Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
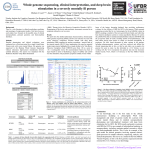
100,000 genomes project and haematological malignancy Dr Andrew Mumford Clinical Director www.genomicseducation.hee.nhs.uk/news West of England Genomics Medicine Centre WEGMC Governance Structure 5 WEGMC objectives 2016-18 1. Enable access to 100,000 genomes project for WoE patients. Whole genome sequencing and ‘omics’ of 4,650 samples from patients and families with rare diseases or cancer. 2. Integrate genomic medicine into standard clinical care pathways. Set up timescale First RD samples 10th June Designation as GMC 23rd Dec Go-live Cancer (NBT) and RD (UHB) 27th May First cancer sample 27th June 01/16 01/17 Launch event Future programme Week 21 152 RD samples 34 cancer samples 1. Who is eligible? 2. Why whole genome sequencing? 3. How does is work for solid cancers? 4. How could it work for haematological malignancy? 1. . Who is eligible? 2. Why whole genome sequencing? 3. How does is work for solid cancers? 4. How could it work for haematological malignancy? 100,000 genomes project includes Cancer and Rare Diseases Genome samples Approved cancers October 2016 1. Ovarian cancer 2. Lung cancer 3. Prostate cancer 4. Colorectal cancer 5. Breast cancer 6. Sarcoma 7. Renal cancer 8. Melanoma 9. Upper gastrointestinal tumours 10.Testicular cancer 11.Childhood solid tumours 12.Adult brain tumours 13.Bladder cancer 14.Endometrial cancer 15. Haematological malignancy 1. Who is eligible? 2. Why whole genome sequencing? 3. How does is work for solid cancers? 4. How could it work for haematological malignanacy? Why whole genome sequencing ? PLT 64 PLT 78 Case 1 PLT 45 MPV 10.1 fl Candidate genes for genetic platelet disorders Next generation sequencing: Bait library design Next generation sequencing •Coding sequence of selected genes: gene panels •Coding sequence of all genes: whole exome • While exome + regulatory regions: whole genome Seelection of a candidate gene PLT 64 CYCS THC4 (OMIM #612004) PLT 78 Case 1 PLT 45 MPV 10.1 fl RUNX1 FT-PAML (OMIM #601399) Case 2 Whole genome sequencing of cancer tissue 1. Who is eligible? 2. Why whole genome sequencing? 3. How does is work for solid cancers? 4. How could it work for haemato-oncology? Defining and testing enrolment process Overview schematic for cancer pathway …How it works Key features of Preliminary report • Domain 1: variants in ‘Actionable Genes’ – annotated for gene-level and variant level actionability – variant level actionability hyper-linked to Genome Oncology (MyCancerGenome.gov) – good, contemporaneous UK clinical trials annotations (ClinicalTrials.gov) • Domain 2: variants in ‘Cancer-related Genes’ • QC metrics: – per sample: % neoplastic cells (pathology), tumour purity (sequence) – per sequence: GL/tumour mapped reads, insert size, chimeric reads, median coverage, ‘eveness’ of coverage – per variant: VRF 1. Who is eligible? 2. Why whole genome sequencing? 3. How does is work for solid cancers? 4. How could it work for haematological maliganancy? Why haematological malignancy? 1. Fifth most common cancer in UK 2. Majority relapse, progress or therapy related morbidity 3. Molecular diagnostics to improve prognostic estimates and direct targeted therapies already standard care • • • • • • GeL Steering Committee approved HM Programme 2016 Proposal developed by HM GeCIP Funding limited to 6,000 samples (3000 patients) Low priority for single gene disorders eg MPD, CML Low priority for lymphoma because practical issues of collecting solid tissue Initial proposal consultation and then modified Stage 1 HM CLL, AML, Myeloma Enrolment alongside FLAIR, AML 18/19 and MUK9/10 1. CLL Saliva and peripheral blood sent to GMC laboratory and UK CLL BioBank 2. AML/Myeloma Saliva and marrow sent to trial biobanks. Marrow cell sorted and both sent back to GMC laboratory 100,000 genomes data collected from data submitted for trial Results and clinical reports distributed by local GMCs Stage 2 HM- Inclusion 1. Newly diagnosed aggressive B and T-cell NHL DLBCL, Burkitt, Mediastinal B cell, high grade lymphoma NOS 1. New AML/MDS outside trial 2. New myeloma outside trial 3. Unclassified HM (eg MDS/MPD overlap, mismatch between clinical and pathological diagnoses) 4. CML extreme responders (compete molecular remission or no morphological response after 3 months TKI treatment 5. Children with ALL with MRD>5% at day 28 Current position Stage 1 disorders Agreements with Cardiff CTRU and ICR October 210 Adapt Informatics pathways October 31st Recruitment start CLL- Nov 15th AML- Jan 31st Myeloma- not specified Stage 2 disorders From November 15th as determined by GMC Feedback? 1. Where are patients enrolling to FLAIR. AML18/19 and MUK9/10 ? 2. How many ? 3. Can trails infrastructure be augmented for additional workload 4. Who are clinical leads for stage 1 and stage 2 disorders? http://www.wegmc.org/ 38