Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
MEDICINE
This text is a
translation from
the original
German which
should be used
for referencing.
The German
version is
authoritative.
REVIEW ARTICLE
Self-Inflicted Injuries:
A Forensic Medical Perspective
Steffen Heide, Manfred Kleiber
SUMMARY
Introduction: Deliberate self harm (DSH) is the term for self inflicted physical injury without
suicidal intent. Among plethora of motivations, it is possible to distinguish between psychological,
legal and material causes. Methods: Selective literature review and dicsussion. Results: Reliable
incidence data on deliberate self harm, which ranges from cutting to limb amputation, are
lacking in Germany. However, data emerging from academic departments of forensic medicine
suggest that periodic clusters of so-called "copycat" DSH episodes arise, in response to episodes
of self harm publicized in the media. Discussion: Self-inflicted injuries show characteristic
features which can be used to distinguish them from injuries inflicted by third parties. The sooner
self harm is recognized as such, the sooner medical help can be offered and possible judicial
consequences avoided.
Dtsch Arztebl 2006; 103(40): A 2627–33.
Key words: self-inflicted injuries, self-mutilation, forensic medical reports, simulation of a criminal
offence, insurance fraud
S
elf-injury as an act of deliberate deception to avoid service in the Roman army was
described as early as the second century AD (1). In recent decades, the phenomenon
has received greater attention from the public at large, particularly because of a large number
of purported "racist" attacks with skin injuries in the shape of the Nazi swastika (2). In the
contemporary view, self-injury may express a psychopathological disorder that can be
considered a disease in its own right; if not, it may still require medical treatment because
of its physical manifestations. This group of patients must be treated with empathy, but also
with the professional diagnostic objectivity of the physician who is aware of the existence
and motivation of self-inflicted injuries committed with the intent to deceive.
The topic "self-injury" has had an expanding presence on the Internet over the last few years
(a Google search now reveals ca. 1,260,000 entries containing this term). Not surprisingly, this
complex entity and the reasons for it are usually dealt with quite superficially. The marked
degree of suffering of the affected persons is revealed in anonymous chat rooms.
Deliberate self-harm is defined as an injury inflicted on oneself without suicidal intent.
Reliable statistics on its incidence in Germany are lacking (3). The English-language
literature reports a prevalence of 0.6% to 0.8% of the population, with overrepresentation
of individuals between 15 and 35 years old. Women are affected two to five times more
often than men (4).
Reliable statistics are even more difficult to find concerning the relative proportions of
deliberate, goal-directed self-injury (e.g., with the intent to deceive persons in authority,
parents, or intimate partners) on the one hand, and overt or hidden self-destructive behavior
based on psychopathology on the other. The two categories overlap with a large "gray area,"
rather than a clear boundary, in between. It may thus be difficult or impossible to render a
clear diagnosis in certain cases. There is no question that expertise in forensic medicine is
required (3, 4).
It is clear from the publications of academic departments of forensic medicine (2, 4, 5, 6,
7) that the extent to which forensic medical expertise is requested in such cases, and the
manner in which the above-mentioned "gray area" is dealt with, vary widely from one
region to another. It is also clear that temporal clusters periodically arise, often because of
imitative self-injuries after widely publicized cases. It seems impossible a priori to assess
the extent of the "dark zone" of self-injuries that are never detected as such. These certainly
exist and are handled by the criminal justice system.
Institut für Rechtsmedizin, Martin-Luther-Universität Halle-Wittenberg (Dr. med. Heide, Prof. Dr. med. habil. Kleiber)
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
1
MEDICINE
DIAGRAM
The motives and causes of self-inflicted injuries
The motivations for self-injury are exceedingly diverse (Diagram) and often multifactorial.
The types of injury are diverse as well, ranging from superficial scratches to limb amputation.
According to Sachsse (8), self-injurious behavior as a clinical phenomenon represents
the far end of a spectrum of normal human behavior. Fingernail chewing, hair extraction,
and the like are part of everyday behavior for nearly everyone. Debate will probably remain
on whether the placing of extreme and excessive demands on oneself, in sports or at work,
should already be considered a type of "self-injurious behavior" (4, 8).
Overt self-injury without any intent to conceal one's own responsibility for the deed is
distinguishable from covert self-destructive behavior. Certain types of injury are characteristic
of particular causes or motivations for deliberate self-harm (3, 4, 9).
The medical aspects of self-inflicted injuries are relevant to physicians in a number of
specialties, including general practitioners. Particular aspects are of special relevance to
each discipline. Forensic physicians are concerned above all with the distinction between
self-inflicted injuries and those inflicted by others. The present review of self-inflicted injuries
from the forensic physician's point of view is based on the authors' practical experience and a
survey of the current literature. We will point out characteristic types of injury that should
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
2
MEDICINE
draw the clinician's attention to
the possibility of self-inflicted
injury and its consequences.
Self-inflicted injury for
psychological gain
Self-injurious behavior is a
relatively common manifestation
of mental disorders and diseases.
The psychological gain that is
obtained can take many forms:
sympathy, attention, sexual
pleasure, recognition, admiration,
or satisfaction of a desire for
revenge.
The pattern of self-inflicted
injury is more homogeneous in
persons with the emotionally
unstable personality disorder of
borderline type than in other
psychiatric patients (10). The
leading manifestation is overt
self-injury of the skin with
numerous, parallel, usually
superficial cuts or scratches
(Figure 1) in areas that are
Figure 1: Numerous cuts and scratches of varying ages on the arm
relatively insensitive to pain.
of a deceased woman with borderline personality disorder (cause of
Cigarette burns may be found
death: suicide by carbamazepine overdose).
as well. According to Sachsse
(11), the psychodynamic functions of self-injurious behavior in borderline personality
disorder are manifold. On the one hand, it serves intrapersonal functions, acting as a global
pressure valve and tranquilizer in states of excess tension, or else as an antidepressant or a
form of self-punishment. On the other hand, in serves interpersonal functions, providing an
intense, non-verbal appeal to others, or a means of escape from excessive demands placed
on the individual by society.
Self-inflicted injuries are also seen in histrionic, dissocial, or paranoid personality disorder,
though less commonly than in borderline patients (10). Neurotic patients most often injure
their own skin by scratching, rubbing, or biting. Severe auto-aggression, on the other hand,
tends to occur in schizophrenia, affective psychoses, oligophrenia, and organic brain disease.
Paranoid hallucinatory schizophrenia, in particular, may manifest itself in bizarre injuries,
mainly involving the violent use of sharp implements. The spectrum ranges all the way to
autocastration and limb amputation (12).
Artificial disorder is characterized by the simulation, exaggeration, or deliberate production
of manifestations of illness. Well-known examples include cutting, scratching, or abrasive
injuries, the self-injection of infectious or toxic material, or the reopening of surgical
wounds (13).
Such patients undergo repeated hospitalization and are often subjected to extensive
diagnostic and therapeutic procedures. Over the course of the disease, permanent damage
ensues, sometimes severe enough to merit the term "mutilation." A subgroup of patients
with artificial disorder contains those with Münchhausen's syndrome, who present with a
detailed history of invented events (pseudologia phantastica), a bizarre collection of
symptoms, and multiple hospitalizations ("hospital hopping").
It is a matter of personal opinion whether certain procedures on the body, such as
tattooing or piercing, that are fashionable in some places and times for sociocultural reasons,
should be considered a type of normal human behavior or a type of deliberate self-harm.
An intensified form of such practices is the infliction of a burning or cutting injury to
produce a desired scar pattern ("branding," "cutting"). The term "body modification" also
covers the visible implantation of pins or other, larger metallic objects on the body surface,
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
3
MEDICINE
as well as splitting of the tongue
(14).
Self-injury for judicial
advantage
Self-injuries to simulate a crime
are usually cutting and scratching
injuries and often show typical
features. Most of the affected
persons are girls and young
women; some are young men.
The "attacks" are described
in relatively uniform fashion,
though the motives can be
very diverse. The underlying
motivation is often to attract
public attention and sympathy.
In other cases, it is to justify an
illicit absence or a late return
home (Figure 2). The particular
Figure 2: 47 individual scratches on the abdomen of a 38-year-old difficulty created by this group
man after a "racist attack" (self-injury to provide an alibi for an extra- of cases is that the deceptive
marital affair).
act, intended for a specific
purpose, automatically activates
the criminal justice system, whether this was the initial intent or not. The proceedings thus
set in motion may have a snowball effect that overwhelms the "victim."
Crimes with a political or xenophobic motive are simulated in order to obtain the maximum
advantage (appellative function) for the "victim." A common variant, breaking an especially
strong taboo, is the scratching of a swastika or the SS double thunderbolt into the skin.
Persons also sometimes injure themselves to incriminate police officers, overseers, and
teachers, to conceal a suicide attempt, or to hide their own misdeeds (e.g., burglary or
embezzlement) (15). The relevant passages in the German criminal code are those dealing
with the simulation of a crime (§145) and, when a specific person is blamed, false
incrimination (§164) or defamation (§187).
Precise data on the frequency of self-injury for judicial advantage are not available. In
2004, according to the statistics of the German Federal Department of Criminal Justice
(Bundeskriminalamt), 13,696 cases of "simulation of a crime" were registered. Some of
these incidents, however, did not involve self-injury (simulated theft, etc.). Patients with
factitious injuries may account for as many as 2% of persons treated in dermatological
clinics (16), yet cases of the type discussed here, such as the simulation of a crime motivated
by xenophobia, are relatively rare, though they sometimes attract nationwide attention.
Self-injury for material gain
Persons in investigative custody are particularly prone to self-injurious behavior. Common
mechanisms include the refusal of food, cutting injuries, self-poisoning, and even the
swallowing of foreign bodies, such as table utensils. These acts may have an appellative
character, as a demonstration of alleged innocence; other possible motivations include providing
a means of escape, alleviating prison conditions, or effecting a transfer to another facility.
Self-injury to avoid military service was more common in the past. Reported types of
self-injury for this purpose include shooting oneself through a piece of ration bread (in
order not to produce the telltale signs of a short-range bullet wound), finger injuries, the
consumption of spoiled rations, and deliberate smear infections (17).
Self-injury for insurance fraud usually consists of the self-amputation of one or two
fingers (usually the thumb and/or index finger of the non-dominant hand) with a sharp
implement; less commonly, an entire hand is amputated (18), and presses, hammers, or
other blunt tools are occasionally used (19). Most affected persons are men. The "accident"
usually occurs in the private sphere and without witnesses. 90% of cases are claimed within
the first 6 months of coverage. About 75% of these persons have more than one insurance
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
4
MEDICINE
policy, and the limbs are often
insured for unusually large
sums of money (20). Precise
information on the frequency of
this type of insurance fraud is
lacking; Gerlach (21) conservatively estimates that there are at
least 200 traumatic limb amputations in northern Germany
over a 10-year interval. Selfinflicted injuries are not separately
listed among the 11,743 cases
of insurance fraud reported in
police statistics for 2004.
Extensive descriptions of selfinflicted injuries for insurance
fraud are provided by Dotzauer
(22), Bonte (18), Püschel (23),
and Möllhof (17), among others.
The medicolegal investigation of potentially self-inflicted
injuries requires the use of all
available sources of information, such as photographs, x-rays,
operative reports, and medical
examination reports (19). The
findings should be thoroughly
Figure 3: Reconstruction of a self-injury for insurance fraud: note the documented with photographs
marked discrepancy between the alleged position of the ax and the taken from a number of diffecourse of the amputation line through the first metacarpal bone.
rent angles (17). The site of
injury, as well as the amputated
body part, should be inspected for the nature of the cut edges, the course of the amputation
line, and any accompanying injuries (22). Traces of injections, if present, may indicate the
prior administration of a local anesthetic; a chemical toxicological study may be indicated.
The injured person should be asked to describe the course of the alleged accident precisely.
Descriptions of deliberate injuries are often at considerable variance from the objective
findings. A visit to the site and an inspection of tools and materials (for bloodstains,
precautionary measures, etc.) may be necessary for a reconstruction of the event (body
posture, position of the hands). Figure 3 shows a major discrepancy between the alleged
position of the ax and the course of the amputation line through the 1st metacarpal bone in
the reconstruction of an "accident" involving amputation of the left thumb.
Most genuinely accidental ax-blow injuries are accompanied by injuries to the neighboring
fingers; thus, an isolated, complete, proximal amputation of the index finger should prompt
suspicion of self-injury (23). In accidental injuries, the edge of the wound is usually irregular
and its course oblique, while, in self-injuries, it tends to be relatively sharp, and the angle of
the cut perpendicular.
So-called tentative injuries adjacent to the actual amputation wound are an important
sign of the deliberate amputation of a finger (22). Other suspicious features pointing toward
self-injury include unusual provisions in the insurance policy, a lack of witnesses or the
influencing of witnesses after the fact, inexplicable disappearance of the amputated body
part, hasty cleaning of the "scene of the accident," and false statements about right- or lefthandedness (18, 22).
It is indisputable that physicians acutely treating persons with self-destructive behavior
must not let their care be negatively influenced by their own ethical or moral attitudes to
such behavior. The unsparing exposure of self-injury with fraudulent intent, with its far-reaching consequences, is certainly not the physician's primary duty, yet the physician should
not shirk this responsibility in his or her capacity as the relevant professional expert. Not all
cases of possible self-injury can be submitted to a judicial inquiry for a final determination
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
5
MEDICINE
(§34 of the German Criminal Code). Ultimately, this decision, like many others that
physicians must make, is a personal matter that is up to one's own conscience.
Differential diagnosis
The medical examination of victims of violence should take place as soon as possible after
the event, particularly for the securing of biological evidence. A forensic physician may be
consulted by the police or by medical colleagues, victim-protection organizations, or legal
advisers.
One of the responsibilities of the physician examining victims of violent crime is to
consider, in every case, the possibility of a self-inflicted injury. The necessary medical
objectivity must be preserved despite the physician's empathy for the presumed victim.
If a self-inflicted injury is not recognized as such, the result may be a continuation or
reinforcement of the self-injurious behavior and a roadblock along the path to appropriate
help for the underlying mental disturbance (16).
The forensic medical examination must take the entire body in view, as even trivial injuries
may be of great importance to the overall assessment. The type, size, location, and color of
all wounds should be exactly described and photographically documented both in survey
images and in close-ups, with a ruler to indicate the scale. Blood or urine specimens may
need to be analyzed if it is thought that alcohol, medications, or illicit drugs may have been
involved in the causation of the violent event.
Important distinguishing criteria for self-inflicted injuries, as opposed to those inflicted
by others, are the intensity, location, surface area, structure, and overall severity of the
injury (Table).
Sometimes the forensic medical examination reveals the presence of nearly all of the
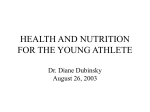
pathognomonic criteria for a self-inflicted injury (24). Figure 4, for example, shows an injury
allegedly inflicted by skinheads on a wheelchair-bound young woman. Each of the about
30 individual scratches runs evenly in a straight line. The scratches are parallel, meet at
right angles, and rarely extend beyond the points where two orthogonal lines meet;
together, they form a precisely drawn, immediately recognizable swastika.
Our experience in forensic medicine indicates that the characteristic features listed in the
Table hardly ever suffice to establish the diagnosis conclusively in individual cases, yet the
more criteria fulfilled, the greater the suspicion of a self-inflicted injury. Discrepancies between the "victim's" description of the event and the objective findings may further strengthen this suspicion. Police detective work may also turn up the implements used, such as a
knife or razor blade, in the individual's possession, sometimes with traces of blood, as well
as the presence or absence of bloodstains at the alleged scene of the crime. At times, even
self-inflicted injuries may be
quite deep (e.g., a stab injury
entering the peritoneal cavity)
or in atypical locations (stab
wounds on the back; see
Reference (4)).
Though the list of typical
features and accompanying
circumstances is long, no
schematic flowchart or checklist
for self-inflicted injuries can be
given that would guarantee a
correct diagnosis in every case.
The indispensable initial step
for clinicians confronted with
this situation is simply to
consider the possibility that the
injury might be self-inflicted.
The physician suspecting
a
self-inflicted injury must
Figure 4: Swastika scratched into the left cheek of a 17-year-old
proceed
with extreme sensitivity
female high school student, with the typical features of a self-inflicted
injury.
and awareness of the attendant
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
6
MEDICINE
TABLE
Characteristic features of self-inflicted injuries versus injuries inflicted by others
Feature
Injuries inflicted by others
Self-inflicted injuries
Type of injury
Usually stab wounds,
occasionally cuts
Nearly always cutting or scratching injuries
or blunt trauma
Number of individual injuries
A large number is rare
Often present in large numbers
Location
Anywhere on the body
Preference for easily accessible parts of the body not
covered by clothing (e.g., limbs, cheeks, forehead,
anterior trunk); sparing of sensitive areas (e.g., lips,
nipples); the back and other inaccessible areas are
hardly ever injured; usually on the side opposite the
dominant hand
Arrangement
Random
Often in groups; there may be large numbers of
parallel injuries, arranged in rows; symmetrical
Form and nature
or individual injuries
Usually short, sometimes of variable
or markedly curved shape, forming
no particular overall figure
Often long, constant in shape, only mildly curved;
may form geometric shapes, symbols, letters,
or words
Intensity of individual injuries
Highly variable, often deep
Always superficial; notably even depth of injury
(also on body surfaces that are not flat)
Fine structure of
individual injuries
Hardly any
Branching patterns, accurate start of new lines
Overall severity of injury
Usually severe or very severe
Nearly always mild or very mild
Self-defense injuries
Common, usually deep; most frequently Absent or atypical, superficial cuts on the fingers,
on the palms, flexor surfaces of the
hands, and forearms
fingers, and ulnar surface of the forearms
Clothing
Included in the injury in a manner
Usually not harmed, or harmed in a manner
corresponding to the presumed posture that is not congruent to the injury
during the attack; many signs of struggle
Accompanying injuries
of other types
Common
Very rare
Evidence of repeated injury
(old scars)
Rare
Often, linear scars of varying ages
modified from 7, 15, 25
difficulties. The diagnosis should be communicated to the patient in a kind and empathic
manner, yet without leaving any possibility of doubt. The patient need not be immediately
and forcefully confronted with the need for treatment (16). There may still be a chance to
point out to the patient that unnecessary difficulties will be avoided if he or she refrains
from making a complaint to the police (4). Sometimes psychiatric or psychotherapeutic
help will only be accepted after a latency period in which the physician offers multiple
times to act as an intermediary.
If a complaint to the police has already been made or cannot be avoided for other reasons,
the police should be informed in timely fashion of the suspected diagnosis of self-injury, so
that they will not embark on an extensive and fruitless search for the supposed perpetrators.
Even when it has become clear that the simulated crime was actually a case of self-injury,
the district attorney has the discretion not to prosecute, despite the fact that the simulation
of a crime itself constitutes a punishable offense. The criminal proceedings can be suspended,
or punitive measures can be dispensed with (§153b of the German criminal procedure
regulations), on the basis of a low degree of guilt or lack of public interest (§153) or upon
the fulfillment of requirements imposed by the authorities (§153a). If the individual has
already been charged with an offense, the court can still terminate the proceedings by
agreement with the prosecution.
Conflict of Interest Statement
The authors declare that no conflict of interest exists according to the Guidelines of the International Committee of Medical
Journal Editors.
Manuscript received on 10 October 2005, final version accepted on 30 March 2006.
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
7
MEDICINE
Translated from the original German by Ethan Taub, M. D.
REFERENCES
This text is a
translation from
the original
German which
should be used
for referencing.
The German
version is
authoritative.
1. Möllhof G, Schmidt G: „Selbstbeschädigungen“ – psychiatrische, rechts- und versicherungsmedizinische
Aspekte (I). Versicherungsmed 1998; 50: 226–31.
2. Püschel K, Kleiber M, König HG, Strauch H: Zum Verletzungsmuster bei Selbstbeschädigung. In: Festschrift für
Gunther Geserick. Heppenheim: Helm 1999; 71–81.
3. Banaschack S, Madea B: Selbstbeschädigung. In: Madea B: Praxis der Rechtsmedizin. Berlin, Heidelberg, New
York: Springer 2003; 268–73.
4. Kernbach-Wighton G: Selbst zugefügte Verletzungen. Rechtsmed 2004; 4: 277–93.
5. Behrmann K, Wienberg H, Püschel K: Zur Vortäuschung von Sexualdelikten. Eine Untersuchung unter
Berücksichtigung selbst beigebrachter Verletzungen. Kriminalistik 1990; 44: 207–10.
6. Kernbach-Wighton G, Thomas RS, Saternus KS: Selbstverletzendes Verhalten: Rechtsmedizinisch-psychiatrischer
Vergleich zu Verletzungsformen und Betreuungsstrategien. In: Saternus KS, Kernbach-Wighton G: Selbstbeschädigung. Forensische Bewertung und Therapiemöglichkeiten. Rechtsmedizinische Forschungsergebnisse Band 14. Lübeck: Schmidt-Römhild 1996; 71–86.
7. Pollak S, Reiter C, Stellwag-Carion C: Vortäuschung von Überfällen durch eigenhändig zugefügte Schnitt- und
Stichwunden. Arch Kriminol 1987; 179: 81–93.
8. Sachsse U: Kommunikationsmechanismen bei selbstverletzendem Verhalten (SSV) - SSV als Kommunikation.
In: Saternus KS, Kernbach-Wighton G: Selbstbeschädigung. Forensische Bewertung und Therapiemöglichkeiten. Rechtsmedizinische Forschungsergebnisse Band 14. Lübeck: Schmidt-Römhild 1996; 103–16.
9. Trübner K, Stiller D, Heide S, Kleiber M. Verletzungsmuster als Ausdruck psychischer Erkrankungen. In: Marneros
A, Rössner D, Haring A, Brieger P: Psychiatrie und Justiz. München: Zuckschwerdt Verlag 2000; 219–24.
10. Herpertz S: Self-injurious behaviour – Psychopathological and nosological characteristics in subtypes of
self-injurers. Acta Psychiatr Scand 1995; 91: 57–68.
11. Sachsse U: Selbstverletzendes Verhalten – somatopsychosomatische Schnittstelle der Borderline-Persönlichkeitsstörung. In Kernberg OF: Handbuch der Borderline-Störungen. Stuttgart: Schattauer 2000; 347–70.
12. Koops E, Püschel K: Selbstverstümmelung und Autophagie. Arch Kriminol 1991; 186: 29–36.
13. Eckhardt A: Artifizielle Störungen. Dtsch Arztebl 1996; 93: A 1622–6.
14. Benecke M: First report of nonpsychotic self-cannibalism (autophagy), tongue splitting, and scar patterns
(scarification) as an extreme form of cultural body modification in a western civilization. Am J Forensic Med
Pathol 1999; 20: 281–5.
15. Pollak S: Vortäuschung einer Straftat. In: Brinkmann B, Madea B: Handbuch der gerichtlichen Medizin, Band I.
Berlin, Heidelberg, New York: Springer 2004; 1230–8.
16. Püschel K, Kleiber M, Erfurt C: Morphologie und Rekonstruktion des Trauma Vortäuschung einer Straftat
durch selbstbeigebrachte Verletzungen. Hautnah päd 1994; 6: 170–7.
17. Möllhof G, Schmidt G: „Selbstbeschädigungen“– psychiatrische, rechts- und versicherungsmedizinische
Aspekte (II). Versicherungsmed 1999; 51: 30–5.
18. Bonte W: Self-Mutilation and private accident insurance. J Forensic Sci 1983; 28: 70–82.
19. Pollak S: Verletzungen durch eigene oder fremde Hand. In: Brinkmann B, Madea B: Handbuch der gerichtlichen Medizin, Band I. Berlin, Heidelberg, New York: Springer 2004; 250–7.
20. Penning R: Selbstbeschädigung – Selbstbeibringung. In: Penning R: Rechtsmedizin systematisch. Bremen,
Lorch: UNI-MED Verlag 1997; 71–2.
21. Gerlach D: Die rechtsmedizinische Beurteilung von Selbstbeschädigungen an Gliedmaßen. Beitr Gerichtl Med
1983; 41: 327–31.
22. Dotzauer G, Iffland R: Selbstverstümmelungen in der privaten Unfallversicherung. Z Rechtsmed 1976; 77: 237–88.
23. Püschel K, Hildebrand E, Hitzer K, Al-Hashimy S: Selbstverstümmelung als Versicherungsbetrug. Unfallchirurgie 1998; 24: 75–80.
24. Kleiber M: Morphologie der Selbstbeschädigung. In: Saternus KS, Kernbach-Wighton G: Selbstbeschädigung.
Forensische Bewertung und Therapiemöglichkeiten. Rechtsmedizinische Forschungsergebnisse Band 14.
Lübeck: Schmidt-Römhild 1996; 11–7.
25. König HG: Spurentechnischer Vergleich realer und fingierter Überfälle. In: Saternus KS, Kernbach-Wighton G:
Selbstbeschädigung. Forensische Bewertung und Therapiemöglichkeiten. Rechtsmedizinische Forschungsergebnisse Band 14. Lübeck: Schmidt-Römhild 1996; 23–49.
Corresponding author
Dr. med. Steffen Heide
Institut für Rechtsmedizin
Martin-Luther-Universität Halle-Wittenberg
Franzosenweg 1
06112 Halle/S., Germany
[email protected]
Dtsch Arztebl 2006; 103(40): A 2627–33 ⏐ www.aerzteblatt.de
8