Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
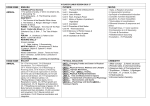
Fisher College Sports Medicine Student-Athlete Pre-Participation Form Instructions for Completion: ● Student-athletes that fail to complete this form fully and accurately will not be allowed to participate in athletics. ● Be sure to mark every answer. After marking yes to a question, please thoroughly describe the condition in the space provided. Information to include: right or left side, injury, treatment, date of injury, etc. ● If you are 18 years of age, you must have your parents or guardians read and sign where indicated. ● You must have and provide documentation of a physical exam completed by a physician prior to the start of your competitive season every year. ● To ensure proof of insurance, we are requiring student-athletes to send in a photo copy (front and back) of their medical insurance card. Failure to provide accurate documentation of insurance coverage will result in a delay in medical clearance. ● Return Forms to: Fisher Athletics Attn: Fisher Sports Medicine 118 Beacon Street Boston, MA 02116 ● All forms should be received by the Sports Medicine Staff no later than Aug 1 st Forms to be handed in include: o This packet o ADD/ADHD medical disclosure (if applicable) o Annual physical form with any updated immunizations received o Copy of insurance card (front and back) 1 Fisher College Sports Medicine Student-Athlete Demographic/Medical History for RETURNING Athletes Please Print Legibly Personal Information Student Name: Sport(s): Class: Institution: Permanent Address: School Address: Email: Gender: Cell Phone #: DOB: Fisher ID #: Insurance Information Do you have the Fisher Student Insurance Plan? Insurance Company Name: Plan Type: Policy Holder Name: Policy Holder DOB: Policy Number: Group Number: Emergency Contact Information Primary Contact Name: Home Phone #: Relationship: Cell Phone #: Secondary Contact Name: Home Phone #: Work Phone #: Relationship: Cell Phone #: Work Phone #: Please list any known allergies: Please list all the medications you are currently taking: 2 Health History Please include any and all explanations in the designated “Yes” section provided below. 1. 2. 3. 4. 5. 6. 7. 8. 9. Yes No Have you had any serious illness, disease, injury, operation, mental illness, infection, accident, or any other significant medical condition during the past year (12 months)? Have you had any injuries, illnesses or other medical conditions that required surgery in the past year (12 months)? If yes, please explain, including date and location. Have you been hospitalized or examined by a physician other than the EC team physician for any type of medical condition during the past year (12 months)? If yes, for what reason? Have you EVER had a concussion that was not evaluated by the EC team physician? If yes, give an explanation, including dates and location. Have you had a family member/relative suffer from sudden death in the past year (12 months)? If so, what was the cause of death? During the past year (12 months) have you had any type of respiratory/breathing problem with exercise? During the past year (12 months) have you ever suffered from a heat related injury/illness (ex. heat cramps, fainting, heat exhaustion, heat stroke)? During the past year (12 months) have you started taking or been prescribed any new medications, supplements, or other substances (ex: birth control, multivitamins, muscle builders)? During the past year (12 months) have you lost or gained a significant amount of weight (>10 lbs)? You MUST explain all “YES” answers below: 10. Complete the chart below and give details to the right if you have sustained any/illnesses injuries during the last twelve (12) months. Yes a. Head/Face b. Neck c. Shoulder d. Elbow e. Forearm f. Wrist/Hand/Fingers i. Chest/Heart/Lungs j. Spine/Ribcage k. Abdomen l. Pelvis No R You MUST explain all “Yes” Answers here: L m. Hip n. Thigh 3 o. Knee p. Ankle q. Foot/Toes If you have any additional conditions, problems, or comments that have not been addressed thoroughly in the above questionnaire, please use the space below to inform us. I, ___________________________________________ (print name) am eighteen years of age or older (if under 18 years of age, signature of parent or legal guardian is required below). As a condition of eligibility for participation in Fisher College Varsity Athletics, I hereby certify and agree to the following: Consent to Treat: · I hereby grant permission for any member of the Fisher College Sports Medicine team (which includes but is not limited to certified athletic trainers and team physicians) to proceed with any needed medical treatment. I understand that medical treatment may include, but is not limited to, the following: preventive measures (e.g. taping, bracing and padding), application of therapeutic modalities, application of ice and heat, rehabilitation exercises for acute, chronic or post-surgical injuries, evaluation of acute or chronic injuries/illness and referrals to other medical professionals. · I understand that in the case of a medical emergency, the student or parent/guardian understands that every reasonable attempt will be made to communicate with the student directly, or in the case of minors, with the student’s parent or guardian, concerning emergency medical treatment of the student. · I understand that in the event of the student-athlete’s incapacity, every attempt will be made by the College and/or Sports Medicine team to communicate with the parent, guardian, or other emergency contact. In the event that the above parties cannot be contacted, the Sports Medicine Team is authorized to act on behalf of the student-athlete even though the parent, guardian, or emergency contact cannot be consulted. My consent to treat applies to treatment involving life saving measures considered to be medically necessary. · I hereby grant permission to the Fisher College Sports Medicine team to discuss any injury/condition with the coaching/administrative staff only as it affects my health and safety during participation in athletics. I give the Fisher College Sports Medicine team permission to obtain and release information concerning injuries/ illness that may impact my health and safety while participating in Fisher College Varsity Athletics. I also, hereby grant permission for any member of the Fisher Sports Medicine team to communicate with Health Services in regards to my general health. In addition, I give permission for Health Services to disclose any medical information as they deem necessary to the Fisher College Sports Medicine team. This permission extends throughout the entire time I am enrolled at Fisher College. _______ (Initial Here) Description of Condition(s)/ Health Status: · I understand the importance of adequate health and conditioning, which is necessary to decrease my risk of illness, injury, or death arising from my participation in varsity athletics. I further understand that it is my duty to completely and accurately disclose all health-related conditions that may, in any way, affect my ability to participate safely. · I recognize that the College’s understanding of my true physical condition is dependent upon an accurate medical history and a full disclosure of any symptoms, complaints, prior injuries, ailments, and/or disabilities I have experienced. I hereby affirm that I have fully disclosed in writing my prior medical history, and at the time of my physical examination, my physician informed me that there was no medical reason for prohibiting or restricting my participation in collision, contact, or non-contact sports. _______ (Initial Here) Change in Health Status: · The information I have provided by to the Sports Medicine team concerning my medical and psychological condition is true and accurate to the best of my knowledge. · I acknowledge that it is solely my responsibility to inform the Fisher College Sports Medicine team of a change in my physical or psychological condition that might affect or impair my ability to participate in varsity athletics, or be detrimental to my health and safety, or that of fellow participants. _______ (Initial Here) Health Insurance Coverage: · I agree to provide the Fisher College Sports Medicine team with proof of insurance prior to commencing any conditioning, training, and/or participation in varsity athletics. I understand that it is solely my responsibility to inform the Fisher College Sports Medicine team of any change in my insurance policy or coverage. I acknowledge that my failure to do so will result in termination of 4 my participation privileges. · I understand that if I sustain an injury while participating in Fisher College Varsity Athletics, any expenses not covered by my primary insurance company may be covered by an excess insurance policy provided by the college only after the primary insurance deductible has been fulfilled and the $50 per injury deductible for the excess insurance has been met. I further understand I must provide Fisher College with the proper documentation demonstrating that the deductible has been met and/or surpassed to initiate the process of additional coverage of medical expenses by the secondary insurance policy. _______ (Initial Here) Student Risk Sharing and Indemnification Agreement: In consideration for the College permitting me to engage in these sports, which permission the College is not otherwise required to grant, I hereby release Fisher College, its Board of Trustees, officers, agents, employees, volunteers, servants, consultants, affiliates, representatives, successors and assignees from any and all liability arising from any injuries or illness to me, including death and serious bodily injury, which in any way results from my participation in these sports while I am enrolled in or otherwise attending or present at Fisher College. Accordingly, I understand that Fisher College will not be responsible for any of my medical expenses, pain or suffering, present or future lost wages or diminished earning capacity, or any other damages to my person or property, which may result from injuries or illness, including serious bodily injury or death, I may sustain while participating in any way in these sports. This waiver shall not apply to losses and injuries resulting exclusively from the negligence of the College or its agents. I HAVE BEEN PROVIDED AN OPPORTUNITY TO ASK QUESTIONS CONCERNING THE TERMS AND CONDITIONS OF THIS STUDENT RISK SHARING AND INDEMNIFICATION AGREEMENT. I HAVE READ THE TERMS OF THIS STUDENT RISK SHARING AND INDEMNIFICATION AGREEMENT AND AM SIGNING IT FREELY AND VOLUNTARILY WITH FULL UNDERSTANDING OF ITS TERMS AND CONDITIONS. I understand that playing, practicing, training, or any other involvement in sports activity can be dangerous involving many RISKS OF INJURY, including but not limited to death, serious neck and spinal injury which may result in complete or partial paralysis or brain damage, serious injury to virtually all bones, joints, ligaments, muscles, tendons, and other aspects of the musculoskeletal system, and serious injury or impairment to other aspects of my body, general health and well-being, mobility, functionality, and overall enjoyment of life. I understand that any improper use or abuse of equipment could result in serious injury to me, my teammates, and/or my opponents. I understand that the use of equipment helps only to minimize the risk of injury and no equipment can prevent all injuries, which I might receive while participating in Fisher College varsity athletics. I recognize the importance of following procedures, policies, guidelines, instructions, and proper technique concerning my participation in these sports due to the inherent dangers of participating in these sports. The risk of injury to myself or others may be increased due to my failure to follow procedures, policies, guidelines, instructions, and proper technique. ________ (Initial Here) _______________________________________________ (Student Signature) ____________ (Date) If student is under 18 years of age, parent or legal guardian must complete the following section. _______________________________________________ (Parent or Legal Guardian Print Name) _______________________________________________ (Parent or Legal Guardian Signature) ____________ (Date) 5