Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
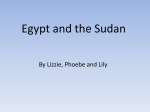
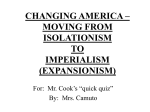
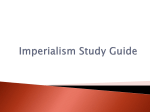
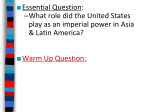
Skull Base Forgotten Foramina: A CT Pictorial Review Poster No.: C-1224 Congress: ECR 2015 Type: Educational Exhibit Authors: N. Trifa, K. Fakhfakh; Sfax/TN Keywords: Trauma, Cancer, eLearning, Computer Applications-3D, CT-High Resolution, Head and neck, Computer applications, Anatomy DOI: 10.1594/ecr2015/C-1224 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 20 Learning objectives Numerous canals and foramina of the skull base are unknown and not familiar to general radiologists Our objectives is to review the anatomy of the "forgotten" foramina of the skull base and their contents, demonstrate the visibility of these foramina in high resolution CT images, study their location and spatial relationships and provide examples of pathological process affecting these structures. Background For the study of these structures we have high resolution images from a 16 channel multidetector CT scanner in axial, sagittal and coronal planes. 0,6 millimeters slices of routine CT head scans, and an advantage workstation GE 4.4 for post-processing are used to study normal CT anatomy of these foramina. We view the slices using a high resolution reconstruction algorithm and bone windowing. We study ten structures: anterior and posterior ethmoidal canals, foramen venosum, craniopharyngeal canal, canalis basilaris medianus, petromastoidal canal, posterior condylar canal, palatovaginal canal and inferior tympanic and mastoid canaliculi. We also review the anatomy of these foramina, their neurovascular contents, and their spatial relationships between the head and intracranial contents. Findings and procedure details • Anterior and posterior ethmoidal canals: The anterior and the posterior ethmoidal canals (AEC and PEC) ( Fig. 1 on page 6 and Fig. 2 on page 7 ) are lateral to either olfactory groove. The AEC transmits the anterior ethmoidal artery, vein and nerve. The PEC transmits the posterior artery, vein and nerve. [1, 2, 3, 4] The anterior ethmoidal artery (AEA) crosses three cavities: the orbit, the ethmoid labyrinth and the anterior fossa of the skull (Fig. 1 on page 6) . This artery irrigates the anterior ethmoidal cells and the frontal sinus; it gives rise to the anterior meningeal artery, and also irrigates the anterior thirds of the nasal septum and the lateral wall of the nose. In its course through the ethmoid labyrinth, the position of the AEA relative to the ethmoidal roof Page 2 of 20 is very variable; the artery thus becomes vulnerable to injury during surgical procedures. [1, 2, 3] CT landmarks used for identifying the anterior ethmoidal artery are: The bony notch on the medial wall of the orbit, which corresponds to the anterior ethmoidal foramen and the bone sulcus on the lateral wall of the olfactory fossa, which corresponds to the anterior ethmoidal sulcus. Anterior ethmoidal canal is seen, showing its course fully or partially. [1] • Foramen venosum: Foramen venosum or foramen of Vesalius is an inconstant foramen seen bilaterally in 48 % and unilaterally in 30% of the population. It is located anteromedially to the foramen ovale and lateral to the foramen rotundum and pterygoid canal. [5] This canal is best seen on axial slices ( Fig. 3 on page 8 ) and connects the middle cranial fossa to the scaphoid fossa. It transmits an emissary vein from the cavernous sinus to the pterygoid plexus ( Fig. 4 on page 9 ), and, on occasion, the accessory meningeal branch of the internal maxillary artery. This vein exits the skull base through the foramen ovale if the foramen Vesalius is absent. [6] When present, the foramina are frequently symmetric. Asymmetry is more likely the result of a pathologic process. Unilateral enlargement of the Vesalius is seen in carotid cavernous fistulas or tumorous invasion from the nasopharynx. [7] • Craniopharyngeal canal: This persistent bony canal can occasionally be detected in the sphenoid bone extending from the sella turcica to the pharynx (Fig. 5 on page 10 ). It is best referred to as an intrasphenoidal canal. The incidence of the craniopharyngeal canal has been calculated as 0.42% from a retrospective analysis of 8338 adult skulls. [8] The term #craniopharyngeal canal or #persistent hypophyseal canal is generally used to describe a small and vertical midline defect in the skull base that measures less than 1.5 mm in diameter. The term craniopharyngeal canal is also used to describe a rarer and much larger bony canal in the same location. Currarino et al [9] provided other names to describe this skull base defect, including the large craniopharyngeal canal and transsphenoidal canal, which differ from the craniopharyngeal canal or persistent hypophyseal canal by virtue of having a greater size and association with special craniofacial anomalies. It has also been suggested that the large craniopharyngeal canals are related not to the persistent craniopharyngeal canal but rather to transsphenoidal meningoencephalocele. [6, 9] The etiology of the craniopharyngeal canal is unknown. There are two main theories regarding to the origin of the canal. One theory proposes that this canal is the remnant Page 3 of 20 of the Rathke pouch. The other theory states that the canal represents the remnant of a vascular channel formed during osteogenesis. [10, 11] • Canalis basilaris medianus: The Canalis basilaris medianus (CBM) is an uncommon anatomic variant or mild anomaly of the basiocciput. It consists of a well defined channel usually more than 2mm in diameter, originating on the intra cranial surface of the basiocciput, in the midline and very close to the anterior rim of the foramen magnum ( Fig. 6 on page 10 ). [12] The occurrence of CBM has been estimated 102 between 2-3% in adults and 4-5% in children. [6, 12] The CBM is generally considered as vestige of notochordal canal without clinical significance. [6, 11, 12] • Canaliculus innominatus: Also known as petrosal foramen or Canal of Arnold, the canaliculus innominatus is a very small canal situated in the greater wing of the sphenoid between the foramen ovale and foramen spinosum and transmits the lesser petrosal nerve. [13] Ginsberg suggested a prevalence of 16%. [5] When the Canaliculus innominatus is absent the lesser petrosal nerve is transmitted through the foramen ovale. [5, 6] • Petromastoidal canal: The petromastoidal canal arises from the subarcuate fossa, which is located at the posterior rim of the temporal bone, courses between the two limbs of the superior semicircular canal, and opens into the periantral mastoidal cells ( Fig. 7 on page 11 ). [11, 14] The canal is lined by dura mater and contains the subarcuate artery and vein. The subarcuate artery mostly originates directly from the anterior inferior cerebellar artery or less frequently from the basilar artery or from the internal auditory artery. [14, 15] In surgical interventions, elevation of the dura along the posterior fossa surface of the temporal bone can cause a cerebrospinal fluid leak; however, the orifice of the canal can serve as an anatomical landmark during surgery. Assessment of the position of the subarcuate canal in relation to the other landmarks prior to surgery can be helpful for orientation during the intervention as well as in order to prevent inadvertent injury of the subarcuate artery. Page 4 of 20 Furthermore, the petromastoidal canal gains clinical importance as a pathway for transmission of infections spreading from the mastoidal cells to the dura and the intracranial cavity. For interpretation of CT images of the temporal bone in traumatized patients knowledge of the course of the subarcuate canal is important, as this structure could be mistaken as a fracture line. [14] • Posterior condylar canal: The Posterior condylar canal forms a communication between the jugular foramen and the condylar fossa just posterior to the occipital condyles. It transmits an emissary vein which allows anastomosis of the jugular bulb or sigmoid sinus to the suboccipital venous plexus.[16] The Posterior condylar canal is the largest of the emissary foramina; its appearance is variable and may depend on its position relative to a particular CT cut ( Fig. 8 on page 17 ). [16] • Palatovaginal canal: This canal found inferomedial to the pterygoid canal ( Fig. 9 on page 12 ) and extends from the pterygopalatine fossa to the roof of the pharynx ( Fig. 10 on page 13 ). It is narrower than the pterygoid canal and foramen rotundum, and hence is the most likely to be confused with a fracture on axial images. It transmits the pterygovaginal artery which is a branch of the maxillary artery, and the pharyngeal nerve, which passes from the pterygopalatine ganglion to the pharyngeal orifice of the Eustachian tube. [11] Identification of this anatomic structure may play a 147 role in detecting canal enlargement due to spread of malignant nasopharyngeal tumors or canal fracture in case of intractable post traumatic epistaxis with injury of ptérygo vaginal artery. [17, 18] • Inferior tympanic and mastoid canaliculi: The mastoid canaliculus and the inferior tympanic canaliculus are seen respectively in 28% and 6% of CT scans of the temporal bone. [19] The inferior tympanic canaliculus is a canal that extends from the jugular foramen to the medial wall of the middle ear seen in only 6% of CT scans of the temporal bone.( Fig. 11 on page 14 ) This canal transmits the inferior tympanic branch of the glossopharyngeal nerve (Jacobson's nerve) from the inferior glosso pharyngeal ganglion. [19] Page 5 of 20 The mastoid canaliculus is a canal that extends from the posterolateral aspect of the jugular foramen to the descending portion of the facial nerve canal seen in 28% of CT scans of the temporal bone.( Fig. 12 on page 15 ) It transmits the auricular branch of the vagus nerve (Arnold's nerve) from the superior vagal ganglion. [19] Both canaliculi form important surgical landmarks for the identification of the cranial nerves within the jugular foramen. Their clinical importance also pertains to the presence of glomus formations along the nerves of Arnold and Jacobsen. The earliest signs of jugulotympanic glomus tumors may therefore be destruction of these canals. [11] In addition, the inferior tympanic canaliculus is enlarged in the setting of an aberrant internal carotid artery, since this represents an enlarged inferior tympanic artery which anastamoses with the caroticotympanic artery after embryonic regression of the cervical internal carotid artery ( Fig. 13 on page 16 ). [11] Images for this section: Page 6 of 20 Fig. 1: Axial slice shows the left anterior ethmoidal canal. Page 7 of 20 Fig. 2: Axial slice shows the left posterior ethmoidal canal. Page 8 of 20 Fig. 3: Axial slice shows the foramen venosum (arrow) between foramen ovale (FO) and pterygoid canal (arrowhead). Page 9 of 20 Fig. 4: Coronal CT reconstruction shows emissary vein passing through the foramen of Vesalius. Fig. 5: Sagittal CT reconstruction shows craniopharyngeal canal (arrows). Page 10 of 20 Fig. 6: Sagittal CT reconstruction shows canalis basilaris medianus. Page 11 of 20 Fig. 7: Axial slice of temporal bone shows the petromastoidal canal. Page 12 of 20 Fig. 9: Axial slice shows palatovaginal canal (black arrowhead) and pterygoid canal (white arrow). Page 13 of 20 Fig. 10: Para sagittal CT reconstruction shows Palato vaginal canal extending from the pterygopalatine fossa to the roof of the pharynx Page 14 of 20 Fig. 11: Coronal CT reconstruction of petrosal bone shows the inferior tympanic canaliculus Page 15 of 20 Fig. 12: Coronal CT reconstruction of petrosal bone shows mastoid canaliculus (arrowhead) crossing between facial canal (arrow) and jugular fossa (JF). Page 16 of 20 Fig. 13: Coronal reconstruction shows aberrant internal carotid artery with enlarged inferior tympanic arteries (arrows) Page 17 of 20 Fig. 8: Axial slice shows posterior condylar canals. Page 18 of 20 Conclusion Conclusion: Knowledge of rare and unfamiliar foramina of the skull base is important in head and neck radiology to recognize the pathologic process affecting these structures and to differentiate canals and fractures. Personal information References References 1. Souza SA, Souza MM, Gregório LC, Ajzen S. Anterior ethmoidal artery evaluation on coronal CT scans. Braz J Otorhinolaryngol. 2009 Jan-Feb; 75(1):101-6. 2. Riehm S, Pénisson L, Charpiot A, Schultz P, Veillon F, Debry C. CT imaging of the anterior ethmoidal artery: anatomic correlation. J Radiol. 2008 Feb;89(2):229-33. 3. Pandolfo I, Vinci S, Salamone I, Granata F, Mazziotti S. Evaluation of the anterior ethmoidal artery by 3D dual volume rotational digital subtraction angiography and native multidetector CT with multiplanar reformations. Initial findings. Eur Radiol. 2007 Jun; 17(6):1584-90. 4. Cankal F, Apaydin N, Acar HI et al. Evaluation of the anterior and posterior ethmoidal canal by computed tomography. Clin Radiol. 2004 Nov; 59(11):1034-40. 5. Ginsberg LE, Pruett SW, Chen YM, Elster AD. Skull base foramina of the middle cranial fossa : reassessment of normal variation with high-resolution CT. AJNR 1994; 15 : 283-291 6. Kuta AJ, Laine FJ. Imaging the sphenoid bone and basiocciput: anatomic considerations. Semin Ultrasound CT MRI 1993; 14: 146-159. 7. Lanzieri CF, Duchesneau 188 PM, Rosenbloom SA, Smith AS and Rosenbaum AE. The significance of asymmetry of the foramen of Vesalius. AJNR Am. J. Neuroradiol, Nov 1988; 9: 1201 - 1204. 8. Arey LB. The craniopharyngeal canal reviewed and reinterpreted. Anatomical Record 1950;106:1-14. Page 19 of 20 9. Currarino G, Maravilla KR, Salyer KE. Transsphenoidal canal (large cranio pharyngeal canal) and its pathologic implications. AJNR Am J Neuroradiol 1985; Vol6: 39-43. 10. Ekinci G , Kilic T, Baltacioglu F et al . Transsphenoidal (large craniopharyngeal) canal associated with a normally functioning pituitary gland and nasopharyngeal extension, hyperprolactinemia, and hypothalamic hamartoma. AJR 2003, vol. 180, no1, pp. 76-77. 11. Connor SEJ, Tan G, Fernando R, Chaudhury N. Computed tomography pseudo fractures of the mid face and skull base. Clinical Radiology (2005); 60: 1268-1279. 12. Currarino G. Canalis basilaris medianus and related defects of the basiocciput. AJNR Am J Neuroradiol 1988;vol 9: 208-211. 13. Kakizawa Y, Abe H, Fukushima Y, Hongo K, El-Khouly H, Rhoton AL Jr. The course of the lesser petrosal nerve on the middle cranial fossa. Neurosurgery. 2007 Sep;61(3 Suppl):15-23; discussion 23. 14. Krombach GA, Schmitz-Rode T, Preschar A, Di Martino E, Weidner J, Gunther RW. The petromastoid canal on computed tomography. Eur Radiol 2002; 12: 2770-2775. 15. Tekdemir I, Asian A, and Elhan 209 A. The subarcuate canaliculus and its artery a radioanatomical study. Ann Anat (1999); 181:207-211. 16. Ginsberg LE. The posterior condylar canal. AJNR Am J Neuroradiol 1994; 15:969-72. 17. Rumboldt Z, Castillo M, Smith JK. The palatovaginal canal: Can it be identified on routine CT and MR imaging? AJR Am J Roentgenol 2002; 179:267-72. 18. Borden NM, Dungan D, Dean BL, Flom RA. Posttraumatic epistaxis from injury to the ptérygo vaginal artery. AJNR 1996;17: 1148-1150. 19. Koesling S, Kunkel P, Schul T. Vascular anomalies,sutures and small canals of the temporal bone on axial CT. European Journal of Radiology 54 (2005):335-343. Page 20 of 20