Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
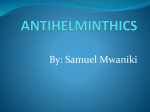
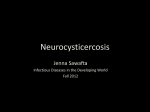
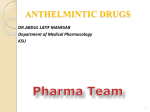
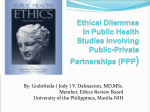
Repurposing Albendazole: new potential as a chemotherapeutic agent with preferential activity against HPV-negative head and neck squamous cell cancer Farhad Ghasemi, Morgan Black, Nicole Pinto, Kara M Ruicci, John Yoo, Kevin Fung, Danielle MacNeil, Joe S Mymryk, John W Barrett, Anthony C Nichols Schulich School of Medicine & Dentistry, Western University, London, ON, Canada Abstract Background: Albendazole is an anti-helminthic drug that has been shown to exhibit anti-cancer properties, however its activity in head and neck squamous cell cancer (HNSCC) was unknown. Methods: Using a series of in vitro assays, we assessed the ability of albendazole to inhibit proliferation in 20 HNSCC cell lines. The HNSCC cell lines were tested for their susceptibility to a range of albendazole doses (1nM-10μM). Cell lines that responded to treatment were further examined for cell death, inhibition of migration, cell cycle arrest and microtubulin distribution. Results: Thirteen of fourteen human papillomavirus-negative HNSCC cell lines responded to albendazole, with an average IC50 of 152 nM. In contrast, only 3 of 6 human papillomaviruspositive HNSCC cell lines responded. Albendazole treatment resulted in apoptosis, inhibition of cell migration and cell cycle arrest in the G2/M phase. Figure 2 – Albendazole caused cell death and apoptosis. A) Live/dead assays were performed with Cal33, HSC2, SCC47, 93VU-147T and WI38 cell samples that were exposed to vehicle (DMSO-only) or 0.5 μM of albendazole (ABZ) for 24 hours (four replicates per treatment). “(S)” marks cells lines susceptible, and “(R)” marks cell lines not susceptible to albendazole in cell proliferation assays. B) Cal33 cells were exposed to vehicle (DMSO-only), 0.5 μM and 1 μM ABZ, and immunoblotted for PARP. Staurosporine (St.) treatment was used as a positive control for apoptosis. Presence of cleaved PARP (c-PARP) at 1 μM albendazole treatment suggests the involvement of apoptosis pathways in cell death. Figure 4 – Albendazole induced cell cycle arrest at G2/M phase. Cal33 (HPV-negative), SCC47 (HPV-positive) and WI38 (normal) cells were exposed to vehicle (DMSO-only) and 0.5 μM albendazole (ABZ) for 24 hours (3 replicates per treatment). BrdU and PI staining were carried out prior to flow cytometry analysis. The average increase in the percentage of G2/M phase cells in the normal WI38 cell line following albendazole treatment was significantly less than the G2/M phase increase in the Cal33 (unpaired t-test, p<0.0001) and SCC47 (unpaired t-test, p<0.0001) cell lines. “(S)” marks cells lines susceptible, and “(R)” marks cell lines not susceptible to albendazole in the cell proliferation assays. * p<0.05, ** p<0.01, *** p<0.001, and NS = not significant. Conclusion: This study indicates that albendazole acts to inhibit the proliferation of human papillomavirus-negative HNSCC cell lines and warrants further study as a potential chemotherapeutic agent for patients suffering from head and neck cancer Introduction • Head and neck cancer is the 6th most common cancer diagnosis worldwide1. • A subset of head and neck squamous cell carcinoma (HNSCC) is associated with the human papillomavirus (HPV). Patients with HPV-positive disease experience better outcomes2. • Poor response of HPV-negative HNSCC patients necessitates the development of new therapeutics3. • Albendazole is a benzimidazole carabamate with a long history of safe and routine use to treat parasitic infections4. • Albendazole works by binding to tubulin, and disrupting microtubule polymerization5. • Accumulating evidence suggests that albendazole may have growth inhibitory capacity against cancer cells6-9. • We have investigated the potential activity of albendazole in HNSCC. Figure 3 - Albendazole impaired cell migration. Scratch assays were performed with 4 HPV-positive and 4 HPV-negative cell lines, exposed to various concentrations of albendazole, and imaged at 0, 2, 5, 8 and 12 hours post-treatment. Albendazole significantly reduced the rate of cell migration in cell lines that were susceptible in IC50 analysis, and led to no significant changes in migration rate in the non-susceptible cell lines (ANCOVA analysis, ns=not significant, ** p<0.01, *** p<0.001). Results Figure 5 – Immunofluorescence shows changes to α-tubulin distribution of Cal33 cells after exposure to various concentrations of albendazole for 24 hours. Experimental treatments included vehicle (DMSO), 0.1 μM, 0.5 μM and 1 μM albendazole for 24 hours. α-tubulin was visualized using IF (green) and nuclei were stained with DAPI (blue). 40x fluorescence microscopy was used to assess changes in cellular morphology and tubulin assembly. A dosedependent disruption in the distribution of α-tubulin was observed. Discussion and Conclusion Figure 1. Albendazole inhibits the cell growth of HNSCC cell lines, with preferential activity in HPV-negative cell lines. A) HPV-negative, HPV-positive and normal cell lines were tested against increasing doses of albendazole in order to calculate IC50 values. Cell lines that did not reach 50% viability at the maximum dose (10 µM) are denoted as NS (not susceptible). B) Mean potency of albendazole for HPV-negative, HPV-positive and normal cell lines. This potency trend suggests that albendazole demonstrates preferential activity in HPVnegative cell lines (unpaired t-test; p<0.05). * p<0.05 and *** p<0.001. • Repurposing available drugs, with established safety profiles, is an attractive alternative to highly costly targeted cancer therapies10,11. • Albendazole had a potent anti-proliferative effect in our panel of HNSCC, with preferential activity against HPV-negative cell lines. • Growth inhibition was associated with cell death in the sensitive lines, likely involving apoptosis based on observed PARP cleavage. • Flow cytometry analysis demonstrated that albendazole treatment arrested HNSCC cells in the G2/M phase, potentially due to the drugs ability to inhibit tubulin polymerization. Cells are most sensitive to radiation during the G2/M phase of the cell cycle, hence, albendazole may have potential as a radiosensitizer in HNSCC treatment6,12. • The low bioavailability of the orally administered drug may serve as a potential limiting factor for its use13. Investigations with intravenous delivery, nanoparticle assemblies and solid-dispersion techniques offer potential solutions to increase plasma concentration of administered albendazole14-16. Grant Support: This study was partially funded by a Canadian Institute Health Research grants MOP 142491 to JSM and ACN, and MOP 340674 to ACN. Conflicts of Interest: Authors declare no conflict of interest. References 1. Jemal et al. 2011 Ca Cancer J Clin 61:69. 2. Fakhry et al. 2008 J Natl Cancer Inst. 100:261. 3. Nichols et al. 2013 Curr Oncol 20:212. 4. Horton 2000 Parasitology 121:S113. 5. Lacey 1990 Parasitol Today 6:112. 6. Patel et al. 2011 Radiat Oncol 6:160 7. Pourgholami et al. 2001 Cancer Lett 165:43 8. Pourgholami et al. 2005 Cancer Chemother Pharmacol 55:425 9. Pourgholami et al. 2006 Clin Cancer Res 12:1928 10. Light et al. 2013 Cancer 119:3900 11.Gupta et al. 2013 Trends Pharmacol Sci 34:508 12. Pawlik and Keyomarsi 2004 Radiat Oncol 59:928 13. Galtier et al. 1991 J Pharm Sci 30:705 14. Liu et al. 2013 Biomed Mater Res 101B:998 15. Kohri et al. 1999 J Pharm Pharmacol 51:159 16. Panwar et al. 2010 Int J Nanomedicine 5:101