Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
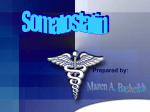
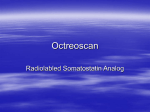
Cardiovascular Drug Reviews Vol. 17, No. 4, pp. 358–373 © 1999 Neva Press, Branford, Connecticut Cardiovascular Effects of Octreotide, a Long-Acting Somatostatin Analog Hironosuke Sakamoto The Second Department of Internal Medicine, Gunma University School of Medicine, Maebashi, Gunma, Japan Key Words: Cardiovascular disease—Octreotide—SMS 201-995—Somatostatin analog. INTRODUCTION Somatostatin, first isolated from ovine hypothalami by Guillemin’s group at the Salk Institute in 1973 (4), is a tetradecapeptide that inhibits growth hormone (GH) release from the pituitary gland (Fig. 1). Large amounts of somatostatin are found in many human tissues, including the D cells of the stomach, intestine, and pancreatic islets; the central nervous system; and the neurons and fibers of both the submucosal and the myenteric plexuses (23,44). In addition to the GH-inhibiting effect, somatostatin suppresses the release of insulin-like growth factor-1 (IGF-1), serotonin, vasoactive intestinal polypeptide, gastrin, insulin, glucagon, secretin, motilin, and pancreatic polypeptides (Table 1). Somatostatin also exerts an extraordinary range of physiological effects on the gastrointestinal tract, such as modifying intestinal transit time, regulating intestinal water and electrolyte transport, reducing splanchnic blood flow, and inhibiting pancreatic exocrine function. These effects suggest that somatostatin might have a broad therapeutic potential, but its clinical application has been limited by its extremely short plasma half-life of 1 to 3 min (54). Octreotide is a synthetic cyclic octapeptide that is homologous with the natural hormone somatostatin at the 4 amino acid sequence (phenylalanine [Phe]–tryptophan [Trp]– lysine [Lys]–threonine [Thr]) within the ring structure that confers biological activity (Fig. 1) (3). Degradation has been slowed by the substitution of L-amino acids with the Dstereoisomers at the first (D-Phe1) and fourth (D-Trp4) positions. The resulting half-life has been reported to be 80 times that of somatostatin (29). Because of its prolonged half-life, octreotide is free from rebound hypersecretion of hormones after it is discontinued (30). Octreotide is now widely accepted as a therapeutic agent for reducing the blood GH and IGF-1 levels in acromegalic patients and as a control for the symptoms of patients with neuroendocrine tumors of the gut. Address correspondence and reprint requests to Dr. Hironosuke Sakamoto, Cardiovascular Division, Brigham and Women’s Hospital, Thorn Building, Rm. 1327, 75 Francis Street, Boston, MA 02115. Fax: (617)-582-6069; e-mail: [email protected]. 358 OCTREOTIDE 359 FIG. 1. Amino acid sequences of human somatostatin and its synthetic analog octreotide. In the field of cardiovascular medicine, the effectiveness of octreotide in the treatment of acromegalic heart disease has been reported. Octreotide has also been tried in the treatment of idiopathic hypertrophic obstructive cardiomyopathy, restenosis after coronary angioplasty, and postprandial orthostatic hypotension. This review focuses on the therapeutic effects of octreotide in cardiovascular diseases. CHEMISTRY A long-acting analog of somatostatin, (−)-D-phenylalanyl-L-cysteinyl-L-phenylalanylD -tryptophyl- L -lysyl- L -threonyl-N-[(1R,2R)-2-hydroxy-1-(hydroxymethyl)propyl]- L - cysteinamide cyclic (2→7) disulfide diacetate (SMS 201-995: octreotide acetate), was synthesized by Sandoz Pharma, Ltd. (Basel, Switzerland) (3). It is a white to light-yellow powder with the molecular formula C49H66N10O10S2-2CH3COOH and molecular weight of 1139.36 Da. The drug is soluble in water, methanol, glacial acetic acid, ethanol, and butanol, but not in acetone or ether. PHARMACOKINETICS Pharmacokinetic study in humans has demonstrated that after s.c. administration octreotide is rapidly and completely absorbed (29). Following s.c. administration of 50, 100, 200, and 400 g of octreotide to eight healthy volunteers, the mean peak plasma concentrations increased linearly with increasing doses, and the values were 2.4 ± 0.8 (S.D.), 4.4 ± 1.5, 10.6 ± 3.3, and 23.5 ± 7.0 ng/mL, respectively. The time to the peak plasma concentrations was independent of the administered doses and ranged from 26 to 35 min. The calculated area under the plasma concentration-time curve increased in a dosedependent manner, and the values were 320 ± 89 (S.D.), 645 ± 201, 1734 ± 583, and Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 360 H. SAKAMOTO TABLE 1. Principal actions of the natural hormone, somatostatin Organ Function Pituitary Pancreas Growth hormone (GH): inhibition of basal and stimulated GH secretion Thyroid-stimulating hormone (TSH): inhibition of basal and stimulated TSH secretion Endocrine Exocrine Gastrointestinal tract Action Gut hormone secretion Exocrine secretion Motor activity Absorption Blood flow to gut Trophic function Insulin: inhibition of basal and stimulated secretion Glucagon: inhibition of basal and stimulated secretion Pancreatic polypeptide: inhibition of secretion Inhibition of bicarbonate and enzyme secretion Inhibition of secretion of gastrin, secretin, cholecystokinin, vasoactive intestinal peptide, gastric inhibitory polypeptide, motillin, enteroglucagon, and neurotensin Inhibition of secretion of gastric acid, pepsin and intrinsic factor, colonic fluid, and bile Inhibition of gastric emptying, gallbladder contraction, and small intestinal segmentation Decreases in absorption rate of Ca2+, glucose, galactose, glycerol, fructose, xylose, lactose, amino acids, triglycerides,and water Decreases in mesenteric blood flow and increases in vascular resistance Inhibition of mucosal cell proliferation Thyroid Inhibition of release of thyroxine (T4) and triiodothyronine (T3), inhibition of calcitonin secretion Adrenal Inhibition of angiotensin II-stimulated aldosterone secretion, inhibition of acetylcholine-stimulated medullary catecholamine secretion Kidneys Inhibition of renin release, inhibition of vasopression-mediated water absorption 3163 ± 1354 ng/mL/min, respectively. Hepatic metabolism of octreotide was extensive, with up to 30% or 40% of hepatic extraction. The total body clearance of octreotide was slow, being approximately 190 mL/min (11.4 L/h). The elimination half-life was independent of the administered dose and ranged from 72 to 113 min. The distribution, excretion, and metabolism of octreotide have been studied in the rat after i.v. bolus administration (31). In rat blood, 96% of octreotide was present in plasma, 59% and 75% being bound to plasma proteins in vitro and in vivo, respectively. No octreotide was taken up by rat blood cells. The urinary and fecal excretion of unchanged drug averaged 19% and 1% of an administered dose, respectively. PHARMACOLOGY Effects on Anterior Pituitary Gland Function In rats and rhesus monkeys, octreotide is longer acting and more selective in inhibiting the secretion of GH than is glucagon or insulin. In rats, by i.m. administration, octreotide was 70 times more potent than the natural hormone somatostatin in inhibiting basal GH secretion, 23 times more potent in inhibiting insulin-stimulated glucagon secretion, and only 3 times more potent in inhibiting glucagon-stimulated insulin secretion (3). In rhesus monkeys, by i.v. infusion, octreotide inhibited basal GH secretion and was 45 times more Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 361 potent than somatostatin. As an inhibitor of basal glucagon secretion, octreotide was 11 times and of basal insulin secretion 1.3 times more potent than somatostatin. It is not known why this somatostatin analog, octreotide, preferentially inhibits GH secretion versus insulin secretion. However, the fact that several subtypes of somatostatin receptors have been described could account, at least in part, for this phenomenon (43,45). In addition, the insulin-saving effect could be of value in the therapy of diabetes, quite apart from the advantages one hopes to gain from normalization of GH levels in diabetic patients. In healthy volunteers, s.c. administration of 50 g of octreotide inhibited arginineinduced GH secretion for 4 to 5 h (11). The GH increment, expressed as the calculated area under the plasma concentration-time curve, was markedly suppressed by octreotide injected just before (1488 ± 607 (S.E.) vs. 203 ± 82 ng/mL ⭈ min, P < 0.001) and 3 h before arginine (1449 ± 591 vs. 236 ± 96 ng/mL ⭈ min, P < 0.02). Administration of 100 g of octreotide s.c. practically abolished the sleep-induced GH surge for 6 h (1132 ± 180 vs. 260 ± 40 ng/mL ⭈ min, P < 0.01), and there was no rebound hypersecretion. By s.c. administration, 50 or 100 g of octreotide inhibited the stimulating effect of thyrotropinreleasing hormone on thyroid-stimulating hormone secretion for at least 3 h (21.8 ± 3.1 for control vs. 11.8 ± 2.2 IU/mL ⭈ min after 50 g, P < 0.001, and 12.3 ± 2.5 IU/mL ⭈ min after 100 g of octreotide, P < 0.001) without modifying basal levels at either dose. Effects on Gastrointestinal and Pancreatic Endocrine System Like the natural hormone somatostatin, octreotide exerts a potent inhibitory effect on the release of peptides of the gastroenteropancreatic endocrine system and has many actions on digestive function. In healthy volunteers, s.c. administration of 50 g of octreotide significantly inhibited both basal and meal-stimulated secretion of insulin, glucagon, pancreatic polypeptide, gastric inhibitory peptide, secretin, gastrin, neurotensin, and motilin (16). Compared with placebo, s.c. administration of 25 g of octreotide twice daily for 7 d prolonged mouth-to-cecum transit time (68 ± 7 (S.E.) vs. 199 ± 11 min, P < 0.01) and increased fecal fat excretion (7.6 ± 1.4 vs. 19.2 ± 2.8 g/day, P < 0.01) (32). Octreotide significantly (P < 0.01) inhibited cholecystokinin-stimulated secretion of amylase, trypsin, and lipase. Octreotide also almost completely inhibited meal-induced cholecystokinin release and postprandial gallbladder contraction. Administration of 25 or 100 g of octreotide (s.c.) 3 times daily for 7 d markedly suppressed peptone-stimulated gastric acid and volume secretion (36). The mean percentage inhibition of gastric acid output was 95% and 88% on Days 2 and 7 for the two doses, respectively; the effect was not dose dependent. The mean percentage reduction of gastric volume secretion at 25 g of the drug was 70% and 36% on Days 2 and 7, respectively. At 100 g of octreotide, the gastric secretion volume was reduced by 75% and 50% on Days 2 and 7, respectively. The possible mechanisms by which octreotide inhibits pancreatic enzyme secretion and gall bladder contraction are abolishment of cholecystokinin release and interruption of nervous transmission (32). The prolongation of mouth-to-cecum transit time may be due to a direct local effect of octreotide on the myenteric plexus or gastrointestinal smooth muscle. Effects on Cardiovascular System The effects of i.v. bolus and continuous infusion of octreotide on hemodynamics have been well studied in patients with hepatic cirrhosis and portal hypertension (39). By either Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 362 H. SAKAMOTO type of administration, octreotide caused bradycardia and systemic vasoconstriction; these effects were more pronounced after bolus dose administration than after continuous infusion. An i.v. bolus of 25 g of octreotide significantly decreased the pulse rate (from 77 ± 3 (S.E.) to 65 ± 3 beats/min, P < 0.01) and cardiac output (from 9.2 ± 0.8 (S.E.) to 7.9 ± 0.8 L/min, P < 0.01). The bolus doses significantly increased mean arterial pressure (from 81 ± 3 (S.E.) to 87 ± 3 mmHg, P < 0.05), mean pulmonary capillary wedge pressure (from 4.8 ± 0.8 to 11.2 ± 1.4 mmHg, P < 0.01), mean pulmonary arterial pressure (from 9.1 ± 1.0 to 16.6 ± 1.5 mmHg, P < 0.01), mean right ventricular pressure (from 7.1 ± 0.6 to 12.5 ± 1.3 mmHg, P < 0.01), mean right atrial pressure (from 3.8 ± 0.8 to 6.6 ± 1.0 mmHg, P < 0.01), mean systemic vascular resistance (from 778 ± 89 (S.E.) to 942 ± 99 dyne ⭈ sec ⭈ cm−5, P < 0.05), and mean pulmonary vascular resistance (from 49 ± 8 to 74 ± 9 dyne ⭈ sec ⭈ cm−5, P < 0.05). On the other hand, by i.v. infusion at 50 g/h, octreotide significantly reduced the mean pulse rate at 3 min (from 78 ± 3 to 72 ± 5 beats/min, P < 0.05) and at 15 min (69 ± 4 beats/min, P < 0.05). By i.v. infusion, octreotide significantly increased the mean pulmonary capillary wedge pressure at 15 min (from 9.2 ± 1.3 to 13.5 ± 1.4 mmHg, P < 0.05) and at 30 min (12.7 ± 1.1 mmHg, P < 0.05) and the mean pulmonary artery pressure at 15 min (from 14.6 ± 1.4 to 19.1 ± 1.5 mmHg, P < 0.05) and at 30 min (18.2 ± 1.5 mmHg, P < 0.05). By i.v. infusion, octreotide also significantly increased the mean right atrial pressure (from 3.4 ± 0.9 to 5.5 ± 1.1 mmHg, P < 0.01) and the mean right ventricular pressure (from 12.0 ± 1.2 to 14.6 ± 1.0 mmHg, P < 0.05) at 30 min, without changing cardiac output, mean arterial pressure, systemic vascular resistance, or pulmonary vascular resistance. The mechanism of octreotide-induced vasoconstriction remains unclear. However, inhibition of secretion of a vasodilating hormone glucagon, a direct action on the vasculature or the heart, or an autonomic neural mechanism may explain this phenomenon. Furthermore, the elevation of pulmonary arterial pressure by octreotide may be passive, because of increased cardiac afterload. Two observations by Gaudin et al. (17), who investigated the cardiovascular effects of somatostatin in patients with cirrhosis and portal hypertension, support this hypothesis. First, the systemic vasopressor effect preceded the pulmonary vasopressor effect. Peak systemic and pulmonary artery pressure increases occurred 1 min and 3 min, respectively, after bolus somatostatin injections. Second, the elevation in pulmonary capillary and arterial pressure was not associated with increased pulmonary vascular resistance. Effects on Pulmonary Function There is limited information available on the effect of octreotide or natural somatostatin on respiration in humans. One study with healthy volunteers has reported that i.v. somatostatin attenuates the ventilatory response to hypoxia but not to hypercapnia (38). Long-term administration of octreotide was reported to ameliorate the dyspnea on exertion in a case of cirrhotic hypoxemia (28). Another group has observed that somatostatin increases the ventilatory roll-off with sustained hypoxia in humans (14). Octreotide therapy in patients with acromegaly is associated with a reduction in the frequency of apnea (20). This effect was particularly manifest in the subgroup of patients with central apnea, a disturbance of breathing during sleep, that is strongly linked to abnormal central control of respiration (21,22). One possible mechanism for this reduction in apnea severity Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 363 is that octreotide may centrally reduce chemoreceptor gain, which is increased in patients with central apnea. In conscious dogs, i.v. injection of 0.5 mg of octreotide altered the breathing pattern with a 23 ± 6% decrease in the respiratory frequency (P < 0.05) and a 16 ± 6% increase in the tidal volume (P < 0.05), resulting in no net change in ventilation (6). No significant change in the ventilatory response to carbon dioxide was observed after octreotide. The drug appears to influence breathing by either a peripheral or a central mechanism. The anesthesia (in dog experiments) or species differences may explain the observed differences in the effects of octreotide in humans and dogs. Effects on the Renin-Angiotensin System and Renal Function The inhibitory effect of octreotide on the renin-angiotensin system has been demonstrated in healthy volunteers (55) and in cirrhotic patients (50). Sieber et al. (55) studied the short-term effect of octreotide on orthostatic stimulation of plasma renin activity following head-up tilting and on angiotensin II-induced aldosterone release under placebo controlled conditions in healthy volunteers. Head-up tilting produced the characteristic increases in plasma renin activity and plasma aldosterone levels. Administration of 100 g of octreotide s.c. significantly (P < 0.05) inhibited the elevation of plasma renin activity from 30 min onward. In contrast, plasma aldosterone levels were not altered by octreotide. Furthermore, i.v. infusions of 10 g of octreotide per h failed to inhibit the stimulation of plasma aldosterone secretion induced by exogenous angiotensin II (2 to 10 ng/kg/min). These results are inconsistent with data showing an inhibitory action of natural somatostatin upon angiotensin II-stimulated aldosterone release in humans (27). This discrepancy can be explained by the absence of octreotide binding sites in tumoral and normal adrenal cortical tissue derived from patients with aldosteronoma (46,47). The effect of octreotide on renal function is controversial. Mountokalakis et al. (40) observed an improvement in renal function in cirrhotic patients treated with an acute i.v. infusion of octreotide. In a noncontrolled study, Rodriguez-Perez et al. (48) observed a decrease in plasma renin activity and aldosterone levels and an improvement in renal function with a decrease in total exchangeable sodium after chronic s.c. octreotide administration in cirrhotic patients with ascites. In contrast, Malesci et al. (37) observed a persistent inhibition of postprandial glucagon response but no effect on renal plasma flow, glomerular filtration rate, blood urea, or creatinine after long-term treatment with octreotide in cirrhotic patients. Sabat et al. (50) observed a decrease in plasma renin activity, plasma aldosterone, and plasma glucagon without any modification of renal function after 5 d of s.c. octreotide administration in cirrhotic patients with ascites. EFFECTS ON CARDIOVASCULAR DISEASES Acromegalic Heart Disease Acromegaly is associated with an excess morbidity and mortality, mainly due to cardiovascular disease (51). Most acromegalic patients present with cardiac hypertrophy, increased cardiac output, and decreased systemic vascular resistance, all of which are characteristic of the hyperkinetic heart syndrome (Fig. 2). However, some patients develop congestive heart failure with dilated cardiomyopathy. Other abnormalities are arterial hypertension, coronary artery disease, and ventricular arrhythmias. Furthermore, Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 364 H. SAKAMOTO FIG. 2. Hypothetical sequence of morphological and functional events in untreated acromegalic heart disease. GH, growth hormone; IGF-1, insulin-like growth factor 1. From ref. 51 with permission. acromegalic patients who do not have diabetes mellitus, hypertension, or coronary heart disease are assumed to have “acromegalic cardiomyopathy.” Effects on Cardiac Hypertrophy Octreotide has been reported to cause a rapid and sustained decrease in left ventricular mass in acromegalic patients with left ventricular hypertrophy (33,58). Using echocardiography, Lim et al. (33) studied 16 acromegalic patients before and after s.c. administration of octreotide (mean dose, 538 g daily) for 2 mo. The 16 patients with acromegaly were stratified into two groups: Group 1 (n ⳱ 10) with and Group 2 (n ⳱ 6) without left ventricular hypertrophy. Both groups showed a large and significant reduction of plasma GH and IGF-1 levels at 1 w, and these decreases were maintained after 2 mo. Ten patients with left ventricular hypertrophy showed an increase in the left ventricular end-systolic dimension (from 33.5 ± 2.7 to 36.5 ± 3.1 mm, P < 0.01) and a decrease in the thicknesses of interventricular septum (from 11.3 ± 0.3 to 10.0 ± 0.3 mm, P < 0.01) and of left ventricular posterior wall (from 11.0 ± 0.3 to 10.0 ± 0.4 mm, P < 0.05) after 2 mo of treatment. These patients showed a rapid decrease in left ventricular mass within 1 w (reduction, 33.9 ± 11.1 g, P < 0.01), which was sustained at 2 mo (reduction, 53.0 ± 22.3 g, P < 0.04) (Fig. 3, left). These patients also showed a rapid and sustained reduction in left ventricular mass index at 1 w (reduction, 18.5 ± 5.4 g/m2, P < 0.02) and at 2 mo (reduction, 19.5 ± 10.0 g/m2, P < 0.05) (Fig. 3, right). Furthermore, the decrease in left Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 365 FIG. 3. Changes in left ventricular mass and left ventricular mass index with octreotide therapy. During the 2-mo treatment period, left ventricular (LV) mass was reduced in patients with left ventricular hypertrophy (LVH) at both time points, but no change was seen in patients without LVH (left). Left ventricular mass index was reduced in patients with LVH at 1 w and 2 mo of treatment, but no changes were seen in patients without LVH (right). **P < 0.01 compared with baseline. From ref. 33 with permission. ventricular mass significantly correlated with the octreotide-induced decrease in GH (r ⳱ 0.79, P < 0.05) but not with blood pressure. In contrast, the remaining six patients without left ventricular hypertrophy showed no significant changes in cardiac dimensions, left ventricular mass, or left ventricular mass index (Fig. 3). Blood pressure, left ventricular dimensions, and the percentage of fractional shortening were not altered by therapy in either group. During treatment, the body weight for all 16 patients was 93 ± 6 kg at baseline and then declined to 91 ± 6 kg at 1 w and 89 ± 7 kg at 2 mo. There was no statistical difference between groups in body weight for any time point or in the decrease in body weight. Tokgözoğlu et al. (58) observed a major regression in left ventricular hypertrophy in acromegalic patients after 3 mo of octreotide therapy. Octreotide (300 to 600 g s.c. daily) was administered to six patients for 6 mo. Blood GH levels decreased significantly in all patients, from 15.8 ± 9 to 5 ± 2 ng/mL at 3 mo (P < 0.01), and they further decreased to 4 ± 4 ng/mL in 6 mo. The left ventricular mass decreased significantly in all patients, from 304 ± 80 to 177 ± 43 g at 3 mo (P < 0.01). It decreased further to 175 ± 47 g in 6 mo. Blood pressure and body mass index did not change during treatment. GH exerts its effects on peripheral tissues via direct and indirect mechanisms (51). Most of the indirect effects are mediated by IGF-1. GH acts by stimulating the local production of IGF-1, which in turn promotes tissue growth by paracrine or autocrine mechanisms. IGF-1 may also act via the systemic circulation as an endocrine growth factor. The GH receptor gene is expressed in the myocardium, and GH increases mRNA and the protein expression of IGF-1 in rats. Cardiac myocytes of rats express IGF-1 receptors, and IGF-1 increases cell size and induces muscle-specific gene expression (26). In patients with acromegaly, a longstanding excess of GH and IGF-1 causes interstitial edema of the heart and increases the cell size of cardiac myocytes. The reduction of hypersecretion of GH and IGF-1 after octreotide treatment decreases interstitial edema and the cell size of myocytes in these patients. Another possibility is that octreotide may cause regression of cardiac Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 366 H. SAKAMOTO hypertrophy by inhibiting the renin-angiotensin system. Previous studies have demonstrated a significant decrease in plasma renin activity after octreotide administration to healthy volunteers (55) or to cirrhotic patients with ascites (50). Effects on Heart Failure Although one rare case of worsening heart failure under octreotide therapy has been described (1), octreotide usually improves congestive heart failure in acromegalic patients (7). Chanson et al. (7) found rapid and sustained clinical improvement in acromegalic patients with refractory congestive heart failure during long-term octreotide treatment. Octreotide was administered s.c. 3 times daily at doses ranging from 100 to 500 g to seven patients with active acromegaly. Three of these patients had congestive heart failure, and the other four patients were free of symptoms associated with heart failure. During octreotide therapy, all seven patients showed decreases in plasma levels of GH (from 28.1 ± 32.7 to 5.2 ± 8.3 g/L, P < 0.025) and IGF-1 (from 740 ± 126 to 372 ± 64 g/L, P < 0.025). The elevated plasma volume returned to normal, and the heart rate decreased significantly. Right heart catheterization in the three patients with heart failure showed a dramatic clinical improvement that was associated with an increase in stroke volume by 24% to 51% within 2 y. In these patients, the cardiac index remained in the normal range, filling pressures were markedly decreased, and the elevated pulmonary wedge pressure returned to normal. This improvement was sustained for up to 3 y in the two patients with heart failure who received long-term treatment. On the other hand, right-heart catheterization in the four patients without heart failure showed a 19 ± 2.5% reduction in the cardiac index, which was related to both a decrease in heart rate and an 18.3 ± 11% reduction in stroke volume, within 3 mo. The direct and indirect effects of octreotide can account for the improvement of heart failure. Two mechanisms, hypervolemia and a direct myocardial effect of GH and IGF-1 hypersecretion, have been implicated in the pathogenesis of acromegalic cardiomyopathy. If the heart is normal, hypervolemia is responsible for the hyperkinetic heart syndrome. Conversely, the effect of hypervolemia on preexisting cardiomyopathy, whatever its origin, leads to congestive heart failure. Octreotide could improve heart failure through normalization of hypervolemia. Another explanation is that GH and IGF-1 have direct myocardial effects that may be reversible with normalization of GH and IGF-1 secretion by octreotide. Effects on Exercise Capacity Octreotide improves exercise capacity in acromegalic patients (9,33,42). In the study of Padayatty et al. (42), 10 patients with acromegaly were treated with 100 g of octreotide s.c. 3 times daily for 2 mo, followed by 200 g 3 times daily if the blood GH level was higher than 5 mU/L, for a total of 1 y. At 6 and 12 mo, GH and IGF-1 secretions were significantly reduced, but the ejection fraction, measured by echocardiography and multigated image acquisition scan, did not change. The patients improved symptomatically: their resting heart rate was significantly reduced, and their body weight significantly increased. The mean exercise duration on the treadmill significantly increased from 637 ± 137 s at baseline to 702 ± 105 s after 6 mo (P < 0.01) and 787 ± 101 s after 12 mo (P Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 367 < 0.01). Mean work significantly increased from 9.0 ± 3.3 (S.D.) METs at baseline to 10.6 ± 3.5 METs at 6 mo (P < 0.001) and 11.9 ± 2.7 METs at 12 mo (P < 0.001). Colao et al. (9) also reported that prolonged suppression of blood GH and IGF-1 levels by octreotide normalized cardiac performance in acromegalic patients. In 30 patients with active acromegaly, they studied the effects of 1-y treatment with octreotide on left ventricular diastolic and systolic function, assessed during physical exercise by gated blood pool cardiac scintigraphy. Octreotide was initially given at a dose of 50 to 100 g, 3 times daily, and the dose was subsequently increased to achieve normalization of GH and IGF-1 levels. After 1-y treatment with octreotide, a significant decrease in blood GH and IGF-1 levels was achieved in all patients, but normalization was observed in only 13 of 30 patients. In the 13 patients with hormone normalization, a significant decrease in heart rate, both at rest (from 75.7 ± 3.3 to 66.5 ± 2.9 beats/min, P < 0.01) and after exercise (from 137.5 ± 4.9 to 123.7 ± 4.1 beats/min, P < 0.01), and a significant increase in left ventricular ejection fraction, both at rest (from 56.5 ± 1.8 to 66.5 ± 2.2%, P < 0.01) and after exercise (from 52.6 ± 2.4 to 67.1 ± 1.7%, P < 0.01), occurred. These patients showed a significant increase in exercise duration (from 7.5 ± 0.5 to 9.3 ± 0.7 min, P < 0.05) and exercise workload (from 80.8 ± 5.5 (S.E.) to 92.3 ± 5.9 W, P < 0.05). On the other hand, in the 17 patients with high hormone levels, the left ventricular ejection fraction was unchanged at rest but was significantly reduced after exercise compared with the basal value (from 64.9 ± 2.4% to 57.2 ± 2.6%, P < 0.01); the systolic blood pressure at rest was significantly increased (from 128.5 ± 4.9 to 141.2 ± 5.4 mmHg, P < 0.05). Their ejection fraction response to exercise was significantly impaired (from 11.6 ± 3.2% to −0.3 ± 5.6%, P < 0.05). However, neither exercise duration nor exercise workload was increased in these patients. Effects on Circadian Blood Pressure Profile Circadian blood pressure rhythm is maintained in patients with acromegaly, and octreotide increases 24-h and nighttime blood pressure with loss of circadian blood pressure rhythm (13). Octreotide (200 to 600 g/day) was administered s.c. to 10 patients with GH-producing adenoma for 6 mo. On the day prior to and on the last day of octreotide treatment, each patient underwent noninvasive 24-h blood pressure and heart rate monitoring. In these 10 patients, there was no correlation between baseline GH and IGF-1 levels and 24-h systolic and diastolic blood pressure values. Before treatment, all patients showed a significant nocturnal decrease of both systolic and diastolic blood pressures, with a significant circadian rhythm for systolic or diastolic blood pressure. During octreotide treatment, 24-h as well as nighttime systolic and diastolic blood pressures significantly increased, whereas daytime systolic and diastolic blood pressures did not change. Not all patients had a nocturnal decline in systolic and diastolic blood pressures, and 8 of 10 patients lost their circadian rhythm of systolic or diastolic blood pressure. Splanchnic vasoconstriction by octreotide, shifting blood to peripheral vessels, may explain this phenomenon. Hypertrophic Obstructive Cardiomyopathy Hypertrophic obstructive cardiomyopathy, the cause of which is unknown, is a heart disease characterized by obstruction of the left ventricular outflow tract and an increase in Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 368 H. SAKAMOTO interventricular septum thickness. This disease deserves consideration since it appears at an early age and has high morbidity and mortality. Octreotide has some beneficial effects on hypertrophic obstructive cardiomyopathy, and the drug seems to represent a new therapeutic approach to this disease. The effect and safety of octreotide were echocardiographically evaluated in 15 patients with hypertrophic obstructive cardiomyopathy (12). Octreotide (100 g) was administered s.c. 3 times daily for the first month and once daily for the subsequent 5 mo. At the end of therapy, the thickness of the interventricular septum decreased from 22.00 ± 2.32 to 17.26 ± 3.57 mm (P < 0.01), and the subaortic gradient decreased from 41.40 ± 10.71 to 28.06 ± 11.42 mmHg (P < 0.05). The ratio of interventricular septum thickness to left ventricular posterior wall thickness decreased from 1.89 ± 0.25 to 1.53 ± 0.28 (P < 0.01). The ratio of the mitral valve wave E to wave A significantly increased from 1.19 ± 0.37 to 1.38 ± 0.24 (P < 0.01). There were no significant changes in heart rate, systolic and diastolic arterial blood pressures, left ventricular posterior wall thickness, left ventricular end-diastolic diameter, left ventricular end-systolic diameter, ejection fraction, and fractional shortening. No adverse effect was observed during the therapy. The mechanism of the octreotide-induced regression of hypertrophy is still unknown. This is not surprising since the pathogenesis of hypertrophic obstructive cardiomyopathy is not known. However, the mechanism is likely to involve IGF-1, microvascular disease, or increased intracellular calcium. Restenosis after Coronary Angioplasty The major limitation of percutaneous transluminal coronary angioplasty is the high (20% to 50%) restenosis rate within the first 6 mo after a successful procedure (41). It is recognized that restenosis can be caused by excessive neointima formation resulting from smooth muscle cell proliferation and migration from the arterial media into the subendothelial space (2,35). The formation of neointima is stimulated by locally released growth factors derived from activated platelets, macrophages, white blood cells, and the smooth muscle cells themselves. In Vitro Studies Sakamoto et al. (52) demonstrated the inhibitory effects of octreotide on smooth muscle cell outgrowth from in vitro explants of both coronary and carotid arterial tissues in a canine endothelium-injury model. After 6 d of culture, smooth muscle cells grew out by 33.3% and 58.3% of the explants from the injured canine carotid and coronary arterial tissues, respectively, whereas cell outgrowth did not occur from any of the explants from normal canine carotid arterial tissue. At a concentration of 10−6 mol octreotide completely inhibited cell outgrowth from injured canine carotid arterial tissue (Fig. 4, left). This drug also inhibited cell outgrowth from injured canine coronary arterial tissue by 57% and 71% of the control value at concentrations of 10−8 mol and 10−6 mol, respectively (Fig. 4, right). Grant et al. (19) demonstrated the localization of IGF-1 in de novo and restenotic human coronary atherectomy specimens by using immunocytochemical techniques. The synthetic phenotype of smooth muscle cells contained a significantly higher concentration of IGF-1 Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 369 FIG. 4. Effects of octreotide on smooth-muscle cell outgrowth from explants of endothelium-injured canine carotid (left) and coronary (right) arterial tissues. Octreotide effectively inhibited smooth-muscle cell outgrowth from in vitro explants from in vivo injured canine coronary and carotid arteries in a dose-dependent manner. Independent experiments yielded similar results. From ref. 52 with permission. than did the contractile phenotype of smooth muscle cells. They also studied the effects of IGF-1, basic fibroblast growth factor, and platelet-derived growth factor on human coronary artery smooth muscle cell proliferation in vitro. All three growth factors stimulated smooth muscle cell proliferation in a dose-dependent manner. Octreotide (10−8 M) significantly (P < 0.01) blocked IGF-1-stimulated smooth muscle cell proliferation by 15% to 20%. Addition of octreotide to basic fibroblast growth factor-stimulated smooth muscle cells resulted in a 40% to 45% inhibition of cell proliferation (P < 0.01). In contrast, platelet-derived growth factor-stimulated cultures were only minimally affected by octreotide. The in vitro effects of octreotide may reflect a direct inhibition of mitogenic signaling of growth factor receptor kinases, which is independent of the presence of GH. Growth factors such as IGF-1 (61), basic fibroblast growth factor (34), and platelet-derived growth factor (49) have been implicated in the regulation of smooth muscle cell proliferation and migration, because they all induce smooth muscle cell mitosis and chemotaxis in vitro. The receptors of these growth factors share the common feature of a tyrosine kinase domain in the cytoplasmic portion of the molecule (60). Binding of growth factors to their receptors induces autophosphorylation of the -subunit of the receptor and activation of tyrosine kinase (8). Deactivation of these growth factor receptors involves specific protein tyrosine phosphatases (10). Octreotide activates protein tyrosine phosphatases and can inhibit the stimulatory effects of selected growth factors (5,56). In smooth muscle cell proliferation studies by Grant et al. (19), octreotide blocked the stimulating effect of IGF-1 and basic fibroblast growth factor but not of platelet-derived growth factor. The reason for this may be related to differences in the protein tyrosine phosphatases that modulate these three growth factors. Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 370 H. SAKAMOTO Clinical Trials In vitro data suggest the use of octreotide in clinical settings to prevent restenosis after coronary interventions by reducing smooth muscle cell proliferation induced by growth factors. However, the results of a recent randomized, double-blind, placebo-controlled trial assessing the effects of high-dose octreotide on restenosis prevention after coronary angioplasty failed to meet expectations. In the VERAS (Verringerung der Restenoserate nach Angioplastie durch einen Somatostatin Analog) trial, 217 patients received s.c. injections of 500 g of octreotide or placebo every 8 h for 3 w (59). Octreotide did not show any effect on the angiographic restenosis rate at 6 mo or the incidence of clinical events during 6 mo of follow-up (Tables 2 and 3). Several possible explanations may account for the discrepancy between the clinical outcomes of the VERAS trial and the results of in vitro experiments. The dosage of octreotide used in the VERAS trial may still be too low. Local delivery of octreotide via a catheter may be the ideal approach to direct the drug at a high concentration specifically to the target lesion and, thereby, to the activated smooth muscle cells. The pretreatment period before coronary angioplasty may be too short. Species differences in the biological response to vascular injury may explain the different outcomes in the treatment of restenosis. Since arterial remodeling has recently been suggested as the predominant factor in restenosis (53), the growth factor inhibition by octreotide activating protein tyrosine phosphatase may not be sufficient to prevent coronary restenosis. Postprandial Orthostatic Hypotension The effectiveness of octreotide in reducing postprandial and orthostatic hypotension has been demonstrated in patients with autonomic neuropathy (25). Octreotide (0.2 to 0.4 g/kg) injected s.c. at the beginning of breakfast raised the blood pressure after breakfast in all six patients with postprandial hypotension. Compared with the patients with placebo, the mean sitting blood pressure in patients with 0.4 g of octreotide per kg was 35 mmHg higher at 6 min after breakfast. Octreotide (0.1 to 1.6 g/kg) raised upright blood pressure during the postprandial period in five of seven patients. Before therapy, three patients were unable to stand after eating; after injection of octreotide (0.8 g/kg) at the beginning of breakfast, they were able to walk for 35 to 100 min. The duration of the therapeutic effect of each injection was 3 to 6 h. The mechanism by which octreotide helps to prevent postprandial orthostatic hypotension has not been adequately studied. Octreotide has been shown to prevent the increase of splanchnic blood flow induced by a meal and to increase splanchnic vascular resistance in patients with autonomic failure (24). Octreotide also TABLE 2. Restenosis rates according to three definitions Octreotide (n ⳱ 108) (%) Placebo (n ⳱ 109) (%) Two-paired Pa 34.3 34.3 29.6 33.9 33.9 24.8 1.0 1.0 0.45 Final stenosis of ⱖ50% Loss of >50% of initial gain Absolute loss of >0.72 mm of MLDb a b Fisher’s exact test. Abbreviation: MLD, minimal luminal diameter. Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 371 TABLE 3. Incidence of clinical events during the follow-up period of 6 mo a Death Myocardial infarction CABGb Premature repeat intervention a b Octreotide Placebo 1 2 5 17 0 1 7 14 Due to allergic reaction against contrast media. Abbreviation: CABG, coronary artery bypass graft surgery. increased forearm vascular resistance and cardiac output in fasting patients with autonomic failure. The most likely mechanism for the beneficial effect of octreotide on postprandial orthostatic hypotension is an increase in splanchnic and forearm vascular resistance. CONCLUSIONS A long-acting synthetic somatostatin analog, octreotide, has been widely accepted as a therapeutic agent for the treatment of acromegaly and neuroendocrine tumors of the gut. In addition to the improvement of acromegalic heart disease, octreotide is potentially useful in the management of several cardiovascular diseases, such as idiopathic hypertrophic obstructive cardiomyopathy, restenosis after coronary angioplasty, and postprandial orthostatic hypotension. Further clinical trials are needed to prove the benefit of octreotide in cardiovascular medicine. In the recently developed formulation, octreotide is slowly released from microspheres containing poly(lactide-glycolide)glucose (15,18,57). This sustained release formulation of octreotide offers the convenience of once-monthly administration compared with daily s.c. drug administration. The good efficacy and tolerability profile of the new formulation should enhance patient compliance and acceptability of octreotide therapy and contribute to an improvement in the quality of life of patients. REFERENCES 1. Albat B, Leclercq FF, Serre I, et al. Heart transplantation for terminal congestive heart failure in an acromegalic patient. Eur Heart J 1993;14:1572–1575. 2. Austin GE, Ratliff NB, Hollman J, Tabei S, Phillips DF. Intimal proliferation of smooth muscle cells as an explanation for recurrent coronary artery stenosis after percutaneous transluminal coronary angioplasty. J Am Coll Cardiol 1985;6:369–375. 3. Bauer W, Briner U, Doepfner W, et al. SMS 201–995: a very potent and selective octapeptide analogue of somatostatin with prolonged action. Life Sci 1982;31:1133–1140. 4. Brazeau P, Vale W, Burgus R, et al. Hypothalamic polypeptide that inhibits the secretion of immunoreactive pituitary growth hormone. Science 1973;173:77–79. 5. Buscail L, Delesque N, Esteve J-P, et al. Stimulation of tyrosine phosphatase and inhibition of cell proliferation by somatostatin analogues: mediation by human somatostatin receptor subtypes SSTR1 and SSTR2. Proc Natl Acad Sci USA 1994;91:2315–2319. 6. Cao K, Grunstein RR, Ho KY, Sullivan CE. The effect of octreotide on breathing and the ventilatory response to CO2 in conscious dogs. Eur Respir J 1988;11:1376–1381. 7. Chanson P, Timsit J, Masquet C, et al. Cardiovascular effects of the somatostatin analog octreotide in acromegaly. Ann Intern Med 1990;113:921–925. 8. Cohen P. Signal integration at the level of protein kinases, protein phosphatases, and their substrates. Trends Biochem Sci 1992;17:408–413. Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 372 H. SAKAMOTO 9. Colao A, Cuocolo A, Marzullo P, et al. Effects of 1-year treatment with octreotide on cardiac performance in patients with acromegaly. J Clin Endocrinol Metab 1999;84:17–23. 10. Cool DE, Andreassen PR, Tonks NK, Krebs EG, Fischer FH, Morgolis RL. Cytokinetic failure and asynchronous nuclear division in BHK cells overexpressing a truncated protein-tyrosine-phosphatase. Proc Natl Acad Sci USA. 1992;89:5422–5426. 11. del Pozo E, Neufeld M, Schluter K, et al. Endocrine profile of a long-acting somatostatin derivative SMS 201-995. Study in normal volunteers following subcutaneous administration. Acta Endocrinol 1986;111: 433–439. 12. Demirtas E, Sag C, Kursaklioglu H, et al. Effects of octreotide in patients with hypertrophic obstructive cardiomyopathy. Jpn Heart J 1998;39:173–181. 13. Fallo F, Barzon L, Boscaro M, Casiglia E, Sonino N. Effect of octreotide on 24-h blood pressure profile in acromegaly. Am J Hypertens 1998;11:591–596. 14. Filuk RB, Berezanski DJ, Anthonisen NR. Depression of hypoxic ventilatory response in humans by somatostatin. J Appl Physiol 1988;65:1050–1054. 15. Flogstad AK, Halse J, Haldorsen T, et al. Sandostatin LAR in acromegalic patients: a dose-range study. J Clin Endocrinol Metab 1995:80:3601–3607. 16. Fuessl HS, Burrin JM, Williams G, Adrian TE, Bloom SR. The effect of a long-acting somatostatin analogue (SMS 201-995) on intermediary metabolism and gut hormones after a test meal in normal subjects. Aliment Pharmacol Ther 1987;1:321–330. 17. Gaudin C, Moreau R, Champigneulle B, Soubrane O, Kleber G, Lebrec D. Short-term cardiovascular effects of somatostatin in patients with cirrhosis. Liver 1995;15:236–241. 18. Gillis JC, Noble S, Goa KL. Octreotide long-acting release (LAR). Drug 1997;53:681–699. 19. Grant MB, Wargovich TJ, Ellis EA, Caballero S, Mansour M, Pepine CJ. Localization of insulin-like growth factor I and inhibition of coronary smooth muscle cell growth by somatostatin analogues in human coronary smooth muscle cells. A potential treatment for restenosis? Circulation 1994;89:1511–1517. 20. Grunstein RR, Ho KY, Berthon-Jones M, Stewart D, Sullivan CE. Central sleep apnea is associated with increased ventilatory response to carbon dioxide and hypersecretion of growth hormone in patients with acromegaly. Am J Respir Crit Care Med 1994;150:496–502. 21. Grunstein RR, Ho KY, Sullivan CE. Sleep apnea in acromegaly. Ann Intern Med 1991;115:527–532. 22. Grunstein RR, Ho KY, Sullivan CE. Effect of octreotide, a somatostatin analog, on sleep apnea in patients with acromegaly. Ann Intern Med 1994;121:478–483. 23. Harris AG. Somatostatin and somatostatin analogues: pharmacokinetics and pharmacodynamic effects. Gut 1994;35(Suppl 3):S1–S4. 24. Hoeldtke RD, Davis KM, Joseph J, Gonzales R, Panidis IP, Friedman AC. Hemodynamic effects of octreotide in patients with autonomic neuropathy. Circulation 1991;84:168–176. 25. Hoeldtke RD, O’Dorisio TM, Boden G. Treatment of autonomic neuropathy with a somatostatin analogue SMS-201-995. Lancet 1986;2:602–605. 26. Ito H, Hiroe M, Hirata Y, et al. Insulin-like growth factor-I induces hypertrophy with enhanced expression of muscle specific genes in cultured rat cardiomyocytes. Circulation 1993;87:1715–1721. 27. Jones CR, Millar JA, Lawrie C, Summer DJ, Reid JL. Specific inhibition of aldosterone response to endogenous and exogenous angiotensin II by somatostatin. Clin Endocrinol 1984;21:279–284. 28. Kobayashi S, Nishimura M, Taguchi H, Miyamoto K, Kawakami Y. Effect of octreotide on ventilation and dyspnea sensation in a patient with cirrhotic hypoxemia. Intern Med 1995;34:401–405. 29. Kutz K, Nuesch E, Rosenthaler J. Pharmacokinetics of SMS 201-995 in healthy subjects. Scand J Gastroenterol 1986;21(Suppl 119):65–72. 30. Lamberts SWJ, Oosterom R, Neufeld M, del Pozo E. The somatostatin analog SMS 201-995 induces long-acting inhibition of growth hormone secretion without rebound hypersecretion in acromegalic patients. J Clin Endocrinol Metab 1985;60:1161–1165. 31. Lemaire M, Azria M, Dannecker R, Marbach P, Schweitzer A, Maurer G. Disposition of sandostatin, a new synthetic somatostatin analogue, in rats. Drug Metab Dispos 1989;17:699–703. 32. Lembcke B, Creutzfeldt W, Schleser S, Ebert R, Shaw C, Koop I. Effect of the somatostatin analogue sandostatin (SMS 201-995) on gastrointestinal, pancreatic, and biliary function and hormone release in normal man. Digestion 1987;36:108–124. 33. Lim MJ, Barkan AL, Buda AJ. Rapid reduction of left ventricular hypertrophy in acromegaly after suppression of growth hormone hypertension. Ann Intern Med 1992;117:719–726. 34. Lindner V, Lappi DA, Baird A, Majack RA, Reidy MA. Role of basic fibroblast growth factor in vascular lesion formation. Circ Res 1991;68:106–113. 35. Liu MW, Roubin GS, King SB III. Restenosis after coronary angioplasty. Potential biologic determinants and role of intimal hyperplasia. Circulation 1989;79:1374–1387. 36. Londong W, Angerer M, Kutz K, Landgraf R, Londong V. Diminishing efficacy of octreotide (SMS Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999 OCTREOTIDE 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 373 201-995) on gastric functions of healthy subjects during one-week administration. Gastroenterology 1989; 96:713–722. Malesci A, Tacconi M, Valentini A, Basilico M, Lorenzano E, Salerno F. Octreotide long-term treatment in patients with portal hypertension: persistent inhibition of postprandial glucagon response without major changes in renal function. J Hepatol 1997;26:816–825. Maxwell DL, Chahal P, Nolop KB, Hughes JM. Somatostatin inhibits the ventilatory response to hypoxia in humans. J Appl Physiol 1986;60:997–1002. McCormick PA, Chin J, Greenslade L, et al. Cardiovascular effects of octreotide in patients with hepatic cirrhosis. Hepatology 1995;21:1255–1260. Mountokalakis T, Kallivretakis N, Mayopoulou-Symvoulidou D, Karvountzis G, Tolis G. Enhancement of renal function by a long acting somatostatin analogue in patients with decompensated cirrhosis. Nephrol Dial Transplant 1988;3:604–607. Nobuyoshi M, Kimura T, Nosaka H, et al. Restenosis after successful percutaneous transluminal coronary angioplasty: serial angiographic follow-up of 229 patients. J Am Coll Cardiol 1988;12:616–623. Padayatty S, Perrins EJ, Belchetz PE. Octreotide treatment increases exercise capacity in patients with acromegaly. Eur J Endocrinol 1996;134:554–559. Patel YC, Greenwood MT, Panetta R, Demchyshyn L, Niznik H, Srikant CB. The somatostatin receptor family. Life Sci 1995;57:1249–1265. Reichlin S. Somatostatin. N Engl J Med 1983;309:1495–1501, 1556–1563. Reisine T, Bell GI. Molecular biology of somatostatin receptors. Endocrine Rev 1995;16:427–442. Reubi JC, Lamberts SWJ, Maurer R. Somatostatin receptors in normal and tumoral tissues. Horm Res 1988;29:65–69. Reubi JC, Maurer R, von Werder K, Torhoest J, Klijn KGM, Lamberts SWJ. Somatostatin receptors in human endocrine tumors. Cancer Res 1987;47:551–558. Rodriguez-Perez F, Albillos A, Groszman RL. Octreotide improves renal function, total exchangeable sodium, and peripheral hemodynamics in cirrhotic patients with ascites. Gastroenterology 1993;104:980A. (Abstract). Ross R. The pathogenesis of atherosclerosis. An update. N Engl J Med 1986;314:488–500. Sabat M, Guarner C, Soriano G, et al. Effect of subcutaneous administration of octreotide on endogenous vasoactive systems and renal function in cirrhotic patients with ascites. Dig Dis Sci 1998;43:2184–2189. Sacca L, Cittadini A, Fazio S. Growth hormone and the heart. Endocr Rev 1994;15:555–573. Sakamoto H, Sakamaki T, Kanda T, et al. The somatostatin analog, octreotide, inhibits in vitro outgrowth of smooth muscle cells from canine coronary and carotid atherosclerotic plaque tissues. Res Commun Mol Pathol Pharmacol 1998;101:25–34. Schwartz RS, Topol EJ, Serruys PW, Sangiori G, Holmes DR. Artery size, neointima, and remodeling. Time for some standards. J Am Coll Cardiol 1998;31:2087–2094. Sheppard M, Shapiro B, Pimstone B, Kronheim S, Berelowitz M, Gregory M. Metabolic clearance and plasma half-disappearance time of exogenous somatostatin in man. J Clin Endocrinol Metab 1979;48:50– 53. Sieber C, Gnadinger M, del Pozo E, Shaw S, Weidmann P. Effect of a new somatostatin analogue SMS 201-995 (Sandostatin) on the renin-aldosterone axis. Clin Endocrinol 1988;28:25–32. Srikant CB, Shen SH. Octreotide somatostatin analog SMS 201-995 induces translocation of intracellular PTP1C to membranes in MCF-7 human breast adenocarcinoma cells. Endocrinology 1996;137:3461–3468. Stewart PM, Kane KF, Stewart SE, Lancranjan I, Sheppard MC. Depot long-acting somatostatin analog (Sandostatin-LAR) is an effective treatment for acromegaly. J Clin Endocrinol Metab 1995;80:3267–3272. Tokgozoglu SL, Erbas T, Aytemir K, Akalin S, Kes S, Oram E. Effects of octreotide on left ventricular mass in acromegaly. Am J Cardiol 1994;74:1072–1074. von Essen R, Ostermaier R, Grube E, et al., for the VERAS Investigators. Effects of octreotide treatment on restenosis after coronary angioplasty. Results of the VERAS study. Circulation 1997;96:1482–1487. Yarden Y, Ullrich A. Growth factor receptor tyrosine kinases. Annu Rev Biochem 1988;57:443–478. Yumi K, Fagin JA, Yamashita M, et al. Direct effects of somatostatin analog octreotide on insulin-like growth factor-I in the arterial wall. Lab Invest 1997;76:329–338. Cardiovascular Drug Reviews, Vol. 17, No. 4, 1999