Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
1
Description
The following is a case about a 72 year old man with hypertension who is ultimately diagnosed with
renal artery stenosis. The case provides an opportunity to integrate physiology with clinical skills, and to
introduce students to elements of pathophysiology and clinical reasoning. Students are expected to
explain the physiology of blood pressure control and to use their basic science knowledge as a
framework to discuss a clinical presentation of secondary hypertension. This resource was designed as a
two hour case based learning activity to be implemented in a first year Physiology course for
undergraduate medical students.
Educational goals:
1) Link physiologic concepts with clinical presentation.
2) Develop critical thinking and group skills to advance individual and collective knowledge.
Specific learning objectives:
Recognize physical exam findings suggestive of chronic hypertension
Explain why serum creatinine concentration may be used as a measure of renal function
Explain the physiological factors and systems controlling blood pressure
Predict how alterations in renal function lead to changes in blood pressure
Interpret an arterial blood gas
Conceptual background:
Experienced health physicians must synthesize and integrate information from multiple sources and
disciplines. In order to foster this skill, undergraduate medical curricula must provide ample
opportunities for guided practice. The first and second years of medical school traditionally focus on
providing basic science foundations and clinical reasoning skills. On the other hand, the third and fourth
years traditionally build on those foundations to hone skills related to the generation of a differential
diagnosis, the interpretation of laboratory and radiologic studies, and the decisions regarding the
treatment and management of disease. Case based discussions (CBD) have emerged as an effective
method to promote student learning and satisfaction. A systematic review of 102 papers regarding the
use of CBD in the education of various types of health professionals (including medicine), revealed that
this teaching method contributes to student learning by enhancing relevance, understanding of
concepts, and problem solving skills. 1 Importantly, according to their self-evaluation, students
participating in CBL are better able to see the connection between knowledge and clinical practice. 2
Different methodologies of CBD-teaching have been used to teach physiology with positive outcomes,
including the promotion of better understanding of integration of physiological systems, 3 and enhanced
student performance when compared to lecture alone. 4, 5
This resource was created as an attempt to emphasize the physiologic interdependence of the multiple
organ systems, and to provide clinical relevance to physiologic concepts taught during the first year. We
selected the topic of hypertension because it requires students to review and integrate concepts from
2
multiple organ systems. To optimize integration between clinical skills and physiological systems, a
collaborative approach between two basic scientists and a clinician was used. Prior to this CBD session,
students learned basic principles of cardiovascular and renal physiology, the function of the autonomic
nervous system, and acid-base homeostasis. The challenge for students was to integrate learning from
across these systems to explain the control of blood pressure, and to apply this information to the
generation of a physiologically determined differential diagnosis.
In addition, to promote self-directed learning, students were asked to complete a clinical inquiry
activity. As a group, students identified additional areas of basic or clinical interest and worked together
to explore and answer their own questions.
Resources files:
This resource contains two parts: 1) The student version and, 2) The facilitator guide. Both parts contain
the case and the questions; the facilitator guide includes answers to all questions, references, and
examples of probing questions that may be used to assist students in further exploration.
Use of resources:
Student version: Students do not know the topic of the case in advance and are not expected to
prepare for the session. Students are divided into groups of about 8-12; each group is led by one
facilitator. The case unfolds in five parts; students are given one part at a time and asked to
discuss it completely before moving on. At the end of the session, the students receive a list of
learning objectives.
Facilitator guide: The facilitator guide is sent to participating faculty 1-2 weeks in advance for
review. Before the session, faculty meets to discuss the case, past experiences, and potential
pitfalls. Participating faculty include clinicians and basic scientists. During the faculty meeting,
the clinician author reviews the interpretation of the history, physical exam, and differential
diagnosis. The basic scientist author reviews the relevant physiology and pathophysiologic
concepts.
Practical implementation
Materials needed: A facilitator guide and a student version of the case, as provided, small
rooms and facilitators. The number of rooms and facilitators depend on the number of students
per class.
Length of the session: We have allotted two hours for the discussion of this case.
Faculty/facilitator needs: Because we have both clinicians and basic scientists facilitating
groups, we have found that meeting as a group prior to the case session helps to assure that all
facilitators are comfortable with the material. The facilitator guide should be distributed with
enough time to be reviewed before the meeting. Although we have always met with the
facilitators, an alternative is to create a podcast for each case.
Preparation needs: Students are not required to prepare in advance and they do not have any
information about the topic of the case. Although not part of our educational goal, an
3
alternative to this method is to assign topics to prepare in advance, in which new case material
can be introduced each time.
Correlation with clinical skills: At the time point the case occurs, students have been introduced
to clinical reasoning and basic differential diagnosis generation through their clinical skills
course. The case was developed with input from the clinical skills instructors in order to
incorporate skills appropriate to the students’ level of learning. The clinical sessions of the case
can be adapted according to the curriculum of individual schools. Additionally, depending on the
time allotted to the session, questions addressing the correlation with other courses can be
incorporated, according to the schools’ individual curricular design.
Evaluation of the session: Students are evaluated by the group facilitator at the end of the
session based on the rubric shown below. At the end, a comment box for written comments is
always included. The rubric is included in the syllabus of the course and presented to the
students during orientation, along with clear outlined expectations. The rubric as well as the
expectations for student’s performance is discussed with all facilitators prior to the session
(facilitator meeting)
Points awarded:
1 point for Participation/ Engagement
Explanation: The student gains this point by being engaged throughout the session,
contributing to the discussion, asking and answering questions
The student loses the point if he/she rushes through activity (premature closure of the case
without appropriate analysis of all the variables)
1 point for Assignment-inquiry
Explanation: In the last part of the session, the students are expected to identify one
question (per group) that was not answered during the discussion. Question can be clinical,
basic or related to research. The group should discuss on site the relevance of the question
and why they are interested to know the answer; the question must be approved by the
facilitator.
- The selected question per group must be turned in at the end of the session to the
facilitator.
- The group is expected to complete the appropriate research and submit ONE
GROUP answer by Monday 5pm to the course director via email. Feedback will be
provided.
- Copy/paste from online sources or any form of plagiarism will not be tolerated and
will lead to losing the point.
The point will be given upon satisfactory completion of all these requirements, showing the
appropriate level of inquiry for first year medical students
1 point for Professionalism
Explanation: The students must be professional at all times. The point can be lost if the
student:
Is not on time
- Leaves the room for more than 10 minutes
- Is disruptive (e.g. do not let other students talk)
- Uses cell phone or other electronic devices not instructed by the facilitator
- Is disrespectful to peers or faculty
4
Lessons learned:
We have incorporated CBD since 2012. The updated version of this resource has been used since 2014.
It has been well received by students.
Earlier iterations of this CBD revealed some pitfalls:
Discrepancies between groups in the amount of time spent on and the emphasis given to the
clinical and basic science portions of the case. Faculty development and pre-/ post-session
meetings with faculty continue to be necessary to minimize this problem. We have modified the
facilitator guide to include some directives on the topics where students should spend
additional time (*).
The expectation of what the students were supposed to learn by the end of the session was not
always clear. To correct this, learning objectives are now included at the end of the case and
facilitators are asked to review the objectives with the group prior to adjourning the session.
Some facilitators had difficulty encouraging students to dig deeper in their mechanistic
explanations or to extend their clinical reasoning beyond the superficial level. The resource has
been modified to include probing questions, which help facilitators to feel confident that the
students are thoroughly exploring all of the intended learning objectives.
Tips for success:
-
-
-
-
-
Include in the facilitator guide a cover page with a summary of the case, the learning objectives,
the format of the case, and a brief description of what students know prior to the session. The
case and/or facilitator guide may be modified to fit other curriculum or educational goals.
Modify the facilitator guide based on feedback: We request feedback from students and
facilitators at the end of the course and adapt the guide/case as necessary.
Faculty development: All facilitators should be trained in Case Based Learning. Additionally, new
facilitators are evaluated by our “Office of Learning and Teaching” and provided with feedback.
Most facilitators prefer to meet after the session to debrief. Whenever possible, new facilitators
are paired with more experienced faculty for several sessions prior to facilitating on their own.
For the question “frame the case” (question number two) we have found that it is helpful to give
students 1-2 minutes to work independently. The individual responses are then discussed with
the group; each student has an opportunity to receive feedback from the other members of the
group (generally the facilitator does not have to intervene).
For the assignment (conclusion), we also give students several minutes to work independently.
The questions are then discussed with the entire group. The students should use relevance and
specificity as criteria to select the question they wish to explore.
If evaluation is part of this session, it is helpful to include a rubric and conduct faculty
development sessions to assure inter-rater reliability.
Include questions from the cases in the assessment of the course. This reinforces the
importance of the sessions.
Provide individual written constructive feedback to students at the end of the case.
5
Self-reflection:
Although questions about content discussed in the cases were incorporated into the course
examinations, we are unable to determine if the cases contributed to a higher performance in students.
The reason for this is that, based on the current curricular design of the class, we cannot determine
whether an increased performance is due to the cases, the lectures and/or the repetition. The goal of
the cases was not to introduce new information, but rather to use them to reinforce topics previously
learned in lectures, integrate information from multiple lectures/courses, or to introduce topics that will
be covered in later lectures.
We are satisfied with the student responses on surveys and examinations. Overall, the cases are well
received and students feel that they significantly contribute to their learning (54% of students strongly
agree and 33% of students agree). We believe that this related to two main factors: 1) The addition of
clinical relevance to the basic science concepts allows the students to situate the newly attained
knowledge, and 2) The interactive group process forces students to actively participate in their learning
as opposed to passively reviewing information. The small group format provides the students with the
opportunity to meet their learning needs and to receive individual feedback; it also allows faculty to
identify students at risk. In our experience, the major limiting factor is the need to have a large number
of adequately trained small group facilitators to equalize the experiences between groups. It is our goal
to expand this approach throughout the first year.
References:
1. The effectiveness of case-based learning in health professional education. A BEME systematic
review: BEME guide No. 23. Thistlethwaite JE, Davies D, Ekeocha S, Kidd JM, MacDougall
C, Matthews P, Purkis J, Clay D. Medical teacher 2012; 34: e421-444
2. Attitudes of faculty and students toward case-based learning in the third-year obstetrics and
gynecology clerkship. Hansen WF, Ferguson KJ, Sipe CS, Sorosky J.Am J Obstet
Gynecol. 2005 Feb; 192(2):644-7.
3. Teaching integrative physiology using the quantitative circulatory physiology model and case
discussion method: evaluation of the learning experience. Rodríguez-Barbero A, López-Novoa
JM. Adv Physiol Educ. 2008 Dec; 32(4):304-11.
4. Effectiveness of case-based teaching of physiology for nursing students. Farrukh
Majeed, FCPS, Journal of Taibah University Medical Sciences. 2014:1-4
5. Impact of case-based lectures on students' performance in vascular physiology module. Rabia Latif.
Advances in Physiology Education. September 2014. Vol. 38no. 3,268-272
6
FACILITATOR GUIDE
Summary: This case is about a 72 year old man with a history of hypertension, presenting with three
weeks of progressively frequent and severe headaches. Ultimately, he is diagnosed with renal artery
stenosis.
Learning objectives:
At the end of the case based discussion, students should be able to:
Recognize physical exam findings suggestive of chronic hypertension
Explain why serum creatinine concentration may be used as a measure of renal function
Explain the physiological factors and systems controlling blood pressure
Predict how alterations in renal function lead to changes in blood pressure
Interpret an arterial blood gas
Timing: This is the third case of the course. Students are currently in the renal segment of the course.
Prior content learned includes cardiovascular physiology, the cardiac clinical exam, neurophysiology,
and musculoskeletal physiology. Students have not learned control of blood pressure as a single unit.
They have discussed a prior case about pulmonary hypertension and they have been exposed to
isolated facts about how different parameters affect extracellular fluid volume, vascular resistance,
and blood pressure. The challenge for them will be to put all of this information together.
Format: The case unfolds in six parts. Please give students one part at a time, discuss one part
completely before giving them the next part. At the end of the session, ask students to review the
learning objectives and discuss as a group whether or not all objectives were met. Students should
understand that material covered during the case session may be seen on exams.
Key concepts this week are indicted with a (*).
Please collect all papers at the end of the session.
The case is scheduled to last two hours.
7
Part 1
Andrew Martin is a 72 year-old man presenting to your primary care clinic with three weeks of
progressive headache.
1.
What questions might you want to ask of the patient?
Facilitators: It is not necessary to provide answers at this point. Relevant information is included in
subsequent parts.
Onset (“When did it start?”)
First noticed it about three weeks ago
Frequency (“How often?”)
Started about 1-2 times per week, now every day for last few
days
Duration (“How long?”)
Started with 1-2 hours, now lasting most of the day until I lay
down to sleep
Location, radiation (“Where, point”)
Mostly behind my eyes, either side, sometimes both, some
tightness in my neck
Quality (“What’s it like?”)
Sort of throbbing
Severity (“On a scale of 1-10…”)
Started at a 3-4 but now usually 7-8
Modifying factors (Anything make it
Worse with stressful situations, exertion; slightly better with
better/worse?”)
sleep, relaxation.
Associated symptoms (“Anything comes No photophobia/phonophobia, no aura, no visual changes, no
with it?”)
nausea/vomiting, no tingling or other neurologic changes
Other complaints?
Fatigue
Other complaints related to potential
None
long term complications of HTN:
-Exertional chest pain/SOB, exertional
pain in the legs
Past medical/surgical history?
“They told me that my blood pressure was high a few years ago.
I took some pills for a few months but I didn’t feel any different
and they were really expensive, so I stopped.”
No surgeries, never hospitalized.
Medications
None
Don’t remember the name of the pills I used to take.
OTC meds, supplements, vitamins?
Occasional Tylenol for the headache but it doesn’t help. Maybe
three times in the last three weeks. One pill, doesn’t know the
mg dosage.
Allergies?
None
Social History, smoking, ethanol, drugs? Lives with wife. Two grown kids living out of state. Retired,
worked in construction. Barely making ends meet on limited
retirement savings. Drinks 3-4 beers on the weekends with
friends, smoked about1ppd between ages 17-61.
Family History?
Mother died age 81 with stroke. Father died age 56 in a car
accident.
8
Part 2
Mr. Martin states that he first noticed the headaches about three weeks ago. When the
headaches started, they were occurring about 1-2 times per week, but for the last few days they
have been occurring every day. In the beginning, the headaches lasted 1-2 hours, but they are
now lasting most of the day. The pain is mostly behind his eyes (either side, sometimes both),
and sometimes associated with some tightness in the neck. The pain is throbbing and he rates it
as a 7-8 out of 10 (they started at a 3-4 a few weeks ago). The headaches seem to be worse
when he is feeling more stressed and when he exerts himself, and slightly better with sleep or
when he is relaxed. There is no associated photophobia/phonophobia, no aura, no visual
changes, no nausea/vomiting, and no tingling or other neurologic changes. He denies chest pain,
shortness of breath, or diaphoresis.
He was told that he had high blood pressure a few years ago and says that he “took some pills
for a few months but I didn’t feel any different and they were really expensive, so I stopped.
The Mrs. and I are barely making ends meet these days, you know we weren’t able to put too
much away in savings for these years… ”
He has had no surgeries and has never been hospitalized. He doesn’t remember the name of
the pills he used to take and takes no medications now. He occasionally takes Tylenol for the
headache (it doesn’t help) but no other over the counter medications, vitamins, or herbals. He
denies allergies. He lives with his wife. He has two grown kids living out of state. He is retired
now but used to work in construction. He drinks 3-4 beers on the weekends with friends and
smoked about 1ppd between the ages of 17-61. He denies drug use. His mother died at age 81
from a stroke and his father died at the age of 56 in a car accident.
2. How would you “frame this case?” What are the key features of this presentation that you must
explain?
Think of the frame as a “problem representation” to be used in the generation of a differential
diagnosis. It is the problem that you must explain. The ‘frame’ consists of the core elements of
the case including the patient’s age, gender, relevant medical history, chief complaint, and time
course of progression.
Students should include these elements and “present” the patient in a succinct 1-2 sentence format.
Example: “This is a 72 year old man with a history of HTN presenting with three weeks
of progressively frequent and severe headaches.”
3. Generate a differential diagnosis to explain Mr. Martin’s headache.
Facilitators: Have the students choose a “scribe” to write down potential diagnoses on the board.
Due to the fact that students have not yet studied pathophysiology, they have limited experience in
generating complicated differential diagnoses. However, with encouragement, they should be able
to come up with at least a few of the following:
- Hypertension related
9
-
Migraine
Stress related (tension) headache
Sinus pressure
Intracranial mass
Intracranial bleeding (aneurysm or other trauma related hemorrhage)
Stroke
Diagnoses that students are less likely to bring up:
o Meningitis/encephalitis (intracranial infection)
o Vasculitis (temporal or giant cell arteritis)
o Temporal-mandibular joint related
o Trigeminal neuralgia
4. What will you be looking for on physical exam to help you narrow your differential diagnosis?
Facilitators: Have the students use their differential to guide them here. They will not have findings
for all diagnoses.
- Hypertension related:
o check blood pressure, but also:
markers of chronic hypertension: retinal changes, S4 gallop, lateral
displacement of cardiac apical PMI, enlargement of cardiac apical PMI,
symmetry and strength of peripheral pulses to suggest vascular disease, carotid
bruits to suggest vascular disease.
Markers of potential causes of secondary hypertension: abdominal bruit over
renal arteries, thyromegaly or thyroid nodules,
- Migraine
- Stress related (tension) headache
- Sinus pressure:
o May have sensitivity to tapping over sinuses or opacification if light is shined on sinuses.
- Intracranial mass
o Focal signs on neurologic exam (students have not yet learned complete neuro exam)
o Possibly papilledema
- Intracranial bleeding (aneurysm or other trauma related hemorrhage)
o Focal signs on neurologic exam (students have not yet learned complete neuro exam)
o Possibly papilledema
- Stroke
o Focal signs on neurologic exam (students have not yet learned complete neuro exam)
o Possibly papilledema
- Meningitis/encephalitis (intracranial infection)
o Kernig’s Sign (inability to extend the knee when the hip is flexed 90 degrees), Brudzinski
Sign (flexion at the hip and knees in response to passive flexion of the neck). Students
will not yet have learned of these signs.
- Vasculitis (temporal or giant cell arteritis)
o Tenderness over the temporal arteries. Students are unlikely to know this.
10
-
Temporal-mandibular joint related
o Tenderness or “clicking” over the temporomandibular joint.
Trigeminal neuralgia
11
Part 3
Vital Signs: T 98.5, HR 90, RR 14, BP 210/100 (right arm, seated), BMI 32
General Appearance: Fatigued appearing, well groomed, obese man sitting in a chair in no
distress.
Head: Normocephalic, atraumatic. Pupils are equally reactive to light and accommodation.
Conjunctivae are pink and moist. Optic fundi show thickening of the arteriolar walls and
arteriovenous nicking. Optic disc margins are clearly defined. There is no tenderness to
palpation of the sinuses. Oral mucosa is moist, no lesions. There is no tenderness over the
temporomandibular joints which move smoothly bilaterally.
Neck: Neck is supple with no lymphadenopathy, thyromegaly, or palpable nodules. No bruit
carotid is heard. Jugular venous pulsation is noted 4cm above the sternal notch.
Cardiovascular: S1 and S2 normal, regular rate and rhythm, no murmurs or rubs. S4 gallop is
heard at the apex. PMI is laterally displaced, sustained, and diffuse. Pulses are palpable and
symmetric throughout.
Lungs: Clear to auscultation bilaterally.
Abdomen: Soft, obese, non-tender, non-distended, normal bowel sounds, no organomegaly. A
continuous bruit is heard both during systole and diastole when auscultating over the right
upper quadrant. The same bruit is heard over the right costovertebral angle.
Extremities: Warm and well perfused. No cyanosis, clubbing, or edema.
Neurological examination: Patient alert and oriented to person, place and time. CNs II-XII intact.
Motor strength, sensation, and reflexes normal.
5. How do you interpret the findings of the clinical exam?
- The blood pressure is elevated.
- Fundoscopic exam suggests sequelae of chronic hypertension.
- Clearly defined optic disc margins make causes of elevated intracranial pressure (like
masses, edema, or bleeding) unlikely.
- No tenderness over the sinuses or temporomandibular joints makes sinusitis or TMJ
related pathology less likely.
- The lack of thyromegaly or nodules may make hyperthyroidism less likely.
- S4 gallop is a marker of possible ventricular hypertrophy. PMI should be in the
midclavicular line, about 2.5 cm in diameter and feel like a brief tap, not sustained –
these changes also suggest ventricular hypertrophy due to chronic hypertension.
12
-
-
Bruits heard in the upper quadrants of the abdomen suggest turbulent flow through the
renal arteries. Classically, the bruit of renal artery stenosis is continuously heard (both in
systole and diastole) and can also be heard with auscultation over the ipsilateral flank.
The normal neurologic exam makes stroke and other intracranial lesions (mass,
hemorrhage, etc.) less likely.
6. What is an S4 gallop? When is it heard? What does it represent? Start by drawing a diagram
showing where the normal heart sounds (S1 and S2) are heard and what causes those sounds.
Where in the cycle would you hear the S4?*
S4 is a pre- systolic sound. It occurs at the end of diastole just prior to systole, before the S1.
Most of diastole is passive filling of blood. Just before systole you have the atrial “kick” which is the only
time blood is actively pushed into the ventricles. If this last bit of actively pushed blood (during the atrial
kick) hits a stiff ventricle, an S4 may be heard.
One can have a stiff ventricular wall due to long standing hypertension, a previous or new infarction, or
anything else that would chronically increase afterload and lead to a hypertrophied ventricle (such as
aortic stenosis). An S4 is always abnormal.
13
Part 4
The patient is asked to sit calmly for five minutes and then the blood pressure is rechecked in
the left arm and found to be 208/102 mmHg.
Labs reveal normal electrolytes with an elevated serum creatinine of 1.9 mg/dL (normal
approximately <1.0).
An EKG is done in the office and shows evidence of left ventricular hypertrophy (thickening of
the muscular wall of the left ventricle).
Dipstick urinalysis is positive for protein (2+) and trace blood.
7. What does the elevated serum creatinine suggest? Explain your answer.*
Elevated creatinine indicates reduced glomerular filtration rate (GFR), suggesting impaired
glomerular function.
If not explained fully, ask the students, “What physiological parameter is an appropriate
indicator of GFR? Why would an elevated serum creatinine signify reduced GFR? ?
Clearance refers to the removal of a substance from the blood. Creatinine clearance is a
good approximation of GFR because creatinine is freely filtered in the glomerulus, not
metabolized, not reabsorbed and only minimally secreted. Therefore, most of the
creatinine that is filtered is excreted. Creatinine clearance is not given, but because
Clearance=excretion rate/plasma concentration, it can be assumed that clearance is
decreasing. An increased in the plasma creatinine concentration (assuming that it is not
accompanied by an increase in production) indicates a decrease in renal excretion rate,
which can be explained by a decrease in filtration rate.
8. How do you interpret the results of the urinalysis? Explain your answer.*
Blood and protein in urine are not normal findings. Proteins are not freely filtered in the
glomerulus due to their negative charge, and red blood cells are not filtered due to their size.
Thus, they should not appear in the urine when glomerular filtration is intact.
If students don’t explain the filtration barrier, ask them: Why are proteins and RBCs not freely
filtered in the normal kidney?
Proteins and cells are excluded from the filtrate due to the existence of a glomerular
filtration barrier containing three layers: fenestrated capillary endothelium; basal
membrane, and epithelial layer containing the podocyte foot processes. The fenestration
and the slit pores of the podocytes exclude larger macromolecules, particles and cells
based on size. The negative charge of the basement membrane and other proteins in the
barrier exclude negatively charged macromolecules, such as proteins. The detection of
proteinuria on urinalysis is consistent with hypertensive damage to the glomeruli.
Results in the urinalysis can be interpreted as evidence for renal and cardiac damage resulting
from his hypertension.
14
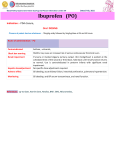
9. Draw a diagram to illustrate the physiological determinants of blood pressure. Based on this
diagram, identify at least three potential causes of hypertension. Describe the physiologic
alterations responsible for each mechanism.*
Diagram should include cardiac output and vascular resistance (see diagram next page for an example).
They should discuss that any condition that increases either of those two variables (which are not
necessarily independent) could lead to an increase in blood pressure.
Cardiac output can be altered by changes in stroke volume or heart rate.
Vascular resistance can be altered mainly by changing the diameter of blood vessels, either
vasoconstriction or vasodilation. Other variations are mediated by changes in viscosity or length
(less physiologically significant).
Examples of physiological alterations leading to hypertension they could discuss are:
Obesity: Increased cardiac output and expansion of extracellular volume, as well as
activation of the sympathetic nervous system
Congenital defects in blood vessels or damage to blood vessels (examples, tobacco use)
Any condition that activates the sympathetic nervous system leading to vasoconstriction,
increased peripheral resistance and cardiac output (examples: anxiety, obesity, pain or
any other stress)
Increased dietary intake of sodium, leading to expansion of the extracellular volume
Drug induced: cocaine, amphetamines (due vasoconstriction and increased cardiac
output)
Hormone mediated (linked to the RAAS or to the autonomic nervous system)
o Primary aldosteronism (high aldosterone)
o Cushing's syndrome (high glucocorticoids-can activate the aldosterone receptor)
o Pheochromocytoma (production of mineralocorticoid)
o Estrogen treatment ("pill hypertension")
Diagram Abbreviations: epinephrine (EPi), norepinephrine (NE), angiotensin II (Ang II), renin angiotensinaldosterone system (RAAS), antidiuretic hormone (ADH), atrial natriuretic peptide (ANP), prostaglandin
(PG), nitric oxide (NO); 1R and 2R are subtypes of the adrenergic receptors; (+) increases, (-)
decreases.
15
16
10. Using the diagram you created, identify the factors involved in the short and long term regulation
of blood pressure. Explain the mechanisms that activate the short term and the long term
responses.
Students do not learn this in class, they have learned the elements individually but they will need to put
them together.
Short term control: changes are sensed by baroreceptors (detect changes in BP) and chemoreceptors
(detect changes in O2, pH, CO2) and send information to brainstem centers to stimulate/inhibit
parasympathetic output and stimulate/inhibit sympathetic output in opposing directions:
Normal function of the sympathetic ANS is to increase cardiac output and total peripheral
resistance (-1 adrenergic mediated vasoconstriction of arteries in skin and viscera,
adrenergic stimulation of heart rate (chronotropy) and stroke volume due to increased
contractility (isotropy).
o Effect of sympathetic system on sodium control:
- Direct stimulation of Na+ reabsorption (-1 adrenergic receptors in proximal
tubule)
- Indirect effect: renin release ( adrenergic mediated, see below); also,
decreases GFR and renal blood flow (-1 adrenergic receptors in arterioles)
Normal function of the parasympathetic system is to decrease heart rate and to induce
vasodilation (mediated by acetylcholine-muscarinic receptor interaction)
Long term control: mediated by hormones
Renin-Angiotensin-Aldosterone system (RAAS) activation in response to low blood pressure (most
significant long term control from the physiological point of view):
o Activation: sympathetic nerve terminals (via 1 adrenergic receptors), low Na+ (via
delivery to the distal tubule), low blood volume.
o Path:
i.
Renin is released from the juxtaglomerular cells in the nephron
ii.
Renin (a protease) converts angiotensinogen (secreted by the liver) to angiotensin I
iii.
Angiotensin I is converted to its active form, angiotensin II by angiotensin converting
enzyme (ACE), which is present mainly in the lungs (conversion also occurs in other
tissues)
iv.
Angiotensin II has several functions:
- Preferentially constricts afferent arterioles, which has the following effects: 1)
decreases renal blood flow and hence filtration fraction, which increases oncotic
pressure in the peritubular capillaries, 2) increases pressure in the glomerular
capillaries, which decreases GFR and retention of waste products, and 3)
decreases peritubular capillary hydrostatic pressure
- Increases Na+ reabsorption directly by stimulating transport in the proximal
tubule, loops of Henle, distal and collecting ducts (e.g. stimulating Na+/K+
ATPase)
17
-
Increases Na+ reabsorption indirectly by stimulating aldosterone secretion
The normal function of aldosterone is to stimulate Na+ reabsorption (increases
ECF volume) and the excretion of K+ and H+ ions.
Non renal role: Angiotensin II is a vasoconstrictor, which will increase peripheral
resistance
Other factors:
Release of Atrial Natriuretic Peptide (ANP) from the atria of the heart in response to high BP
o Stimulates Na+ and water excretion in the urine by the kidney.
o Promotes vasodilation
Antidiuretic Hormone (ADH/ Vasopressin)
o The normal function of ADH is to promote water reabsorption in the collecting ducts,
thus increasing ECF osmolality (diluting ECF)
o ADH is released from the posterior pituitary when there is an increase in plasma
osmolality (too much sodium)
Epinephrine release from the adrenal medulla:
o Mimic sympathetic actions
o Normal function is to increase heart rate and vasoconstriction via alpha and beta
adrenergics, which lead to high BP)
11. Generate a problem list for Mr. Martin. Your list should include all of the issues that you will need
to address with your patient. How will you address each of these issues?
Facilitators: This is one of the first times that students will be asked to generate a problem list, so
they may need help in figuring out which types of issues should be included. Have them choose a
scribe to record their thoughts on the board. They should include all medical issues as well as
any social issues that may interfere with the patient’s health or access to care. In addition, we
encourage them to include health maintenance as a category in all primary care problem lists.
They are unlikely to come up with a perfect list or perfect management strategies, but should
understand the basic idea of the problem list and attempt to put together a plan for each
problem. A sample might be:
1) Hypertension
- Lifestyle modifications: weight loss, exercise, low salt diet
- Treat with medications (they don’t need to name which ones)
- Order renal ultrasound with Doppler to evaluate for renal artery stenosis because of
bruit on exam and evidence of renal insufficiency.
2) Headache (possibly secondary to #1)
- Bring blood pressure under control and then re-evaluate if still having headaches
3) Renal Insufficiency with proteinuria and hematuria (possibly secondary to #1 or the cause of
#1)
- Order renal ultrasound as above to investigate for potential renal artery stenosis or
evidence of other parenchymal kidney disease.
18
-
Further work up of causes of renal disease like 24hr urine protein, creatinine, electrolytes
(they will likely not know all of the test one could order)
4) Obesity
- Lifestyle modification: diet, exercise
- Possibly referral to nutritionist
5) Former tobacco use
- Encourage continued cessation
- Annual low dose CT screening for lung cancer (students are unlikely to bring this up)
6) Financial stress/medication non-adherence
- Discussion with patient about importance of medications for BP and why he may not
“feel” the effects of the medications
- Attempts to minimize costs of individual medications chosen
- Referral to social work or case manager for investigation of ways he may gain additional
help with coverage of medication costs
7) Health Maintenance
Colorectal cancer screening if not done (students are unlikely to know which exams are needed for which
patients at this point, but you can refer them to the USPTF website which has helpful guidelines.
19
Part 5
Mr. Martin is diagnosed with hypertension and started on medical treatment with
hydrochlorothiazide (a blocker of the Na+/Cl− transporter in the distal collecting ducts) and
Lisinopril (an ACE inhibitor). Unfortunately, the blood pressure remains elevated despite
incremental increases in the anti-hypertensive regimen.
He is referred to a nephrologist for further evaluation of the renal dysfunction and for work up
of potential renal etiologies of secondary hypertension.
A renal ultrasound is ordered and reveals that the right kidney is 3cm shorter in the longitudinal
axis when compared with the left. Renal Doppler ultrasound reveals waveforms consistent with
renal artery stenosis near the origin of the right renal artery. An angiogram of the renal arteries
is performed and confirms renal artery stenosis with 90% stenosis of the proximal segment of
the right renal artery.
12. Why are hydrochlorothiazide and Lisinopril used to treat hypertension?
Hydrochlorothiazide inhibits the Na+/Cl - transporter (symport) in the distal collecting ducts
This drug acts as a diuretic (promotes water excretion): Reabsorption of water depends on ADH
secretion and the creation of a hyperosmolar gradient that permits the movement of water from
the lumen to the interior of the epithelial cell (reabsorption). Because of the blockade of
electrolyte reabsorption, diuretics such us thiazides collapse the gradient required for water
absorption by increasing the amount of electrolytes present in the lumen. Consequently, the
excretion of sodium and chloride increases.
Lisinopril is an angiotensin converting enzyme (ACE) inhibitor
Blockade of ACE prevents the conversion of angiotensin I to angiotensin II, inhibiting in this way
the RAAS effects (neither angiotensin II nor aldosterone are produced). Because the RAAS
increases blood pressure, blocking this system will result in a reduction in blood pressure
13. How does renal artery stenosis lead to hypertension?*
Renal artery stenosis causes underperfusion of the kidney, which may leads to activation of the RASS:
less Na+ arriving to the nephron stimulates the RAAS, which enhances sodium and water reabsorption,
increasing extracellular fluid volume and BP. Angiotensin also promotes vasoconstriction, which
increases resistance and thus BP.
The other kidney, assuming it is normal, may have increased perfusion and thus reduced RAAS activation,
and increased sodium excretion due to pressure natriuresis.
14. An ABG is done and reported as: pH 7.49, pCO2 48, pO2 100, HCO3 29. This ABG is consistent with
which primary acid-base disorder? Why might renal artery stenosis cause this to occur?*
20
This is a compensated metabolic alkalosis.
Acid-Base
Disturbance
Metabolic Acidosis
Primary
Disturbance
↓ [HCO3-]
Compensation
Predicted Compensatory Response
↓ PCO2
Metabolic Alkalosis
↑ [HCO3-]
↑ PCO2
Expected PCO2=( 1.5 * HCO3) +8
Or 1 mEq/L decrease in HCO3- → 1.3 mm Hg decrease in
PCO2
Expected PCO2=( 0.7 * HCO3) +20
Or 1 mEq/L increase in HCO3- → 0.7 mm Hg increase in
PCO2
Respiratory Acidosis
Acute
↑ PCO2
↑ [HCO3-]
Chronic
↑ PCO2
↑ [HCO3-]
Respiratory Alkalosis
Acute
↓ PCO2
↓ [HCO3-]
Chronic
↓ PCO2
↓ [HCO3-]
Expected HCO3= 24 + [(PCO2 -40)/10]
Or 1 mm Hg increase in PCO2 → 0.1 mEq/L increase in
HCO3Expected HCO3= 24 +{4* [(PCO2 -40)/10]}
Or 1 mm Hg increase in PCO2 → 0.4 mEq/L increase in
HCO3Expected HCO3= 24- {2* [(40- PCO2 )/10]}
Or 1 mm Hg decrease in PCO2 → 0.2 mEq/L decrease in
HCO3Expected HCO3= 24 – {4* [(40-PCO2)/10]}
Or 1 mm Hg decrease in PCO2 → 0.4 mEq/L decrease in
HCO3-
Possible causes:
Proximal tubule: Reabsorption of Na+ increases reabsorption of HCO3− to maintain
electroneutrality.
In the cortical collecting ducts: Reabsorption of Na+ by the principal cells renders the
tubular lumen electronegative and stimulates both K+ and H+ secretion by the K/H+ATPases. Inside the cell, for every proton made, a “new” HCO3− will be generated and
returned to the ECF, contributing to the alkalosis. The increased plasma HCO3− will be
filtered, but the cycle continues
The RAAS system stimulates Na+ reabsorption and K+/H+ excretion (this generally
maintains alkalosis)
21
Part 6: Conclusion
The right renal artery lesion is dilated by balloon angioplasty and a short metallic stent is implanted to
maintain luminal patency. Several days after the procedure, the serum creatinine stabilizes at 1.1 mg/dL
and the blood pressure responds more appropriately to medical treatment.
Assignment: As a group, identify one additional question about this case that you would like to
explore further. Before you leave today, decide on your question, get approval from your facilitator,
and submit your question in writing to the course director. You are required to work as a group to
answer the question.
Responses are limited to 300 words.
Before leaving today, please review the learning objectives as a group.
Learning objectives:
At the end of the case based discussion, students should:
Recognize physical exam findings suggestive of chronic hypertension
Explain why serum creatinine concentration may be used as a measure of renal function
Explain the physiological factors and systems controlling blood pressure
Predict how alterations in renal function lead to changes in blood pressure
Interpret an arterial blood gas