cases 1,2 485 Ongoing Active Treatment and Active Follow-Up Cases 3,4,5 1,999 6 Pediatric Long-Term Follow-Up/ AfterCare 3,6,7 2,022 Total Caseload 3,8 4,021 Source: POGONIS 1. 2. 3. 4. 5. 6. 7. 8. Based on most recent 5-year average available from POGONIS (CY 2005-2009) New Cases include new malignancies, neoplasms of indeterminant behaviour (NIB) and limited registry (LR) patients. Based on the most recent 5-year average available from POGONIS (CY 2004-2008) Ongoing Active Treatment Cases include those undergoing chemotherapy, radiation, surgery or other therapies not in the first year of diagnosis. Active Follow-Up Cases are monitored for cancer recurrence for 2 years after acute treatment ends. Based on provincial tertiary data; however, data is currently being reviewed/ validated with one tertiary hospital. Pediatric Long-Term Follow-Up/ AfterCare includes pediatric cases two years after treatment end date who are being followed by their primary oncologist or in pediatric AfterCare. Total Caseload includes new cases, ongoing active treatment and active follow-up cases and pediatric long-term follow-up/ AfterCare cases. Pediatric Oncology Cases in Ontario CY 2004 to 2009 New Childhood Cancer Cases, Ontario Total Childhood Cancer Caseload, Ontario (Source: POGONIS) (Source: POGONIS) 600 500 400 5-Year Average (2005-2009): 485 300 200 100 0 2004 2005 2006 2007 2008 2009 5,000 4,500 4,000 3,500 3,000 2,500 2,000 1,500 1,000 500 0 5-Year Average (2004-2008): 4,021 2004 2005 2006 2007 2008 Five-Year Average Annual Active Treatment & Active Follow-Up Service Volumes in Ontario1 FY 2005/06 – FY 2009/10 Ambulatory Visits Source: Management Information System (MIS) database Inpatient Days Source: Discharge Abstract Database (DAD) Inpatient Admissions Source: DAD Average Length of Stay (in days) Source: DAD 32,899 26,640 2,932 9.1 1. Reported data is retrieved by standardized query of populationbased administrative databases (as identified in the table). The query is provided by POGO and is used by all POGO partner Decision Support Units. Active Treatment & Active Follow-Up Service Utilization Trends in Ontario FY 2004/05 – FY 2009/101 40,000 Ambulatory Visits, Ontario Inpatient Days, Ontario (Source: Management Information System) (Source: Discharge Abstract Database) 35,000 35,000 30,000 30,000 25,000 25,000 20,000 20,000 15,000 15,000 5-Year Average 32,899 10,000 5,000 5-Year Average 26,640 10,000 5,000 0 0 2004/05 2005/06 2006/07 2007/08 2008/09 2004/05 2009/10 2006/07 2007/08 2008/09 2009/10 Average Length of Stay (in days), Ontario Inpatient Admissions, Ontario (Source: Discharge Abstract Database) (Source: Discharge Abstract Data) 12.0 3,500 10.0 3,000 8.0 2,500 6.0 2,000 1,500 5-Year Average 9.1 days 4.0 5-Year Average 2,932 1,000 2.0 500 0.0 0 2004/05 1. 2005/06 2005/06 2006/07 2007/08 2008/09 2009/10 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 Active treatment and active follow-up service utilization data prior to FY 2004/05 under review using standardized query of population-based administrative databases for tertiary centres other than SickKids. AfterCare Service Utilization Trends in Ontario1 FY 2005/06 – FY 2009/10 Provincial Pediatric and Adult AfterCare New Cases Provincial Pediatric and Adult AfterCare Cases Seen (Source: Annual Service Metrics reported by AfterCare Data Managers) (Source: Annual Service Metrics Reported by AfterCare Data Managers) 500 2,500 400 2,000 300 1,500 5-Year Average 398 200 100 5-Year Average 2,114 1,000 500 0 0 2005/06 2006/07 2007/08 2008/09 2009/10 2005/06 2006/07 Provincial Pediatric and Adult AfterCare Ambulatory Visits 3,000 (Source: Annual Service Metrics Reported by AfterCare Data Managers) 2,500 5-Year Average 2,536 2,000 1,500 1,000 500 0 2005/06 2006/07 2007/08 2008/09 2009/10 2007/08 2008/09 2009/10 Privileged Data Custodian Status Provides the ability to link POGONIS data with third party population databases, e.g. Hospital Discharge Database Physician Billing Database Vital Stats, others Putting it All Together POGO Exports • To developed countries o USA, Australia, UK and provinces across Canada o Program guidelines, prototypes and database architecture/content/expertise • To developing countries o Jordan, Egypt, India, Central America (Guatemala, Nicaragua, Costa Rica, Panama, etc.) o Safe handling guidelines, nursing leadership mentoring and program prototypes Knowledge Transfer Successes Value Added by POGO Integrated vision of childhood cancer control Leadership Rationalization of services Consensus-based, stakeholder-inclusive, planning Education Standardization of available data Equity of access to equivalent care across the province Critical Success Factors of Model dynamic problem identification + expertise-based leadership + multi-centre, multi-source input + excellent provincial data (45.1) + dedicated, knowledgeable Ministry consultant/team + provincial integration and coordinated delivery system = implementable system with built-in refinement/renewal HOW TO people WHAT TO people The DATA HOW TO people WHAT TO people POGO Partner Programs Tertiary Centres Satellite Centres CH-LHSC London AfterCare Clinic WRH Windsor MCH-HHS Hamilton CHEO Ottawa SRH Sudbury OSMH Orillia SickKids Toronto CHEO Ottawa CH-LHSC London TOHRCC Ottawa SRHC Newmarket GRH Kitchener SickKids Toronto KGH Kingston MCH-HHC Hamilton CVH Mississauga PMH Toronto RVHS Toronto East KGH/KRCC Kingston Five-Year Average Annual Satellite Activity in Ontario 1,2 FY 2005/06 – FY 2009/10 New Referrals 119 Patients Treated 3 328 Ambulatory Visits 4,256 Inpatient Days 827 Inpatient Admissions 232 Average Length of Stay (in days) 3.6 Source: Annual Service Metrics Reports submitted by Satellite Nurse Coordinators 1.Sudbury Regional Hospital (SRH) provides long-term follow-up to a portion of the patients followed for AfterCare due to the distances from their tertiary centres. These cases have been excluded from Satellite service volumes from FY 2006 to FY 2010 inclusive. 2.A seventh Satellite centre, Southlake Regional Health Centre, Newmarket, began operation of its Satellite program in February 2009. 3.Patients Treated include POGO’s Satellite clinic new referrals and ongoing cases. Five-Year Average Annual AfterCare Service Volumes in Ontario FY 2005/06 – FY 2009/10 Pediatric and Adult AfterCare New Cases1,2 398 Total Cases Seen1,3 2,114 Total Cases Enrolled 3 (FY 2010 Cumulative) 3,823 AfterCare Visits 1 2,536 Source: Annual Service Metrics Reported by AfterCare Data Managers 1.Sudbury Regional Hospital (SRH) POGO Satellite partner provides long-term follow-up to a portion of the patients followed for AfterCare due to the distances from their tertiary centres. These cases have been included in the AfterCare service volumes from FY 2006 to FY 2010 inclusive. 2.New Cases refer to all survivors who have completed treatment for at least 2 years and who are seen in an AfterCare clinic. 3.Total cases seen refers to new cases plus carry-over seen in AfterCare in the years summarized. 4.Total patients enrolled refers to the total patients enrolled in AfterCare, where they may or may not be served in a given year but have been seen in AfterCare at least once; does not include patients lost to follow-up, defined as those who have missed scheduled AfterCare follow-up appointments for 3 or more years. The Patient Event Model Patient Demographics Snapshot information i.e. most current Patient Current Status Patient timeline Event Event Event Event Event Name Temporal information Data Form Data Form Data Form Data Form Data in temporal context POGO Mission • To improve the circumstances of all children afflicted with cancer, and those of their families and caregivers • To ensure equitable access to, and availability of, state-ofthe-art cancer care for all Ontario children through research, planning and advocacy • To facilitate team-based, multi-disciplinary care - treating the whole child and the whole family • To build consensus within the childhood cancer community re: directions for growth and standards of care • To carry out cancer surveillance • To facilitate unique population focused research