Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
i
The Recruitment and Retention of a Care
Workforce for Older People
Jill Rubery, Gail Hebson, Damian Grimshaw, Marilyn Carroll,
Liz Smith, Lorrie Marchington and Sebastian Ugarte
February 2011
European Work and Employment Research Centre (EWERC)
University of Manchester
Project funded by the Department of Health as part of
the Social Care Workforce Initiative
Disclaimer
This is an independent report commissioned and funded by the Policy Research Programme
in the Department of Health. The views expressed are not necessarily those of the
Department.
EWERC
i
Acknowledgments
This report is based on the final two years of a University of Manchester research project on
the recruitment and retention of the social care workforce for older people under the
Department of Health‟s Social Care Workforce Initiative undertaken by a team based in the
European Work and Employment Research Centre in Manchester Business School. The
results of the first year of the project were reported on separately by the Manchester PSSRU
unit in 2009.
We are grateful to the Department of Heath for funding this project, while the usual
disclaimer applies (see above). We would also like to thank the academic coordinator of the
initiative, Hazel Qureshi, for her support and guidance over the course of the project. We are
extremely grateful for the time taken by the participants in this research project to provide us
with the data without which the report could not have been written. The participants ranged
from local authority commissioners and contract managers, to independent sector providers
(owners and managers), human resource managers of national chains and nearly 100 care
workers. The project has also benefitted from the active participation of members of our
advisory board, whose names are listed below. We are particularly grateful to Mary Murphy
for facilitating the setting up of a focus group of users and to Dan O‟Donoghue for
facilitating the piloting of our telephone questionnaire. Over the course of this project a
number of researchers have been involved in this project in addition to those named on the
report; these include Colette Fagan, Carrie Hunt and Claire Shepherd, and we would like to
record our thanks to them.
Members of the Project Advisory Board
EWERC
Name
Position/Organisation
Ged Taylor
Mary Murphy
Judy Scott
Sharon Brearley
Peter Urwin/ Ray Short
Michael Wyatt
Dan O‟Donoghue
Sue George
Gillian McCormack
Chris Hopwood
Consultant
Lay Person
Lay person
Age Concern
Unison
St Helens Council
Home Care Support
Skills for Care
Skills for Care
ACAS
ii
Table of Contents
Part/Section
Page
I. The study context
1
I.1. The research framework
1
I.2. The impact of external environmental factors on recruitment and retention
I.2.1. Policy environment
I.2.2. Commissioning and contracting practices of LAs
I.2.3. Labour market conditions
4
4
7
15
I.3. Management and organisational factors in the recruitment and retention of
a social care workforce
I.3.1. Management and human resource practices
I.3.2. Reward practices
I.3.3. The organisation of care work
I.3.4. Training and development
19
I.4. Recruitment and retention from the user and employee perspectives
I.4.1.What makes a good care service and what makes a good care
worker?
I.4.2. Is care work a good job or a bad job? The employee perspective
I.4.3. Time and space in the recruitment and retention of a social care
workforce
36
36
I.5. Key research questions
42
I.6. Research strategy and methodology
I.6.1. The project research stages
I.6.2 The first stage survey
45
45
48
I.7. The research methods for stage two
I.7.1. The local authorities
I.7.2 The telephone survey
49
49
53
I.8 The research methods for stage 3 case studies
I.8.1 Rationale for the case study approach
I.8.2. Stage three: design of the case studies
I.8.3. Stage three: selection, conduct and analysis of the case studies
58
58
58
60
I.9 The plan of the report
64
EWERC
19
22
28
34
38
41
iii
II. Commissioning and Contracting in the Selected Local Authorities
65
II.1. Key commissioning and contracting characteristics
II.1.1. Extent and form of external commissioning and contracting
II.1.2. Provision of fees for externally provided care
II.1.3. Role of HR factors in tendering, contracting and monitoring
II.1.4. Extent of support for providers through forums and training
provision
65
65
72
78
80
II.2. Approaches to commissioning and contracting: the qualitative interview
data
II.2.1. Making the market
II.2.2. Price versus quality.
II.2.3. Integration of social care and health
II.2.4. User choice
83
84
91
96
98
II.3. Classifying the strategic approach
102
II.3.1. Typologising the local authorities
102
II.3.2.The coherence, stability and sustainability of LAs‟ commissioning 110
and contracting practices
II.4 The selected LAs and user satisfaction surveys
113
II.5 Summary and conclusions
116
III. The provider telephone survey: Recruitment, retention and employment
conditions
118
III.1. Recruitment and selection
III.1.1. Recruitment difficulties
III.1.2. Recruitment practices: Attracting a suitable pool of applicants
III.1.3. Selection: Choosing the right applicant
III.1.4. Selection problems
120
120
124
129
134
III.2. Turnover and retention
III.2.1. Staff turnover
138
138
III.3. Pay and rewards
III.3.1. Level of pay
III.3.2. Pay differentials and pay supplements
III.3.3. Pay uprating
III.3.4. Payment for travel time, overtime and training time
III.3.5. Payment for upfront costs of starting work
143
143
147
150
152
155
III.4. Flexibility, Working Time and Work Organisation
III.4.1. Flexibility, working time arrangements and work organisation in
domiciliary care.
157
157
EWERC
iv
III.4.2. Flexibility, working time arrangements and work organisation in
care homes
173
III.5. Employee development and training
III.5.1. Induction of new staff
III.5.2. Training
III.5.3. Appraisal and staff development
177
177
178
184
III.6. Performance management, job autonomy and employee voice
III.6.1. Performance management
III.6.2. Discretion and autonomy
III.6.3. Employee voice and communication
186
186
191
193
III.7. Summary
195
IV. The impact of organisational, commissioning and labour market factors on
HR practices and outcomes
199
IV.1. Organisational characteristics and the management of independent sector
providers
IV.1.1. Organisational characteristics
IV.1.2. Management in the independent sector
200
IV.2 HR practices and outcomes by provider characteristics
IV.2.1. HR practices and outcomes by provider characteristics
IV.2.2. HR outcomes by provider characteristics
IV.2.3. HR practices and strategies by individual provider
IV.2.4. Employer views on the effectiveness of HR strategies
213
214
223
228
230
IV.3. LA commissioning and contracting and provider HR practices
IV.3.1. The influence of LA fee levels on pay
IV.3.2. HR practices and outcomes by type of LA
233
233
237
IV.4. Labour market conditions and provider HR practices and outcomes
IV.4.1. The influence of local labour market conditions on pay
IV.4.2. The influence of local labour market conditions on HR practices
and outcomes
246
246
247
IV.5. Internal and external environmental factors associated with good HR
practices and HR outcomes
IV.5.1. Exploring the factors associated with the adoption of good HR
practices
IV.5.2. Exploring the factors associated with good HR outcomes
253
IV.6. Providers‟ views on the social care policy and commissioning
environment
IV.6.1. Providers‟ attitudes towards and experiences of local authorities
IV.6.2. Providers‟ attitudes towards and experiences of monitoring
systems
267
EWERC
200
205
253
259
267
273
v
IV.6.3. Providers‟ attitudes towards, and experiences of, policy
developments likely to affect social care
IV.7. Summary
280
283
V. Recruitment and Retention in the Care Sector: A Case Study Approach
289
V.1. Case studies in four local authorities: exploring the impact of
commissioning and contracting arrangements
V.1.1 Introducing the local authorities
V.1.2. Pay practices of providers by local authority.
V.1.3. Working time practices of providers by local authority
V.1.4. Work organisation of providers by local authority
V.1.5. Training and development of providers by local authority
V.1.6. Comparing national providers in different LA environments.
V.1.7. Overview of HR outcomes for providers by local authority
291
V.2. Care workers‟ perspectives on recruitment
V.2.1 Factors that influence entry into the care sector
V.2.2. Role of employers versus employees in access to information on
care job vacancies
300
303
309
V.3. Care workers‟ perspectives on turnover and retention
V.3.1. Care workers‟ intentions to stay or to quit.
V.3.2. Factors that may contribute to turnover
313
313
318
V.4. Care workers‟ perspective on pay and working time
V.4.1 Pay and travel time
V.4.2 Working time
321
321
325
V.5. Care workers‟ perspective on work organisation and the quality of care
330
V.6. Care workers‟ perspectives on training and development
V.6.1 Experiences of training
V.6.2 Development and opportunities training
337
337
340
V.7 Summary and conclusions
344
VI. Research Findings and Conclusions
347
291
293
294
295
297
298
300
VI.1. The local authority commissioning environment
347
VI.2. Explaining the variety of HR policies and HR outcomes of providers
352
VI.3. Recruitment and retention from a care worker and user perspective
362
VI.4. Prospects for recruitment and retention under expanding demand: the
policy issues
366
Appendix
376
Bibliography
419
EWERC
vi
List of abbreviations
ADSS
CIPD
CQC
CRB
GMB
HR
IDP
KPI
LA
LADP
LPC
MaROT
R2
Association of the Directors of Social Services
Chartered Institute of Personnel and Development
Care Quality Commission
Criminal Records Bureau
GMB Trade Union
Human resource
Independent sector domiciliary care provider
Key performance indicator
Local authority
Local authority domiciliary care provider
Low Pay Commission
Management of recruitment and retention, reward policy, organisation of work
and training and development
National Health Serivce
National Minimum Data Set
National Vocational Qualification
Primary Care Trust
The policy environment, commissioning practices of local authorities, and
labour supply factors
Coefficient of determination of a linear regression
R&R
Sig.
TUPE
UKHCA
Recruitment and retention
Significant ( statistical)
Transfer of Undertakings Protection of Employment
UK Home Care Association
NHS
NMDS
NVQ
PCT
PoCLS
EWERC
vii
Notes on coding used through the report
We have used a number of coding systems to provide identifier throughout the report. The 14
local authorities have been given a two letter identifier. This has been used as the first part of
the identifier for the providers interviewed in the telephone survey. After the LA identifier we
use the codes D, H and IH to signify domiciliary, homes or inhouse (LA) provider. The first
number indicates whether they are the first, second, etc; domiciliary provider or home
interviewed in the LA. Other codes have been added to facilitate identification by the
research team of the key characteristics of the provider, but readers may ignore them. In part
V we provide a simplified coding structure for the case study providers and the
correspondence between the two sets of codes is outlined in appendix table V.A1.
Variable codes used in part IV are fully explained in the appendix to part IV.
EWERC
Part I. The study context
1
I. The Study Context
I.1. The research framework
The overall aim of the project is to contribute to the debate on how to recruit and retain a
social care workforce for older adults to meet current and future needs. The specific focus is
on care assistants and on care for older adults. Improvements in recruitment and retention are
critical to enhancing the quality and the availability of care staff, an objective which has been
a long standing policy concern (Cm 4683 1971, Cm 6233 1975). Its importance for policy
has increased as a consequence of the policy emphasis on the provision of care for vulnerable
older people both in their own homes and in care homes (Cm 849 1989). The research project
also responds to an increasing policy focus on quality in domiciliary and residential care
(Department of Health 2000), particularly as perceived by users and carers (Nocon and
Qureshi 1996, Department of Health 2009), and on the regulation of these care sectors
(Department of Health 2000, 2003a, 2003b).
The focus of the research is on the recruitment and retention of care workers in the
independent private and voluntary sectors. The shift from local authorities (LAs) to
independent providers of care, particularly from 1993 onwards, has diminished our
knowledge of the context for recruitment and retention due to the much larger variety of
organisations providing care, the diversity of organisational approaches to HR policy and
practice and the important new role of LA commissioning arrangements.
The starting hypothesis for our project was that the recruitment and retention of the
workforce would be influenced by the environment in which the providers operate – namely
the policy and commissioning environment and the labour supply conditions – and by the
policies and practices of the independent sector providers. Recruitment and retention is also
influenced by the experiences and aspirations of the workforce and an additional emphasis in
our research is to include employee experiences and voice in understanding the current
context. The project design did not allow for extensive engagement with users‟ perceptions of
care quality and the links between their perceptions and quality HR polices. However, as
chapter two makes clear, we have aimed to include user perspectives in survey design and
analysis wherever possible. Also, as the project was designed in 2004, the potential role of
personalised budgets in shaping future patterns of recruitment and retention is only
considered to a limited extent. However, recent policy favouring the development of
individual budget arrangements (Department of Health 2008) makes it even more important
to gather information on the problems of sustaining and developing a social care workforce in
a context of potentially even more fragmented employment arrangements.
EWERC
Part I. The study context
2
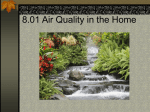
Figure I.1 sets out the overall framework that we have used for understanding the influences
on the recruitment and retention of the social care workforce. The figure depicts first of all
the key external environmental factors (PoCLS) including:
the Policy environment (central government and devolved government policy);
Commissioning practices of local authorities, including inhouse arrangements and
purchaser-provider relations; and
Labour Supply factors, including local market conditions, changing gender relations
and the structure of the care labour market.
We have elaborated the central government policy agendas to include not only the direct
relationships between central government and LAs in the form of budget setting and policies
with respect to care arrangements but also government policy towards the NHS and personal
budgets, thereby bringing the users directly into the picture. A second set of influences on
recruitment and retention are depicted by the role of independent providers in shaping the
conditions of work within the organisation (MaROT), including:
Management of recruitment and retention, including the use of „high performance
bundles‟ of HR practices, and mechanisms for employee voice;
Reward policy, including pay rates, pay premiums and travel pay, and particularly in
relation to part-time work and women returners;
Organisation of work, including the nature of care work, the pace and timing of work,
the skill content and scope for autonomy and discretion; and
Training and development, including formal training provision and the effects of
regulatory standards.
The experiences and aspirations of the care workforce are influenced by the commissioning
and provider policies in social care but also by the general labour market conditions and by
their own experiences of both work and care, both inside and outside the labour market. The
users are shown as having a potentially more active role in the future in both employing the
workforce directly and by using brokers or independent sector domiciliary providers, with or
without LA involvement to commission services.
This figure provides the framework for this review of current literature and knowledge. We
start in section I.2 with the external environment factors that impact on the recruitment and
retention of social care staff including policy, commissioning and labour supply conditions
(PoCLS). This section is informed by government policy documents and academic research
literature but also by the results from a survey of all Local Authorities in England involved in
commissioning social care (sample number 149, achieved sample of 90) conducted as the
first stage of this project but reported separately by the PSSRU research team that had
responsibility for this stage (Hughes et al. 2009). Section I.3 discusses the key organisational
factors (MaROT) likely to impact on recruitment and retention with sections on the
management of provider institutions and approaches to quality care standards, on resourcing
and reward policies, and on the organisation of work and the approach to training and
development. Section I.4 considers recruitment and retention from users‟ and employees‟
EWERC
Part I. The study context
3
perspectives. Here we focus on what we know about user perspectives on care quality,
namely what makes both a good care worker and a good care service. We then consider the
literature on what makes a good and a bad job from an employee perspective, focusing
particularly on the literature on care work and on low paid work. Drawing on this literature
review, section I.5 identifies the key research questions for the project and the methods
adopted to investigate these questions are outlined in sections I.6 to I.8.
Figure I.1. Framework of influences on the recruitment and retention of care workers
Policy environment
Commissioning practices
NHS
INDEPENDENTSECTOR PROVIDERS
Management,Rewards,
Organisation of work, Training )
SOCIAL CARE WORKFORCE
Personal
budgets
EWERC
USERS/ QUALITY OF CARE
Labour
supply
Personal
and family
experience
Part I. The study context
4
I.2. The impact of external environmental factors on recruitment
and retention
Figure I.1 above identifies three key external influences (PoCLS) on the recruitment and
retention of the social care workforce for older adults: the Policy environment, the
Commissioning practices of local authorities and Labour Supply factors. We review each in
turn in the following discussion.
I.2.1. Policy environment
The policy environment for social care for older adults is first of all informed by social needs.
Three main factors are increasing the need for social care: the ageing population and
increased life expectancy; the associated need to reduce costs of healthcare for older adults by
speeding up hospital discharge; and the decline in availability of unpaid carers due to changes
in women‟s roles and the trend towards single independent living for the elderly. This general
policy environment which applies across the developed world means that social care is and
will remain a critical area for welfare state policy. A fourth key policy issue is the increasing
demands from users to have greater control over their care arrangements. This is leading to
policies to make care more user-centred and for care commissioning to be assessed not only
on cost but also on quality outcomes as perceived by users.
While this policy context raises a very wide range of issues, including how care should be
funded and the like, our prime concern is with those questions which impact upon the
employment environment for the social care workforce. Of particular salience here are
policies which have an impact upon who employs the social care workforce, under what
conditions and for what types of work. Three main policy developments can be highlighted:
the development of commissioning and contracting to the independent sector; the integration
of health and social care and the current policy of devolving budgets to care users.
Commissioning and contracting to the independent sector: government sets the
policy environment
The foundations for the current high levels of commissioning and contracting to the
independent sector were laid by the 1989 White Paper, Caring for People, which required
LAs to promote „the development of a flourishing independent sector alongside good quality
public services‟. In 1993 the roles of purchaser/commissioner and providers were formally
separated (Department of Health 1990) and the 1998 White Paper required LAs „to plan,
commission, purchase and monitor an adequate supply of appropriate, cost effective and safe
social care provision for those eligible for local authority support‟ (Cm 4169 1998: 111).
Around the same time the Labour government decided to replace compulsory competitive
tendering with Best Value (Cm 4014 1998). In doing so it also decreed that it had „no
preconception about whether the public or the voluntary or private sector should be the
EWERC
Part I. The study context
5
preferred providers‟ (Cm 4169 1998: 119). Instead the mix of providers was to be
determined by the outcome of Best Value commissioning and contracting. Local Authorities
have also been under pressure to increase efficiency in their procurement policies as a
consequence of the Gershon (2004) review of public sector efficiency. Further pressure for
efficiency in procurement has come from a relatively tight budget settlement for social care,
certainly in comparison to health. A recent report from the House of Commons Health
Committee notes that overall gross expenditure on adult personal social services increased by
57.4% in real terms between 1997–98 and 2007–08 but spending on the NHS doubled in the
same period (House of Commons 2010). Furthermore, central government grants to LAs only
increased by 48% in real terms over the same time period. The impact of this environment on
the commissioning and contracting practices of LAs is explored further in section I.2.2.
Integrating health and social care
Coordination and integration of health and social care services to older people became a
major element of government policy after new Labour made a manifesto commitment in
1997 to bring down the so-called Berlin wall between health and social care. The range of
initiatives since then to promote joint commissioning are outlined in box 1.1. These include
the specification under Best Value that there should be an integrated review of health and
social care. Nevertheless, it is still the case that in most LAs only a minority of social care
services are jointly commissioned. According to this project‟s first stage survey conducted in
2007-8 (Hughes et al. 2009), 77% of LAs were engaged in some joint commissioning and
45% pooled some ring fenced monies but two thirds of LAs said that under 20% of services
were jointly commissioned. A small minority of LAs undertake all their commissioning with
the NHS (5%) and a similar share (7%) pool all their budgets for adult social care with the
NHS.
Although integration of health and social care is claimed to have positive benefits for
reducing waste and promoting better quality services through joined up government, some
research has questioned whether these benefits are automatic. The key concern is that the
NHS tends to be the dominant partner and may use integration primarily to reduce pressures
on the NHS by facilitating early discharge from hospital. This approach may not serve the
interests of those older people who are not recent or prospective admissions to the health
service (Glendinning et al. 2002, Lewis 2001). Too great a focus on early discharge may
distract attention from the other long term cost reduction strategy - that of keeping more older
people in their own homes and reducing admissions to residential homes of people able to
live in their own homes or in extra care facilities (see Challis and Hughes (2002) for evidence
of „too high‟ admission to residential homes). A further concern is whether re-ablement
services will be primarily used to help people return to their own homes after hospital and not
be used to help prevent admissions to homes where the person has not been a hospital
admission (Glendinning et al. 2002). Moreover, research suggests that integration has so far
been rather limited and that without more radical institutional changes such as the integration
of the health and social care information systems significant benefits may not be realisable
(Brown et al. 2003). Hudson (2002), however, found that even where cooperation across
EWERC
Part I. The study context
6
boundaries was limited it was yielding positive benefits in collaboration across traditional
hierarchical and professional divides.
Box 1.1. Initiatives to promote joint commissioning
Pooled budgets: where health and social services put a proportion of their funds into a
mutually accessible joint budget to enable more integrated care.
Lead commissioning: where one authority transfers funds to the other who will then take
responsibility for purchasing both health and social care.
Integrated provision: where one organisation provides both health and social care.
Introduction of practice based commissioning.
Creation of Care Trusts: to commission and deliver primary and community health and
social care for older people and other user groups.
Duty of partnership: local health and social care planners to achieve both national
standards and local milestones.
Local Strategic Partnerships: councils to work with other local agencies to improve
economic, social and environmental well being followed by the introduction of Local Area
Agreements to facilitate the work of government, local authority and its partners by
agreeing the design and delivery of outcome targets which reflect national and local
priorities.
The introduction of national service frameworks, in partnership with the NHS: to create a
greater level of consistency and fairness in social care.
Requirement for Primary Care Trusts and local authorities to produce a joint strategic
needs assessment of the health and well being of its local community.
Streamline budgets and planning cycles between Primary Care Trusts and local authorities,
based on a shared, outcome-based performance framework.
Sources: adapted from Hughes et al. (2009: box 1.4).
Implementing personal budgets
Currently LAs have main responsibility for commissioning social care services for older
adults. However, since the 2005 Green Paper, Independence, Well Being and Choice, the
government has committed to allow all users to have a personal budget to enable them to
commission and organise their own care arrangements. This has coincided with a renewed
commitment in the 2006 White Paper, Our Health, Our Care, Our Say (Cm 6737 2006), to
increase the use of direct payments to users which started in 1997. These changes introduce
considerable uncertainty into the system as they could in principle significantly reduce the
role of LAs in managing the social care provision and the social care market. It is not only the
likely extent of take-up of personal budgets that is unclear but also their impact on both LAs
and current independent sector providers is unknown. The evaluation of pilot programmes for
individual budgets did find that older adults were more likely to see the additional
responsibilities that come with managing individual budgets as a burden (Glendinning et al.
2008a), suggesting a possible lower take-up than anticipated. These concerns may also
suggest a continuing need for LA involvement in brokering services for individual budget
holders. Other researchers have raised concerns over potential conflicts, for example between
EWERC
Part I. The study context
7
the choice policy agenda and the safeguarding of vulnerable adults (Manthorpe et al. 2008)
and between choice and the organisation of services to reduce travel times by appointing only
one provider to a particular area (Glendinning et al 2008b). The same research also indicates
that the independent sector providers are concerned about a number of new risks, such as late
or non payment for services and poaching of care staff by users, particularly if they pay
higher wages. However, the risk that a user who was also the employer may only be able to
offer short and uncertain employment may enable agencies to retain their staff. The
independent sector providers also face a further uncertainly that although they need to
develop a wider range of services to meet the more diverse priorities of individual budget
holders, the new services would not be available to all users if only a minority take up the
individual budget option.
I.2.2. Commissioning and contracting practices of LAs
The change in the primary LA role: from direct providers to commissioners
Since the 1989 White Paper, Caring for People (Cm 849 1989), LAs have moved from being
the primary providers of social care services to being enablers and commissioners of social
care services. This change in role has been progressive but has accelerated at certain key
periods. Furthermore the extent and pace of outsourcing has varied between LAs. Withdrawal
from residential care came first in most cases. The first stage survey for this project reports
that three fifths of LAs had moved the majority of their residential care into the independent
sector before 2000, 17% having done so even before 1993 (Hughes et al. 2009).
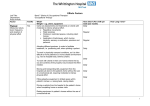
Figure I.2 displays the rapid expansion of private beds in England throughout the 1980s.
Total provision plateaued and then declined from the early 1990s, while public sector
residential care continued to fall. Figure I.3, also drawing on Knapp et al. (2001), shows that
the overall drop in residential places was in part the result of a shift to domiciliary care
LA withdrawal from domiciliary care came next. Only a quarter of LAs (26%) in this
project‟s first stage survey (Hughes et al. 2009) reported they had moved the majority of their
domiciliary care into the independent sector before 1999. But the pace of externalisation
accelerated in the 2000s so that by 2004 three quarters (77%) of LAs used the independent
sector for the majority of domiciliary care. By 2008 less than one in ten LAs (7%) had 60%
or more of domiciliary care provided by inhouse staff. By comparison, close to one fifth of
LAs (17%) still retained the majority of residential care inhouse. Overall then, with respect to
both types of care services, the majority of LAs by 2008 had become primarily reliant on the
independent sector for their social care provision for older adults.
EWERC
Part I. The study context
8
Figure I.2. Residential care places for elderly people in the public and private/voluntary
sectors, England 1980-1998
Source Knapp et al. (2001: figure 3)
Figure I.3. Residential and domiciliary care trends, England 1993-1997
Source Knapp et al. (2001: figure 4).
EWERC
Part I. The study context
9
To explore the impact of these developments we first consider what previous studies have
revealed with respect to the role of LAs in developing the independent sector market through
commissioning, contracting, monitoring, regulating and other forms of engagement and
consultation. These activities in „developing the market‟ have to be understood in the general
context of public sector procurement and public sector budgets. Thus the second topic we
review is how the general budgeting and commissioning environment, characterised by Best
Value principles, on the one hand, and the continuing and intensifying budget pressure, on
the other, has influenced the development of commissioning and contracting for social care.
Developing the market
The making of the market for social care through commissioning, contracting and
engagement involves a number of elements or stages. First, there is an evolving division of
labour or specialisms between the remaining inhouse and externalised activities. This may be
a dynamic relationship as priorities change. In some cases inhouse facilities may be at the
forefront of new initiatives and innovation - for example, in extra care or re-ablement - but in
other cases LAs may look to the independent sector for new ways of working and innovation.
Drake and Davies (2006) in fact identify six different strategies used by LAs, including
outsourcing most domiciliary care but providing specialist services inhouse (primarily reablement), providing the full range of services using both inhouse and external providers and
using outsourcing only as means of topping up inhouse services.1
Evidence from the first stage survey suggests there is now a high level of specialisation in the
inhouse departments. For intermediate care, more than four fifths of LAs use inhouse staff
and less than two fifths use independent sector staff. In comparison, for community care
nearly all LAs use independent sector staff and less than three fifths use inhouse staff. Mental
health care was a more equally shared activity with nearly three fifths of LAs using inhouse
staff and four fifths using independent sector staff. Given the increasing focus on re-ablement
as the route to long-term policy goals such as reducing the share of older adults who are
unable to stay in their own homes, the remaining LA inhouse departments are in an important
strategic position to maintain and/or increase their importance within the older adults care
services. Indeed Drake and Davies report LAs explaining their decision to keep these skills
inhouse in order to retain core skills that are „mission critical‟ (2006: 185). Thus there could
even be a reverse dynamic of increasing the role played by the inhouse departments.
However, some LAs have already outsourced their re-ablement as well as their community
care work. An important issue for research is the extent to which these different governance
models promote or hinder the development of a re-ablement service. Drake and Davies
(2006) demonstrate that while some LAs may have outsourced specialist care simply because
they no longer have inhouse capacities, others exhibit a policy of outsourcing both high and
1
One LA in the Drake and Davies (2006) study that had used the top-up model reported problems that the
independent providers were able to push up their prices when they knew the only reason for the outsourcing was
the exhaustion of in house capacities.
EWERC
Part I. The study context
10
low skill activities to independent providers - as well as maintaining some inhouse - in order
„to give independent providers the professional integrity to provide specialist services if they
can.‟ (Drake and Davies 2006: 185). In some areas of care –for example smart housing and
xtra care - there is clearly some reliance on partnerships with private or voluntary sector
companies for developing new ways of delivering care. However, there appears to be no
research on whether external providers have engaged in innovative activities related to the
actual delivery of home care or residential services. As external providers are still
infrequently engaged in the assessment and design of care packages (Hughes et al. 2009) it
seems unlikely that they have played a major role in innovation in ways of delivering care or
new ways of working.
A second concern for LAs is to secure an adequate supply of providers; this follows the
requirement in the 1989 Act to ensure a flourishing supply, but is of critical concern where
LAs dominate the social care market, particularly that for domiciliary care but also for
residential care in areas where most beds are funded by the LA. The supply of providers
depends on a host of factors, including:
the overall price or fee level;
the security of work flows and/or fee income;
the availability of information;
undertakings that enable providers to plan their work loads and their staffing policies;
and any hidden or additional costs that are not compensated for (that is the risk
involved in contracting at a given price).
LAs are also expected to take into account the need to foster local and diverse providers to
meet the needs of specific groups and ensure effective choice. This fits with the national
procurement strategy for LAs, which requires them to „confidently operate a mixed economy
of service provision, with ready access to a diverse, competitive range of suppliers providing
quality services, including small firms, social enterprises, minority businesses and voluntary
and community sector groups‟ (ODPM/LGA, 2003 quoted in Hughes et al, 2009: Box 1.10).
However, there may be conflicts between, on the one hand, the provision of security and
planning and the requirement to promote small providers and diverse providers and, on the
other, the requirement to use competition between suppliers to increase public services
responsiveness and efficiency (Kirkpatrick 1999). Furthermore both the LAs and the
Department of Health retain ultimate responsibility for the delivery of care to vulnerable
adults and for ensuring its quality. Although to meet these responsibilities a regulatory regime
external to both LAs and the independent providers has been set up, LAs still assume some
responsibility for ensuring that aspects of the quality agenda can be delivered, ranging from
ensuring continuity of care to ensuring that training is available to independent sector staff.
With respect to securing an adequate supply of care homes, a number of studies in the 1990s
and early 2000s investigated the reasons for home closures. Two studies attribute the closures
to a combination of LAs paying low fees or not raising them in line with an increase in high
dependency residents, coupled with the costs of complying with new national care standards
(Darton et al. 2003, Netten et al. 2003). Most homes closing were small so that overheads
EWERC
Part I. The study context
11
were high relative to fees but the quality of care provided had been of a high standard. In a
subsequent study, Netten et al (2005) report that fear of an undersupply of care beds, with
implications for hospital discharges, led the government „to retreat on the standards and to
increase funding to local authorities‟ (op.cit: 319). Andrews and Phillips (2000) argue the
long-term outcome of the trend towards both higher dependency and lower residential care
fees will be increasing concentration in the sector (that is, a smaller number of very large
providers) contrary to the apparent policy goal of diversity and choice.
With respect to contracting for residential care the Audit Commission (1997 quoted in
Kendall 2001) recommended a greater use of longer term contracts to foster better working
relations and information flows as well as assisting residential homes providers to engage in
longer term planning. Research also emphasises the need for better information flows
between LAs and independent care homes (Matosevic et al. 2007, 2008). Relatedly, Knapp et
al. (2001) argue that, „Complaints are legion from independent providers about poor
matching of users to services, poor signalling of purchasing intentions and priorities‟ (op.cit:
302). Filinson (1998) also found that most residential home providers did not participate in
the planning of social care. Changes to contracting arrangements are not necessarily the
answer: three quarters of LAs have some block contracting but the share of beds contracted
was below 10% in nearly 50% of cases) (Hughes et al. 2009: table 3.39). However this block
contracting to larger homes has been identified as a factor in the closure of smaller homes
(Netten et al.2003). Moreover, Kendall‟s (2001) research casts doubt on the Audit
Commission‟s view that providers of residential care would welcome more block contracting
as residential home owners were concerned to maintain a balanced client base between LA
contracted and private clients, thereby reducing LA control over their operation. Matosevic et
al. (2008) also suggest that LAs tend to ascribe more purely financial motivations to care
home providers than the care home providers themselves reveal in parallel questionnaires,
suggesting a need for new practices that can develop trusting relations between providers and
LAs.
Very similar issues emerge in relation to developing the supply of domiciliary care providers,
although this market has developed more recently; a survey of providers in 1999 found that
two thirds (64%) had been established during or since 1993 (Ware et al. 2001). The same
study also found that LAs were at different stages in the development of the market with
some still seeking sufficient providers to cover the market while others had already
developed a sufficient supply and were now in a position to start to work closely with
„selected and proven providers‟(op.cit.: 340). The first stage survey for this project found a
relatively high level of satisfaction among LAs with the number of potential providers; three
in four LAs reported the number of responses to their tender was „about right‟ and only 17%
and 7% stated the number was too few or too many, respectively.
With respect to contracting for domiciliary care services, most published research points to
the development of larger block contracts that tend to squeeze out the smaller providers
(Ware et al. 2001, Drake and Davies 2006). In response, some LAs are reported as willing to
pay higher fees to smaller local providers to ensure diversity of supply, despite potential
ethical and legal problems of favouring local providers in procurement (Drake and Davies
EWERC
Part I. The study context
12
2006). Our first stage survey in fact suggests strong polarisation between LAs with two fifths
(39%) recording no block contracts and a similar proportion (37%) using block contracts for
three fifths or more of their total expenditure on domiciliary care with the independent sector.
However, this division between LAs is likely to change. LAs appear to be moving towards an
intermediate category of preferred providers, in part in response to the personal care agenda
(see section II.2 below).
In addition to securing a reliable supply of providers, LAs have a responsibility to promote
competition between providers. Several studies test the assumption that greater competition
encourages improved responsiveness to user needs. For example, Lewis et al. (1996) find that
care services had become more responsive (measured by the likelihood of a user being put to
bed at a time they prefer) in several LAs following the purchaser/provider split but that it was
too simplistic to attribute this simply to competition. In some LAs it was in fact inhouse
provision that had become more responsive, and in at least one case this resulted from
devolution of budgets to care managers rather than competition per se (op. cit.). Drake and
Davies (2006) comment that block contracting involves fierce competition only at the point
of the contract award, whereas spot contracting encourages continuous competition. They
also point to the danger that large contracts may lead to concentration and a shift of power
back from consumers to independent providers. Nevertheless when LAs seek a step increase
in outsourced provision they often resort to block contracting with large providers to achieve
cost reductions. Another incentive to contract with a small number of suppliers is to reduce
transaction costs (that is, the costs and time of designing and negotiating contracts)
particularly if LAs do not fix a standard price for services (op. cit.).
Effective competition as described in an economics textbook should involve multiple
providers and multiple purchasers. But on the purchasing side, LAs are in fact dominant
clients and may fix prices which providers have to accept or else risk losing the majority of
their business in the locality (Knapp et al. 2001). Fixed prices may also mean that care
services requiring different levels of skill are priced at the same level. Drake and Davies
(2006) report that some providers find it fair to have a fixed price but others argue the price
should reflect differences in costs such as training costs. Another issue is whether there is
only one or more providers for a geographical locality. Drake and Davies (2006) report at
least one LA making a decision to select more than one provider per area to prevent the
formation of monopolies.
Although the issue of quality standards has in part been taken over by national regulatory
standards and inspections provided by the Care Quality Commission, LAs still play a role in
monitoring and regulating standards in their independent providers and have scope to require
particular approaches to both quality of care and to the approach taken to the management of
staff in their tenders, contracts and monitoring procedures. The first stage survey found that
almost all LAs included some HR requirements in their tenders and contracts for both homes
and independent domiciliary providers – particularly related to induction training and training
achievements against national standards. Also, all LAs monitored domiciliary providers
throughout the contract period, with over four fifths monitoring staff development and
training and recruitment practices (Hughes et al. 2009: figure 3.14, tables 3.32-34 and 3.41).
EWERC
Part I. The study context
13
LAs are also involved in providing support to providers although research suggests there are
problems in information sharing (Wistow and Hardy 1999) and in developing long-term
trusting relations (Curtice and Fraser 2000, Ware et al. 2001), except with voluntary
providers in some areas. Provider forums have become more common (Ware et al. 2001) and
although on balance have been welcomed by providers they are also found to be highly
controlled with clear limits set to the flow of information. LAs also provide support for
training the independent sector workforce, even extending to some higher level skills such as
re-ablement when they have outsourced all their own provisions (Drake and Davies 2006).
However, there is also evidence that LA provision of training is strongly linked to availability
of funds to provide the training (Rainbird et al. 2009). Thus once the ringfenced monies for
training ended in 2004 there was a move to mobilise more general funds such as „Train for
Gain‟ and European Social Fund related monies. But once these alternative funds became
scarce problems of training provision have arisen (Rainbird et al. 2009, Rubery and Urwin
2010). Not all problems of training are attributable to lack of availability of courses or
funding for the training. There is evidence of reluctance on the part of independent providers
to train their staff (Balloch et al. 2004, Fleming and Taylor 2006), caused by both pressures
of workloads and costs. These reasons are in part also the result of the conditions under
which providers are contracted by LAs.
Price versus quality: an issue of budgets?
The increasing budget constraint faced by LAs in relation to social care is illustrated by the
growing gap between expenditures and central government funding. During the ten years
from 1997-98 and 2007-08, real expenditures on social care increased by 57% and central
government funding rose by just 48% (House of Commons 2010). Given the strong pressures
on demand for services, the tendency for commissioning strategies to increasingly rely on the
independent care sector is underpinned by the strong cost differences between inhouse and
external provision. Data from the NHS Information Centre for Health and Social Care show
that the average hourly cost of home care services in 2008 was £23.40 when provided
inhouse by LAs and only £13.00 when provided by other organisations. 2 Part of the cost
differential is accounted for by the more specialised services provided by inhouse LA care
workers but this is unlikely to account for the majority of the large cost difference.
In fact the cost difference reflects to a large extent the collectively negotiated terms and
conditions of employment for LA staff that deliver relatively high basic pay levels (Eborall
and Griffiths 2008), as well as more generous benefits and provisions for travel time and
unsocial hours payments. Pay and conditions in the private and voluntary sectors tend to be
determined unilaterally by management and are characterised by lower basic pay and non-pay
benefits typically set at the legal minima. One of the key questions for this research project is
to investigate the degree to which these conditions are the outcome of both LA
2
The average hourly cost was £15.20, indicating the dominance of the private sector in delivery. All data
accessed from the website http://www.ic.nhs.uk/statistics-and-data-collections/social-care/older-people.
EWERC
Part I. The study context
14
commissioning policies and the HR policies of provider organisations. We know that many
LAs fix the price for the service at tender. Figures vary, including an estimate of around two
thirds of LAs in the study by Forder et al. (2004), just over one third (36%) in our first stage
survey and around one third (32%) in a UKHCA survey (Mathew 2004: table 10). A fixed
price does not necessarily mean a low price; the UKHCA survey idenitifed one LA that
moved from variable to fixed prices and this led to considerable increases for providers that
had entered the market with low tender prices. Research suggests that LAs also operate with a
fixed price system for residential care, although there may be lower prices for block than spot
contracts (Forder and Netten 2000).
Research suggests that LA fees for both domiciliary and residential care have not always
risen in line with costs that providers are unable to avoid. These include:
statutory improvements to employment conditions – the National Minimum Wage
and the working time directive, including the recent extension of guaranteed holiday
entitlements (Andrews and Phillips 2002, Clarkson et al. 2005, Knapp et al. 2001,
Netten et al. 2003, Angel 2007); and
implementation of the National Minimum Care Standards - especially the additional
training costs to meet the 50% NVQ level 2 target and providing higher staffing ratios
in response to higher levels of dependency at the same price (Andrews and Phillips
2000, Darton et al. 2003, Forder and Netten 2000, Netten et al. 2005, Ware et al.
2001).
This accumulating evidence suggests LAs are requiring providers to do more for the same or
even lower prices. The likely outcome is reductions in quality of service or closure of
suppliers. Indeed, Netten et al. (2003) report that three quarters of homes that had closed
claimed LA fees were insufficient to cover their costs following the introduction of higher
care standards. This has particularly affected small homes and small domiciliary care
providers – a further factor promoting concentration in the sector.
Not all problems relate to basic fee levels. Many of the difficulties in covering costs are
associated with the absence of specific fees to cover travel costs or to provide sufficient time
for care delivery. In their study of users‟ perceptions of care services, Francis and Netten
(2004) point to the practice of not paying for travel between appointments and allowing
insufficient time for quality visits as a major perceived barrier to quality of care. Ware et al.
(2003) also comment that the increasing emphasis of LAs on procedure-based care
management subordinates personal relationships between care worker and user to short-term
task delivery, which, in their words, „may threaten patterns of trust and accountability‟ (op.
cit.: 411). A UKHCA survey (Mathew 2004: 37) found that while higher paying LAs were
the least likely to make any adjustment to their hourly fee to compensate for short visits
(thereby providing for more travel time payment), there were also examples of low paying
LAs that also failed to provide any enhanced fee for short visits.
The Best Value framework for commissioning services, along with the national minimum
care standards, are expected to establish a dual focus on quality and price. Drake and Davies
(2006) found some authorities that admitted to having been willing to use low quality
EWERC
Part I. The study context
15
services to meet excess demand before the passage of the Care Standards Act and the Best
Value regime. However, research also suggests that the Best Value regime has had less
impact on reducing cost pressures on commissioning practices than might be expected, in part
because of requirements for continuous improvements in public service efficiency of 2% per
annum (Cunningham 2008: 382). Cunningham‟s detailed study of the conditions facing
voluntary sector providers of social care suggests Best Value placed additional pressures on
providers to meet both higher quality employment standards and higher care standards
without any relief in cost pressures. Also, LA commissioning focused on improving quality
of care rather than quality of HR practices, with the main HR focus on compliance with
statutory regulations (including CRB checks and equal opportunities and disciplinary and
grievance practices) rather than developing high performance working (op. cit.). Aside from
LA commissioning, other important influences on HR practices in providers derive from the
Care Commission and its focus on training standards.
There is also no evidence that the Best Value regime has fostered long-term relationships
between LAs and independent providers, or contributed to greater stability in employment
relationships in the independent sector (Cunningham and James 2009). Kirkpatrick (1999)
has indeed questioned the feasibility of partnership arrangements between LAs and
independent providers, not only because of the low levels of trust within the sector and the
difficult of building trust but also because of the disconnect between a partnership agenda and
the requirement to „shop around‟ to achieve best value and continuous performance
improvements, and because of the need for probity in the management of public monies, with
strong trusting relationships leading to a risk, in the extreme case, of corruption.
Overall, the research suggests that Best Value may be seen as an additional requirement for
independent providers to meet at the same price. Instead of a move towards a quality
approach through partnership, quality has become a requirement of the competitive tendering
regime in social care. Furthermore where the quality standards are based primarily on care
standards, these may create some problems for HR standards, including the promotion of
employee-oriented flexible working.
I.2.3. Labour market conditions
The adult social care sector now employs around one million workers (Moriaty et al. 2008)
with 900,000 located in the private and voluntary sector. According to the Low Pay
Commission (2008) it is the third largest low-paying sector in the UK economy, with around
one million jobs being paid at or around the level of the minimum wage. Although local
labour market conditions vary across the country 2010 data from the National Minimum Data
Set (NMDS) for Social Care (see www.nmds-sc-online.org.uk/) show a remarkably narrow
range of variation in rates for care workers.
EWERC
Part I. The study context
16
For example, across the nine English regions, the wage at the 20th percentile3 only varies
from £5.73 in the North East (equal to the national minimum wage from October 2008September 2009) to £6.10 in the South East. If London, the South East and the South West the three highest paying regions - are excluded, then the range of variation is only 17p.
Likewise the range of median hourly pay rates varies by just 67p from the lowest in the North
East at £5.95 to the highest in the South East at £6.25; again, excluding the three highest
paying regions leads to a variation of just 50p (see table I.1).
Table I.1 Hourly pay for care workers by English region: 20th percentile and median
rates.
North East
North West
Yorkshire and Humberside
West Midlands
East Midlands
Eastern
South West
London
South East
20th Percentile
£5.73
£5.80
£5.80
£5.80
£5.80
£5.90
£6.00
£6.00
£6.10
Median
£5.95
£6.10
£6.15
£6.25
£6.30
£6.45
£6.55
£6.58
£6.62
Source NMDS online data (June 2010).
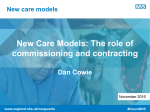
This range of pay rates does not reflect the range of variations in labour demand, as is
indicated for example by the strong regional differences in use of migrant workers. A study
by Experìan (2007) for Skills for Care found that over two thirds of care staff in London were
migrants (defined as „born abroad‟) compared to less than a fifth in seven out of nine regions
(figure I.4). Also, the low level of pay has not established a neat equilibrium of supply and
demand. For example, turnover rates are very high for care workers, running at around 22%
(NMDS 2010). Also, vacancy rates were estimated at over 3% in social care compared to
1.4% for all sectors, with 25% of care providers reporting vacancies compared to 12% for all
sectors (2009 National Employer Skills Survey data, cited in Eborall et al. 2010).
Although the level of vacancies has declined with the recession the impact on turnover has
been less, and the differentially higher rates of vacancies compared to the average position
has been maintained. However, high vacancy rates are not attributed so much to actual skills
shortages as to high turnover compared to other sectors with high vacancy rates. The
evidence therefore suggests that the social care market has tended to adjust to shortage not
through pay rates but by use of migrant workers to fill employment gaps in those areas with
greatest recruitment problems. Labour shortage is also acute for senior care workers;
JobCentre Plus data show that the vacancy-to-unemployment ratio for the period February
3
This is the wage level at which 20% of the category of workers earn less.
EWERC
Part I. The study context
17
2008 to January 2009 is much higher for this group than the ratio for all occupations (1.88
compared with 0.38) (House of Commons 2009).
Figure I.4. Percentage of social workers and care workers born abroad, by region
Source : Experìan (2007) for Skills for Care.
Although turnover is clearly high, there is as yet no conclusive evidence that social care
workers are subject to labour market churning between sectors rather than between different
social care providers. The NMDS finds 13% of care workers leaving for other care sectors
and only 2%, for example, to the retail sector. However, more than half (55%) of worker
departures do not have a recorded destination so these data are not yet reliable.
Social care work is still largely women‟s work and women still account for over 85% of care
assistants and home carers (Skills for Care 2010). Macro level evidence on women‟s
changing employment pattern may therefore provide more solid indicators of future problems
for social care. Research suggests that the tendency for women to stay in employment with
the same employer over the period of childbirth, now supported by the right to request
flexible working, is likely to reduce the number of women trading down the occupation and
pay hierarchy in order to find part-time work (Neuburger et al. 2010). This greater continuity
of employment should in principle allow women to pursue more upwardly mobile careers
which may reduce the labour supply for job sectors with limited opportunities for pay or
career advancement. However, the evidence cited here relates to the period before the 2008-9
recession. Increased unemployment and the overall shortage of jobs may lead to a
postponement of the upgrading of social care jobs which is indicated as necessary by the
employment gaps and the compression of wages at or near to the national minimum wage.
EWERC
Part I. The study context
18
Beyond these regional and cyclical labour market influences, the locality is likely to have
significance for the recruitment and retention of the social care workforce due to both the
nature of social care work - particularly domiciliary care - and the primary source of labour
supply, mainly mature women. The locality takes on importance because of the delivery of
care work in the users‟ own homes and the need for repeated and short visits to these
locations and for visits to multiple locations. These characteristics are likely to lead to a
labour force drawn primarily from the immediate locality to reduce the costs of travel
between home and workplaces, particularly where work is organised on a split shift basis or
where the hours of work are variable and may involve short shifts. This pattern of work
organisation is likely to reinforce the reliance on female labour, as there is strong evidence
that women in all types of jobs (due to both care responsibilities and less access to private
transport), as well as part-time workers of both sexes, commute a shorter distance to work
and are therefore likely to be attracted by jobs in the immediate locality (Green and Owen
2006, Houston 2005, Yeandle et al. 2006).
However, this apparent matching of demand and supply side preferences is both positive and
negative for the recruitment and retention of a social care workforce. It is positive in that it
may help organisations to recruit workers and also ensure retention, even when wages may be
low relative to the nature of the job and to alternative job opportunities involving longer
commutes. This could be regarded as also opening up an opportunity for providers to exercise
monopsony4 power over the workforce - that is, to rely on their staff‟s commitment to the job
due to its convenience with respect to place and time, even when wages and conditions fall
below relevant rates (Barth and Dale-Olsen 2009, Hirsch 2010, Manning 2003). However,
these work characteristics are also negative for recruiting and retaining a social care
workforce if there is a desire or a need to expand the size of the workforce once the supply of
those for whom the work is convenient is exhausted. It may be difficult to attract similar
workers located in different neighbouring localities as they may also prefer to work in their
own locality and to minimise commuting time. Indeed economic theory would suggest that
monopsonists would tend to keep employment down to maintain low wages even if some
vacancies remain unfilled (Manning 2003). In the UK social care sector, employers do not
have a free choice to raise the wages to solve these supply constraints since to a large extent
the wage levels are shaped by LA fee levels rather than by their internal HR policies.
4
A monopsony employer is one that controls the market for hiring a particular type of worker, defined by skill,
expertise or occupation, for example.
EWERC
Part I. The study context
19
I.3. Management and organisational factors in the recruitment
and retention of a social care workforce
In this section we discuss the key organisational factors (MaROT), as described in figure I.1
above, which are likely to shape the recruitment and retention of a social care workforce.
These include: first, the formal and informal Management of recruitment and retention,
including consideration of so-called „high performance bundles‟ of HR practices and
provisions for individual and collective employee voice; second, the Reward practices,
particularly in relation to part-time work and women returners; third, the Organisation of care
work, including discussion of the nature of care work, scope for worker autonomy and skill
content; and fourth, evidence of Training and development practices as a factor in shaping
recruitment and retention.
I.3.1. Management and human resource practices
The management of human resources varies by character of organisation, particularly by size
and by ownership. The social care sector is characterised by large numbers of small
establishments with over 40,000 local units employing care staff engaged with adult social
care belonging to over 17,000 organisations (Eborall et al. 2010). There are now 5,319
domiciliary care providers – an increase of over a quarter between March 2006 and August
2009. In contrast the number of care-only homes has declined by 9% over the same period
(although the number of beds increased) and now stands at 14,138 while the number of care
homes providing nursing increased by 4% to 4,303. Overall there is a very high share of
small establishments with three quarters of the 40,000 total employing fewer than 20
employees.
Although the sector is still highly fragmented there is a general trend towards more
concentration of ownership. Published data are only available for the care home sector
(Eborall et al. 2010). Here the concentration is particularly notable among care homes
offering nursing where according to Laing and Buisson‟s definition of a major provider - any
company listed on the London Stock Exchange - the major providers‟ share of private sector
homes increased from 36% in 2000 to 58% in 2009. For care-only homes the increase was
almost as striking but from a lower level – from 8% to 28% over the same period -, while the
share of major providers in the voluntary sector (accounting for around 17% of all homes5) is
even higher, rising from 64% to 73% over the same period. Overall, despite the trend towards
more concentration, the sector is still dominated by small establishments and the practices of
the major providers may still be to treat human resource policies as largely a local issue,
delegated to local management. There is an extensive literature on differences between large
and small firms in recruitment methods, human resource policies and employee voice
5
The 17% figure refers to all care homes while the Laing and Buisson data only refer to homes for the elderly
and physically disabled.
EWERC
Part I. The study context
20
mechanisms. These characteristics of the employers within the social care sector are thus
likely to be shaping the recruitment and development of the workforce.
Recruitment practices
Larger firms are known to make more extensive use of formal recruitment methods than
small firms where recruitment is often by word of mouth or informal channels. A range of
explanations have been offered for this tendency towards informality. First, there is the
obvious incentive to avoid the costs of advertising and formal procedures (Ram et al. 2004),
particularly if recruiting in this way may reduce turnover further reducing hiring costs
(Carroll et al. 1999). Secondly, small firms and establishments may be more concerned with
ensuring a good fit between the new employee and the established team due to the close
working environment for all employees (Holliday 1995). However, such considerations may
apply less to domiciliary care than to care homes due to the work being undertaken in users‟
homes with staff often working alone. A third explanation is that the use of a network may be
a means of hiring staff with already developed tacit understandings and tacit skills related to
the area of work. The network through which hiring takes place can thus be considered to be
an extended internal labour market (Manwaring 1984). The idea is that employees with the
required skill and experience may be found both inside and outside the organisation, where
employees outside are connected through informal channels and social and family relations to
those inside. Such an approach may suit management‟s need to control the workforce; the
informal channels and social networks can diffuse certain attitudes towards work, such as
compliance with organisational practices, thereby reducing the need for direct management
intervention (Collinson et al. 1990). In many areas of social care, managers are not in a
position to directly supervise the work and therefore may be reliant on social networks to
spread norms and attitudes towards work discipline among potential future recruits.
A key issue is how and when organisations change from informal to formal recruitment
methods. Change may occur because the organisation faces rapid expansion, or reaches a
critical size beyond which the owner or head manager is unable to devote time to informal
methods (Carroll et al. 1999). In social care, there are particular regulatory pressures that
promote greater formalisation. These include the monitoring of minimum care standards and
the inspection processes of both the CQC and the commissioning LA, as well as the
requirement that all social care providers check the references of job applicants and apply for
CRB checks. Research suggests there are mixed attitudes towards the effect of regulations on
recruitment processes in social care: some employers welcome it as a catalyst to a
professionalization process, which should improve the status of care work and, in turn, ease
recruitment in the long term, while others see it as adding to bureaucracy and delays
(especially the wait for CRB checks) thereby inhibiting recruitment (Edwards et al. 2003).
EWERC
Part I. The study context
21
Human resource practices
Perhaps the most dominant research theme in human resource management over recent years
has been the investigation of bundles of HR practices that might be associated with high
performance or high commitment work systems, whether measured by productivity,
profitability or staff turnover (Appelbaum et al. 2000, Huselid 1995). High performance
bundles of HR practices are expected to provide benefits that outweigh the costs of their
introduction and maintenance by creating the kind of work culture in which workers are
likely to feel both more satisfied and more motivated and committed.
Most research applies to large organisations and there is evidence that small organisations are
less likely to adopt high performance HR practices (Bryson et al. 2007). Nevertheless, to the
extent that small organisations do adopt these practices, there is some evidence that they may
be associated with some performance benefits. One UK study shows that the adoption of nine
specific HR practices – namely, careful selection, formal performance appraisal, performance
related pay, group incentives, multi-skilling, job rotation, quality circles, team working and
disclosure of information - is associated with higher profitability, although no impact was
found on productivity or staff turnover (Stirpe et al. 2009).
Importantly, the simple formula that predicts a positive relationship between a given set of
HR practices and organisational performance is contingent upon (and complicated by) the
sector. Within social care, there are first of all multiple obstacles to the adoption of certain
HR practices. Managers may be unfamiliar with particular HR practices, or sceptical of their
assumed benefits, especially where they involve considerable upfront costs. Other HR
practices may be difficult to implement within a social care environment. For example, the
practice of performance-related pay would raise ethical issues, not to mention the concrete
problem of how to assess and measure performance. A fundamental problem with the HR
bundles approach is its presumption that organisations already apply certain basic HR
practices and provide stability of income and employment. But in the UK social care sector,
such basic stability and protection of pay and employment is often lacking (Rubery and
Urwin 2011). We may therefore need to consider an alternative bundle of HR practices that
differentiates organisational performance in terms of whether employers provide basic
employment conditions such as guaranteed working hours, stable weekly income, payment
for all time spent at work (including, for example, travel time and training time), a decent
level of pay and pay progression in recognition of skill and experience.
Employee voice
The opportunity for employees to exercise „voice‟ in an organisation rather than „exit‟ is an
important factor in improving rates of staff retention. The outsourcing of social care to the
independent sector means that the majority of care workers no longer enjoy the opportunity
for collective voice through trade union representation and collective bargaining. This is both
a result of a shift from the public sector, where collective bargaining is strong, to the
independent sector where it is weak, and a shift from large to small organisations, since
EWERC
Part I. The study context
22
presence of all types of voice mechanisms and communication channels is positively related
to firm size. Non union forms of employee voice offer a potential alternative but the evidence
suggests that in the absence of strong formal voice mechanisms alternative communication
mechanisms tend to be ineffective (Willman et al. 2006). All of this does not augur well for
voice and communication systems in social care. In addition the highly fragmented work
processes in domiciliary care makes mobilisation and organisation of collective voice
especially difficult.
Nevertheless, while the circumstances of the sector may present obstacles to the formation of
strong collective voice, there are good reasons why social care workers may require a
minimum set of standards that ensure individual voice. Marsden (2007) argues that
opportunities for informal, one-to-one renegotiation of tasks between employee and employer
(or manager) ought to be considered and promoted as a form of employee voice. He makes
this argument in relation to work which may change only periodically; in social care,
particularly domiciliary work, there are changes on an almost daily basis associated with
changing users and user needs, as well as the timing of work, such that there is a need for
individual care workers to negotiate with their manager about whether such changes are
acceptable. Much depends on how the boundaries of acceptability are defined and whether or
not these are mutually accepted be employee and manager - as we learn from the many
studies of the employment relationship and the „psychological contract‟ between employer
and employee. Some research does suggest that it is individual relationships with managers
that matter most and make people feel involved and listened to. McClimont and Grove‟s
(2004) survey of the causes of high employee motivation at work identified good managers
and access to them as very important. Also, in Eaton‟s (2000) discussion of low quality care
jobs some of the most important characteristics of such jobs were a lack of feedback on
effects of their work, little or no supervision and, no information about the condition of
patients. How managers manage the work allocation among staff and how far they are able to
match employees‟ expectations and preferences with respect to the mix of users and tasks, as
well as the available working time, is likely to be a very important factor in improving rates
of retention of the care workforce
I.3.2. Reward practices
We turn now to consideration of how reward practices shape the extent to which care
organisations enjoy a positive experience in their recruitment and retention of workers in the
UK context. We know from general research on pay practices, as well as specific studies of
the social care sector in the UK, that pay practices have a significant impact on the ability of
organisations to recruit and retain staff. Our discussion distinguishes three issues: the relative
level of pay in the social care sector, the influence of upratings in the National Minimum
Wage and use of pay enhancements.
EWERC
Part I. The study context
23
Relative level of pay
Higher pay places employers in a stronger position relative to competitors and increases their
attractiveness both to prospective employees who are more likely to apply for a job and
current employees who are less likely to depart. Such an assertion is confirmed by wellknown economics models – „efficiency-wage‟ models - which argue it may be rational for
some employers to pay a wage above that offered by competitor organisations since higher
pay can reduce staff turnover and attract a better pool of job applicants (Akerlof and Yellen
1986). Several studies provide an empirical test. Levine‟s (1993) study of a US
manufacturing firm, for example, showed that a higher relative wage improved workers‟ job
satisfaction, their intentions to stay with the company and their willingness to work harder.
Also, Barber and Bretz (2000) demonstrate that higher pay is an effective tool to attract larger
pools of interested job applicants (cited in Guthrie 2007). But to what extent is such a
strategy applicable in the UK social care sector?
Compared to other labour market competitors there is limited evidence of use of higher pay
in the social care sector. Table I.2 presents pay data for the residential elderly care sector6 and
the retail sector, the sector consistently cited as a key labour market competitor (eg. Yeandle
et al. 2006: 24). Pay data are provided for the two dominant groups of care workers, female
part-timers and female full-timers, at different points of the pay distribution, along with the
pay differential between sectors.
Table I.2. Women’s pay in the residential care sector and the retail sector compared,
2009
All sectors
D10
All male and
female employees
6.19
D20
Residential care for the
elderly (SIC 873)
Part-time
Full-time
Retail trade (SIC 47)
Part-time
Full-time
Pay differential
between sectors
Part-time Full-time
5.73
6.03
5.73
6.00
0.0%
0.5%
7.15
6.00
6.48
5.76
6.32
4.2%
2.5%
Median
10.99
6.81
7.96
6.25
7.80
9.0%
2.1%
Mean
14.43
7.88
9.32
7.02
9.74
12.3%
-4.3%
Note: Gross hourly earnings, overtime excluded.
Source: Annual Survey of Hours and Earnings, own compilation.
The earnings data in table I.2 show that average hourly pay at the bottom decile of the pay
distribution7 is similar in the social care sector and the retail sector – equivalent to, or a little
above, the national minimum wage of £5.73 that applied in April 2009, the time of data
collection. Further up the pay distribution there is some evidence of higher rates paid to
6
Using the industry classification this category gives the most precise estimate of earnings for workers in the
sector. No separate industry category exists for the domiciliary care sector.
7
That is, the level at which 10% of the workforce earn less.
EWERC
Part I. The study context
24
women in part-time jobs, up to a premium of 12% at the average point, but the pattern is
reversed among women in full-time jobs where pay is actually 4% lower than the average
hourly wage in the retail sector. Overall, the inter-sectoral comparison suggests employers in
the care sector are not using pay to address recruitment and retention issues, despite the
evident need.
Prior to the recession, the low level of pay in the sector was a major reason explaining
difficulties in recruitment and retention. Surveys of employees in the care sector suggest that
the level of pay falls below expectations, given the required responsibilities, skill and
emotional demands of care work. A Unison survey in 2002 reported more than four fifths
(82%) of domiciliary workers disagreed with the claim that their pay was fair, a higher
proportion than other groups surveyed such as social workers and housing workers (Unison
2003). The detailed study completed by Yeandle and colleagues identifies low pay and the
attractiveness of less demanding jobs in other sectors offering similar pay. The following
quote from the one of the independent domiciliary providers in their study is illustrative:
At the end of the day, [care workers] are going to look at what the salary is, and then they are
going to look at Tescos where they can make a hell of a lot of money without the
responsibility, without being out in the community themselves, in charge, and having to be the
first person in an emergency. It‟s an awful lot of responsibility (Newcastle provider, cited in
Yeandle et al. 2006: 25).
The issue of low pay and problems of comparability with other sectors such as retail is
especially pronounced in the private sector, where pay is lower on average than in the local
authority and voluntary sectors. Estimates from the National Minimum Dataset for Social
Care (NMDS-SC) suggest median pay for care workers in the private sector in 2009 was just
£6.00, compared to £7.03 in the voluntary sector and £7.73 in the LA sector. For senior care
workers the differences are even larger – median rates of £6.70, £8.08 and £10.69,
respectively (Eborall et al. 2010: 111). If we compare pay data from the different sectors of
care work with pay for retail assistants, we see a strikingly divergent pattern of pay premiums
and pay penalties for social care work (figure I.5). At the median pay level, care workers in
the LA sector earn over 20% more than retail sales assistants, those in the voluntary sector
around 10% more but care workers in the private sector 5% less. At the average level of pay,
the penalty in the private sector is even higher at 15%, compared to a premium of 13%
among LA care workers. Overall, therefore, the evidence on levels of pay suggests the
majority of employers are not using pay-setting as a strategy to enlarge the pool of job
applicants or to improve staff retention among existing employees.
EWERC
Part I. The study context
25
Figure I.5. Pay difference with retail sales assistants among care workers in the private,
voluntary and LA sectors, 2009
25%
20%
15%
10%
5%
0%
median
-5%
average
-10%
-15%
private
voluntary
LA
-20%
Source: Eborall et al. (2010: 111) for care worker earnings data and Annual Survey of Hours and Earnings for
retail sales assistants data (SOC code 7111). All earnings data are for all adult employees, gross hourly pay
excluding overtime.
Regarding oppotunities for pay progression in the sector, the very small differential between
pay at the bottom decile for care workers and the median pay suggests limited chance for pay
advancement. The median pay for female part-time workers in the residential care sector is
only £1 or so above the bottom decile pay (table I.2 above). This might be expected if care
workers stay for very short periods in the job, and fail to accumulate the stock of experience
and skill that can lead to higher pay. However, estimates from the national minimum dataset
for social care (NMDS-SC) suggest two thirds of workers (64%) have more than five years
experience in social care, and more than a third (36%) register experience of at least 11 years
(Eborall et al. 2010: 93).
The influence of the National Minimum Wage
In low-paying sectors such as social care a statutory minimum wage can play an important
role in shaping pay practices, which in turn influences recruitment and retention. On the one
hand, steady uprating of the statutory minimum wage can provide a valuable benchmark for
employers (by providing a coordinated wage floor to labour market competition) and
employees (by protecting against exploitative wage levels). However, a minimum wage also
presents serious challenges to organisations that operate in product markets where there are
obstacles to increasing revenue, typically achieved by passing on higher labour costs to
clients in the form of higher prices. Grimshaw and Carroll (2006) identify three types of
obstacle associated with particular product markets:
first, in international markets prices are set through international not domestic
competition and are therefore not responsive to trends in national minimum wages;
EWERC
Part I. The study context
26
second, a product market dominated by one or two client organisations can make
negotiation of price rises difficult; and
third, where a product market includes firms operating in the informal economy there
is a risk that unscrupulous employers undercut organisations that raise prices in line
with the minimum wage (op. cit.).
The second type of product market constraint prevails in the social care sector. Care
providers are strongly reliant on LA fees as a source of revenue. The longstanding disconnect
between annual raises in LA fees (adjusted in line with inflation and average earnings
growth) and the national minimum wage (which was purposefully adjusted above average
earnings growth during 2003-2006) generates a major squeeze on providers‟ income. This, at
a time of new regulations to introduce national minimum care standards, has presented care
providers with a major challenge. The Low Pay Commission (LPC) has repeatedly
recommended that government address this issue (eg. LPC 2009: 73). Also, in light of the
third constraint listed above concerning informal activities, the LPC has also raised a new
concern that personal payment plans risk problems of non-compliance with minimum wage
legislation:
In circumstances of individuals purchasing their own care, both the service user and
those performing the personal assistant role may not be fully aware of their rights and
responsibilities in respect of their employment relationship, including payment of at
least the national minimum wage (LPC 2009: 73).
Because low-paying sectors in the UK have a high proportion of jobs paid at the adult
minimum wage, trends in the minimum wage have a major influence on the setting of pay.
According to the Low Pay Commission (LPC 2009), the cleaning sector has the highest
incidence of workers paid at the minimum wage (22% in 2008, up from 19% in 2007). In
social care, there is a public-private divide; in 2008 nearly one in ten workers (7.8%) were
paid a minimum wage in the private sector, compared to around one in a hundred (1.3%) in
the public or voluntary sectors (LPC 2009: 71). The difference reflects the influence of
collective bargaining and joint agreements for LA employed care workers and their general
absence in the private sector.
National earnings data for the occupational group of care assistants and home carers
demonstrate a very close relationship between nominal pay trends and changes in the
minimum wage. For female part-time care workers, figure I.6 shows that the differential in
pay at three different points of the pay distribution (the bottom decile, lower quintile and
median) has remained very stable since 2005 suggesting a very strong influence of minimum
wage rises on pay-setting.8 The influence is most striking at the bottom pay position (D10)
where care workers‟ pay has fluctuated around 5% higher than the adult minimum wage. The
rising differential from 2002 to 2003 occurred at a time when the minimum wage rise was
very low (10p, from £4.10 to £4.20), and preceded a decision by the LPC to increase the
minimum wage at a pace above average earnings growth.
8
Earnings data for female full-timers reveal a very similar trend as the one shown in figure I.6
EWERC
Part I. The study context
27
Figure I.6. Pay trends of female part-time care workers relative to the national
minimum wage, 2002-2009
45%
40%
% differential with NMW
35%
30%
D10
D20
25%
Median
20%
15%
10%
5%
0%
2002
2003
2004
2005
2006
2007
2008
2009
Source: Annual Survey of Hours and Earnings, gross hourly pay excluding overtime, SOC 6115 „Care assistants
and home carers‟, own compilation.
Pay enhancements
Pay enhancements offer an additional tool to address recruitment and retention issues.
Theories of compensating differentials maintain that pay supplements for night work or
weekend work, for example, are explained by the need for employers to compensate the
disutility experienced by employees working during unsocial hours. However, in many 24-7
areas of the UK economy, pay supplements for unsocial hours working have been eliminated
or reduced, alongside the decline in trade union influence on wage-setting. The trend appears
to have been led by the retail sector. Tesco, for example, abolished a customary 50% pay
premium for overtime work, reduced a percentage premium for night work to a fixed sum
payment, and reduced the premium for Sunday and public holiday working from 100% to
50%.
The representative survey of 502 care workers undertaken by the market research firm, TNS,
provides evidence of the use of pay premiums for overtime and unsocial hours working in the
social care sector. Regarding overtime, 34% of jobs involved paid overtime compared to 25%
with unpaid overtime (TNS 2007: 30). It is notable that those workers with longest
experience in care work are most likely to undertake unpaid overtime, suggesting that longserving workers are either more likely to volunteer to cover for absent colleagues without
pay, or more likely to be pressured to take on extra work by managers with the knowledge
their alternative job opportunities are limited, a problem that will be more pronounced now
EWERC
Part I. The study context
28
during a period of high unemployment. Overall, while jobs in care homes are more likely to
involve overtime work, it is the jobs in domiciliary care that are more likely to demand unpad
overtime – 33% of all domiciliary care jobs.
Shifts are a major feature of care work but only a third of jobs requiring shiftwork pay a
supplement; in private firms this share drops to one fifth (18%) (TNS 2007: 33). Similarly,
nightwork is required in around two fifths of care jobs (43%) but most workers (61%) in such
jobs do not receive any form of pay enhancement, making them worse off than retail
supermarket chains which at least pay a fixed supplement for nightwork. Again, private
providers are least likely to pay a nightwork enhancement – only 28% of the surveyed care
workers employed in the private sector (op. cit.). Any notion of compensating differentials in
the social care sector thus appears to have been abandoned.
One pay enhancement peculiar to the social care sector is payment for travel time, given the
requirement in around one third of care jobs to travel between users‟ homes. The TNS survey
reports that of those care workers in jobs involving travelling, some 37% travel more than 5
hours per week (TNS 2007: 34). Again, around half of workers are neither paid for their
travel time (52%) (in contravention of the national minimum wage legislation) nor
compensated for travel costs (petrol, etc.) (45%) (op. cit.). The issue is an obstacle to
improving recruitment and retention (Yeandle et al. 2006) and recognised as problematic by
the industry employer body, the UKHCA. The following quote illustrates the interlinkages
with commissioning arrangements that focus on precise units of care time, an issue we
explore further in the following section:
[Local authority] commissioners will also use other cost saving mechanisms, such as
only paying for contact time, sometimes as short as 2 to 10 minutes, or using short
care episodes for personal care tasks to reduce costs. As care is generally purchased
by reference to “contact time” (ie the time spent in the user‟s home) the rate paid is
crucial. Providers must be able to reach National Minimum Wage - which must cover
travel time – from increasingly small units of time. In addition, there is an impact on
the wellbeing and job satisfaction of the workforce, and the user‟s satisfaction with
care received. It also constrains providers‟ ability to pass on wage costs for
careworkers undergoing training as they are only able to derive fees for billing for
services provided (UKHCA 2009: 9).
I.3.3. The organisation of care work
In this section we identify the ways recruitment and retention in care work may be affected
by the organisation of care work. The nature of care jobs, how these jobs are designed, the
pace of work, the skill content of the job and the opportunities for workers to exercise
autonomy and discretion when performing the role can all be expected to influence both
recruitment and retention. Likewise, how working time is organised, including shift
arrangements, the flexibility available to meet workers‟ needs and requirements for travel
may be critical to both entry and retention. While low pay exacerbates recruitment and
retention difficulties, wider debates relating to job quality indicate that broader measures of
job satisfaction are also helpful in understanding labour market behaviour such as turnover
EWERC
Part I. The study context
29
for example. Indeed, Clark (2005) argues that restricting analyses to wages and hours of work
„gives a misleading picture of what makes a good job, and hence of workers behaviour‟ (op
cit: 2005: 12).
The nature of the job
The limited research that has looked at why people choose to work in the care sector reveals
that even when there are pragmatic motivations, such as choosing a job that fits with other
commitments or fits with a chosen career, „the choice is unlikely to be motivated purely by its
extrinsic rewards. Rather, if a care worker feels she has made a choice it will be for reasons
that touch upon the work itself‟ (Himmelweit 1999: 34). McClimont and Grove‟s (2004)
survey of 3,000 care workers found the three most cited reasons for entering the care sector
were enjoying helping others, liking care work and working time flexibility and a survey of
500 workers commissioned by Skills for Care (TNS 2007) found that enjoying working with
people and wanting to enter this type of care work were the most important reasons along
with the desire to work flexible hours (box 1.2).
Case-study research indicates that this predisposition to caring for others is not formed within
the workplace (Cunningham 2005: 4) and in domiciliary care the lack of a fixed workplace
means that management and colleagues in the workplace are less influential on care workers‟
commitment to care work. However, for recruitment and retention it is important to see if
care workers have the opportunity to act on these values once they have entered the sector.
The survey results indicate that these pre-entry values, expectations and motivation continue
to take precedent in explanations of job satisfaction. Job satisfaction is high in the sector with
almost nine in ten (88%) care workers in the Skills for Care survey saying they were happy in
their jobs. Box 1.2 presents the main factors underlying this broad finding of job satisfaction,
and points to the importance of the nature of care work, including the relationships with users
and caring and looking after others.
Social care work can therefore be described as „intrinsically satisfying‟ in the sense that
workers feel they can, in principle, „make a difference‟ in their job (Eborall 2003: 11). If
there are no barriers to care workers making a difference, then „job satisfaction will
automatically be high‟ (Eborall 2003: 11). Yet it is important to recognize that the way the
work is organized may indeed present barriers to care workers making a difference and that
such barriers may impact on care workers‟ propensity to remain in the sector. Likewise,
survey research shows the importance of being able to work flexibly and again if this need is
not met there may be an adverse effect on recruitment and retention. Therefore, a crucial
factor is the way organisations manage and meet expectations in relation to the nature of the
work and the flexibility on offer.
EWERC
Part I. The study context
30
Box 1.2. Reasons for entering care work and for remaining in care work
Two surveys provide evidence of the reasons people cite for entering care work:
McClimont and Grove‟s (2004) survey reports
the following eight most cited reasons:
1. Enjoy helping others
2. Like care work
3. Flexibility to fit around other
commitments
4. Easy, quick application process and
rapid start to work
5. Pay
6. It was convenient
7. It provides a way into a career into
nursing
8. Just needed a job
The survey for Skills for Care (TNS, 2007: 59)
reports the following commonly cited reasons:
1. Always enjoyed working with people I
care for (40%)
2. Always wanted to enter this area of
work (25%)
3. Convenient/flexible hours (25%)
4. Knew someone that did it (21%)
5. Just needed a job/ to earn money (19%)
6. Someone recommended it (18%)
7. Was unpaid carer for family member
(15%)
8. Was close/ easy to get to (15%)
And the same surveys also report evidence about the factors held to be important by care workers
already in employment in shaping their satisfaction with the job:
McClimont and Grove‟s (2004) survey reports
The Skills for Care (TNS 2007: 64) survey
13 factors cited by care workers:
identified the following ten „favourite things
about work‟:
1. Relationship with clients [users]
1. Job satisfaction (14%)
2. Good managers
2. Chatting with clients [users] (12%)
3. Being able to get hold of managers easily
3. Meeting different people (11%)
4. Training
4. Caring/looking after people (1%)
5. Being trained before starting work
5. Helping people (10%)
6. Flexibility to do what client [user] wants
6. Knowing you are making a difference
or needs
(10%)
7. Clear and easily understood contract
7. The people I work with (8%)
8. Opportunity to undertake an NVQ/SVQ
8. Keeping clients [users] happy (7%)
qualification
9. Flexibility of working hours (3%)
9. Being involved in decisions about clients
10. Building relationships with/gaining the
[users] or work
trust of clients [users] (3%).
10. Staying with the same clients [users]
11. Being able to say „no‟ to work
12. Opportunity to progress to senior care
worker or higher
13. Clearly defined career path
EWERC
Part I. The study context
31
The organisation of work shapes the nature of care work in three key ways:
the degree of standardization of tasks and the amount of time allocated to perform
these (pace of work);
the job content and specifically the level of skills required to perform the role,
including opportunities to exercise autonomy and discretion (control over work); and
the opportunities for employee involvement and supervisory support (voice at work).
Standardization of care and pace of work
A certain amount of standardization of care work is a requirement in the relationships that
develop between LAs and providers. LAs purchase from providers a specified period of time
to carry out a range of tasks for individual service users (Glendinning et al. 2008b). These
tasks are set out in a care plan where the care needs of users are broken down into specific
tasks and the time needed to carry out these tasks. Care workers have no involvement in the
organisation of care plans and in this sense it mirrors the notion of „service sector Taylorism‟
(Bosch and Lehndorff 2001) characterised by a separation of the planning and execution of
tasks. A key issue for care workers is the extent to which they have enough time to do all the
tasks allocated within the time frame they are given. In other words, is the volume of work
and pace of work acceptable and compatible with care workers‟ expectations and needs about
what the job should involve and what they value from it? Research suggests that when this is
not the case care workers are dissatisfied with their work and this can adversely impact upon
retention. According to McClimont and Grove‟s (2004) survey, commissioning arrangements
that facilitate tightly specified time slots lead to short visits that create feelings of being
rushed and this is a key factor in retention. Staff shortages may require the existing workforce
to accommodate many more visits across a wide area (Francis and Netten 2004).
Cunningham‟s (2005) case-study of a not-for-profit care provider reveals pressure on care
workers to concentrate on the more basic parts of their work rather than aspects they valued
because of limited time.
The current move to more outcomes-based care can be interpreted in part as a response to
these problems and provides some recognition that this model of standardization and
fragmentation of care tasks is „inappropriately rigid when it comes to the needs of people
receiving care‟ (Bosch and Lehndorff 2001: 87). Greater control by the user over the care
they receive may also give some scope for the care worker to respond flexibly to users‟ needs
(Sayer 2005). While the focus has been on what this has meant for users, studies of
outcomes-based services have also identified improvements in staff retention. Sayer argues
that, „It seems that clarity about the results they are trying to achieve, together with the
autonomy to respond flexibly to service users, is making the provision of domiciliary care
services much more fulfilling and satisfying to staff‟ (op cit: 2005: 23).
EWERC
Part I. The study context
32
Job content: skills, autonomy and discretion
While care work is low paid and is often categorized alongside other routine service work as
a „bad job‟ (Coates and Max 2005) the job of a care worker does not fit a standard
classification of routine work (Rubery and Urwin 2010). It shares with other types of
frontline work the simultaneity of production and consumption (Korcynski 2002) but
management scope for controlling service quality in this sector appears to be more limited
than in other frontline service work such as call centres, hospitality and retail because of the
amount of discretion the role potentially offers workers (Bolton 2004). For the recruitment
and retention of the care workforce a key question is therefore whether the skills and
discretion involved in care work can be considered a positive or a negative aspect of the job.
Gospel (2008) and Gospel and Lewis (2010) identifies three kinds of skills in care work:
technical skills needed to perform physical lifting, bathing, feeding and the administration of
medicine; interpersonal skills or social skills required to interact with older people; and
administrative skills for record-keeping and administration (2008: 22). Despite the required
multiple skills, however, Gospel found that in care homes care workers enjoy limited
discretion. Care workers have little input into personal care plans and have to refer to senior
care workers if they want to change minor aspects of this (op. cit.). Moreover, Gospel‟s
research demonstrates that care workers are keen to take on a wider range of tasks. However
unlike similar jobs in the NHS where a national programme of skill development and job
redesign has been implemented in part in response to shortages of cleaners and assistant
nurses (Cox et al. 2008, Grimshaw and Carroll 2008), there is no such evidence in the care
sector, except with regard to specialist services provision in some LA inhouse providers.
However, the lack of a sector-wide approach appears to have caused a polarisation of job
quality between LA and independent providers. McClimont and Grove (2004) argue the
focus of many LA providers on specialist care restricts the range of job opportunities
independent providers can offer their staff. Sayer‟s (2005) work on outcome-based care also
suggests independent domiciliary providers design jobs that fulfill basic „maintenance
outcomes‟, such as meeting basic physical needs, rather than „change outcomes‟. Sayer
argues the involvement of all providers in the full range of outcomes „is probably an
important step in enabling all providers to build stable, successful workforces‟ (op cit: 23).
The specialisation of activities among LA providers and accompanying process of skill
enhancement has also involved certain costs for the workforce, including enhanced temporal
flexibility (see below). But the general effect, like the pay gap between providers reported
above, is a polarization of jobs in terms of the skill and opportunities available between those
offered by LA inhouse providers and those by independent providers.
Like other types of service work, any depiction of care work that focuses on the more
tangible aspects of skill, such as certified knowledge, training, accredited qualifications and
career progression, misses the relational, or interpersonal, features of the job which are
essential to what constitutes a good care worker and a good care service. The relational
aspects of the work create positive opportunities for a worker to exercise discretion and
autonomy because of the relationships involved in caring and the absence of direct
supervisory control over these. Eaton (2000) cites a range of tasks involved in relational and
EWERC
Part I. The study context
33
emotional work, and elaborates the types of tacit knowledge required to perform the job well
(box 1.3). The challenges of decision-making in a context of intensive relational work are
perhaps most evident in the domiciliary care sector. Here, care workers often work alone and
have to be able to negotiate with the user all the aspects involved in the delivery of personal
care, including both the preset or routine tasks and the idiosyncratic or changed tasks. This
feature of their job can be a source of satisfaction, as we described above, but can also be a
source of stress. Care workers are expected not only to express empathy with the user but
also simultaneously to negotiate and manage boundaries between their commissioned tasks
and the user‟s expectations (Rubery and Urwin 2010: 3).
Box 1.3. The relational work of care workers
A review of studies by Eaton (2000) and Himmelweit (1999) suggest the following characteristics
of relational work and tacit knowledge are present in care work:
Relational work and emotional labour:
- conveying information
- providing comfort or companionship
- preventing a problem
- the „display‟ of a felt state, such as kindness, compassion and cheer
- ability to complete tasks patiently and gently with tolerance, even if one is being
physically abused or attacked
Tacit knowledge:
- how to lift and turn patients
- how to cheer patients
- to know who has grandchildren
- to know who prefers warm water for bathing.
The extent to which relationship work can be considered a type of skill is disputed (Lloyd and
Payne 2008). However, in contrast to other service areas where there is tight managerial
control over the formation of customer relationships through scripting and prescriptive modes
of behaviour - for example, flight attendants or call centre work - social care workers have
relatively high levels of discretion and freedom in their development of relationships.
However, there are tensions between discretion and control within care work. On the one
hand, managers rely on workers to sort out the changes in care associated with changes in
user needs (Francis and Netten 2004) and to establish positive personal relationships with
users in order to improve the perceived quality of the care delivered. But on the other hand,
managers and LAs seek to increase control over costs by introducing new methods for
monitoring care work, such as electronic monitoring where discretion is limited by increased
EWERC
Part I. The study context
34
pressure on time taken to deliver the care package. Cunningham‟s (2005) case-study research
demonstrates that care workers‟ discretionary behaviour and caring values were indeed
compromised by the work intensification that resulted from specific commissioning practices.
Moreover, the diminished opportunity for care workers to act out their values meant they
were more likely to express the desire to quit. However, the resilience of workers‟
commitment to helping and caring for others may still be enough to ensure this discretionary
behaviour continues despite the rigid targets in place (Bosch and Lehndorff 2001, Hebson et
al. 2003). Research evidence suggests that those individuals who are motivated intrinsically
or by a „calling‟ to their work may engage in more expansive „job crafting‟ – that is, the
exercise of discretion in defining and extending what the job entails - than individuals who
are more extrinsically motivated by financial reward or career advancement (Wrzeniewski
and Dutton 2001).
I.3.4. Training and development
Our fourth organisational factor described by the acronym MaROT (figure I.1 above) is
training and development. High quality provision of training and development of the social
care workforce is a vital aid to recruitment and retention. It can provide workers with much
needed support in their job through expanding their knowledge and skills and also establish
opportunities for career development.
At the national level, the development of minimum care standards9 and LA commissioning
requirements related to induction training and having at least 50% of care workers qualified
at NVQ level 2 (including agency staff and excluding managers) was found to be an
important driver for professionalization of care work and a boost to recruitment and retention
(see Gospel and Thompson 2003: 21-22 for details). In particular induction should ensure that
recruits are aware before they start work what a job in the care sector actually entails; this
might increase turnover in the very short term, but undoubtedly reduces wasteful investment
in new recruits who do not have the appetite for care work.
Training requirements can also exacerbate the recruitment and retention difficulties facing
independent providers. High turnover means not only that more time has to be spent on
training, thereby compromising the ability of providers to deliver services, but also that a
provider may fall below the training target, causing problems with both the CQC and the LA.
Even from the perspective of future or current employees, training is not always welcome;
those already experienced may resent being required to train and those considering entering
social care may be apprehensive about their academic ability to complete the training or
disillusioned by the lack of financial reward in the form of a pay rise (Gospel and Lewis
2010: 16-18). Yet training and development on its own may not be sufficient to improve
either the image or experience of care work particularly if completion of training does not
9
These minimum standards with respect to NVQ training have been discontinued in 2010
EWERC
Part I. The study context
35
lead to any advantages in terms of pay or future career opportunities. There is now evidence
that the introduction of regulations has stimulated the amount of training in social care
(Gospel and Lewis 2010),even if there are differences in the extent to which providers
actively engage with the training agenda, linked in part to the availability of support for
training from LAs and other agencies (Rainbird et al. 2009). Overall, however, the low pay
rates that still prevail suggest that this has not done much if anything to improve the status or
rewards of care work. Other countries have higher requirements for training for social care
than the UK (Ungerson and Yeandle 2006, Simonazzi 2009, Fagan and Anxo 2005) and these
training requirements are often associated with a greater professionalization and higher status
attached to social care work (Christopherson 1997). These higher training standards are often
implemented in contexts where there are sector-wide pay regulations, often based on
collective bargaining so that it is not the training in and of itself that raises status but training
combined with more regulated pay setting and the opportunity for social partners to engage in
social dialogue.
EWERC
Part I. The study context
36
I.4. Recruitment and retention from the user and employee
perspectives
The above discussion has shown how some of the ways care work is organized can shape the
quality of the care jobs on offer to a potential and existing care workforce. In this section we
assess the potential linkages between the quality of the care job on offer and the quality of the
care provided. Through a review of existing research on users‟ views of what constitutes a
good quality care service we identify the complementarities between user perspectives and
employee perspectives. Thus poor quality care jobs may not only exacerbate recruitment and
retention difficulties but also curtail opportunities to provide good quality care. In contrast
good quality care jobs have characteristics that improve service quality and job satisfaction,
which is pivotal to improving recruitment and retention. A key issue then is whether there are
complementarities or contradictions between user-centred services and employee-centred
work organisation (Kirkpatrick and Martinez Lucio 1995). The review below suggests a
greater presence of complementarities than contradictions, although only if the interests of
both the workforce and users are taken into account in the design and organisation of service
delivery. A final section considers the importance of time and space in shaping employee
perspectives on care work.
I.4.1.What makes a good care service and what makes a good care worker?
What makes a good care service?
In their summary of Qureshi et al.‟s (1998) research on older people‟s definitions of quality
care Glendinning et al. (2008b) suggest the priorities include change outcomes (such as
improvements in physical, mental and emotional functioning), maintenance outcomes
(prevention of or delay in deterioration in health, wellbeing and quality of life) and process
outcomes (such as feeling valued and respected, being treated as an individual, having a say
over how and when services are provided, perceived value for money and compatibility with
cultural preferences and informal sources of support) (op. cit.: 6-7). In case-study research
examining users‟ views on the care they receive and what they value, it is often process
outcomes that are emphasized which puts the care workforce, and how they are managed
trained and treated, at the centre of explanations of user satisfaction.
Francis and Netten‟s (2004) study of user views identified reliability, flexibility, continuity of
care, communication and good staff attitudes as the most important dimensions. However,
when talking about flexibility, it was flexibility to go beyond the care plan that users valued
most - that is, the attitudes of care workers and their willingness to help and undertake jobs
beyond those stipulated in the care plan (op. cit.: 295). In particular, users believed a „caring
motivation‟ was more important than the skills and knowledge defined in training standards;
Francis and Netten put it simply as follows, „if` care workers care they are good carers, if
they don‟t they are poor carers‟ (op. cit: 300). Two further reports (Henwood 2001, Sinclair
et al. 2000) identify older people‟s dislike of care workers‟ lack of flexibility and autonomy
EWERC
Part I. The study context
37
to deliver the type of service which users want. Both studies point to the importance of the
relationship between user and care worker, the need for user choice and flexibility over tasks
undertaken, and the need for users to have more control over the tasks undertaken. Such
flexibility may be compromised by organizational and commissioning practices where these
lead to fragmentation of tasks and short task-oriented visits (Sayer 2005).
Furthermore, problems of recruitment and retention directly impact upon the quality of the
service users receive. Users value reliability of care visits because it gives a sense of control
over their lives (Francis and Netten 2004: 295). Missed calls and waiting for calls along with
rushed visits are often the result of staff shortages and all compromise good quality care
standards. However users do not blame care workers for this and understand the pressures
they face (op. cit.). Interestingly, the desire for flexibility in service delivery not only
concerns temporal flexibility but also involves the desire for care workers to be responsive to
individual needs. On the basis of this discussion it is now possible to put forward some
tentative ideas about what makes a „good care worker‟ that is sensitive to the way
organizational and commissioning environments may shape this.
What makes a good care worker?
Caring involves caring for and caring about a person (Himmelweit 1999). A good care
worker must thus not only be able to care for the person to the best of their ability, putting
into practice skills and training they have acquired, but also, and significantly, must care
about the person they are caring for, respond flexibly to the user and their needs and ensure
process outcomes are achieved, including respect and independence and quality of life
outcomes that only come through the relationships that develop between the care worker and
user. To do this the onus is on the care worker displaying „citizenship type behaviour‟
(Hodson 2001) and „voluntarily giving extra effort to ensure production takes place
efficiently‟ (op. cit.: 68). In short, being a good care worker often involves going beyond
what they are expected to do out of commitment to either the user or the service
(Cunningham, 2005).
Significantly, managers may rely on this discretionary behaviour to deliver quality of care but
as we have seen in our discussion about job satisfaction (I.3.3 above), this is also an aspect of
the job care workers value. Relationships with users are a key source of job satisfaction and
helping and caring for users using tacit skills would appear to be a key component
underpinning the pride care workers experience in their job and the dignity they derive from
work. However, this discretionary behaviour and flexibility, so clearly valued by users and
central to definitions of „good care workers‟, may prevail despite organisational factors rather
than because of them. As Bosch and Lehndorff argue, „it is the standards of the employees
themselves that ensure such a system can operate irrespective of the targets set‟ (2001: 87).
EWERC
Part I. The study context
38
I.4.2. Is care work a good job or a bad job? The employee perspective
The success of any recruitment and retention strategy for the social care workforce is likely to
depend upon whether care work is considered a good or bad job from an employee
perspective. Here we first of all review debates on good versus bad jobs before addressing the
relationship between care work and attitudes towards women‟s employment and women‟s
skills.
Care work and job quality: complementarities, trade-offs and contradictions
A range of dimensions are used in measurements of job quality including pay and benefits,
job security, training and career opportunities, task discretion, job content and pace of work,
employee involvement and voice and ,work-life balance (Tilly 1997, Appelbaum et al. 2010).
However, because some dimensions such as pay are more easily measured compared to
others good and bad jobs are often defined in relation to these (Goos and Manning 2003). Use
of pay as a proxy for job quality is of course only valid to the extent that low pay is
accompanied by other low quality job dimensions. Some studies confirm such an association,
with evidence of „multiple deprivation‟ (Ritter and Anker 2002, Clark 2005) and
segmentation of jobs, such that „some groups of workers may have better jobs than others‟
(Clark 2005: 21).
Efforts to use HR practices to improve job quality need to recognise the potential for
complementarity and positive inter-linkages. Recent comparative research on the hospital
sector suggests that redesigned jobs have limited impact on job satisfaction if they are not
supported by training and compensated by wage increases (Méhaut et al. 2010: 16-17). This
has also been found to be the case in relation to good quality care jobs. Gospel and Lewis‟s
(2010) research on the impact of training regulations in the care sector found that this did not
have the desired impact on job quality because training initiatives were not complemented by
newly designed job roles, the provision of financial reward for qualifications, and
opportunities for workers to pursue clearly defined and managed career pathways. Studies by
Hunter (2000) and Eaton (2000) also identify a bundle of HR practices that make a positive
difference to job quality and quality care.
However, this additive approach to job quality does not sit easily with a workforce that
appears to have accepted a trade-off between different dimensions of job quality. As
suggested above, care work does not fit the picture of routinised, low paid and low status
work since the discretionary content and levels of job satisfaction can potentially be quite
high. For care workers it would appear that their job is not so much a „good job‟ constituted
by a bundle of complementary, „good‟ dimensions, but a job riddled with trade-offs and
contradictions reflecting in part the importance of one or other dimension from the
perspective of providers and care workers.
These trade-offs are found both within a single dimension and between job quality
dimensions. For example, with respect to discretion and control we have seen that care work
EWERC
Part I. The study context
39
provides for a high level of discretion but the value of this discretion is not necessarily
recognised even though it is contributing to quality of outcomes. Moreover new electronic
monitoring techniques, although introduced by LAs to monitor the provider, are being used to
monitor employee behaviour which could reduce employees ability and willingness to engage
in discretionary work effort. However, Brown and Korczynski (2010) have shown that while
organizational commitment to the employer may decline because of this form of monitoring,
it can lead to higher discretionary effort because of the care workers‟ commitment to provide
quality care despite the constraints such monitoring can place on achieving this.
There also appears to be a trade-off between pay and job satisfaction. A report for the
employer body for provider organisations (McClimont and Grove 2004) highlights the
problem in assessing how important pay is in workers‟ perceptions of the job since most
surveys, including their own, only focus on care workers in employment. These workers
ranked pay fifth out of eight in terms of importance, but this may not reflect the importance
of pay to those care workers who quit to work elsewhere. Therefore, it may be unwise for
policymakers to place too much weight on evidence of high satisfaction and low concerns
over pay among existing care workers when seeking to identify means of expanding the
workforce.
Measures of job dissatisfaction may provide more useful information on where the barriers to
recruitment and retention may lie. In the Skills for Care survey (TNS 2007), of the few care
workers who said they were unhappy, the most commonly mentioned reasons cited were poor
pay, wanting more support from the management, disliking the unsociable or long hours and
not liking the particular company they worked for. McClimont and Grove (2004) also show
how important managerial support is for job satisfaction and how dissatisfaction tends to
relate to the employer rather than the job itself. What becomes clear is that if workers are
dissatisfied with the job, and in particular feel they cannot take pride in their work and act
upon their values and expectations about caring for users, other dimensions such as pay, that
are often cited as relatively unimportant by those working in the sector, become increasingly
more important and low pay becomes a reason to quit (Cunningham 2005, Sayer 2005).
Issues around working hours also seem to be a dimension of job quality that can determine
intentions to enter the occupation or quit (Cunningham 2005).
One area where there is evidence of cumulative poor job quality is in relation to both pay and
pay promotion prospects. Social care not only offers low initial pay but also poor
opportunities for advancement (section I.3.2 above). These combinations of job
characteristics may be tolerated by older female care workers who may expect limited
chances of advancement wherever they move to in the labour market (Grant et al. 2005) but if
new recruits from under-represented groups are to be targeted, for example younger workers
and men, their expectations and aspirations for career and pay promotion will be different.
EWERC
Part I. The study context
40
Care work and women‟s skills
Care work is often regarded as low skilled by virtue of its low pay and the lack of formal
qualifications required for entry. As we argued above, this latter characteristic is in some
sense specific to the UK as other countries require acquisition of more formal qualifications
and have gone down the route of professionalising care work. However in all countries there
remain residual problems of low pay and status for this kind of work that are associated both
with a general tendency for women‟s work and skills to be undervalued in the labour market
(Grimshaw and Rubery 2007) and with a specific tendency for care work to be undervalued
due to its association with unpaid work undertaken by women in the home.
It is this potential for women (and indeed men) to acquire skills through informal experience
in domestic environments that in part enables the skills involved in care work to go
unrecognised. A third of respondents in McClimont and Grove‟s (2004) survey who were
recruited into care work had previous informal care experience. However, skill in care work
is not primarily technical but involves emotional labour or emotion work or more specifically
described by Bolton (2005) as „philanthropic‟ emotional labour, given as a gift. Moreover,
unlike other frontline service work where connections are transitory, care workers form real
attachments to users and suffer emotional dissonance if the relationship involves dealing
with, for example, abusive service users (Eaton 2000). The outcome is that care workers may
prefer to remain with users even if it is not convenient (Himmelweit 1999: 35) and may
become as England (2005) has suggested „prisoners of love‟ where their attachment to the
user may lead them into more intensive or more extensive work than they have been
commissioned to undertake or are rewarded for.
However, it is open to debate whether the relational and emotional content of this care work
should be emphasised over that of improving technical skills and training and encouraging
the professionalization of care work. The latter approach may make care work more
appealing to a wider range of groups including some men as they are reluctant to enter work
that stresses the need to have communication and social skills (Lindsay 2005). Furthermore,
although generic skills such as social skills and communication are emphasised as important
by employers when recruiting the relational aspects of work are not rewarded financially
(Hebson and Grugulis 2005). In other caring occupations it has been found that care work is
„contaminated‟ by the skill of caring, leading to undervaluation. Findlay et al. (2009) argue
that nursery nurses have much to gain from focusing on the educational element of their role
and a parallel strategy for care workers could be to focus on the emphasis on quality of life
and dignity that is crucial in good quality care. However, as we have seen, care workers and
users prioritise this relational aspect of care. If this aspect of the job is underplayed then there
is a danger of deterring the very people who users want to have care for them, as well as
exacerbating retention difficulties. Fagan and Anxo (2005) show that job satisfaction and
service quality are both adversely affected where staff have insufficient time, training and
other resources to meet the demands of emotional labour.
EWERC
Part I. The study context
41
I.4.3. Time and space in the recruitment and retention of a social care workforce
Time and space factors are important positive and negative factors in the recruitment and
retention of the social care workforce, particularly in domiciliary care where work is carried
out in a range of locations through repeat visits at key points in the daily and evening cycle.
The workforce is thus likely to be recruited from a localised pool of labour and this tendency
is reinforced by the use of informal methods of recruitment by employers and by the
relatively high job satisfaction found among care staff. In the Skills for Care survey, three
fifths of care workers (59%) said they definitely would recommend their job to a friend, and a
further one in four workers (24%) said they possibly would, meaning more than four in five
workers (83%) overall would recommend care work to a friend.
The mobilisation of local networks for recruitment does not necessarily mean people enter
the profession by chance as Lee-Treweek (1997) suggests. Rather, new entrants may feel they
know more about the job than if they had applied through formal channels without the
insights provided by the recommendation of a friend. But this form of recruitment may itself
set limits to the pool of labour on which the sector can draw.
While there may be a general case for those seeking work to expand their spatial horizons and
seek work outside their immediate area, this approach does not necessarily follow for
domiciliary care work given current patterns of work organisation and employment rewards
and guarantees. Travel to work time is always an issue for those in part-time work but where
the work is fragmented over the day, not necessarily continuous and involves travel within
the work day as well as from home to work the problems of expanding the geographical pool
of workers is even greater. While care homes are more able to recruit staff for regular hours
and for continuous shifts they also face the problem of operating on a 24 /7 basis and the need
for staff to work nights and weekends increases the problems of commuting any distance to
work as public transport may not always be available.
For such a feminised sector, and one so reliant on more mature women often with caring
responsibilities, it is important to recognise that the hours of work do not fit with standard
notions of family friendly or employee-flexible working time. Instead the hours of work are
set more with respect to user needs and may directly clash with family responsibilities,
including early mornings, teatime and evening shifts, weekend work and, in care homes,
night shifts. These working time arrangements further increase the likelihood that the work as
currently organised would only be considered „convenient‟ for local labour and may only fit
with quite specific family arrangements (for example where the partner is able to take the
kids to school or make the supper). This fits with early research on working time
arrangements in women‟s‟ jobs where what constitutes a convenient working time might be
highly family specific and would be reinforced by specific childcare and other arrangements
(Horrell and Rubery 1991a, b). However, in domiciliary care and to some extent in care
homes the workforce has to cope not only with working time patterns that do not conform to
standard family friendly arrangements but also with working time patterns that may be
subject to constant flux.
EWERC
Part I. The study context
42
I.5. Key research questions
The above review of literature on social care and the social care workforce has revealed a
range of key issues that have been used to inform the design of research questions for this
research project. We divide these into questions related to the LA commissioning
environment, questions related to the HR policies and practices of providers and questions
related to the recruitment and retention of care workers from the perspectives of both users
and care workers. Our final research question relates to the underlying policy issue, that is the
prospects for recruiting and retaining a larger and higher quality social care workforce to
meet increasing demands for social care under current institutional arrangements and
employment conditions.
LA commissioning environment
The LA commissioning environment was explored through an extensive postal survey in the
first stage of this project. The research questions identified for the second stage of the project
built upon this survey information but focused in particular on the following inter-related
issues.
1. How do those in the Local Authorities responsible for commissioning and/or
contracting make sense of the multiple, changing and potentially contradictory
pressures on commissioning policy?
The potential contradictions arise not only because of the need to contain costs while also
ensuring quality and adequacy of supply, but also because short term pressures may conflict
with longer term or strategic objectives to provide a more integrated service for older people
covering social care and health or even housing or to develop more user-centred service
delivery including the involvement of users themselves in the commissioning process.
2. What are the variations and trends in the specific characteristics of LA commissioning
and contracting practices, from price and contract to quality monitoring and provider
relations?
For both questions the key issue is the attention paid by LAs to factors that may impinge on
the recruitment and retention of the social care workforce. This attention may involve on the
one hand LAs monitoring their own commissioning policies to ensure they facilitate rather
than prevent providers adopting good HR policies. On the other hand the LAs may use their
positions in tendering, commissioning on contract monitoring to require providers to offer
good HR practices.
EWERC
Part I. The study context
43
HR policies and HR outcomes of providers
Our analysis of the role of providers in the recruitment and retention of the social care
workforce requires an initial mapping of the human resource practices in use within the
sector. These practices include:
recruitment and retention practices;
pay and reward systems;
work organisation and working time arrangements;
employee development and training; and
systems of performance management and employee voice.
A related objective is to map the range of approaches to human resource management
deployed by individual providers, measured across all these dimensions to HR practices. This
then sets the foundations needed for our key research questions as follows.
3. What is the current state of HR practices and outcomes in the sector?
What are the current employment practices and employment outcomes in the independent
sector and how do they differ between homes and IDPs.
4. What role do provider characteristics play in shaping HR practices?
In line with the findings from other studies we can anticipate several provider characteristics
to be potentially influential, including ownership (national, local chains, single
homes/agencies), sector (public, private, voluntary sector), size of establishment (eg. by
numbers employed) and different quality ratings, as determined for example by the CQC star
ratings.
5. What is the impact of the external policy and commissioning environment and the
local labour market demand factors on HR practices?
6. What is the combined impact of HR practices, environmental conditions, and
organisational characteristics on the quality of recruitment and retention outcomes?
These fifth and sixth research questions follow the analytical framework set out in figure I.1
by interrogating the inter-related effects of different environmental factors (related to LA
commissioning and local labour market conditions) and internal approaches to human
resource management on the overall outcomes for recruitment and retention.
Recruitment and retention from a care worker and user perspective
Due to the design of the project and to ethical issues relating to access to users, the research
questions that could be explored empirically within the project related primarily to the
experience of work from a care worker‟s perspective, although these were related to the
quality of care and the user experience wherever possible. The key research issues
EWERC
Part I. The study context
44
highlighted by the literature review and explored primarily through the stage three case
studies involving interviews with care workers were as follows.
7. What factors shape the recruitment of care workers?
8. What factors influence the retention of care workers?
The multiple factors include on the one hand the HR practices of providers and on the other
hand the personal motivations, expectations and experiences of the care staff. Both questions,
however, need to be set within the wider question of the nature of care work and its impact,
both positive and negative, on recruitment and retention, which leads to a further question as
follows.
9. Is care workers‟ job commitment influenced by the nature of the job and does it
involve trade-offs between „bad‟ and „good‟ aspects of the job?
In particular, we aim to identify and explore whether care workers enjoy opportunities to
provide good quality care and whether the relationship between „good‟ and „bad‟ aspects of
the job are in practice synergistic, with good HR practices potentially offering more job
satisfaction and better opportunities for good quality care from the perspectives of users and
care workers. In exploring this question we also consider whether the current care staff‟s
commitment to their work is linked to their particular interests and circumstances that may
not be easily generalised to an expanded labour pool.
Prospects for recruitment and retention under expanding demand: the policy
issues
The final research question relates to the context in which this research was funded, namely
the expectation of increased demand for the social care workforce, in relation to both quantity
and quality. We draw on the answers to all nine research questions to ask:
10. What are the prospects of meeting current and future increased demands for a social
care workforce under present conditions – that is without major changes in
commissioning arrangements, the policies of provider organisations and the
conditions of employment?
EWERC
Part I. The study context
45
I.6. Research strategy and methodology
I.6.1. The project research stages
The project to explore the recruitment and retention of the social care workforce involved
three main stages as detailed in table I.3: from local authority commissioning practices to HR
practices of providers to the experience of care workers. These are outlined in figure 1.7.
Figure I.7. The project stages
Survey of 92 LAs
Follow up study of
14 LAs
Part II
Telephone survey 115
provider establishments
10 national provider
interviews
20 case studies
of providers
Part V
98 care staff
interviewed
Part V
Parts III and IV
The first stage – a postal survey of LA directors of social services conducted by the PSSRU
unit in Manchester- has already been reported on (Hughes et al. 2009) and provided a
framework for the first part of stage 2, namely the selection of local authorities for follow up
interviews (stage 2a) and as sites for the telephone survey of providers (stage 2b)-. These
providers include domiciliary care providers (IDPs), residential and nursing homes in the
independent sector (homes) and local authority based domiciliary care providers (LADPs).
We also added a third element to stage 2, a survey of national providers (stage 2c).Stage 3
involved the selection of four LAs from our initial sample of 14 for cases studies of providers
with particular focus on the experience of care workers employed by these providers.
All three stages are described in more detail below. Table I.3 also provides a summary of
how and when user views and issue were taken up and explore within the project, with
further detail provided in the sections below. The project benefitted from the setting up of a
helpful, well informed and active advisory board (see box I.4 for information on the
EWERC
Part I. The study context
46
composition of the advisory board). This board met annually and an individual member of the
board provided valuable assistance at key stages, in particular in setting up a focus group of
users to inform the development of the case studies. The results of the project were presented
at each meeting and then the board was consulted on issues to bear in mind in developing the
next step.
Box 1.4: Membership of the Advisory Board
Social Care Consultant
Representative from Age Concern
Full-time Officer from Unison
Local Authority Service Director (LA not included in Stage 2)
Owner of a domiciliary care agency
Representative from Skills for Care
Representative from ACAS
2 lay persons
EWERC
Part I. The study context
47
Table I.3 Summary of project stages
Responsibility and project
stages
PSSRU and EWERC
Project development
PSSRU
Stage 1. January 2008
Dates/ responsibility /sample frame
Ethics approval sought from university ethics
committee –stage 1 by PSSRU, stages 2 and 3 by
EWERC.
Agreement form ADASS for stages 1 and 2 secured
by PSSRU.
Postal survey of LA directors of social services
Sample frame and number
of responses
Inclusion of user perspectives/ user issues
Formation of Advisory board including representatives
from all key stakeholders including users
92 responses
(149 LAs surveyed)
Information collected on consultations with users by
LAs and on flexibility in service provision at the level
of service user - one dimension to typology
Advisory board including users consulted on follow-up
questions on commissioning.
National user attitude surveys used to explore/validate
typology of LAs (see part II ).
Advisory board including users consulted on most
important care standards from a user perspective.
Challenges in meeting CQC care standards, importance
of continuity of care and attitudes to personal budgets
included in questionnaire.
Attitudes towards personalisation, care standards etc.
EWERC Stages 2 and 3
Stage 2a October 2008 to
June 2009
Follow up interview with key actors in LA
commissioning and contracting
14 LAs
(15 LAs approached)
Stage 2b. November 2008 –
February 2010
Telephone survey with independent providers and
LA inhouse departments in 14 LAs
(Targeted sample – 3 to 4 homes /IDPs plus LADP
per LA. Achieved in 12LAs, 2 undersampled)
115
(>300 providers
approached)
Stage 2c.
January 2010 - May 2010
Telephone survey with national chains Target 10all to have a branch within telephone survey – 5
IDPs, 5 homes
Case studies of providers
10
( 12 chains approached)
Stage 3
June 2009 to March 2010
Target cases studies in 5 providers in each of 4 LAs
- 5 care workers per provider
EWERC
20 case studies of providers,
(30 approached in total )
98 employee interviews
Focus group of care users to inform themes within case
studies. Two themes highlighted (see Box 1.6)
Part I. The study context
48
I.6.2. The stage one survey
Stage one of the project was designed to provide an overview of commissioning and
contracting practices in local authorities and to use that information to provide the basis for
the systematic selection of sites for stage two of the study. Data was collected from local
authorities with responsibility for social services through a postal survey distributed in 2008.
It comprised questions relating to the commissioning and contracting arrangements for
domiciliary care and care home provision and care management (care coordination)
arrangements for older people. The results of the first stage are reported separately in Hughes
et al. (2009). Ninety two of a total of 149 local authorities returned completed questionnaires,
a response rate of 62%.
To identify local authorities using common approaches to commissioning and contracting the
PSSRU study identified fourteen indicators relating to three domains of interest:
commissioning and contracting arrangements; employment practices; and flexibility in
service provision at the level of the service user. A cluster analysis was undertaken which
suggested the presence of seven types of local authority (table I.4). These were found to vary
in the level of activity in each domain of interest. For example, local authorities in type seven
were seeking to develop their commissioning activities, particularly in partnership with
health, and the processes associated with contracting; sought to reflect employment practices
in this context; and were striving to promote flexibility in service provision. Conversely, the
opposite appears to be the case in type four authorities. The remaining two thirds of the
sample displayed varying levels of activity in each of the three domains of interest.
Table I.4. Typologies of Local Authorities: Stage 1 of the project
Type (No. of
authorities)
1 (15)
2 (19)
3 (11)
4 (15)
5 (6)
6 (13)
7 (13)
Commissioning and
contracting arrangements
Medium
Medium
High
Low
Medium
Medium
High
Source: Hughes et al. (2009: p.9)
EWERC
Employment practices
Medium
Medium
Medium
Low
High
Low
High
Flexibility in service provision
at the level of the service user
Medium
Low
High
Low
Medium
Medium
High
Part I. The study context
49
I.7. The research methods for stage two
I.7.1. The local authorities
The selection of local authorities for the second stage of the research was driven by a range of
factors. These included the typology developed in the first stage; geographical spread; local
labour market conditions; and types of local authorities.
The seven cluster typology of local authorities influenced, first of all, the decision on how
many LAs to include in the second stage of the project. As the aim was to include both
independent sector domiciliary care providers and independent sector residential homes in the
telephone survey in each area, together with, where present, the inhouse domiciliary care
provider, 14 was considered the largest number of LAs that would allow for a normal sample
of six to eight independent sector providers within our target of around 100 to 120 achieved
interviews. Selecting a smaller number of local authorities would have raised two different
problems; first as the number of domiciliary care providers in one area was often quite
limited, we would not necessarily be able to achieve a sample much greater than four in some
cases, particularly if, as could be anticipated given the nature of the industry (see above), we
encountered difficulties in securing responses. Furthermore, as the indicated sample frame for
selection was the seven clusters of LAs generated by PSSRU‟s first stage survey, it seemed
appropriate to select two local authorities from each cluster. We made one variation to this
approach, namely we selected three from the largest cluster accounting for 19 local
authorities and only one from the smallest which included only six local authorities.
Three additional criteria of geographical spread, local labour market conditions and types of
local authorities were also taken into account in the selection to ensure that we covered a
broad range of types of external conditions and local authority characteristics. We contacted
the local authorities in stages as it was thought important to embark as soon as possible on the
telephone survey of providers after agreement had been secured from the local authority to
support their involvement in the second stage. For practical reasons, therefore, the
development of the local authority sample was done on a rolling programme with these
criteria in view. Of the 14 initially selected LAs, one did not agree to cooperate so that we
were able to achieve our initial selection of LAs with only this one exception. This was an
outer London borough and was replaced by another outer London borough in the same
cluster.
The characteristics of the achieved sample are shown in table I.5. Five local authorities were
located in the north, three in the midlands and six in the south including two in outer London.
The types of LAs were also spread over the main categories of shire counties (2), shire
unitaries (4) principal metropolitan (2) other metropolitan (4) outer London (2) with inner
London the main missing category (completion rates for both types of London boroughs were
lower at 50-54% compared to the highest rate of 83% for Principal Metropolitan Authorities
in the first stage survey). This variety of types of LAs is also reflected in the size of
EWERC
Part I. The study context
50
population: five had populations of under 250,000, five between 250 and 350 and four over
350,000 with two of these exceeding 600,000.
Table I.5. Characteristics of the selected LAs
LA
Population
size a
Type of LA
Cluster
Area
Female
employment
conditionsb
Female
part-time
earningsb
Labour
demand
conditionsc
AH
small
Shire unitary
2
South
5
M
Strong
ON
medium
Other
metropolitan
7
North
3
L
Weak
RT
medium
Outer London
3
South
3
M
Medium
RN
medium
Shire unitary
6
South
5
H
Strong
UY
medium
Other
metropolitan
1
Midlands
4
L
Medium
AD
small
Other
metropolitan
4
North
3
L
Weak
AW
small
Outer London
2
South
3
H
Medium
IL
medium/
large
Principal
metropolitan
7
North
2
L
Weak
OM
medium
Shire unitary
2
Midlands
2
L
Weak
XD
large
Shire counties
5
South
6
H
Strong
HD
medium/
large
Principal
metropolitan
6
North
5
M
Strong
TE
small
Shire unitary
1
Midlands
2
L
Weak
LK
large
Shire counties
4
South
6
M
Strong
RD
small
Other
metropolitan
3
North
4
M
Medium
a
Small <250k, medium 250-350k medium/large >350k<600k large > 600k
See appendix table I.A1
c
See appendix figure I.A1
b
The local labour market indicators that we focused on were those related to the potential
availability of a labour supply for care work, related to both quantity and wage level. As
most care workers are women we decided to look at the local labour market conditions for
women as the core indicator. The available labour supply for women is not necessarily fully
or appropriately captured by the unemployment rate as many women move directly from
inactivity to employment. We therefore took into account the unemployment rate, the share
of the working age population who are inactive but want a job and the achieved employment
EWERC
Part I. The study context
51
rate (see appendix table I.A1). We combined these measures to indicate the strength of
demand for female labour in the local labour market. Using a scale of 1 to 6 table I.5 shows
that as an average for the period July 2008 to June 2009 (source LFS NOMIS), the 14 local
authorities were spread rather evenly with each of the possible points 2 to 6 including at least
two of the selected local authorities. We also looked at evidence of pay levels in the LA area,
focusing on the median hourly wage for female part-time workers. We combined this
information to come up with a classification of local labour demand as strong, medium or
weak (see appendix figure I.A1). The two outer London boroughs are located in the medium
category: this reflects the polarised nature of London labour markets, with wide wage
inequalities even among women (median full-timers‟ pay being much higher relatively than
female part-timers‟ pay) and low employment participation by some ethnic groups.
Stage two interviews with Local Authorities
The local authorities selected for further study and for the telephone survey sites were
contacted via a letter to their director of Social Services. The letter drew the LA‟s attention
both to the approval of the project by the Association of Directors of Adult Social Services
(ADSS) (obtained at stage 1 of the project) and to the LA‟s prior participation in the postal
survey. This letter was followed up by a request for an interview with those responsible for
commissioning and contracting domiciliary care for older adults and residential and nursing
home care for older adults. Due to differences in organisational structures and arrangements
for commissioning and contracting, the person or persons interviewed and their
responsibilities varied between the LAs. However, in most cases we were able to interview
officers with responsibility for both commissioning and contracting - either in the same
person or by joint or separate meetings with relevant managers. In most cases only one main
interview was undertaken lasting between 90 minutes and two hours in most cases, and with
two or more officers in nine of the cases. Some follow up telephone interviews were
undertaken where key people – for example on training - were not able to be present. In one
case where contract implementation and monitoring was undertaken by a different
department from commissioning and outside of social services, the main interview was with
the contracting and monitoring group (the staff concerned had previously been located in
social care but had been moved to a general contracting department) and a follow up
interview by telephone undertaken with the officer with main operational responsibility for
commissioning. In one LA (AD) a second visit was made to interview a key actor at a
different site and in another (RN) sequential interviews were held with key actors. In all other
cases the interviews were joint and no attempt has therefore been made to separate out the
views of the different officers concerned. Table I.6 shows the number of interviewees and
area of responsibility in each LA.
The interviews at the LAs focused on two issues. First of all we asked for support for the
research team‟s study of external providers in the area. At a minimum we asked for lists of
current contracted providers and key contact names and email addresses if available. Many of
the LAs, however, also gave more active support by informing their providers through their
EWERC
Part I. The study context
52
forum, their newsletters or through emails that we would be contacting them and that the LA
was aware of and supportive of the research. In providing this support it was made clear to
the LA that they would not be able to have direct feedback on their own providers in order to
ensure confidentiality but they would be sent a copy of the report. The second purpose was
to follow up on the information already provided in the first stage survey and to explore in
more depth the relationship between LA commissioning and contracting and the recruitment
and retention practices of their providers. A semi structured interview schedule was used.
Table I.6. Local authority managers interviewed in stage two
LA
Initial interviews and
follow up interviews
Managers interviewed
AH
ON
1
1 joint + 1 telephone interview
Manager responsible for commissioning
Service director
Managers responsible for:
contracts
performance management
training
RT
1
Managers responsible for:
commissioning
contracts
quality
training
RN
2
Service Director
Manager responsible for contracts
UY
1 joint
Managers responsible for:
business services
training
commissioning
AD
2
Managers responsible for
commissioning
older people‟s services
AW
1 +1 telephone interview
Managers responsible for
commissioning
contracts
IL
2
Managers responsible for
commissioning
contracting
OM
1 + 1 telephone interview
Manager responsible for commissioning and contracting
XD
1
Manager responsible for commissioning and contracting
HD
1 joint
Managers responsible for:
older people‟s services
commissioning
HR
contract
TE
1 joint
Service Director
Manager responsible for commissioning
LK
1 joint
Managers responsible for
contracting
quality
training (2)
care homes
RD
1 + 1 telephone interview
Service Director
Manager responsible for commissioning
EWERC
Part I. The study context
53
I.7.2. The telephone survey
Design of telephone survey
For the telephone survey of providers, in each of the 14 LAs we aimed to include three to
four care homes, three to four domiciliary care providers and the LA inhouse domiciliary care
provider (where applicable). Within this sample we aimed for a mix between star ratings,
local and national providers and, in the homes, nursing and residential care.
The survey of providers took the form of a questionnaire administered mainly by telephone.
The questionnaire was designed for the owner, manager or person responsible for the day-today running of the home or independent domiciliary care provider. Because of the differing
nature of work organisation in domiciliary care and care homes separate questionnaires were
drawn up for each, but the greater part of the questionnaire was common to both. The
questionnaire was primarily aimed at three issues: identifying the current situation with
respect to the recruitment and retention of care staff; identifying the range of HR practices
used by the providers with potential relevance for recruitment and retention; probing the
providers‟ views of the influence of the external commissioning and labour market
environment on their HR policies and outcomes. The broad topics covered are:
general information on the establishment,
recruitment and retention of care workers,
pay,
organisation of work,
training and development,
relationship with LA
and experience of the policy and regulatory environment.
Parts of the questionnaire were designed to be filled in and returned prior to the telephone
interview. The rationale for this was twofold; firstly to enable the respondent to gather
certain information, particularly on workforce statistics, in advance, and secondly to cut
down the length of time managers‟ would need to spend on the telephone. A copy of the
questionnaire for IDPs and care homes combined is provided in the appendix to part I. The
shaded sections indicate those parts sent in advance.
Consultation with the advisory board/ users over inclusion of quality questions
During the first meeting of the project Advisory Board held in July 2008 a consultation
exercise was held with the members of the Board, including service users, and the members
of the research team to consider the care standards and associated indicators of best/quality
practice developed by PSSRU. Members each selected the 20 best practice indicators they
considered to be the most important determinants of quality in each area of service. Analysis
of the documents completed by members of the Advisory Board was undertaken to identify
the most frequently reported indicators of quality and best practice. However, this analysis
EWERC
Part I. The study context
54
suggested that there was no real consensus. A decision was therefore made to include the
whole set of CQC standards as the framework for questions on quality standards in the
telephone survey questionnaire.
Piloting the questionnaire
The questionnaire was piloted with the manager of a care home not situated in any of the LA
areas chosen for the study. The pilot interview took 35 minutes. Following the pilot
interview some minor changes were made to the questionnaire. Further changes were made
following suggestions from a local authority contracts manager.
Conduct of telephone survey
Following each of the local authority interviews we asked for lists of their current providers
of domiciliary care and care homes, with contact details where possible. Table I.7 shows the
numbers on the lists for each LA.
Table I.7. Potential sample of providers for telephone interviews
XD
Homes
147
IDPs
41
RN
63
10
AH
37
16
UY
62
10
OM
45
9
RD
35
15
HD
95
14
RT
27
7
AW
29
10
AD
51
10
IL
96
8
ON
40
22
TE
36
6
LK
145
80
Some LAs offered to smooth the way for us by informing their providers of our research, and
letting them know that they supported our project. The researchers made initial contact with
the managers by telephone and/or email to obtain their agreement in principle to take part
and, if possible, arrange a time and date for the telephone interview. Those who agreed were
sent further information about the project, and a factsheet about the implications of taking
part (including issues of confidentiality and anonymity) as agreed by the University of
EWERC
Part I. The study context
55
Manchester Research Ethics Committee. They were also sent the parts of the questionnaire
that had been designed to be completed in advance.
The managers were telephoned at the agreed time for the interview. If the manager agreed,
then the interview was recorded digitally but the responses to the questions were also noted
on the questionnaire as the interview progressed. The recorded interviews were used to check
responses and for additional qualitative data. Most of the interviews were between 45 minutes
and one hour in length.
Composition of the achieved sample
In practice the quota was obtained by contacting more than the target number of providers in
each LA area and stopping contact once the target number had been achieved. In order to
achieve the sample of 105 providers (excluding the inhouse providers) it is estimated that a
total of 303 providers were contacted. Furthermore it was often necessary to contact each of
these providers on several occasions. Even when an interview had been arranged the
researchers often found that the manager was not available at the allotted time, and the
interview would have to be re-arranged (several times in some cases). To some extent these
difficulties reflect the nature of managerial work in domiciliary care and care homes where
diaries tend to be „fluid‟ and managers are often, for example, required at short notice to meet
with service users and families, deal with practical problems or cover for absent staff. The
composition of the achieved sample is shown in table I.8.
Table I.8. Composition of the achieved sample
Homes
IDPs
LADPs
Total
XD
5
4
1
10
RN
4
4
1
9
AH
4
5
0
9
UY
3
3
1
7
OM
4
3
1
8
RD
4
3
1
8
HD
4
4
1
9
RT
3
4
0
7
AW
2
3
0
5
AD
4
4
1
9
IL
4
4
1
9
ON
4
4
1
9
LK
4
6
1
11
TE
4
1
0
5
Total
53
52
10
115
EWERC
Part I. The study context
56
The table shows that the target sample for IDPs and care homes was achieved in 12 of the 14
LAs. In the case of TE it was difficult to achieve the target sample of IDPs because of the
limited number contracted by the local authority. On the other hand the target sample was
overachieved in three LAs. Two of the LADPs (AW and RT) had no inhouse domiciliary care
provision, but ten of the remaining twelve were included in the sample.
Additional interviews with national providers
Stage two of the project also included interviews with senior managers of national providers
of care homes and domiciliary care. We decided to aim to interview five national providers of
care homes and five national chains of IDPs. Our priority was to include national providers
that were represented in our telephone survey of providers (all of the ten achieved
interviews). The response rate was relatively high with twelve national providers contacted to
achieve the sample of ten. The interviews were semi-structured; eight of the interviews were
conducted over the telephone, and two were face-to-face interviews. One of the telephone
interviews was conducted with two managers simultaneously by conference call. The
interviewee sample by job title/area of responsibility is shown in box I.5.
Box I.5. National Provider Interviewees
Homes
Recruitment Director
HR Director (2)
Group HR Director
Corporate Services Director
IDPs
HR Director
Commercial Director
Managing Director and Head of Recruitment and
Retention
Managing Director
National Recruitment Manager
Coding and analysis
The responses to the telephone survey were entered into an SPSS data file. Efforts were made
to complete missing data, particularly where the respondents had not returned the advance
questionnaire but a number of the providers still did not complete the information. For those
who did complete the advance questionnaire (96 out of 115) the information was of a higher
quality than could have been achieved in one telephone interview.
Cross-tabulations were used to produce the descriptive statistical tables in part III of the
report to provide an overview of recruitment and retention in the selected providers and to
EWERC
Part I. The study context
57
document the rage of HR practices in use. To compare the use of HR practices between
individual providers and between groups of providers - by organisational and local authority
characteristics- the data on HR practices and outcomes were converted first into indicators
and then into subindices and indices to represent a range of practices from poor to good with
the value 1 for the best practices. Part IV, including the extensive appendix tables, gives more
detail on how these were constructed and used, and provides further analysis of the telephone
survey data. Multivariate analyses were also carried out using these indicators and indices.
EWERC
Part I. The study context
58
I.8. The research methods for stage three case studies
I.8.1. Rationale for the case-study approach
The role of the cases studies in the project design was to provide a more in-depth exploration
of how the HR practices of providers influenced recruitment and retention and to do this
through exploring the experience of work among the care staff. While the cases studies were
designed to explore the care workers‟ experience of the providers‟ HR practices it was also
recognised that many factors that shape recruitment and retention may be related to their own
personal and social circumstances. While some of these may be influenced by the employer,
others may not be. An understanding of some of the personal motivations and expectations of
those who enter the sector could help providers to put in place HR practices that can facilitate
a smoother entry into the sector and a more long term commitment to stay. The case-study
data was thus designed to provide more in-depth data on a range of areas including:
firm level practices and their impact on recruitment and retention in the care sector;
the characteristics and experiences of care workers including their entry into the
sector, their desire to stay or leave, and the levels of satisfaction with key aspects of
their employment;
the linkages, where they exist, between commissioning practices, employer practices
and job quality issues for care workers;
differences, where they exist, between the views of established staff and those of new
recruits to gauge potential problems in retention in the sector;
linkages, where they exist, between the provision of good quality care and good
quality care jobs.
I.8.2. Design of the case studies
Focus group with users
Involvement of service users was sought by holding a focus group with users in February
2009 under the auspices of Age Concern. Two researchers from the project and four service
users, including one member of the project advisory group, attended. The aim of the focus
group was to solicit care users‟ views on the most important issues to follow up on the
linkage between recruitment and retention issues and the quality of care. Issues discussed
were:
the attitudes, attributes and quality of care staff
working conditions
the organisation of care delivery
The views of the focus group on these issues were used to inform the case-study survey
design as outlined in Box I.6.
EWERC
Part I. The study context
59
Box 1.6. Focus group held with care users
During the focus group care users identified a number of issues relating to quality of care, the
working conditions of care workers and the organisation of care delivery and these themes
were integrated into all case study interview schedules. Some of the issues identified relating
to low pay and training were anticipated but other themes were unexpected. For example, the
focus group revealed that care users often have contradictory expectations of care workers;
they expect both the informality of friendship and the formality of a host/guest and
employer/employee relationship. To explore this further in the case study interviews we
included a section entitled „Relationships with users‟ in the interview schedule. This includes
questions that asked care workers whether they find it is easy to meet the expectations of
service users and whether they find it difficult to fulfil the different roles of both a care
worker providing a service and a friend. This theme is explored in part V which reveals that
care workers are constantly having to negotiate this difficult balance and when done well this
appears to improve both the working experiences of the care workers and the feedback they
receive from the care users.
Another important theme that emerged in the focus group with users related to the
organisation of care delivery and, in particular, the care users‟ concern about timekeeping,
timing of visits and care workers‟ capacity to deal with unanticipated events when timings of
visits are tightly defined. These issues were included in a section entitled „Doing the job‟. We
asked care staff about the lengths of visits, any difficulties that arise when carrying out tasks
in defined times and what happens when unforeseen events mean visiting schedules cannot
be met. These are particularly revealing questions as they ensured that care staff gave
concrete examples of what they were expected to do in the times they were allotted and the
problems that could arise because of the unpredictability of service users‟ needs. Specific
stories about the day to day reality of caring may be more informative than generalised views
about „being a care worker‟. Some of the difficulties and frustrations of working as a care
worker are revealed in responses to these questions as well as the good practice in the sector.
We therefore feel involving care users at the preliminary stages proved invaluable in ensuring
that the case studies generated meaningful data on the linkages between quality of care and
recruiting and retaining a quality workforce.
Design of the cases studies
In stage three of the project we aimed to interview five staff in five provider organisations
(two homes, two IDPs and one LA inhouse provider) in each of four local authority areas.
The interviews were semi-structured and separate interview schedules were designed for care
workers and supervisors. The interviews with care workers covered background information
EWERC
Part I. The study context
60
and work history of the employee, recruitment, pay, working time, job content, relationships
with service users, communication with management, training and development, career
prospects and future plans for working in care or elsewhere. Similar topics were covered in
the supervisor interviews, but we also asked additional questions about their supervisory role.
I.8.3. Selection, conduct and analysis of the case studies
Selection of LA areas for case studies
The selection of LA areas for case studies was done on a „rolling‟ basis which started before
the completion of the LA interviews in stage two. This was necessary in order to ensure
completion of the fieldwork within the project schedule. It was not, therefore, possible to use
the analysis of all 14 LAs as a basis for selection from the outset. We did, however, aim for a
good contrast between the four areas in terms of high/low wage areas, geographical areas,
local labour markets, a variety of LA commissioning approaches and fee levels. The four
chosen were IL, ON, XD and RN. IL was identified as a very low fee payer, RN a medium to
high payer and XD a high payer. These LAs also provided examples across the range of types
of LAs as subsequently classified through our interview material even though this typology
was not available at the time of selection of the first two LAs ( see section II. 3): XD and RN
feel into the partnership category, IL the cost minimising and ON fell into the mixed
category. IL and ON are in the north of England, RN and XD in the more affluent south. IL,
ON and RN are urban, or mainly urban, and XD covers a mixed urban and rural area. Parts II
and V give more details of the selected LAs.
Selection of case study organisations
In stage two of the project we asked the managers at the end of the telephone interview
whether they would agree to their establishment taking part in the project at a later date as a
case study. When selecting the case studies we approached those in the four selected LA
areas who had agreed in principle. We approached 30 organisations at this stage in order to
achieve the target sample of 20.
Selection of staff to be interviewed in each case study
The case studies primarily focused on the experiences of care workers within organisations
where a large amount of information had been collected through the telephone survey with
respect to their working conditions. In each case study we sought to interview two relatively
new recruits, and two longer serving, more senior members of staff. We also interviewed
someone with supervisory responsibilities, in addition to the four care workers. All the
telephone interviews with managers for the case-study organisations were fully transcribed
and analysed in detail to provide the organisational context in which to locate the care
workers‟ interviews. Nevertheless, the case studies were somewhat more employee-focused
EWERC
Part I. The study context
61
than was originally planned but the problems experienced in gaining cooperation from
managers to give of their own time for the telephone surveys made it very difficult to require
further cooperation from management as a condition for participation in the case study stage.
The stronger focus on the experiences of care workers themselves could be considered a
strength of the case-study data as it was revealing of a range of key issues in recruitment and
retention that is not visible from a management perspective.
Conduct of the case studies
A time and date convenient for the case study interviews was arranged with the manager in
each case. The managers were asked to identify five potential interviewees: we informed the
manager that the interviewees would be offered £ 15 shopping vouchers as an incentive to
take part and this proved very successful in helping to recruit interviewees. One or two
researchers travelled to the case study site on the agreed date, and individual interviews took
Table I.9. Composition of the achieved case studies
ON
ON.D.1 DN
ON.D.3 DN
ON.HN.1 BS
ON.H.2.ML
ON.DIH.1 DP
IL
IL.D.1 CN
IL.D.2 DL
IL.H.3 BN
IL.H.4 BS
IL.HIH.1 CP
XD
XD.D.1 CN
XD.D.3 CN
XD.HN.4 DN
XD.H.5 BS
XD.DIH.1 DP
RN
RN.D.1 CN
RN.D.2 CN
RN.H.1 AL
RN.H.3 AN
RN.DIH.1 DP
EWERC
Type
CQC
Star
rating
Local/
national
Private/public/
voluntary
Total no.
of staff
Established
IDP
IDP
Home with
nursing
Home
LADP
2 star
3 star
2 star
National
National
Local
Private
Private
Private
102
30
24
2005
1983
1979
1 star
3 star
Local chain
Local authority
Private
Public
52
128
2001
Registered 2003
IDP
IDP
Home
Home
LA Home
2 star
2 star
2 star
2 star
2 star
National
Local chain
National
Local
Local authority
Private
Private
Private
Private
Public
70
210
25
30
2008
1995
2004
1998
Registered 2003
IDP
IDP
Home with
nursing
Home
LADP
3 star
2 star
3 star
National
National
National
Private
Private
Voluntary
50
60
113
2004
Registered 2004
2006
3 star
2 star
Local
Local Authority
Voluntary
Public
26
130
1947
1947
IDP
IDP
Home
Home
LADP
2 star
2 star
3 star
2 star
3 star
National
National
Local chain
National
Local Authority
Private
Private
Private
Private
Public
60
52
23
24
150
Registered 2004
2005
1979
2003
Registered 2004
Part I. The study context
62
place in a location which ensured privacy. Before each interview the interviewee was given
printed information about the project, an information sheet on ethical issues approved by the
University of Manchester Research Ethics Committee, and asked to sign a form consenting to
be interviewed and for the interview to be recorded. The interviews lasted around 30 to 40
minutes. All recorded interviews were fully transcribed.
Composition of achieved case studies and staff interviewed
In all four of the selected LA areas we achieved the target number of case studies, i.e. two
homes, two domiciliary care agencies and one local authority provider. Four of the LA
providers were domiciliary care providers and one was a local authority care home. Table I.9
shows the characteristics of the case studies by type, star rating, local/national,
public/private/voluntary, total number of staff in the home or branch and date established or
registered.
Table I.10. Composition of staff interviewed
ON
ON.D.1 DN
ON.D.3 DN
ON.HN.1 BS
ON.H.2.ML
ON.DIH.1 DP
IL
IL.D.1 CN
IL.D.2 DL
IL.H.3 BN
IL.H.4 BS
IL.HIH.1 CP
XD
XD.D.1 CN
XD.D.3 CN
XD.HN.4 DN
XD.H.5 BS
XD.DIH.1 DP
RN
RN.D.1 CN
RN.D.2 CN
RN.H.1 AL
RN.H.3 AN
RN.DIH.1 DP
Total
Less experienced
care workers
Experienced care
workers
Supervisor
Total
2
1
2
2
2
2
2
3
2
1
3
1
1
1
5
5
4
6
5
2
2
2
2
2
1
3
2
2
2
2
1
1
1
1
5
6
5
5
5
2
1
2
2
2
2
3
2
2
2
1
1
1
1
1
5
5
5
5
5
2
2
2
2
2
36
1
2
2
1
2
40
1
1
4
5
4
4
5
98
1
1
22
Table I.10 shows the numbers of staff interviewed at each organisation. In most cases the
target number was achieved. In two cases we interviewed more than the target number,
because more than the requested numbers arrived for interview, and it would have been
EWERC
Part I. The study context
63
difficult not to interview them all as they had been promised shopping vouchers. In five cases
we interviewed fewer staff than we needed, or did not achieve the desired mix of experience.
In the IDPs in particular the number and experience mix of interviewees was constrained by
the practicality of staff coming in to the office in their spare time to be interviewed. In one
home one interviewee was working as a cook, but was interviewed because she had daily
contact with residents and had previous experience of care work. This interview is not
counted in the total sample.
Analysis of the case studies
In total we conducted 98 interviewees and the desired split between new recruits and
established staff was achieved (see table I.10 and table I.11). Although we tried wherever
possible to include a mix of care workers in the sample that are underrepresented in the care
workforce, including men, younger workers, care workers from different ethnic background
and migrant workers, the sample was predominantly female and white British and over half
within the 30-49 age category (see Table I.11).
Table I.11. Sample composition by job tenure
1
Sample No.
2 yrs or under
(%)
2-5 years
(%)
6-10 years
(%)
Over 10 years
(%)
IDPs
381
71
21
3
5
Homes
38
50
26
13
11
LAs
20
25
25
20
30
Total
1
53
24
10
12
96
Two IDP care workers- no information
Table I.12. Sample composition by age: all and new recruits
Under 30
(%)
Total
New
recruits
30-49
(%)
Total
New
recruits
50-59
(%)
Total
New
recruits
Sample
No.
No.new
recruits
IDPs
40
21
28
33
53
52
18
Homes
38
12
26
42
53
42
LAs
20
10
10
10
60
50
Total
98
43
23
30
54
49
Over 60
(%)
Total
New
recruits
14
3
0
16
8
5
8
30
40
0
0
19
19
3
2
For each organisation we developed a template where relevant extracts and quotations
relating to a number of themes were recorded for each interviewee. An inductive approach
was adopted: while some themes were determined by the interview schedule and the research
questions of the project, others were unanticipated and were generated by the responses of
interviewees. For example, we did not anticipate the extent of the use of family and social
networks in shaping entry into the sector and when this theme started to arise in many of the
EWERC
Part I. The study context
64
interviews we ensured all interview data had been analysed with this theme in mind. The
template facilitated comparisons between providers within case study local authorities and
across local authorities. It also allowed comparisons between new recruits and well
established staff as well as staff with supervisory roles and coordinating roles. The templates
also allowed us to quantify some of the trends found in the case study data. While the aim of
the case study data was to explore the care workers‟ attitudes and experiences using
qualitative techniques, the number of interviews also allowed us to identify some general
trends. This opportunity was particularly useful because of the limited data on care workers
as a group. While the case studies of each organisation were interesting in their own right, for
this project the comparisons between cases within and across different local authorities was
also significant as this could help tease out any explanatory factors that could account for any
similarities or differences across the sector. Of particular interest here were the two case
studies of national chains operating branches under two different local authorities as this
offered insights into the relative impact of company policy versus commissioning and local
labour market conditions on HR practices.
I.9. The plan of the report
This first part of the project report has described the research framework, reviewed the
relevant literature, formulated the key research questions and provided an overview of the
methodology adopted and the samples achieved. The organisation of the rest of the report is
as follows. Part II describes the commissioning and contracting practices identified in the 14
selected LAs and provides a typology or classification of commissioning practices. Part III
provides a mapping of the current HR practices according to the telephone survey of our
achieved sample of 115 providers, analysed by IDPs, homes and LADPs. Part IV explores the
role of LA commissioning practices, local labour market conditions and characteristics of
providers in accounting for variations in HR practices and HR outcomes. It also explores
relationships between providers and LAs from the providers perspectives, including those of
national chains. Part V also explores the impact of different LA commissioning
environments and different provider HR practices but this time from primarily a care worker
perspectives. Here the role of work organisation and staff recruitment and retention in
providing quality of care is also emphasised. Part VI draws together the different pieces of
evidence to address our nine research questions including the pointers for public policy to
promote the recruitment and retention of the social care workforce.
EWERC
Part II. Commissioning and contracting in the selected local authorities
65
II. Commissioning and Contracting in the
Selected Local Authorities
One of the project‟s key hypotheses is that the commissioning and contracting practices of
Local Authorities shape the environment in which private and voluntary sector providers are
able to seek to recruit and retain the social care workforce. Here we explore the
characteristics of these commissioning and contracting practices in the fourteen LAs that we
selected for further study. The chapter is divided into four parts: in II.1 we combine
information from the first stage survey of LAs with information from the second stage LA
interviews to provide a quantitative analysis of the key characteristics of commissioning and
contracting practices. In II.2 we analyse the qualitative material based on the interviews with
key actors in commissioning and contracting in stage two of the project to explore the
different pressures placed on LAs and to identify the approach taken by our selected LAs. In
II.3 we draw together the two sources of information to provide a categorisation of the
approaches by the selected LAs to be used to inform our analysis of the telephone survey of
providers. Finally in II.4 we use our classification of LAS to explore variations in user
satisfaction scores in the home care survey of LAs 2008-9 (NHS Information Centre 2009a).
II.1. Key commissioning and contracting characteristics
II.1.1. Extent and form of external commissioning and contracting
Extent of outsourcing in domiciliary care
The fourteen LAs all contracted the majority of their domiciliary care work to independent
providers (see table II.1 column 1)10. The shares outsourced varied between 55% and 100%:
two outsourced under 60%, five between 60 and 80%, five over 80% but still with some
inhouse and two outsourced 100% with no inhouse provision. This level of outsourcing was
relatively new in some cases with 6 reporting that the majority was outsourced only after
2005, five between 2000 and 2004 and three before 1999. There is no link between the date
of outsourcing and current levels: two that started early have relatively low levels of
outsourcing and two that moved late to significant outsourcing have ratios above 80%. There
is also a continuing tendency for the LAs to increase the share of work outsourced with
10
This share is higher by contact hours than by price due to higher unit costs for LA provision. Most of the LAs
when asked in interview gave the information on an hours basis; this difference in measurement in part explains
the higher levels of reliance on external providers in our follow up interviews from the first stage survey.
EWERC
Part II. Commissioning and contracting in the selected local authorities
66
increases in several between the stage one survey and the stage two interview and six LAs
had plans for further increases. Only one anticipated a possible reversal of this trend if more
emphasis was placed on re-ablement; this was an LA that currently outsourced over 90% but
its inhouse provision, joint with the NHS, was focused on re-ablement.
Of the twelve still with some inhouse provision, five were providing both specialised and
general domiciliary care from its inhouse provision while seven had already moved towards a
specialised focus for inhouse provision (Table II.1 column 3). Two LAs (OM, TE) had
changed from more general to more specialised inhouse provision between the first stage
survey and the second stage interview. In six LAs only inhouse units were engaged in
intermediate and/or mental health elderly care (table II.1. column five). In the remaining
eight, six recorded involvement by both inhouse staff and independent provider staff while
two, those with no inhouse provision, relied entirely on independent providers.
Involvement in unsocial hours working is common across both LADPs and IDPs. All LADPs
were involved in daytime, evening and weekend work. Likewise, all independent providers
were involved in these forms of work. The majority of evening and weekend work is likely to
be carried out by the independent sector given their high share of total care hours and
expenditure. The main differences among LAs were found in night work (table II.1. column
six). One carried out no night work by either type of staff. A further two had no inhouse
facility and five more undertook no night work, leaving six LAPDs that were involved in
night work. Three of these six did not involve any IDPs in night work. In the 10 LAs where
IDPs were involved, this concerned all providers in five LAs but only some providers in the
other five. Overall, there is a strong reliance on the IDPs for the unsocial hours working but
as inhouse operations have become more specialised, there is also a high involvement among
the remaining inhouse staff.
Among our LAs all but three commissioned jointly for intermediate care with the NHS (table
II.1. column seven). The three exceptions had either no or very limited inhouse provision.
This may suggest that the lower the direct involvement of LAs in service provision, the less
likely their involvement in joint commissioning. While the stage one survey found that three
LAs did most of their commissioning with the NHS all the rest recorded an involvement of
under 20% except for one other at 40-60%. One LA (AH) had become fully integrated with
the NHS between the stage one survey and the stage two interview. In several cases there
were plans for more involvement, even in one case when currently there was no involvement.
Independent care staff were involved in providing jointly commissioned services in half of
our LAs (table II.1. column eight).
EWERC
Part II. Commissioning and contracting in the selected local authorities
67
Table II.1 Key commissioning and contracting characteristics for domiciliary care
LA
%
Outsourced
Planned
change to
outsourcing
AH
80%-99%
Less
Specialised
Both LA and IDPs
IDPs only
High
Joint commissioning but no IDP staff involved
ON
60%-80%
More
Specialised
LA only
IDPs only
Low
IDP staff involved in more than one area
RT
100%
No change
None
IDPs only
IDPs only
Very low
No joint commissioning
RN
80%-99%
No change
Specialised
Both LA and IDPs
LA only
High
Joint commissioning but no IDP staff involved
UY
≤60%
No change
Mixed
Both LA and IDPs
LA only
Low
IDP staff involved in more than one area
AD
60%-80%
More
Mixed
LA only
IDPs only
Low
IDP staff involved in more than one area
AW
100%
No change
None
IDPs only
IDPs only
Very low
No joint commissioning
IL
60%-80%
More
Mixed
Both LA and IDPs
High
Joint commissioning but no IDP staff involved
OM
80%-99%
More
Specialised#
LA only
Both LA
IDPs
Neither
Low
IDP staff involved in one area
XD
≤60%
No change
Mixed
Both LA and IDPs
LA only
High
IDP staff involved in more than one area
HD
≤60%
More
Specialised
LA only
IDPs
Low
IDP staff involved in more than one area
TE
80%-99%
No change
Specialised#
LA only
and
Medium
No joint commissioning
LK
80%-99%
No change
Specialised
LA only
and
Low
Joint commissioning but no IDP staff involved
RD
60%-80%
More
Specialised
Both LA and IDPs
Both LA
IDPs
Both LA
IDPs
IDPs only
Low
IDP staff involved in one area
*Integration with the NHS:
Role of the
LADP
Involvement in
night work
High = ≥60% intermediate care joint commissioned
Medium = >20%≤60% intermediate care joint commissioned
Low = ≤20% intermediate care joint commissioned
Very low = no joint commissioning of immediate care
# Recent change from general to specialised
EWERC
Involvement in
intermediate and/or
mental health care
and
Integration
with the
NHS*
Independent sector staff involved in joint
commissioned intermediate care
Part II. Commissioning and contracting in the selected local authorities
68
Number of providers and contract form in domiciliary care
The number of domiciliary care providers that the LAs contracted with at the time of the
stage 2 interview varied w from five to 35 (table II.2. column two). The extent of additional
spot contract arrangements varied between LAs, complicating comparisons of the number of
actual providers. For example, one LA (AW) had intended to use almost exclusively two
main providers for each of its two main geographical areas but due to major post contract
problems with one of the providers, much of the work was being undertaken by providers
with only spot contract arrangements with the authority.
Table II.2 sets out the different types of contracts and number of providers under each type
that were active within the fourteen LAs. One of the major areas of change, both over recent
years and planned for the future, was the switch from block contracts to preferred providers.
The most common form now of contracting is through selected preferred providers but often
contracted under a framework agreement or under a cost and volume contract but with no
guaranteed hours. This applied to nine of the LAs. The five other LAs used block instead of
preferred providers but only four of these put most of their work though block contracts. The
fifth LA had a large rural hinterland served by a large number of spot contract providers.
Compared to the stage one survey results for early 2008, the number of our LAs with block
contracting had reduced by late2008/2009 from six to four. A further four had also recently
moved from block to preferred provider, three of them in 2007/8 (table II.2. column six).
Two of the LAs using blocks in 2008/9 had in fact moved to block contracting in the
relatively recent past (since 2005), so that the direction of travel was not all in one direction.
Furthermore, the move from block to preferred provider was not in all cases associated with
an increase in the number of providers. Two LAs had in fact reduced providers while moving
from block to preferred provider (AH, AW). One of these LAs (AH) also described the new
arrangement as a „new block‟ contract, that is involving similar commitments to block but
without minimum guaranteed hours. Overall there is quite a diversity not only in the number
of providers contracted with but also the direction of change; eight had explicitly sought to
decrease the number of providers it mainly dealt with while four had sought to increase the
number (and only two recorded no change). The outcome of these various strategies had also
resulted in quite a diversity among the LAs in the extent to which they were primarily reliant
on relatively few or quite a large number of domiciliary care providers to deliver the bulk of
their domiciliary care. Thus four relied on five or fewer, four on six to ten providers, four on
11 to 20 and two on more than 20.
All the LAs had divided up their tenders by geographical areas but still had adopted quite
different strategies with respect to the designation of providers by area. In some LAs (at least
seven) there was only one provider per area. In others there was a main provider and one or
more second tier providers (either spot providers or preferred providers who had a main and
one or two more subsidiary areas). Only three had a number of main providers per area (two
had three and one five). The characteristics of the areas had an impact on the tender
arrangements in some cases. For example, XD required bidders to choose an easy to service
EWERC
Part II. Commissioning and contracting in the selected local authorities
69
area and a difficult to service area as an explicit means of increasing the supply of services in
the more rural areas.
Table II.2. Characteristics of LAs’ organisation of domiciliary care contracting.
LA
Number of
external providers
of domiciliary care
LA contracts with
Number
of block
contracts
Number
of
preferred
providers
Number
of spot
providers
Recent changes in
block contracting
Experience of
TUPE
transfer
AH
5
0
5
10
Away from block
none
ON
17
0
10
7
Away from block
none
RT
7
1
6
0
LADP to IDP
10
0
10
0
No change some
block
No change no block
RN
UY
10
0
6
4
none
AD
10
0
4
6
No change some
block
To block
AW
10
0
2
8
Away from block
IL
9
0
9
0
Away from block
LADP to IDP.
IDP to IDP
IDP to IDP
OM
17
0
17
0
Away from block
none
XD
35
11
0
24
To block
none
HD
17
10
0
07
none
TE
5
0
5
0
LK
30
30
0
50
No change some
block
No change some
block
Away from block
RD
14
0
6
8
Away from block
none
none
none
IDP to IDP
none
In three of the LAs, inhouse staff had been TUPE transferred to external agencies and in one
case the same staff had been TUPE transferred a second time to a new agency (Table II.2.
column seven). The TUPE regulations protect the terms of employment of transferring staff,
resulting in continued LA pay and non-pay conditions which are more generous than in the
private sector (see part 1). In all three cases these arrangements were still having a significant
impact upon the fees paid to the providers concerned. TUPE arrangements affected not only
ex-LA employees, but also cover staff moving from one independent sector provider to
another. In at least three LAs there were examples of staff TUPE transferred from one agency
to another due to changes in the providers, either because of outcomes of tenders or because
of closures of providers.
EWERC
Part II. Commissioning and contracting in the selected local authorities
70
Commissioning and contracting of care homes
Twelve of the fourteen LAs still provided some residential home care inhouse (table II.3.
column two). Those without LA provision included one which also had no domiciliary care
but the second LA with no domiciliary care was still providing a range of forms of inhouse
residential care. The second LA (XD) with no inhouse provision had transferred its homes to
one specific provider. Ten of the LAs provided short term intermediate care and ten
dementia-specific short term care (though not the same ten as two provided intermediate and
not dementia and two vice versa). Four of the twelve with some inhouse provision only
provided short term care of some kind (including short term care in a resource centre
although this was always combined with either intermediate or dementia short term care or
both) (table II.3 column three). The remaining eight were involved in some forms of long
term care: all eight provided dementia long term care and three provided resource centre
based long term care but none provided short or long term care under the heading of other,
suggesting all had withdrawn from standard residential care provision.
Ten LAs have some block purchase contracts with independent providers for residential care
of various kinds (Table II.3 column four). While the purposes of the block purchases are
spread across dementia, respite and intermediate care- with only two mentioning other
purposes (non specific and carer support respectively), the proportion of the residential care
accounted for by block purchases was most commonly under 10% ( six LAs). Two LAs (IL
and XD) had shares above 40% while two (AW and LK) had shares at 20-29% and 10-19%
respectively. The high share at XD was due to the transfer of its homes to a specific provider.
In IL intermediate care is contracted out through a block contract although consideration is
being given to changing the inhouse provision form long term care to short term care which
might reduce the use of block contracting. With these exceptions, contracting was thus
mostly on a spot basis, usually according to the preferences of the user. LAs usually had a list
of homes that they were prepared to place users in; in some cases they had a policy of only
placing users in homes above a minimum CQC star rating (either one or two star) but
sometimes they would still make exceptions if there was either a shortage of beds or a strong
reason why the user preferred the home even though it had a poor quality rating. Under this
spot contract policy the number of homes that the LA was currently contracting with was
normally quite large although the numbers quoted varied from 30 or so to 400. Where the
area bordered other residential areas- for example in the outer London boroughs- there was
more use of homes outside the area. In some cases (RD) this was a planned strategy as labour
costs were lower across the border so that those not able to pay top up fees were encouraged
to choose a home outside RD.
EWERC
Part II. Commissioning and contracting in the selected local authorities
71
Table II.3 Commissioning and contracting of residential care
LA
Local authority is a
provider of
residential home
care?
Type of residential care
provided
(all intermediate,
dementia or resource
centre – no ‘other’)
LA has any block
purchase
arrangements with
residential or nursing
homes
Estimate of block
contracting as share of
total beds by external
providers,
Residential care price per
week for older people
provided by others.
PSS EX1 Return for 2007-081
Higher fees for
higher quality
homes
AH
Yes
Long and short term
Yes
1-9%
High >£460
No
ON
Yes
Long and short term
Yes
1-9%
Low £350-£390
No
RT
Yes
Long and short term
Yes
1-9%
Medium £390-£460
No
RN
Yes
Short term only
Yes
1-9%
High >£460
Yes
UY
Yes
Long and short term
No
N/A
Medium £390-£460
Yes
AD
Yes
Long and short term
Yes
1-9%
Medium £390-£460
Yes
AW
No
None
Yes
20-29%
High >£460
No
IL
Yes
Short term only
Yes
40-49%
Very Low <£340
No
OM
Yes
Long and short term
No
N/A
Very Low <£340
Yes
XD
No
None
Yes
50% or more
High >£460
No
HD
Yes
Short term only
Yes
1-9%
Low £340- £390
No
TE
Yes
Short term only
No
N/A
Low £340- £390
Yes
LK
Yes
Long and short term
Yes
10-19%
High >£460
No
RD
Yes
Long and short term
No
N/A
Low £340- £390
No
1
Definition- based on unit costs residential care for older people provisions by others Unit Costs Summary Sheet PSS EX1 return 2007-8 annex council tables.
http://www.ic.nhs.uk/statistics-and-data-collections/social-care/adult-social-care-information/personal-social-services-expenditure-and-unit-costs:-england-2007-08
EWERC
Part II. Commissioning and contracting in the selected local authorities
72
II.1.2. Provision of fees for externally provided care
Fees for domiciliary care
Six of the LAs set a fixed fee per hour when they published the tender for IDPs and all
providers were contracted at that rate11 (table II.4. column two). In the remaining eight cases
fees varied across providers according to the price at which different providers tendered to
provide services. Those paying fees according to tender price were much more likely to ask
for the wage element to be separated out at tender: this applied to seven of our LAs and an
eighth that asked for it at short list stage. Only one of these eight (LK) paid a standardised
fee. The practice thus seems to be more about the LAs wanting additional information if it
were to pay above a standard rate than a policy to select on the basis of fair treatment of staff.
Only two of the LAs specified a minimum wage to be paid (TE that did not ask for the wage
elements to be spelled out and XD that did). In practice even if the fees were fixed according
to the IDPs‟ tender price, the variation within an LA was quite low, that is at £2 to £3.50
except for one LA (XD) where the range was £12 between the lowest and the highest fee
(table II.4, column four). The LA (LK) that had different prices by area had a differential of
£4 between the most difficult and the easiest to service and it is likely that some of the
variations in the other LAs reflected differences by geographical area. The three LAs which
contracted with agencies where TUPE transferred inhouse staff were employed paid these
agencies a fee that exceeded the median rate for the other IDPs by between £4 and £7.50 per
hour12.
The average fee paid to IDPs (excluding these TUPE related fees 13) ranged from £10.45 to
£14.50 for 13 LAs. XD was again an exception with a higher implied average fee as well as
large range of £16 to £28; we have classified the average fee for XD as £20. To classify the
LAs by fee level we paid attention to both the lowest fee and the midpoint or modal fee level
(where this was indicated to us). Two paid a fixed fee to all below £11 and we classified
these as very low payers. Two more had average fees below £12 and we classified these as
low payers (one paid a fixed fee14 and the other had variable fees). Those paying between £12
and £14 – both minimum and average fee levels were classified as medium fee payers and
those paying above £14 on average and above £13 as a minimum were classified as high fee
payers (table II.4 column three).
11
In the case of LK there were three fixed prices related to the nature of the geographical area- easy to service,
medium and hard to service.
12
No precise information for RT but a significant differential was paid
13
The fees rates reported for agencies with LA TUPE transferred staff were £22 compared to an average of
£14.50 to other providers (AH) and £16 to £19 compared to an average of £13 to other providers (AW) (table
II.4. columns 2 and 3)
14
In the case of ON there was a move from a fixed flat rate of £11.17 per hour with a higher price for half an
hour contact visit to a fee of £1 per hour plus a proportion of £12.15 per hour depending on the actual recorded
minutes of the visit. The flat rate element was to be reduced in 2010 to 60p.
EWERC
Part II. Commissioning and contracting in the selected local authorities
73
Table II.4 Fee levels and fee setting for domiciliary care
LA
Standard price or
contract price
AH
Varies by tender
offer
ON
RT
RN
UY
AD
AW
IL
OM
XD
HD
TE
LK
RD
Standard price
or midpoint of
price range
14.50
Range of price variations
- maximum minus
minimum 1
£3
£9 including TUPE
Price set by LA
11.17
£0
Source of
variations across
providers
Tender offer,
preferred/spot,
TUPE
None
Varies by tender
offer
Price set by LA
Price set by LA
Price set by LA
Varies by tender
offer
Price set by LA
Varies by tender
offer
Varies by tender
offer
Varies by tender
offer
Varies by tender
offer
Price set by LA
Varies by tender
offer
13.00
10.78
12.53
£2 (estimate)
TUPE price not known
£0
£0
£0
£2
£7 including TUPE
£0
£3.49
Tender offer
TUPE
HR performance
None
None
Tender offer
TUPE
Urban/rural
Tender offer
20.004
£12
11.74
£1.93
13.08
£2.60
14.25
12.5
£4
£3
Tender offer
Urban/rural
Tender offer
Urban/rural
Tender offer
Performance
Urban/rural
Tender offer
Urban/rural
1
13.10
13.16
10.45
13.00
Additional
payments for
unsocial hours
Bank holidays
Weekends or nights
Travel costs
Bank holidays3
Higher price for 30 minute visit.
Require payment in contract
Higher price for 30 minute visit
Low+3
Higher price for 30 minute visit
Monitor for gaps
No specific provision
No specific provision
Medium+
Medium+
Very low
Medium
No specific provision
No specific provision
Very low
Medium
Rural price
High+
Rural price
Low
No specific provision
Medium
Rural price
Rural price
High+
Medium+
Weekends or nights
Weekends or nights
No specific provision
Classificati
on of LA
by fee level
High +
Medium+
These ranges exclude fees paid to IDPs with TUPE transferred staff
+ indicates either some provision for unsocial hours payments, for travel time or for performance bonus
3
These were withdrawn between our LA interview and our survey of providers
4
This LA had a range of £12- the norm was estimated on the basis of the interview to be closer to the bottom of the range- we thus took the point one third of the way up the range rather than the
midpoint.
2
EWERC
Part II. Commissioning and contracting in the selected local authorities
74
The fee paid per contact hour may not, however, capture all the dimensions of the generosity
of fee provisions. In particular it does not provide us with information on how contact hours
are calculated. Such information is difficult to collect in detail in a comparable form and was
beyond the scope of this project. However, some information was collected on additional
aspects of fee provision, particularly with respect to issues such as type of care, the treatment
of travel time, unsocial hours, etc. The first point to note is that the fee paid for domiciliary
care was a flat rate fee, not normally differentiated by level of care provided, except in some
cases where the LA was commissioning intermediate care in conjunction with the NHS. This
pattern for our selected LAs complied with that found in the stage 1 survey. For the 90
responding LAs over one third, 36%, had a standard price for domiciliary care. Of the
remaining 64%, only 10% of LAs, just over 6% of the total sample, reported variations in fee
by individual user and this did not include any of our LAs. The implication of this policy is
that there are no gains for providers in relation to the fee paid if they have more skilled staff
able to undertake care work for those with a higher level of dependency, unless this work
falls under a different commissioning process.
Very few LAs also provide for travel time explicitly in their pricing and fee policy. Of the
fourteen in our survey only three paid more for short hours visits (usually a higher rate for 30
minutes) and two of these were phasing this practice out (ON, RN). A number of other LAs
said they had paid higher rates in the past but had already phased them out in the interests of
administrative simplicity. One other LA (UY) said it paid for travel time in calculating
contact hours. Four had an explicit policy of paying extra for rural domiciliary visits but this
was normally built into the standard price for the provider who covered the rural area. This
information was confirmed at the stage two interview but also matched answers to the first
stage survey with respect to variations by ease of travel, except for one LA (LK) that
responded to the stage one questionnaire that it had a standard price for domiciliary care but
in practice it had recently introduced three standard prices which varied according to the
travel issues in the area. As eight of the fourteen LAs did pay different rates to providers
there may be more allowances for travel issues than perhaps is captured by these measures.
One LA (TE) paid a higher fee not on the basis of travel time per se but if the provider agreed
to take on a case that was outside their specified geographical area. This may reflect a
tendency to only allow one fee per provider under the contract, unless something unusual
outside the standard terms occurs. Another factor affecting payment for travel time is whether
or not electronic monitoring is used. One LA (ON) moved to payment by minutes based on
electronic monitoring during the period of our telephone survey of independent providers and
this was changing how providers compensated staff for travel time (see part III and part V
below). There was even less evidence of additional payments for unsocial hours in the fees
paid by our fourteen LAs. Two (ON, AH) paid extra fees for bank holidays but one was
considering phasing this out (ON). Only three paid extra for nights or weekend work (AH,
RN, XD).
This low incidence of additional payments is similar to the overall results for the stage one
survey where only just over 20% of the LAs without a standard price said they paid extra for
travel time. Two LAs, both medium fee payers (RN and TE) provided some additional fee for
EWERC
Part II. Commissioning and contracting in the selected local authorities
75
providers who met performance targets, with RN specifically setting HR performance targets
and requiring providers to spend the additional fee on their staff.
If we include additional payments for unsocial hours or travel time into the analysis (table
II.5 column five) we find that these additional payments on the whole reinforced divisions
between LAs rather than compensated for low basic fees. The one low payer that was making
additional payments was withdrawing from these as it moved to payment by minutes
recorded by a new electronic monitoring system (although it was also raising the fee level,
potentially pushing it into the medium category). However, the greater incidence of
additional fees for travel among the high payers reflected the rural nature of the areas covered
in the two cases concerned.
Fee levels are related to geographical location: Table II.5 shows that all the very low and low
fee payers are located in the north and all the high payers in the south. Among the medium
fee payers three are southern LAs, three in the midlands and one a northern LA. All the high
fee payers were in areas of high female labour demand (see section I.7 and appendix table
I.A1). Local labour market conditions may explain the positioning of two southern LAs (the
two outer London boroughs) within the median fee category as they scored only three for
female labour demand but the final southern LA had a score of five for female labour
demand. Another outlier is the northern LA that is a low fee payer but has a five score for
female labour demand. The other three low or very low payers were in areas of low or
medium female labour demand. Fee levels in the majority of the LAs thus bear some relation
to geographical position and local labour market conditions but the relationship is not fully
consistent.
Table II.5. LA fees for domiciliary care by geographical area and local labour market
conditions
Total
Geographical area
Local labour market
conditions:
Additional payments for unsocial
hours, travel or performance
Number of LAs given + in table
II.4 column 8
Low and very
low fee payer
4
4 north
1 strong, 3 weak
1+*
Medium fee
payer
7
1 north, 3 midlands,
3 south
1 strong, 4 medium, 2
weak
4+
High fee payer
3
3 south
3 strong
3+
Note: *These were withdrawn between our LA interview and our survey of providers
Fees for residential care
Table II.3 column six classifies the LAs by the average cost of their residential care for older
people (without nursing or dementia) according to the data provided by the LAs themselves
EWERC
Part II. Commissioning and contracting in the selected local authorities
76
in their PSS EX1 Return for 2007-08. We have used these data in preference to that provided
by the LAs in our survey as it became apparent that there were inconsistencies in how these
fees were reported to us. However, the published data corresponds to our information in most
cases, except where we were doubtful of its accuracy. One- that for OM- appears rather low
but there have been changes in its system since 2007-8 including quality uplifts which may
account for this divergence. Only broad categories have been used here to preserve the
anonymity of the LAs. There are major problems in classifying the LAs according to fee
levels as it is clear that the variations in fee levels are very large and reflect differences in
property markets more than in labour markets. For example, the two outer London LAs are
classified here as high and medium payers but both pay below average for outer London.
While this could be an alternative way to classify the LAs for the two cases, there is a very
wide variation in property and labour markets in for example unitary authorities, metropolitan
areas and shire counties so that these average fee data are less helpful for the purpose.
The information that we did gain from our interviews is that many LAs have introduced
quality enhancements. Five of the LAs are currently paying higher fees to higher quality
homes (table II.3. column seven) and ON pays an additional fee for Investors in People award
and is considering a more fully developed quality framework. As we discuss further below,
there are differences in the strategies used by LAs with respect to setting their fee level; some
aim to minimise any pressure for those placed in homes to pay top up fees, while others
expect most to have pay an additional fee or even seek to place those unable to pay additional
fees in homes located in cheaper property areas outside their own boundaries.
Classifying the LAs by fee level: domiciliary and residential combined
To put all this pricing information together we have combined information on domiciliary
and residential care. In Figure 3.1a.we classify the LAs on the basis of average fee for
domiciliary (table II.3. column 8) and the average cost of residential care (table II.3 column
six). We allocate a score of 1 to 4 for very low to high for each category and for overall
categorisations we take high payers as having a score of eight, medium six or seven, low five
and very low four or less. On this basis we have five very low fee payers (IL, HD, AD, OM,
ON ) two low fee payers (TE, RD) four medium (AW, RN, RT, UY) and three high (AH,
LK, XD) (note the squares are shaded from light to dark as one moves from very low to low,
medium and high fees). In Figure 3.1b to capture the extent to which LAs provide additional
payments for quality in the cases of homes we add 0.5 to every LA that has a quality uplift
and for LAs that pay for either unsocial hours and travel to IDPs we add a 0.5 to the score for
domiciliary fees (table II.4 column seven). We then adjust our scoring categories with very
low still 1 to 4, low 4.5 to 5.5, medium 6 to 7 and high 7.5 to 9. On this basis three move
from very low to low (AD, OM, ON) and one (RN) moves from medium to high. Indeed all
but IL, HD and AW increase their scores by 0.5 points.
EWERC
Part II. Commissioning and contracting in the selected local authorities
77
Figure II.1a. Categorising the LAs by standard fee levels- domiciliary and residential
Domiciliary care fee
Very Low
Very Low
Residential home fee
Medium
IL
Low
Medium
Low
High
OM
ON
TE
HD
RD
AD
RT
UY
High
AW
AH
RN
XD
LK
Figure II.1b. Categorising the LAs by standard fee levels and quality enhancements domiciliary and residential
Domiciliary care fee
Very
Low
Very Low
Very
Low+
Low
Low+
Medium
HD
Low+
ON
RD
TE
Medium
Residential home fee
High+
OM
Low
High
High
IL
Very Low+
Medium+
Medium+
RT
AD
UY
AW
AH,XD
LK
High+
EWERC
RN
Part II. Commissioning and contracting in the selected local authorities
78
II.1.3. Role of HR factors in tendering, contracting and monitoring
The stage 1 survey asked whether LAs required providers to conform to up to ten HR policies
in either the tender or their contracts for IDPs. In practice most LAs included the same
number of policies at tender as at contract15. In practice only three LAs (AH, IL, RD see
Table II.6 column 3) included most or all of the ten policies, at nine or ten policies each. The
majority of LAs (six at tender, five at contract) included six to eight policies while four at
tender, five at contract included fewer than six. (One LA (XD) had missing data). Three
policies were categorised as concerned with pay (pay for training, travel or mileage) and five
with training and development16 (staff development and appraisal, management training,
induction and training, specialist dementia training and training achievement against national
targets). More LAs (11) scored high on training and development (with at least four out of the
five policies) compared to only four LAs who included at least two out of three pay policies.
Only three LAs required payment for training time (AH, ON, IL) and only five for travel time
(AH, ON, RN, IL, RD).
15
One LA (ON) included more policies at contract stage and one (OM) at the tender stage
The two excluded were payment for sick pay as it was not clear if this referred to more than statutory sick pay
and supervision of staff as all but one LA included this in their requirements.
16
EWERC
Part II. Commissioning and contracting in the selected local authorities
79
Table II.6 LAs’ monitoring and quality frameworks
LA
Domiciliary care providers
Number of policies
Quality monitoring by LA
In tender/In contract
training
pay
HR policies Own framework
Use of electronic
policies
policies
Maximum
without/ with financial
monitoring
Maximum
Maximum 103
incentives
51
32
Residential homes
Number of policies
Quality monitoring by
In tender/In contract
LA
training
pay
HR
Own framework with/
policies
policies
policies
without financial
Maximum
Maximum Maximum incentives
51
12
83
AH
4/4
3/3
9/9
Yes
None
4/5
1/1
7/8
None
ON
0/2
0/2
0/5
Yes
Planned*
m
m
m
RT
5/5
0/0
6/6
No
All
5/ 5
0/0
6/6
Yes with financial
incentives
None
RN
4/5
2/2
7/7
None
5/ 5
0/0
6/6
UY
4/4
0/0
5/5
Yes with financial
incentives
Yes
Some
0
0
0/n,a,
AD
5/5
0/0
6/6
Yes
Planned
5/ 5
0/0
6/6
AW
0/3
3/0
4/4
No
All
0/3
0/0
0/4
Yes with financial
incentives
Yes with financial
incentives
Yes with financial
incentives
None
IL
5/5
3/3
10/10
Yes
All
5/5
1/1
8/8
Yes
OM
5/3
2/0
8/4
No
Some
0
n/a
0/n.a.
XD
m
m
m
Yes
All
4/0
0/0
5/0
Yes with financial
incentives
Yes
HD
5/4
0/0
6/6
Yes
Planned
4/n/a
0/n/a
4/0
Yes
TE
4/4
0/0
4/4
All
4/n/a
0/n/a
4/0
LK
5/5
0/0
6/6
Yes with financial
incentives
Yes
None
5/5
0/0
6/6
Yes with financial
incentives
Yes
RD
5/5
2/2
8/8
Yes
None
3/n.a.
0/n/a
4/n.a
Yes
EWERC
Part II. Commissioning and contracting in the selected local authorities
80
In relation to tenders with care homes LAs were only asked about eight HR practices as travel
time and payment for mileage were much less relevant. Three LAs specified no policies in
their tenders and for another data were missing. Of the remaining ten, six specified six or
more policies and four between four and five. However, only two specified payment for
training, the only pay policy apart from the ambiguous sick pay question. Most policies were
related to training with nine LAs specifying at least four training policies, not including the
pay for training policy. The question about contracting referred only to block contracting
which only applied to ten LAs. Of these, two did not provide for any HR policies in their
contracts and one had missing data while six specified six policies or more and only one had
a low score at four. Only two LAs specified pay for training while six had at least five other
training policies in their contracts.
The majority of the LAs were also actively involved in monitoring the provider with respect
to HR practices and many were active in developing their own quality framework: only twothe two outer London boroughs- relied entirely on external monitoring by CQC and one was
planning to introduce its own framework. Of the remaining 12, all but one had a quality
framework for IDPs and nine for homes. Two LAs (TE and RN) offered financial incentives
to IDPs for meeting quality targets, with the target explicitly related to HR issues in one case
(RN). Although quality frameworks were somewhat less common for homes, they had
potentially more impact on providers as they were associated in six LAs with a quality-based
pricing framework. Five however had their own quality framework for monitoring (RD, IL,
HD, XD, LK) without any financial incentives.
Another mechanism for monitoring IDPs was electronic monitoring. This was another area of
rapid change. At the time of the stage two interviews five LAs had already introduced
electronic monitoring for all17 (table II.6 column six) and two were using it with some
providers In almost all cases this was a very recent development and another LA (ON)
introduced it over the period of the survey with a further two having active plans to introduce
it. This left four with no current use or plans for its use.
II.1.4. Extent of support for providers through forums and training provision
Local authorities provide additional support to independent providers in two main ways: first
by providing or organising training for independent sector staff; second by consulting with
providers through forums and in relation to commissioning strategies.
17
AW said it had a mix as not all spot contractors had introduced it but further probing revealed that it was only
those with electronic monitoring that were being actively commissioned.
EWERC
Part II. Commissioning and contracting in the selected local authorities
81
Table II.7 LAs’ support for providers through training and provider forums
1
LA
Frequency of
forum
meetings per
annum
High- 6+
M-3 -5
L-1 or2
Organisation of
forums for
domiciliary and
residential homes
providers
Training
partnership
with
independent
providers
1st stage
survey/ 2nd
stage interview
Number of
types of
training1
provided by
LA to
Independent
sector
Stage 2
interview
Assessment of
training
activity by LA
alone or in
partnership
Involvement in
commissioning
: Providers of
social care
services
AH
M
Combined
No/No
Low
Low
Yes
ON
M
D and H separately
No/Yes
Low
High
Yes
RT
M
D only
No/No
Low
Low
Yes
RN
H
D only
Yes/No
Medium
High
Yes
UY
H
D and H separately
Yes/Yes
High
High
No
AD
H
Combined
Yes/Yes
Zero
High
Yes
AW
M
D and H separately
Yes/No
Zero
Low
Yes
IL
H
D and H separately
Yes/Yes
Medium
High
Yes
OM
M
D and H separately
Yes/yes
Medium
High
Yes
XD
L
Combined
No/No
Zero
None
Yes
HD
M
D and H separately
No/Yes
Zero
High
No
TE
M
D and H separately
No/Yes
Medium
High
Yes
LK
H
D only
Yes/yes
Medium
High
No
RD
H
D and H separately
Yes/Yes
High
High
Yes
Coding Zero-none Low up to 4 Medium 5- 9 High 10 + more
Training support may be provided through training partnerships; in the stage one survey eight
of the LAs said they had formed training partnerships with independent providers but
information from the stage two interviews suggests that this should be nine. In fact three
more said they had partnerships while another two did not currently have a partnership (table
II.7 column four). Of the two who said they had a partnership at stage one but not at stage
two one (AW) did not provide any training themselves, probably because it had no inhouse
staff, while RN did not have a training partnership but was nevertheless very active in the
provision of training for independent staff. Table II.7 column five shows that the formation of
a training partnership was associated with higher levels of support for the training of
independent staff but not in all situations. All who provided medium or high levels of training
to independent sector staff had a partnership according to our stage two interviews – except
for RN that opened up its own LA training to independent staff. Some that recorded a low or
zero incidence of training on the stage one survey were found in the stage two interview to
have high levels of activity (for example ON, HD, AD). In each case the training was
provided by a partnership and the respondent may therefore have decided to answer no with
respect to LA provision. Column six of table II.7 provides an overall assessment of activity of
the LA in training provision based on the stage two interview supplemented with the stage
one information and finds: one LA (XD) not involved currently in training provision due to
EWERC
Part II. Commissioning and contracting in the selected local authorities
82
the collapse of a previous partnership when funding sources dried up, three LAs (AH, RT,
AW) with either no or very limited inhouse provision recording low involvement; all
remaining ten have been classified as having a high level of involvement.
With respect to consultative arrangements, all but two LAs involved the providers in
consultation over commissioning (the exceptions were HD and LK table 3.7 column seven).
All also held provider forums for care providers according to the stage one survey. In one
case these forums met only once a year but for the others the frequency was three to four
times a year for seven LAs and up to six times for six LAs. Through the stage two interviews
we gained more information about these forums; in all cases there were forums held for
domiciliary care providers and in three cases these were joint with providers of residential
homes. In seven LAs separate forums were held for domiciliary care and residential care
providers and in three LAs no forums were organised for the residential home providers. In
six LAs the interviews with the LAs suggested that these were not very active bodies,
whether for domiciliary or residential. One of these had only recently re-established the
forum18. In another (AD) in principle the forum met six times a year but in practice
attendance was low so meetings were often cancelled. A particular problem here was that
many providers worked for more than one LA so that they felt they had too many meetings to
attend (see part IV for providers views in the telephone survey with respect to the usefulness
of the forums).
18
Under the stage 1 survey this was the LA- XD where the forum met only once a year but there were plans for
it to be more active.
EWERC
Part II. Commissioning and contracting in the selected local authorities
83
II.2. Approaches to commissioning and contracting: the
qualitative interview data
The qualitative interviews with key actors responsible for commissioning and contracting in
the 14 selected LAs revealed the multiple and potentially conflicting influences on
commissioning practices19. Not only is social care commissioning taking place within the
wider local authority and is thereby subject to specific local organisational and political
environment but there are also multiple and often competing longer term policy agendas for
the development of social care. In respect of policies towards independent providers there are
competing agendas between the need to support providers and develop the supply base
against the need to take costs out and control price while improving quality. Further
competing agendas stem from the issues of whether LAs should continue to be the drivers in
commissioning or whether this should be developed jointly with the NHS or devolved to
users.
The issues of direct concern for this project were how LAs made sense of and prioritised the
various influences on their commissioning and contracting strategies. The two main current
conflicting pressures were the pressure on budgets and costs on the one hand and the need to
develop capacity in the market on the other hand if both quantity and quality targets in
delivery were to be met. Linked to these cost versus capacity issues was a parallel potential
conflict between pressure to respond to short term factors versus the need for more strategic
longer term changes to the approach to social care provision. Cutting across the traditional
conflicts over cost and quality and the short and the medium term came the new policy
agendas of integrated health and social care provision on the one hand and personal budgets
on the other. These new policy agendas were adding to some of the conflicts between short
term concerns and long term strategic directions, in part because they provided potentially
alternative long term strategic visions of the future of social care and the role of LAs within
that provision. To explore further the nature of these conflicts and how they were being
resolved within our selected LAs we follow the same four themes as identified in the
literature review, namely:
o making the market
o price versus quality
o integrating health and social care, and
o the personal choice agenda
19
Note in this section we attribute quotes to the LA commissioners in general not to specific interviewees. This
is done because most of the interviews involved multiple participants and to preserve the anonymity of the
official concerned. In one LA- IL- we interviewed the contracting and commissioning departments separately
and as they had very different and distinctive positions on the polices pursued we have made an exception and
linked the quotes to either the contracting or the commissioning branches. In other cases we use commissioners
to denote interviewees in contracting and commissioning. For further information on whom we interviewed at
the LA level see section I.7.
EWERC
Part II. Commissioning and contracting in the selected local authorities
84
II.2.1. Making the market
The need to develop the supply of independent providers, both to secure an adequate supply
of care hours and to promote the quality of the independent sector, emerged as a repeated
theme within our interviews on commissioning approaches and strategies. The diversity of
issues that came up under this general heading was large and we discuss them below under
three main subthemes: capacity development and managing the spatial market; purchaserprovider relationships; and interventions on quality.
Capacity development and managing the spatial market
The first concern with respect to capacity related to overall supply. Many of our selected LAs
had been expanding the share of their social care hours that were outsourced and several were
also planning further expansion. However, some LA commissioners were concerned about
the capacity of the independent sector to supply the desired number of hours. For the
contracting department managers in one LA (IL), the problem in their view lay in the fact that
there was a fixed pool of staff and offering more hours to one provider, as the commissioners
suggested as a solution to capacity, just increased labour market churning. In another LA
(AD) interviewees reported that they had expended a lot of effort in encouraging its existing
suppliers to make a step change in their contracting hours from around 400 or 600 to 2000
hours a week. This was to enable the LA to provide better and more guaranteed geographical
coverage and to increase the share of work outsourced. In another LA (TE) commissioners
spoke of the dual problems of both getting existing suppliers to cooperate in delivering
according to their service needs and also in judging just from a tender what a new supplier
would be able to deliver in practice.
The providers are a mix of small local providers and national providers. There is one charity
and one very small local company that the council has had to offer a great deal of support to
to enable them to deliver what the council wanted. ….Some of it was dire, really! TE
While the need to develop supply was a key part of the LA commissioners‟ concerns, these
questions were primarily considered at a local rather than a national level. Thus, for example,
the concerns of UKHCA that a focus on large volume contracts may ultimately reduce supply
nationally by squeezing out the middle level supplier was not an issue that came up in our
interviews. More concern was expressed about the actions of national providers in „asset
stripping‟ the residential homes that they took over, but here the strategies of the national
providers were seen as independent of any specific policy initiatives by the LA.
A second set of capacity concerns related to geographical coverage. These included the need
to ensure an adequacy of supply, particularly in those LAs with a large rural area, the need to
to develop the spatial coverage to reduce travel time and the need to use allocation by
geographical areas to reduce uncertainty over likely volume of demand for contracted
providers.
EWERC
Part II. Commissioning and contracting in the selected local authorities
85
Different solutions were used in the two LAs with sizeable rural areas- XD and LK- to ensure
supply. In XD providers were required to bid for a city and a rural area at the tender stage; in
LK where most of the area was rural the tactic adopted was to offer a guaranteed stepped
higher price for difficult to reach and very difficult to reach areas.
It was a real challenge providing service in rural areas as workers don‟t want to travel. So
they have linked urban with rural so providers work in both difficult and easy areas. XD
These rates were agreed with the providers on a parish by parish basis, and will be reviewed
periodically. The result of this has been that recruitment has improved in the agencies – it
was good to acknowledge that providers need extra cash as encouragement. UK
In less rural areas the main concern around geography was to minimise travel time and
reduce inefficiencies (for example IL, HD, TE, RN). For one LA (HD) the move towards one
local provider was said to be part of a wider strategy to „rebalance the market „by establishing
a clearer division of labour between the inhouse re-ablement function and the transfer of
cases to the independent provider selected on the basis of the LA‟s geographical mapping of
the city:
We have mapped every home care client across the city where they live in terms of the street
and which provider, and so from there you can spot a couple of providers who are going to
the same street which kind of doesn‟t make any sense. It adds additional challenges for the
providers. HD
Another LA (TE) had also undertaken a major reorganisation of its supplier network around a
new five area geographical division, with one provider per area. This was partly related to
issues of travel time but more importantly was a response to a user survey indicating
problems of time keeping, rushed visits and inconsistency of care workers, all issues
indirectly linked to operating a city wide rather than a geographically specific service. For at
least two LAs (AD, AW), organisation by geographical area was said to be part of a wider
strategy to guarantee higher volumes of hours to providers.
A third set of capacity issues related to ability to meet specific needs such as care during
unsocial hours or care for diverse client groups. Some LA commissioners were aware that in
order to be able to outsource their social care work, independent providers needed to be in a
position to provide flexible and unsocial hours services. In the case of one LA (AD) the
solution seemed to be one of encouraging cooperation rather than competition between
providers. This illustrates the potentially conflicting motivations in commissioning when LAs
may also be concerned to encourage competition in the interests of keeping costs down.
I said really you need to establish a framework for an evening service. If you are recruiting
people in cars you can work across boundaries. You can come to some agreement with each
other. And really what I was trying to sell them was the whole idea that this does not need to
be businesses in competition. This actually could be businesses working in consensus and
supporting each other. AD
EWERC
Part II. Commissioning and contracting in the selected local authorities
86
Promoting a diversity of supply was a major concern of the employers‟ association in this
sector (UKHCA) and a principle of both the best value regime and the personal choice
agenda is that there should be a range of suppliers available in the sector to provide for choice
and to reflect diversity of the population. Some of the commissioners in the selected LAs
were also conscious of these issues- for example, as discussed above, those in TE had
provided support to a small organisation to enable it to fit with its reorganisation. However, it
was one of the outer London boroughs with a diverse population where there was most
recognition of the diversity of supply agenda.
Because we have such a diverse community, and we tend to have more smaller voluntary
organizations rather than great big national ones….I think in terms of working with the
voluntary sector to provide these services if anything we‟re very slightly ahead of the curve,
certainly compared to other boroughs I‟ve worked in. RT
Some LA commissioners did express concern at the increasing role of national chains in the
residential homes sector and the long term impact on both diversity and quality of supply:
The hugely big providers just asset strip, not to put too fine a word on it. So they move in,
they strip the food budget, they strip the training budget, the decorating budget, they cut down
people‟s wages, you know, they do the whole bit really, as their first act, and it never gets reinstated. RT
Purchaser - provider relationships
The need to develop the market had led commissioners in a number of LAs to make a
strategic decision to change their relationships with their providers. One LA (AH) had
entered into longer term strategic relationships with a smaller number of preferred providers.
A key advantage was said to be benefits in improving access and reducing processing of
people coming into the system. The LA commissioners felt the smaller number of providers
meant that uncertainty over volume of business would be reduced, allowing them to refer to
these new preferred contracting arrangements as the „new block‟ contracts.
The whole idea was that we wanted to create strategic partnership and therefore we would
work with fewer partners and we knew that unless we gave them a reasonable amount of work
they wouldn‟t want to go with it AH
Other LA interviewees also talked about actions to change relationships into more
partnerships.
Our commissioning practices have changed and I very much base this on the relational
aspect of commissioning. ..it‟s about the relationship with providers which is important –
sharing our values, and looking to achieve a principled outcome. Win win for us all.. UY
However, in some LAs the motivation for changing the relationship with providers was more
to reassert LA control over the relationship. Commissioners at XD sought to reduce the
power that spot contract providers had in a context of constrained supply.
EWERC
Part II. Commissioning and contracting in the selected local authorities
87
What we were faced with in terms of home support was a position where the balance of risk
and the balance of power firmly rested with the current in county providers. We were starting
to get demands - for 3 successive years we had demands for increases of 10%.... Prior to
2006 we worked purely on the basis of spot contracts, so no guarantee of incomes for them,
no guarantee of service,...
The strategy adopted was one of expanding the number of contractors but then moving to
block contracts and consolidated pricing to include mileage.
The idea behind the block contracts was that providers had told us that they couldn‟t recruit
and retain staff because they hadn‟t got the guaranteed income and they didn‟t have a block
contract like the internal service, so we tried to replicate that [the internal service] …around
salary levels, then our internal service was on a basic of around £7.24 per hour weekdays
and so the bids we generally accepted were those who pitched at around £7 per hour.
Previously it had been around £6 per hour so we knew we were going to take a financial hit
but we compensated for that by looking at how we might address some of the weaknesses
around invoicing by bringing in electronic timed monitoring system and paying from this
system. So this was the whole strategy. XD
However, the ability of the LA to use its provider relationship depended upon their own
power within the market. LAs could face particular problems of limited leverage on care
home providers in more affluent areas due to the rather low share of LA funded clients in the
total client population.
If you have 128 providers with 30 beds and only 5 of those beds are local authority funded,
it‟s very difficult to engage with them as they don‟t necessarily need to engage with the LA.
RN
Quality interventions
As a key aim of „making the market‟ was to improve and to guarantee quality standards, one
way of addressing the issue was to intervene directly in the development of quality standards.
Most of the LAs in our sample had in fact developed their own quality framework for
monitoring both domiciliary and care home providers there were some exceptions. LK which
had a large number of providers on its books because of its highly spread out population. had
adopted a policy of leaving it primarily to CQC to establish standards.
Any provider can go through the accreditation process with the LA, and the LA then decides
whether or not to take them on. …They are registered with CQC, and they agree to work to
our terms, conditions, and service specifications. For a dom care agency we require them to
have either been through 1st key inspection so we have evidence of type of service they
deliver, or they have undertaken a customer survey with at least 6 current customers and
analyzed that. However, we mainly rely on CQC accreditation.LK
Where LAs had their own monitoring, this was often linked for care homes to quality uplifts
on LA fees. Examples of how these quality uplifts worked were provided by three LAs (UY,
OM and AD).
EWERC
Part II. Commissioning and contracting in the selected local authorities
88
We have incentivized our contract now with care homes we want to rid ourselves of poor
homes, ….We pay an additional amount of money for excellent care homes if they are
excellent they have had 2.5 % uplift plus the inflation, if good they get 1% plus inflation, and
if adequate they get inflation uplift, if poor they get nothing. This is with national minimum
standards, but we like to think our contract takes this further as we are outcome focused we
have gone way from days of what we want them to do to specifying what we expect the
outcomes to be as a consequence of that engagement.UY
What we now have is a banding arrangement applying to our older persons care homes, and
there‟s a quality banding and there‟s quality uplift and you can sit within one of four or five
bands. …what we have done is we have dedicated £800,000 to the city residential care homes
and our service users within that, and we have said that for every banding uplift that you
achieve, as determined through our quality monitoring, ….you will receive an uplift of X. So
you can lift your unit cost for each …city resident by an appreciable sum. And we‟re not
talking about two percent, we‟re talking about somewhere in the region of twenty percent in
some cases (OM)
Fifty percent of the quality framework will be based upon the quality of the care delivered,
thirty percent of the framework is delivered upon the environmental … arrangements, ten
percent will be based around their CSCI star rating and ten percent will be based upon the
views of carers and service users who use those services. So that‟s the way we‟re doing our
split.AD
Only a small number of LAs provided such uplifts for domiciliary care. In fact only TE
provides a quality uplift in relation to care standards, as explained below.
Our service users told us that there were three things wrong with it. One was that people
didn‟t turn up on time, that they didn‟t stay the allocated time and there was inconsistency of
carers. So using the feedback from our customers we developed contracts aligned to that,
and we put three key performance indicators in it, so that ninety percent of the contract value
would be paid as normal, but they would only get the extra ten percent if they could
demonstrate that the KPIs had been met, which was very painful for them and us... which
were also tortuous! Just so that we could demonstrate to our customers that the service was
being delivered in the way that they wanted it to be, that we were getting value for money. TE
In contrast one LA (IL) had discontinued its quality premium on the grounds that it had
served its purpose in raising the minimum quality threshold so that it was no longer necessary
to reward the good performers.
We used to pay a premium for quality service, but not all organizations met the quality
standards. Presumably, this was to bring up quality, because it was very low. Over time, the
quality of all services improved, so we were paying for quality when we didn‟t need to. ..so, it
was almost a unanimous decision – about one fee and we expect quality to be in there for the
price. IL
In some cases the moves towards improving quality standards through commissioning were
currently aspirational due to a shortage of supply of providers that reached the desired quality
standards as the contracting manager at RN explained.
EWERC
Part II. Commissioning and contracting in the selected local authorities
89
For care homes we have just recently introduced a process called fairer contracting and
that‟s about actively encouraging higher quality and we want to work towards only
contracting with good and excellent care homes but if we did that at the moment there
wouldn‟t be enough care homes! RN
Some LA commissioners (for example RT) stated that they were committed to working with
providers to improve their star ratings so that they saw themselves a playing an active role in
developing as well as monitoring standards.
Another way of managing capacity was to intervene in the development of the workforce.
Most of the LAs are engaged in providing training for the independent sector staff whether
through partnerships or other routes.
We‟ve put a lot of time and effort into improving the quality of the product, if you want, and
that includes the staff. So for example, I say we‟ve invested heavily in the training
partnership, which has really been very successful. RD
I think the issue of how people are treated and how they are employed and whether they are
invested in and developed in the independent sector is a concern that we have. [UY area]
partnership forum that we have is about encouraging employers to invest in their staff and
provide leadership training for managers. UY.
A particular attraction in providing training for one LA (ON) was that they had control over
its quality.
I mean I‟m quite interested in that wider debate we‟re having about cost and fees, is there
other things we could deliver that adds value to them that (…) necessarily tied up with what
we pay them for an hourly rate. And training is definitely one of them, cos then we can quality
assure the training that they receive, i.e. we will have delivered it.ON
For another LA (OM) the advantage of involvement was said to be the opportunity to
undertake better planning of training provisions than was possible if it was left up to
individual small providers.
Rather than them saying yes that looks like a good course we can actually evidence base it
through the workforce planning, not got to that stage yet but we are looking to it (OM).
One LA had set a target of 70% NVQ level 2 for its providers compared to the national
standard of 50%.
We target 70% of care workforce to have NVQ. One group of 16 workers, all over 50 had no
qualifications and no learning since leaving school. All reluctant learners – anxiety and
stress of embarking on that as well as a full time job. All got a lot out of it. LK
Beyond interventions on training we found isolated examples of LAs intervening to improve
employment quality along other dimensions. At one LA (AD) commissioners had tried to get
providers to agree to offer guaranteed hours contracts to staff, now that they were in receipt
of block contracts but one national provider had refused, leading to the overall scheme being
EWERC
Part II. Commissioning and contracting in the selected local authorities
90
abandoned. In another LA (ON) there was concern to ensure that providers did pay for travel
time and training time. However, although the commissioners said they specified payment for
travel and training time in the tender they felt themselves to be still primarily reliant on good
relations with providers to ensure compliance.
We‟re trying to monitor it to see there is some degree of travel time. So it‟s not just what we
say it‟s what they plan. I mean we don‟t do it in a very precise sense but there is some gap
between the ordered period of time and the next. I suppose … we‟re morally trying to … take
the moral high ground. Obviously we can‟t instruct people to pay…. ON
Another LA, RN, built in differential payments to reflect the type of care and the time
dimension to care but was moving away from this system by the time we undertook
interviews in the area.
The price levels vary by standard/special care (i.e. needing 2 carers, medication, colostomy
etc) by weekday/weekend and length of visit (60, 45, 30 and 15 mins) and then they have
waking nights (though not many of them)
Some LAs such as XD had used its tendering process to identify in detail the HR policies of
the providers and were using this information as a key element in selection and in the price
paid to providers which was highly variable.
So they tried to build provisions within their contracts to meet these challenges. Also when
they assessed tenders they asked providers to give them a build up of their unit costs as they
knew recruitment and retention was a big issue and they wanted to make sure providers were
pitching their salaries at a level were they could recruit, and they also wanted to know that
tenders were viable for the future. So they had a pre-tender conference for providers where
they explained to them what they would be asking for and that the purpose of it was
recruitment around business continuity and viability. XD
Only one LA (RN) was directly rewarding HR performance during the course of the contract.
RN had a policy of monitoring its domiciliary providers against national turnover rates and
rewarding those whose performance was better than the national average but only if the
additional money was used to improve staff conditions.
One of the evaluation criteria is staff turnover, we said the national average is 17.5% we got
that of the DoH website and so we look for anything under that, that would go some way,
though we have to look at size of provider as well
…..They have incentive payments: 4/5 different ones! Continuity of care; take up of work;
NVQ training and whether they‟ve met the 50%; and staff turnover. What they get depends
on these criteria and the amount of work they provide as a company. Each quarter they send
performance indicators and a formula is used to calculate the incentive payment which they
will get each quarter – that‟s paid separately. They have to prove that they use the incentive
money on training, staff bonuses, staff incentives and team building to encourage low staff
turnover. RN
EWERC
Part II. Commissioning and contracting in the selected local authorities
91
One particular concern expressed by a manager at AD was that the capacity of LAs to
intervene on quality standards in general might diminish if LAs continued to withdraw from
being providers themselves as much of the monitoring was dependent upon the current
managers‟ knowledge of the sector in operational as well as contracting terms.
I actually think that if we pushed all our work out now there‟s a generation of managers who
all of a sudden are late forties, early fifties, who will be gone within ten plus years time. Now
if we‟ve stopped providing during that time you do have this sort of notion that, actually, we
won‟t have any expertise any more. And if we don‟t have any expertise then, as I say, I have a
real concern about, well, then who will develop that market. AD
II.2.2. Price versus quality.
The outsourcing decision
The explicit reason for increasing outsourcing of domiciliary care in many of our LA cases
was to reduce costs. However, those LAs that had outsourced all their services had found
themselves with a high cost legacy due to the transfer of staff under TUPE to IDPs who
charged a higher fee to cover the protected conditions. Interviewees at these LAs now
regretted the total outsourcing decision, made in haste and no other LAs, according to our
interviews, were planning any TUPE transfers even if planning further shrinkage of the
internal capacity to reduce costs.
Differences in the proportion of domiciliary care outsourced in part reflected both political
decisions and the strategy of the LA with respect to re-ablement. Political decision was also
important in residential care. One LA, LK, had quite a high proportion of inhouse residential
provision and commissioners explained this practice by reference to the fact that there had
always been cross-party support for inhouse provision in the council. In residential care it is
clear that factors other than wage costs influence decisions to maintain or close inhouse
provision; for example in one LA (RT) it was said that said that reducing inhouse provision
was not
„a result of overall policy decision. It‟s much more about the fact that we simply can‟t afford
to maintain the buildings.‟ RT.
Commissioning and contracting for low prices
Although all the LAs were outsourcing to reduce costs, the importance attached to cost
reduction nevertheless varied. For example many appeared to value continuity in their
relations with providers but one LA (AW) made wholesale changes in their preferred
providers at their most recent tender as new providers had come in at lower tender prices.
This complete change of providers also involved a second TUPE transfer of former inhouse
staff to two new agencies. Another LA (IL) had also pursued a strong policy on keeping rates
EWERC
Part II. Commissioning and contracting in the selected local authorities
92
low, including removing the quality premium. It pursued a policy of paying at the bottom of
fee levels across the country. The officer responsible for commissioning justified this on
market grounds, even though she recognised that the market may be undervaluing the skills
required for the work.
We have benchmarking information and understand that we‟re not the highest payer, but we feel
it‟s reasonable. The problem with Dom Care is it is a minimum wage skills set, or perceived to
be. I personally don‟t think it is, but that‟s what the market is currently paying. Because of that,
they often lose staff‟. IL commissioning
Several examples demonstrated that LA commissioners were aware of their position as
dominant clients and pursued strategic objectives to achieve lower average cost levels. One
LA (RD) had used the strategy of moving to a single price for all providers to reduce the
average price level, an approach also found in AD.
I think there‟s a standard price now, but we‟ve been through a whole series of getting the prices
down through the tendering process, and we have tried to move to a much clearer pricing
structure. We have moved to a much better, more competitive pricing structure that is a
reasonable one for[our area], and that‟s, you know, the whole tendering process has been around
delivering that.RD
So you really had an absurd situation where some providers were getting £2 an hour more than
other ones, purely and simply because that‟s what they‟d asked for. So we used the opportunity to
consolidate and have one price. And we also wanted to get a way where all the things like
evenings and weekends were just paid an hourly rate, and that‟s it. AD
In one LA (OM) commissioners were concerned that LAs would lose their ability to „keep
the lid‟ on the price level if the personalisation of budgets was widely implemented.
So what we will have is a position where we do not lift the lid off the role of competitive
tendering, and tendering and procurement as a principle for ensuring quality at a good price,
which is the role of the local authority as a procuring body. But if you just suddenly lift the lid off
and go for spot contracts then what are you gonna base your price on,…. you will find then the
providers have a more robust position to just put their prices up irrespective of what the care
needs are and the intensity of the care needs.OM
Even under current conditions commissioners in some LAs – for example RD and IL – felt it
was important to ensure sufficient competition in the market to keep costs down. In one LA
(RD) commissioners were wary of reducing their number of suppliers too far in case this
changed the balance of power within the commissioning environment, again leading to higher
prices.
„from our point of view we get the service at a lower rate because of competition‟. IL
You need, I would say, at least six decent sized providers, otherwise you‟re at the mercy of the
market. There is value for the local authority in having both small and large players in the
market, plus new players …. A really good balance RD
EWERC
Part II. Commissioning and contracting in the selected local authorities
93
In another LA (ON) interviewees justified a move to a uniform price from a different
block/spot price system as a way of reducing wasteful competition between providers for
staff.
We used to have a range of prices and that, if nothing else, encouraged the 5, 10, 20p an hour
more which encouraged the movement between agencies. …. It‟s not identical, but I think it‟s
closer. ON
While LAs‟ fee policies varied, commissioners in some higher paying LAs (such as AH)
were worried that they may have pitched their contract at too high a price, given likely future
budgetary constraints.
But in terms of the way the contracts have been set up has restricted us some ways – for
example tied into inflationary uplifts – which are a lot more than other providers might expect
to receive. AH
In one LA fees for residential homes were pitched at a level where top up fees would almost
always be payable. The availability of places in an adjacent lower priced area provided a
rationale for keeping fees below actual residential home care prices in RD.
Quite a lot of people are placed outside the borough where there is available space so RD
would pay their rates under a reciprocal deal. Within the borough many establishments
charge top-ups, so if people want to go into those homes there has to be a third party
agreement. RD
Commissioning and contracting strategies to take cost out
In addition to these pricing strategies there were three commissioning strategies to take cost
out of social care that emerged out of our interviews. The first involved tightening up on the
time paid for through electronic monitoring and other strategies; the second involved moving
from block to spot or call off contracts; and the third involved minimising the skill
requirements of specific services.
The rather rapid spread of electronic monitoring was being used not only to provide more
accurate information on lengths of visits but also to tie payments more closely to time spent.
In practice this also involved removing premia for short visits in several LAs where they had
traditionally paid more for half hour than thirty minute visits. Thus as commissioners in one
LA (OM) explained, the outcome is much tighter costs control over.
We commission to the provider, half hour slots, pay for half hour slots, but.. some of those
care packages are no more than fifteen minutes….. But new care agreements will be -You‟ll
be getting fifteen minute payment for fifteen minute care package.OM
Another LA, HD, had also used retendering to simplify fee systems to one flat rate, removing
block and spot differences for the individual providers (although providers only doing spot
may have different rates) and removing additional payments for short visits. Another LA
EWERC
Part II. Commissioning and contracting in the selected local authorities
94
(ON) introduced in the period covered by our survey a move to payment by the minute as
registered by electronic monitoring. Not only did this replace the higher premium per half
hour visit that was in place when we visited the LA but it also introduced penalties for short
visits. As we explore in our case studies (see part V), some providers responded by giving an
incentive bonus to staff who stayed at least 25 minutes for a half hour visits. In the interim
period a flat rate £1 per hour fee was paid in addition to the timed minutes but this flat rate
fee was to be reduced in 2010 to only 60 pence. At XD electronic monitoring was explicitly
used to recoup some of the costs incurred by its policy of raising prices to allow for higher
basic wages among the domiciliary care providers. At IL the tightening of control over visits
was said to have arisen out of the change from block to spot contracting.
Travel time is not included in the price. It was „sort of‟ included in block which was taskbased so they did the jobs and then left to travel. The new tenders show times, for example 15
minutes, so there is no leeway for travel time. Service users are charged for 30 minutes, but
carers HAVE to leave to get to the next call on the rota and there is no time. On the schedule,
one call ends at 10 am and the next one starts at 10 am. Some calls are time critical e.g.
where there are medical needs. All of this is in the care plan, but if you leave a few minutes
early, we get complaints. The new charging went ahead without consulting us….the complaint
is not about the care, but about the charge. IL contracting
The commissioning department thought that travel time should have been factored into the
fee at which organisations tendered for work so that it was not the responsibility of the LA to
be concerned with travel time costs.
I think people should be paid for travel but I think that should be worked out when
organizations are bidding for work – how much they can do their business for per hour – they
should factor in that travel time. I think it should be included in the overall cost – when they
say we can do that for £10 70 an hour, they will factor in say, 70p for travel time. IL
commissioning
A number of LAs had moved away from block to spot or call off contracting in order to
improve the efficiency of use of providers as they were not able to make full use of all the
guaranteed hours ( for example AW, ON). The development of the personalisation agenda
was also increasing concerns among LA commissioners about being tied long term into block
contracts in case they would not have this volume of work commissioned through LAs in the
future. Commissioners at one LA (IL) justified the move from block to spot as giving the
providers an opportunity to prepare for the uncertainties under the personalisation agenda. In
another LA (ON) the move from block to spot was justified as a means of increasing
flexibility and reducing overhead costs but also the change was reinforced by awareness of
the personalisation agenda.
[It‟s] quite expensive to manage the blocks, because with home care people are absent in
hospital, respite, whatever, and you either accept there‟s a higher cost or you manage it at a
cost to make sure you‟re maximising the use, and with spot buying you pay for what you get.
And it used to be an argument, it always was argued that ... dom-care moved to blocks to give
stability and security, but in fact the good providers have either grown or stayed very stable
EWERC
Part II. Commissioning and contracting in the selected local authorities
95
since we moved to this, and we haven‟t had providers saying, „Oh, we do need blocks to give
us security.‟ And so on. So it‟s not proved to be a problem. And then with the personalisation
agenda anyway …ON
For the most part LAs did not pay extra for cases requiring more intensive care or more skill
on the part of the workforce. This tended to be different when there was joint commissioning
with the NHS for intermediate care where in principle care staff should be trained to NVQ
level 3 in order that they can carry out instructions from professional (nurses etc) staff. In one
LA (IL) these staff were notably higher paid and at a domiciliary care providers forum
attended by one of the project researchers the possibility of only using NVQ level 2 staff on
lower pay for those cases which were deemed not complex, said to be the majority of cases,
was to be explored by the LA.
Contingent commitments to provider support
Another dimension to the price versus quality trade off was the tendency for support to
providers through training provision to be in some cases contingent on the availability of
external funds to the LA. In one extreme case –XD- the training partnerships had been
entirely closed down due to a drying up of funding streams.
XD has no training partnership currently with independent providers. They used to have
[one]– managed by the LA but a change in funding meant that it collapsed. They are trying
to invest some money into the establishment of an employers‟ forum which they say is needed
because of the move towards self directed support and perceived demand for personal
assistance. XD
LAs with no inhouse unit for domiciliary care were also much less likely to be involved in
training independent providers. The implication of some comments might be that this joint
provision of training would only continue if LA staff still had a significant involvement in the
training.
we just have a huge demand for the basic training, so health and safety, manual handling, so
there‟s just huge demand, and the individual providers find it quite hard to catch up and
….you‟d be running huge programmes wouldn‟t you. Some of them have got 300 carers. We
couldn‟t possibly put that many through. RT
EWERC
Part II. Commissioning and contracting in the selected local authorities
96
II.2.3. Integration of social care and health
Perceptions of the need for integration
The LAs were found to be pursuing different agendas and strategies with respect to the
development of a more integrated or holistic approach to social care provision. Some had
moved a long way towards integration with health involving joint commissioning and pooling
of budgets- indeed one LA (AH) merged its adult social car and housing function with the
PCT- between the stage one survey and the stage two interview. The rationale for this
change was explained as:
The big two agendas for commissioning are the transformation of social care and
transformation of community health services- so we have pulled together our commission
intentions for both of those big agendas. AH
Some other LAs had not integrated that far with health but were nevertheless said to be
attempting to develop an integrated approach across for example social care and housing:
We have an approach of promoting universal services, not just about health and social care
and this where the link with housing is very important, because a lot of people have other
needs other than just health and social care, benefits needs, housing needs, general support
needs etc….…. Overall strategic direction is about independence, well being and choice, not
promoting institutional care. We have re enablement team (care at home) – 40% of people
receive 6 week intense re enablement, generally 40% less need for care packages. UY
Whether the integration is with health or with other aspects of social services, one of the
underlying motivations for a change of approach is a recognition that too many resources are
going in to residential care.
We‟re spending about forty percent of our budget on care homes. That‟s too much. It‟s
reducing, I mean we‟ve seen fairly dramatic reductions so I think you are beginning to see a
shift, but personally, I mean I just think that‟s far too much. But we need to do something that
provides a range of stuff at an earlier point. ON
At one LA (RT) commissioners expressed more radical views as to what should be happening
to social care services:
I mean, with residential care, and again, we‟d just stop using it. We‟d close it. It‟s a very
unhelpful model of care. And it makes people poor. It strips them of their assets apart from
anything else. I wish they‟d stop doing that. Again, this is all magic wand stuff. If you take
what we spend on residential care –…it‟s just millions upon millions. Well, if we took it out of
there and put it in our community support we could have a brilliant support. ….for example,
one of the major reasons that older people in particular lose their independence is an
increase in sensory impairment, particularly dual sensory impairment, so you can train a
homecare worker who sees them every day to start noticing sudden deterioration in their
EWERC
Part II. Commissioning and contracting in the selected local authorities
97
hearing or their sight and flag it up earlier. Plus they can do all the early stroke warning
stuff. I mean, we could really use this.‟ RT
The identification of the causes of this problem varied. For LK, the LA among our selected
14 spending the highest share of its older people‟s social care budget on residential care
(NHS Information Centre 2009b), commissioners thought the problem lay in the interface
between the hospitals and the care service, a problem in their case exacerbated by the rural
nature of much of the county.
One of the issues, my personal view, is the hospital system - no valid assessment before they
come out of hospital – they will be put into residential because it is hard to get a package for
them to stay at home.….There may be a rural aspect to this – complex packages more diff in a
rural area. You may need two carers, and this isn‟t happening as the providers can‟t or won‟t
provide it. LK
For RT, the LA where the commissioner interviewed would in principle like to close
residential care, the problem is short termism.
Instead all we do is, it‟s just like a sticking plaster job but actually what we could really have
is a real network of workers who are experienced and trained and know their area intimately,
and know the neighbours, and know what the support system is and they could support people
for ages with much better early warning signs of what‟s going on. RT
Hospital discharge as the driver of the care system
Awareness of the long term need for a more holistic approach to social care did not prevent
tensions developing between the social care and the health services. In one case (UY) the
performance regimes attached to a foundation trust were said to be stretching the availability
of care services which was only resolved by bringing in more suppliers on a spot purchase
basis.
We have great pressures at the moment, our district general hospital is a foundation trust so
they want throughput so it means we have to have services and interventions for people to be
discharged so we need to increase our services so we have preferred and then they approved
that we spot purchase.UY
In another LA (AD) the drive towards consolidation of commissioning around four block
contract providers was driven by problems of meeting the demands from the health service.
It was about growth. Like everybody else we were having difficulties with hospital
discharge…., there was basically just a blockage at the front end. So the idea was very much
about trying to create much more fluidity. AD
EWERC
Part II. Commissioning and contracting in the selected local authorities
98
Harmonising commissioning strategies
While in some LAs the key driver towards integration was the need for better services, in
other cases the driver was the efficiencies to be gained from joint commissioning and the
avoidance of competing approaches to commissioning within the same geographical space.
It is pretty joined up in that respect…., rather than us going out to tender for something and
them tendering for something similar. HD
„You avoid duplication …and the PCT would be commissioning dom care packages from
providers we had just decommissioned. LA and PCT pay different fee rates, and PCT pay
more than LA, even for cases where there is little health input. IL
In the case of one LA (RN) involvement with the PCT in joint commissioning was in fact
holding back a strategy of implementing a policy of fair commissioning based on financial
incentives for reaching quality standards for residential homes. The NHS staff had had less
experience of commissioning in social care and were convinced, on the basis of information
on lower prices in other LAs that it may be possible to bring down the costs of social care by
more aggressive commissioning strategies.
This procurement hub model [with the NHS] is more cost and block focused and less fairer
contracting! RN
II.2.4. User choice
The fourth policy agenda to impinge on LA commissioning and contracting was that of
personalisation or user choice. At the time of our interviews its main effect was in the
planning of future commissioning rather than on current practice but all LAs were actively
involved in considering the implications. Four types of implications were under
consideration: for the contracting form; for the organisation of care delivery on a
geographical basis; for the inhouse facility; and for the organisation of care assessments and
care delivery.
Form of contracting
The tendency to move away from block contracts that we identified was associated in six
cases (ON, RD, IL, OM, LK, AW) with an awareness of the possible incompatibility
between block contracting and user choice.
Well, there‟s no point signing three or four year contracts at this point, .. because, of course,
in terms of home care people may well start to exert their own personal choice. RD
We‟re just not gonna go near blocks, thinking about the future ON
EWERC
Part II. Commissioning and contracting in the selected local authorities
99
We have just tendered for 3 year contract, but built in break clause after 2 years so we can
assess where we are with personalisation agenda. UY
In two LAs (IL and TE) the changing of contractual relations from block to preferred
provider or spot was said to be a means of preparing the providers for the changes, but in one
LA (TE) there were concerns about moving too quickly because of the LAs continuing
responsibility for ensuring the availability of care.
The reason why providers need to build capacity into their organisations, is to prepare for the
personalization. In other words, they will be attracting their own customers, so they won‟t
need them coming from us anymore. ….and that is one of the reasons we didn‟t want to eat
up all their capacity with our own blocks. Apart from the fact that we didn‟t want to pay for
stuff we didn‟t want to use.IL
However we also need to make them aware about the implications of personalization. And
that has massive implications for the domiciliary care market, and particularly block
contracts, which we probably wouldn‟t want to have. So we‟ve got personalization events
with the independent sector – voluntary sector in April and private sector in May. It‟s about
raising awareness of the implications of people having personal budgets, about making sure
that people will be able to choose where they go. What we can‟t do is go the whole hog. We
can‟t afford to destabilize the market and then find that we can‟t fulfil our statutory function.
TE
Care delivery by geographical area
Considerable concern was expressed by LA commissioners over the implications of
personalisation for their contracting by geographical area. These arrangements had been put
in place to reduce travel times but were recognised to conflict with the notion of user choice.
In two LAs (AD and TE) commissioners were concerned that they would have to undo the
recent work they had undertaken to rationalise travel problems.
if one provider‟s working in the centre of AD and you live in the far west but that‟s the
provider you want to deliver your care, personalisation would say you can go and buy your
care from them but that does mean that all the work we did around reducing travel times,
which actually has an impact on the cost, starts to shift and change. AD
So the pain of splitting into the 5 neighbourhood areas was actually not necessary under the
personalization agenda really, because they can go wherever they like. TE
Two more LAs (IL and XD) had already however moved towards more than one provider per
area in response to the choice agenda
We were looking for 10 in order to offer a choice of providers in each geographical area
(ward). This is because if there is only one provider, service users don‟t have a choice and it
becomes a closed shop. Contracts said they could handle 8-10 providers.IL
EWERC
Part II. Commissioning and contracting in the selected local authorities
100
Future for inhouse provision
Some LA commissioners believed the personalisation agenda would lead to significant
changes in the inhouse provision of domiciliary care. In one LA (ON) there were concerns
that personal budgets were going to put pressures on the inhouse provision as the key issue
would be „whether the public want to buy our inhouse services and what‟s the unit cost
gonna be... That could be the big tipping poin‟t. ON
In another LA (AD) there were also concerns expressed that the inhouse provision might be
priced out by personal budgets but that the consequence would be a loss of skills and capacity
of re-ablement that would be difficult to replace in the local area. As a consequence more
radical options such a setting up the inhouse facility as a social enterprise were being toyed
with.
I think the issue is around considering whether... because of the quality of our inhouse service
and because of the skill levels of the staff, I think what we feel quite strongly is we would not
want to take that out of the marketplace in terms of a choice that the public would want to
take. ….our stall would be set out in the same way as all the other providers. We might be
more expensive but do we deliver a better quality service? …. it might be that the inhouse
service becomes a different kind of business model, I dunno, social enterprise, whatever. AD
A quite different approach to the impact of personal budgets on the inhouse facility was being
taken by another LA (RD). Here we were told that the change in policy was to be used to
legitimize a complete withdrawal from directly provided long term services.
We have a different plan. They don‟t know it, this is the problem. … Basically, we‟re gonna
allow individual budgets to be a driving force. No need for a workforce. Okay. When people
have choices over costs I think it‟s going to have a significant effect, isn‟t it? ….… It‟s going
to expose big cost differentials that are unsustainable. … This is not a sentimental authority.
There will be no subsidy. RD
Changes in care assessment and delivery of care
For the most part, at the time of the stage two interviews, few changes had been made in the
organisation of care assessments or in the planning and commissioning of care. In two LAs
(AD, OM) interviewees spoke of moving towards more responsibility for the provider, either
in undertaking assessment or in working out how a total block of hours over a week would be
delivered.
It‟s meant to actually specify outcome needs, rather than, she needs a wash at three o‟clock
on a Tuesday afternoon. There‟s an expectation that once they have those needs the provider
goes and works out the detail. I didn‟t want providers having to come back to us because they
thought somebody needed an extra twenty minutes... AD
Now, what we haven‟t done is to move the providers into a position where they are
fundamentally challenged, professionally, to provide assessments, cause the assessment is
EWERC
Part II. Commissioning and contracting in the selected local authorities
101
always undertaken by the authority as the local commissioner, and that has to change.….
OM
A third LA (RN) was engaged in a pilot programme on outcome based care, the principles of
which involved moving away from an hours target to outcome based target.
We give the providers a care plan, so rather than saying this is 12 hours and we‟ll pay them
for 12 hours, we say this is what we want for Mrs Smith and she‟ll be in charge of that and its
much more detailed and will be delivered reaching the goals and outcomes of Mrs Smith,
rather than us saying that‟s 10 hours Outcome based pilot RN
However, as we have seen in our discussion of price and costs based commissioning and
contracting above, these developments were very much in the minority of LAs. A stronger
trend was towards more detailed control of care delivery through electronic monitoring and
tight time specification of visits.
EWERC
Part II. Commissioning and contracting in the selected local authorities
102
II.3. Classifying the strategic approach
II.3.1. Typologising the local authorities
The LAs in our sample were clearly engaged in addressing four separate but potentially
conflicting agendas. Recognition of the need for provider support and development coincided
with strategies to take costs out and increase competition between providers. Likewise there
was both awareness of the need for LAs to develop a long term strategic approach towards a
more integrated and joined up system of social care provision and a recognition that the
personalisation agenda might reduce or weaken the strategic planning role of LAs in social
care provision in the future.
While all LAs were being pulled in different directions, there were nevertheless differences
expressed between the commissioners in the different LAs in their preferred strategic
approaches and in what they were doing to implement these approaches. Indeed the starting
point for this element of the project was that one might expect to find variations in
recruitment and retention of care staff influenced by differences in the approach taken by LAs
to commissioning and contracting. This hypothesis is backed to some extent by evidence of
divergent practices across LAs as indicated by the stage 1 postal survey and by the stage 2
interview survey. However, as table 3.8 shows the range of approaches pursued by the LAs
makes classification into neat and bounded categories somewhat problematic.
Thus the classification is based around multiple criteria. First we take into account the pricing
strategies of the LAs. Second we summarise in table II.8 the strategic approaches adopted by
the LAs focusing on evidence of an approach to partnership with the providers, in the sense
policies aimed at developing and stabilising the market, rewarding and promoting quality in
care and/or employment. We use these two criteria to classify the fourteen into three
categories:
o partnership focused;
o cost minimisation focused;
o or mixed.
Clearly all fourteen are „mixed‟ to some degree but we classify those as partnership focused
where they are either high payers and have a partnership orientation or medium payers and
have specific policies of promoting and rewarding quality.
Five LAs fall into the partnership category. This includes three of the four LAs classified as
„high‟ fee payers in figures II.1a and II.1b (AH, XD, LK) for both residential and domiciliary
care and all of which also face strong demand conditions for women‟s employment in the
locality (see section 1.7 and appendix table I.A1). All three combine high fees with either a
strategic partnership approach within an integrated NHS/LA unit (AH), a commitment to
allow independent providers to match inhouse basic pay levels (XD) or higher pay in rural
EWERC
Part II. Commissioning and contracting in the selected local authorities
103
areas and maintaining a high share of inhouse residential homes (LK). We also include UY
and RN in the partnership category. Both are „medium‟ fee payers when quality is not
included (figure 3.1) but RN moves into the high fee paying category when quality
enhancements are taken into account. RN also faces strong labour demand conditions while
UY is in the medium demand category. They are included here as they also have a forwardthinking approach to their providers. UY has a strategic approach, linked to its integration
into housing and has developed its own strong quality monitoring and incentive approach;
RN has a commitment to fair contracting and rewards good HR performance with bonuses to
be spent on staff. The quotes in box II.1 illustrate that these five „partnership LAs‟ have
focused on support, innovation, improving quality and developing the market.
Box II.1. The partnership LAs
The idea behind the block contracts was that providers had told us that they couldn‟t recruit and
retain staff because they hadn‟t got the guaranteed income and they didn‟t have a block contract
like the internal service, so we tried to replicate that[the internal service] …around salary levels
XD
For care homes we have just recently introduced a process called fairer contracting and that‟s
about actively encouraging higher quality and we want to work towards only contracting with good
and excellent care homes.
Each quarter they [domiciliary care providers] send performance indicators and a formula is used
to calculate the incentive payment which they will get each quarter – that‟s paid separately. They
have to prove that they use the incentive money on training, staff bonuses, staff incentives and team
building to encourage low staff turnover.RN
We target 70% of care workforce to have NVQ.LK
We have an approach of promoting universal services, not just about health and social care and this
is where the link with housing is very important UY
It‟s about the relationship with providers which is important – sharing our values, and looking to
achieve a principled outcome. Win win for us all - we get the services we want UY
I think the inflationary uplifts have already been agreed for the full duration of the contract which is
5 years, that differs quite significantly from other areas of commissioning .AH
The whole idea was that we wanted to create strategic partnership and therefore we would work
with fewer partners AH
At the other end of the spectrum four LAs fall into the category of „cost minimising‟. Two
(IL and HD) are classified as „very low‟ fee payers (figure II.1a and II.1b) and in fact pay
either very low (IL) or low (HD) fees for both domiciliary and residential homes. Moreover,
they have no quality uplifts; IL has removed its premium for iDPs and accepts that the
EWERC
Part II. Commissioning and contracting in the selected local authorities
104
consequence of low fees will be wide use of top up fees for care homes even in a low income
area. The third LA in this category, RD, is a low fee paying authority. It pays medium level
domiciliary care fees but prices its residential fees such that they require top ups, with low
income clients encouraged to use homes out of area that are cheaper. The fourth cost
minimising LA , AW, is a medium fee payer (high for residential but lower than the outer
London average). It has outsourced 100% of domiciliary care and is prepared to change all
suppliers on the basis of costs. Moreover, it has kept residential fees at low or zero uplift for
some time. These four LAS have very different local labour demand conditions, with HD
recording strong demand, AW and RD medium and IL low demand. Neither RD nor AW
commissioners wished to take an interest in the HR policies of providers as this might, they
felt, interfere with competition. The examples provided in box II.2 illustrate that interviewees
at these four LAs made positive comments about the flexibility and responsiveness of the
market, priced residential care at a level that they knew would lead to top up fees being the
norm, distanced themselves from responsibility for the HR polices of providers and treated
quality as an additional requirement, not something to be paid for. One LA, HD, had
previously made an attempt at partnership but had retreated due to conflicts over fees.
Box II.2. The cost minimising LAs
External providers just recruit people, they‟re very quick, they‟re very slick, very flexible.RD
I don‟t think you can be too prescriptive on HR issues [since] it would have a direct impact on the
rates we charged.. RD
Quite a lot of people are placed outside the borough where there is available space so RD would
pay their rates under a reciprocal deal. Within the borough many establishments charge top-ups, so
if people want to go into those homes there has to be a third party agreement. RD
The council doesn‟t really get involved in providers‟ HR issues In terms of conditions of service,
that‟s nothing to do with us in a sense. AW
We used to pay a premium for quality service, but not all organizations that met the quality
standards. Presumably, this was to bring up quality, because it was very low. Over time, the
quality of all services improved, so we were paying for quality when we didn‟t need to.IL
Approximately 82% charge top-up, in some cases this is a small amount (£10-15), sometimes it is
more, e.g. £355 from us, and the charge is £470. IL
The City Council has been committed for some years to working in Partnership. When Building
Capacity came out we did try and secure Partnership based on that. This is about six years ago
now, and at the time mainly with the residential sector there are big issues about fees and fair fees
and stuff, which kind of gets into the way. But we actually do have regular meetings with providers
HD
EWERC
Part II. Commissioning and contracting in the selected local authorities
105
This leaves five LAs (ON, AD, TE, OM, RT) that we categorise as „mixed‟ and in each case
there are strong elements of both cost minimisation and partnership. Three of the five are
very low payers, as defined in figure II.1a – ON, AD, OM- but move into the low paying
category (figure II.1b) if quality uplifts are included. One pays very low domiciliary fees
(AD) and one low fees (ON). Four of the five face weak local labour market demand with RT
the exception with medium levels of local labour demand. ON commissioners espoused a
partnership approach, but in practice have not only set low fee levels but also moved away
from their strong commitments to paying for travel time during the course of the project as a
consequence of moving to electronic monitoring (which led to the removal of the half hour
supplement). The authority did pay extra to homes with Investors in People awards but in
general had not progressed very far in thinking about how to promote quality.
„I think the thing we‟re beginning to consider… do we begin to link what we pay
against some level of quality and is that, you know, the kind of CSCI ratings or
something like that. And that‟s only a thought at the moment.‟ ON
AD also pays low domiciliary care fees but at present does not require the outsourced
providers to undertake complex work or indeed evening work with inhouse covering these
areas. Moreover, unlike ON, it pays high residential fees. Commissioners at AD had made
efforts to develop the market (through involving providers in person-centred care) and to
stabilise the market- for example by offering block contracts and then encouraging block
providers to offer guaranteed hours contracts- which were rebuffed.
Interviewees at both ON and AD in fact seemed to be expressing a desire to move to a high
trust approach but in practice were torn between that and ensuring value for money through
for example introducing electronic monitoring. These contradictions are summarised as
follows.
We‟re the local government who hold the service users and the purse strings, and we recruit
these people to do some jobs for us. But we don‟t really trust them. We‟re not really sure
they‟re not going to rip us off. And we‟re not really sure about whether we trust them to turn
up when they say they will. So it‟s still a very unsure market place to be honest. So the degree
to which we actually kind of move away from a task based processes is patchy, I think. AD
The other two low fee payers, OM and TE, pay medium domiciliary care fees, but do not
offer additional fees (for shorter visits or unsocial hours working). Nevertheless, both have
sought to develop a more strategic approach to their providers. OM has been expanding its
providers to use greater competition to boost quality and keep down prices but it also has a
strategy of its providers playing a greater role in assessments. In residential care it is
investing £800,000 in quality uplifts. TE comes closest among this category of mixed LAs to
a partnership approach with its focus on partnership and rewards for quality in both homes
and domiciliary care. However, interviewees reported that the process of change had been „a
very difficult situation, and the providers and the staff here and the service users went
through significant pain‟. The reorganisation had required a lot of TUPE transfer of staff
EWERC
Part II. Commissioning and contracting in the selected local authorities
106
between agencies and although the relations may settle down into a partnership approach a
mixed categorisation for the current situation seemed more appropriate.
The fifth LA in this mixed category, RT, is medium authority according to our figure II.1a
and figure II.1b classification. However, it is an outer London borough and therefore could be
considered (along with AW) to be a relatively low fee payer for the area. But it differs from
AW in that its commissioners were seeking to develop a partnership approach based on
longer term and renewed contracts with the providers and a commitment to working with a
wide diversity of organisations reflecting the diversity of the population. On the other hand,
however, it had underdeveloped links with the NHS and no retained specialised inhouse
services provision. RT managers also acknowledged serious contradictions in their approach
towards providers‟ HR practices.
In terms of workforce training and development, I mean, it‟s clear that practices that we
encourage because we want to keep the prices down, militate against having a properly
trained and maintained workforce. RT
EWERC
Part II. Commissioning and contracting in the selected local authorities
107
Table II.8 LAs’ strategic approach: from partnerships to cost minimisation
a.
Partnership LAs
LA
code
Fee level
AH
H/H
Without/
with
quality
Local labour
market
conditions
Strategy towards providers
Change within past 3 years plus plans for
change
Strong
100% joint NHS- integrated health and social care teams for re-ablement.
Social services and housing merged with PCT
(post PSSRU).
Strategic partners in dom care chosen 60/40 quality/cost. High paying but with
no variations by time/care.
RN
M/H
Strong
NHS joint commissioning/ 90% outsourced- additional support for providers
increased outsourcing (e.g. fire officer)- also in response to publicity on poor
care Guarantees providers 55% of work in an area.
To 5 strategic partners/more outcome based
approach. Away form unsocial hours payments
Outcome based care pilot.
Moving away from additional payment by
length of visit.
Fair contracting/quality uplift. HR related bonuses/ pay for weekends etc.
UY
M/M
Medium
Integrated with housing/ extra care
Specialised inhouse provision
Quality incentives and partnership approach
Quality monitoring now around excellence,
previously qualifications- no relation to star
rating.
XD
H/H
Strong
High and variable prices –costs offset by electronic monitoring and requirement
for services in rural areas. Built in continuity standards into contracts and
ensure wage levels adequate. High inhouse share due to similarity of prices and
problems of supply
2006 introduced block contracts by easy/difficult
area to change power balance and provide more
equitable conditions between independent sector
and inhouse (but end to unsocial hours payments
and costs offset by electronic monitoring).
LK
H/H
Strong
Fixed but variable price by area reflecting variations in availability across areamaximise recognised suppliers. Specialised inhouse. 70% target NVQ 2.
Political commitment to LA homes but high incidence of top up fees. Too much
capacity in homes/ too little in domiciliary care. Commitment to own
monitoring
Introduced fixed but variable price by area
EWERC
Part II. Commissioning and contracting in the selected local authorities
b.
108
Mixed LAs
LA code
Fee level
Without/ with
quality
Local labour
market conditions
Strategy towards providers
Change within past 3 years plus plans for
change
To payment by minute/ electronic monitoring
away from unsocial hours payments and pay
for travel
ON
VL/L
Weak
Partnership approach to stabilize the market but combined with value
for money. Pay for travel/training but moving to payment by the
minute.
RT
M/M
Medium
100% outsourced- strategy to develop the partnership and maintain
diversity of supply
AD
VL/L
Weak
High/specialised inhouse plus unsocial hours- routine out of house
but with person-centred care
Quality fees for homes- top ups only out of borough
Blocks with few providers since 2006-single
price- some personalisation. Plans to transfer
evening work.
High quality inhouse (3*).
OM
VL/ L
Weak
Enhancing role of providers in interests of performance and
personalisation. Increased competition through more providers.
Specialisation for inhouse. Quality fee uplift for homes. Quality
monitoring for both.
Increase in providers, from block to
framework agreement. Providers to make
assessments and more performance/ quality
oriented. Paying by minutes not in half hour
blocks. Plan to increase quality monitoring
with stronger HR focus.
TE
L/L
Weak
High share with NHS. Quality strategy- star rating raises home fees10% paid to IDPs if meet KPIs.Response to user survey through
enforced geographical reorganisation
Geographical reorganisation including TUPE
transfers. Fee rises to reflect costs but removed
higher prices for short visits. Large inhouse
redundancies 2006/7- no TUPE transfer as
independent sector expanded later
EWERC
Part II. Commissioning and contracting in the selected local authorities
c.
109
Cost minimising LAs
LA code
Fee level
Without/ with
quality
Local labour
market conditions
Strategy towards providers
Change within past 3 years plus plans for
change
AW
M/M
Medium
Price focused; prices to reduce over next three years for one IDP; 20
minute time slots and no pay for travel time; sets maximum fees for
homes- existing placements kept at lower levels/ zero increase in fees
for out of area homes. Requirement to meet user needs with respect
to diversity in contract. High number of LA TUPE transferred staff
Moved from 4 to 2 block contracts/ change of
all main providers. TUPE transferred staff had
to change provider.
IL
VL/VL
Weak
Price focused. Removed quality premium once threshold met.
Monitor but do not pay for quality. Allow wide use of top ups
From block to spot.
Removed quality premium.
Split between contracting and commissioning
HD
VL/ VL
Strong
Specialised inhouse plus area block contracts
Geographical reorganisation
specialisation of inhouse role
RD
L/L
Medium
Price focused. Use homes outside area as cheaper; fee set at too low
a level for own area .
Brought in new providers . Plans to end
inhouse for regular care.
EWERC
and increased
Part II. Commissioning and contracting in the selected local authorities
110
II.3.2.The coherence, stability and sustainability of LAs‟ commissioning and
contracting practices
While we have provided a categorisation of the commissioning and contracting strategies of
the LAs, a triangulation of the various sources of information on LA strategies and
approaches casts some doubts on the coherence, stability and long term sustainability of some
of the apparent differences in commissioning and contracting stances.
There was wide recognition of the existence of vicious circles that stood in the way of
developing a coherent and sustainable approach. For example in one LA (RT) interviewees
felt that the competition requirement for repeat tendering ( to comply with EU law) stood in
the way of developing the quality of domiciliary care providers in ways that would enable
them to move forward with the longer term objective of reducing reliance on residential care.
So instead of kind of focusing on really working with providers to try and develop those kinds
of things that we could do, we‟ve suddenly got this dreadful kind of treadmill of block
contracts, tenders, problems, you know, cut the price down. …and you just go round and
round in this awful circle instead of really focusing on what you should spend your money on
to improve the standards.RT
At another LA (LK) officers were concerned that those concerned to reduce hospital
discharge delays were too ready to move patients into residential care, a problem
compounded by the difficulty of putting together care packages in rural areas. At OM the
concern was that personalisation would reduce the strategic role of LAs in managing the
social care market thereby leading to a major increase in the price of care services. Others
such interviewees at TE and AD feared that personalisation would make it more difficult to
minimise the problems of travel and create more problems in guaranteeing supply. Other
concerns included whether specialist re-ablement services built up by LAs inhouse might not
be financially viable under personalisation (AD, ON). Innovative re-ablement services
provided by integrated health and social care teams (AH) might be the strategic way forward
to reduce residential care but whether further development along these lines might require
reducing the share of outsourced work was unclear. At another LA (HD) concerns were
raised over how „extra care‟ specialised housing schemes could be managed under
personalisation.
The model of the extra care scheme is to have the care provider obviously on site and
delivering services as a domiciliary care provider in the individual homes. And for that to
work as it does as the extra care model there‟s always got to be an element of block within
that. But then there could also be an element of people having their own care provider (HD).
Some of the contradictions arose simply out of the different regulations and pace of change
under different budget headings. For example XD had been forced to withdraw temporarily
from supporting providers in their training provision due to the sudden cutting back of
government funds under different budgets to support such training. This decision was at odds
with their more partnership approach.
EWERC
Part II. Commissioning and contracting in the selected local authorities
111
In some cases we found examples of incoherence and contradictions in the policy approach
that were already calling into question the longevity of current commissioning approaches.
For example, at one LA (IL) there was some recognition that their flat rate fee and spot
contract system was causing some problems of delivering care for complex cases that they
were having to recognise how far the flat rate system could be maintained.
So we have hot spots around the city where it is really, really difficult to get care, and if you
talk to an agency, they will say it is because we have difficulty recruiting in those particular
areas. And because it‟s spot, they say it doesn‟t enable them to plan very well. IL
Another challenge to current policies might come from the response by providers. For
example one LA (LK) had raised their price significantly for rural providers but
commissioners were not convinced that this increase was being passed to care workers in the
form of paid travel time. If this proved to be the case then support for the higher prices might
wane.
In the case of RN the decision to increase joint commissioning with the NHS was directly
causing a problem with the implementation of RN‟s fair contracting policy. The NHS was
regarded as new to the game and was requiring RN to go through the motions of seeing if
they could reduce prices, while the LA officers felt they had already explored that route and
knew that they needed to do more to improve the quality rather than going for the lowest
priced service. Nevertheless it was unclear whose approach would win out.
The interviews with the LAs also brought out the difficulty of classifying commissioning
approaches by reference to government policy agendas for in a couple of cases the LAs
made it clear that they were openly embracing a particular policy agenda in order to achieve a
specific objective which was independent of the policy agenda itself. The clearest example of
this was in the case of RD where the personalisation agenda was said to offer a justification
for closing down the inhouse social care team for more routine work, a policy which was
being pursued primarily as a cost reducing agenda. And at IL we were told by the contracting
officers that the decision to end block contracts and move to spot contracts was for cost
reason but the commissioning officer legitimised the move as a way of helping IDPs prepare
for personalisation.
One of the most consistent findings from the second stage interviews was that there was a
continuing rapid pace of changes in all aspects. Table 3.8 in its last column summarises the
main changes in policy that had been implemented over the three years prior to our interview
together with any changes that took place after our interview and before or during the
telephone survey and future planned changes. These summarise the high level of change.
Some of the frequent changes that had taken place included moving away from block
contracts, decreasing or increasing the number of providers, moving away from enhanced
payment for short visits to single flat rate minute-based payments through introducing
electronic monitoring, introducing more quality monitoring and more fee enhancement
related to quality, enhancing re-ablement functions, particularly inhouse, movements towards
more user-centred care or more involvement by providers in assessments and stronger
EWERC
Part II. Commissioning and contracting in the selected local authorities
112
geographical divisions between providers. As we discussed above, many LAs were said to
have plans for more outsourcing and some were engaged in plans to develop or expand joint
commissioning with the NHS. All were developing some response to the personalisation
agenda and many mentioned possible ways in which they may have to reverse their previous
changes or at a minimum make adjustments to their policies to fit the personalisation agenda.
Examples of significant changes that occurred within the period we were looking at the LA
include the change in payment arrangements and electronic monitoring in ON, the merger
with the PCT in AH (after the stage 1 survey), moves away from additional payments for half
hours at RN, contracting with more providers and moving to payment by minutes rather than
enhance pay for short hours at OM.
In addition to a fast pace of current change it also become apparent that what had seemed the
right strategy in the past had in some circumstances proved to be a disadvantage in the
current policy climate. This was particularly the case where LA had outsourced all or almost
all of their domiciliary care and to do so had TUPE transferred a large number of staff. Not
only was this adding to the cost base for these LAs but the legacy of TUPE transferred staff
was causing problems in developing a pricing structure for personalised budgets as
individuals were unlikely to wish to pay the higher prices that agencies with TUPE
transferred staff typically receive from the LA.
With hindsight we‟d have been better doing what some other councils have done, which is to
take their inhouse workforce, either retain it inhouse, or put it out to one organization but
then to use that for re-ablement AW
Where a high share of domiciliary care work had been outsourced, as in AH, there was the
possibility that this may not provide the best arrangements for the future when cost savings
might in the future come more from specialised re-ablement which may be better developed
by LAs directly or in partnership with the NHS.
The overall finding is thus of a high rate of changes plus a considerable likelihood of change
in different directions over future years. This uncertainty over the future was well captured by
the comment by a TE officer that they had started off developing a ten year strategy for
health and social care for older people in the city but „we soon discovered that that was
completely wrong, that the world was changing too fast for us to have a nice plan for 10
years, so we have reviewed it and we are redoing it.‟ (TE)
EWERC
Part II. Commissioning and contracting in the selected local authorities
113
II.4. The selected LAs and user satisfaction surveys
We complete this investigation of the commissioning practices of our selected LAs and their
approach towards the providers of care, whether IDPs or residential homes, by drawing on
published evidence of their relative scores in user satisfaction surveys. These satisfaction
scores were analysed only after we had undertaken the classification of our LAs. They
therefore provide an interesting test as to whether our classifications have any linkage to user
satisfaction scores.
We have computed average scores for both the overall level of satisfaction with care and for
each of a series of eight questions on care quality. The average scores for the overall level of
user satisfaction (a scale of 1 to 10) for the 14 LAs do not vary greatly. The range of scores
for LAs classified by partnership orientation of the LA is as follows:
Partnership (AH, RN, UY, XD, LK): 5.67 – 5.87;
Mixed (AD, RT, ON, OM, TE): 5.47 – 5.84;
Cost minimising s (RD, AW, IL, HD): 5.44 – 5.52.
Further interrogation of the rankings of each LA among the group of 14, however, reveals
significant patterns.20 Table II.9 presents the average rank scores for all nine questions for
each of our three categories of LAs - partnership, mixed and cost minimising. For the first,
overall satisfaction question the data reveal that while the partnership and the mixed
categories have quite similar levels of satisfaction, the cost minimising LAs are clustered at
the bottom of the distribution. A similar pattern also applies to the averages for the other
eight questions as indicated by the very low average ranking for cost minimising LAs,
ranging from 8.0 to 12.0. In contrast the average rankings for the partnership LAs were
between 5.2 and 8.8 and for the mixed LAs between 4.0 and 7.0. This evidence therefore
appears to provide some support for the more partnership oriented LAs generating higher
user satisfaction.
Table II.10 presents the rank scores for each of the LAs separately for the overall satisfaction
question, the average ranking for the other 8 questions and a total rank score. Five LAs stand
out as having very consistent high rankings: two are from the partnership category- AH and
UY and three from the mixed category – AD, TE and OM. It should be noted that AD had a
very large inhouse provision and these ranks relate to the provision by the LADP as well as
the IDPs. The five are in the top five rankings on both measures so that their average ranks
were 4 or less, while the next in line is LK another partnership at 6.5.
20
Use of ranking scores rather than actual satisfaction scores also preserves anonymity of LAs. Scores for the
separate questions were standardised in order to facilitate comparison across answers. This was necessary due to
the use of different scales for questions, including a 1-7 scale for question 1, a 1-5 scale for question 6 and a 1-4
scale for questions 2-5 and questions 7-9. The 14 LAs were grouped into the three defined types of partnership,
mixed and cost minimising and an average score calculated for each question for each type.
EWERC
Part II. Commissioning and contracting in the selected local authorities
114
Table II.9. Average ranking of user satisfaction scores by type of LA
Partnership
(AH, RN, UY,
XD, LK)
Mixed
(AD, RT, ON,
OM, TE)
Cost
minimising
(RD, AW, IL,
HD)
Q.1. Q1: Overall, how satisfied are you with the help from
[Social Services] that you receive in your own home?
5.2
6.2
11.8
Q2: Do your care workers come at times that suit you?
7.0
4.4
12.0
Q3: Are you kept informed, by your home care service, about
changes in your care?
5.8
5.8
11.8
Q4: Do your care workers do the things that you want done?
5.2
6.6
11.3
Q5: Are your care workers in a rush?
5.8
7.0
10.3
Q6: Do your care workers arrive on time?
8.8
4.0
10.3
Q7: Do your care workers spend less time with you than they
are supposed to?
5.6
6.4
11.3
Q8: Do you always see the same care workers?
8.4
6.2
8.0
Q9: Overall, how do you feel about the way your care
workers treat you? (e.g. whether they are understanding and
treat you with respect for your dignity)
6.0
6.0
11.3
Survey questions.
Note: LAs ranked by average scores with highest satisfaction ranked 1 and lowest 14.
Source: NHS Information Centre 2009a Home Care Survey 2008-2009, own compilation.
Two more partnership LAs - XD and RN - come next at 8.5 followed by ON, a mixed LA, at
9. The lowest satisfaction scores include all four cost minimising LAs along with the mixed
LA, RT. The rank scores are 9.5 for AW and 11 for RT, the two outer London boroughs, and
11, 12 and 14 for the other cost minimising LAs.
These satisfaction scores thus provide support for the categorisation of the LAs as cost
minimising but suggest that there may be some aspects of quality commissioning we are not
capturing particularly for the three mixed LAs with high scores – TE, AD and OM. We have
already suggested why AD may be in this category and TE is the LA we identified as closest
to our partnership category. OM was going through a period of change at interview so it is
difficult to know whether the changes will lead to a reinforcement or reversal of these high
satisfaction scores, if there is indeed a connection between commissioning and contracting
and these user outcomes.
EWERC
Part II. Commissioning and contracting in the selected local authorities
115
Table II.10. Ranking of user satisfaction scores by individual LA*
LA
Type of LA
Rank for question 1
Rank by average of
ranks for questions 2-9
Average of column 2
and 3
UY
Partnership
1
1
1
TE
Mixed
2
3
2.5
AD
Mixed
5
2
3.5
AH
Partnership
3
5
4
OM
Mixed
4
4
4
LK
Partnership
7
6
6.5
XD
Partnership
6
11
8.5
RN
Partnership
9
8
8.5
ON
Mixed
8
10
9
AW
Cost minimising
12
7
9.5
RT
Mixed
13
9
11
IL
Cost minimising
10
12
11
RD
Cost minimising
11
13
12
HD
Cost minimising
14
14
14
Note: Scores based on responses to 4, 5 or 7 point scale. LAs ranked by average scores with highest
satisfaction ranked 1 , lowest 14.
Source: NHS Information Centre 2009a Home Care Survey 2008-2009, own compilation
EWERC
Part II. Commissioning and contracting in the selected local authorities
116
II.5 Summary and conclusions
In line with the findings from the first stage survey of LAs, we found significant variation in
the specific practices adopted by our selected LAs with respect to commissioning and
contracting, particularly in the case of domiciliary care, although some general trends can
also be detected. In both domiciliary and the care home sectors the majority of the service
had been outsourced to the independent sector and further outsourcing was planned.
Nevertheless most interviewees anticipated keeping some inhouse provision, although this
would be increasingly focused on specialised re-ablement services and none were planning
any TUPE transfers of existing LA staff. Indeed those that had TUPE transferred staff in the
past believed this to have been a strategic error. Contracting in domiciliary care had in many
cases moved away form block contracting and instead LAs were establishing a set of
preferred providers, in part as a cost efficiency measure to reduce risks of unused hours but
also in preparation for the personalisation agenda. However, five still used block contracts
and two had recently moved to such contracts. In the care home sector the majority of
contracting was on a spot basis, following the preferences of the user. Twelve of the 14 LAs
did still provide some residential home care inhouse and ten had some block purchase
contracts with independent sector homes.
Pricing strategies also varied between LAs. In domiciliary care there was a general trend
towards simplification of fees around a standard fee with many LAs not making any
differences in payments for shorter visits, unsocial hours, higher dependency of users or
travel time, although some had introduced more differentiation between rural and urban
abased agencies. However, although the trend was towards a single rate, in eight LAs fees
still varied by providers according to their tender price. Nevertheless overall the average fees
only ranged from £10.45 to £14.50 for 13 LAs and the range among providers within a
locality rarely exceed £2 to £3. One LA was an exception on both counts with a range from
£16 to £28. The main motivation for the simplification strategy tended to be to reduce both
direct costs and transaction costs for the LA. Likewise the move towards use of electronic
monitoring was primarily driven by the interest of reducing costs and ensuring clients
received their full visits. Only two LAs offered any IDPs any quality enhancement to their
fees for meeting quality targets.
Variations in fees for residential care were much wider than for domiciliary care between
LAs and reflected regional variations in housing costs, not just wage costs. However, the
level of fees set did not simply reflect local conditions as in some LAs the policy was to set
care home fees at a level where it most LA funded clients would not be faced with requests
for top up fees unless they had a special room of some kind. Other LAs expected most
residents would be asked to pay top up fees because of the low level of their fees relative to
local home fees for private clients. More LAs had introduced quality enhancements for
homes with five currently offering quality premia and a sixth offering extra to those with
Investors in People awards.
EWERC
Part II. Commissioning and contracting in the selected local authorities
117
The variation in commissioning and contracting practices was found in our qualitative
interviews with key actors to reflect different priorities and approaches adopted by LAs in a
context where each LA was being required to make sense of a range of potentially conflicting
influences on commissioning practices. We found social care commissioning not only to be
influenced by the specific council‟s organisational, budgetary and political environment but
also influenced by the longer term policy agendas for the development of social care. Policies
towards commissioning were found to generate competing agendas from the need to support
providers and develop the supply base to the need to take costs out and control price even in a
context of policies aimed at driving up the quality of care delivered. Further competing
agendas stemmed from whether commissioning would in the future continue to be dominated
by LAs or either undertaken jointly with the NHS or devolved to users.
While all LAs were being pulled in competing directions, we were able to identify
differences between LAs in their espoused strategic approaches and in their implementation
of policies. We therefore classified LAs according to their concerns to develop partnerships
with independent providers on the one hand and to reduce costs on the other hand. This gave
rise to three groups of LAs: partnership focused; those focused on cost minimisation; and
those falling into a mixed category. This classification was found to have some resonances
with the national user satisfaction scores as recorded by LA, with the cost minimising LAs
assessed by users as providing less good quality care than the partnership or mixed
categories. Some of the mixed category LAs topped the user satisfaction scores and in one
case there was a particularly high share of LA directly employed staff in a 3* rated unit
providing domiciliary care services, suggesting perhaps that it is share of services outsourced
as well as commissioning strategies towards the independent sector providers than may
influence user satisfaction scores.
While we have provided a categorisation of the commissioning and contracting strategies of
the LAs, a triangulation of the various sources of information on LA strategies and
approaches casts some doubts on the coherence, stability and long term sustainability of some
of these apparent differences in commissioning and contracting stances. Above all there was
a very high rate of change in commissioning policies, some of them implemented during the
course of our project. This rate of change reflected both the changing commissioning
environments and the recognition of potential contradictions between some of the LAs‟
objectives and its current commissioning approach. It was thus not necessarily the case that
the commissioning strategies were sufficiently stable and coherent for independent providers
to be able to act on the practices to develop different approaches to managing the social care
workforce. Furthermore it was also increasingly the case that LAs were becoming reliant on
national providers. Some LA commissioners were concerned about the quality of these
providers and about the impact on of their growth on the local supply chain and their ability
to foster a diversified supply of care provision but nevertheless most LAs were increasing
their contracting with national chains. LA commissioners were also aware that their current
policies were vulnerable to future changes in central government policy which might, for
example, reduce the finance available for social care or even reduce the role of LAs in the
planning and commissioning of care due to the health integration and personalisation
agendas.
EWERC
Part III. The provider telephone survey
118
III. The Provider Telephone Survey:
Recruitment, Retention and Employment
Conditions
This part of the report presents the key findings concerning recruitment, retention and
employment conditions for the social care workforce. The analysis draws on the telephone
survey sample of 105 independent providers, including 53 independent sector residential and
nursing care homes (referred to as homes) and 52 independent sector domiciliary care
providers (referred to as IDPs). The data are complemented by interviews with 10 of the
Local Authority domiciliary care providers (referred to as LADPs).21 This original dataset,
which comprises a quantitative dataset and qualitative open-ended responses to questions,
forms the basis of analysis for this part of the report as well as part IV. Our objective here is
to present an introductory mapping of the descriptive statistics in order to address a set of
first-order questions:
what types of HR practices are in use within the sector?
how much variation of practice is there both between homes, IDPs and LADPs
and within these categories?
do all providers face similar recruitment difficulties and staff retention
problems?
An understanding of both the range of approaches to human resource management deployed
by individual providers and the key employment outcomes and differences therein between
IDPs, homes and the LA sector is a necessary first step in our knowledge before undertaking
a more detailed and complex analysis of the data in Part IV. There, we interrogate the
underlying factors that are associated with good HR practices and good HR outcomes and test
the statistical significance of the impact of provider characteristics on the one hand and
external commissioning and labour market factors on the other in explaining variations in HR
practices and outcomes. As such, it is the combination of results in both parts III and IV that
generate our conclusions concerning the role of internal factors and external environmental
conditions in shaping HR practice and recruitment and retention performance.
21
Two of the fourteen local authorities had no in house provision and interviews were not possible with the
other two due to pressures of restructuring and other issues.
EWERC
Part III. The provider telephone survey
119
This part of the report is structured into six sections with each section presenting a map of
results for homes, IDPs and LADPs related to a particular area of employment organisation
as follows:
III.1. Recruitment and selection
III.2. Retention
III.3. Pay and rewards
III.4. Working time and work organisation
III.5. Employee training and development
III.6. Performance management, job autonomy and employee voice
EWERC
Part III. The provider telephone survey
120
III.1. Recruitment and selection
Recruitment and selection practices are a core element of what care organisations do and are
instrumental in improving their performance. But to what extent do we find similarity of
approach across the different care organisations? For example, one issue highlighted in our
literature review (see section I.3) is variation in use of formal and informal methods of
recruitment. On the one hand, all organisations are being nudged towards greater formality by
the inspection processes of the CQC and the commissioning local authority. On the other
hand, providers may benefit from an informal approach to connecting with people with a
known reputation. In this section we investigate this issue and other issues related to
providers‟ approaches to recruitment and selection. Throughout we disentangle the variation
between homes and IDPs and, where appropriate, LADPs. We begin with an overview of the
extent of recruitment difficulties reported by the care organisations surveyed.
III.1.1. Recruitment difficulties
Our survey evidence reveals that one third of care organisations reported difficulties in the
recruitment of care staff, ranging from quite difficult to very difficult. The reasons underlying
these difficulties are likely to vary. While much depends on the conditions in the local labour
market – the presence of competitor organisations, the level of unemployment and the
availability of a suitable pool of job applicants – difficulties may also result from poorly
managed recruitment procedures, an inadequate pay offer, or inappropriate working-time
conditions. Here we set out a general assessment of patterns. The analysis in part IV
investigates the underlying causes.
Figure III.1. Percentage of organisations reporting the ease or difficulty of recruiting
care workers
45
Homes
IDPs
LADPs
40
35
Percentage
30
25
20
15
10
5
0
very difficult
quite difficult
neither difficult nor
easy
quite easy
very easy
Note: Total responses: 53 (homes), 51 (IDPs) and 10 (LADPs). Missing responses: 1 (IDPs).
EWERC
Part III. The provider telephone survey
121
The type of care organisation matters in explaining the likelihood of recruitment difficulties.
Recruitment difficulties were more likely to be experienced by IDPs than by either homes or
LADPs (figure III.1). Although more homes - at 11% compared to 6% of IDPs - said
recruitment was very difficult, only 17% of homes compared to 33% of IDPs said recruitment
was quite difficult. Among LADPs a far smaller share reported difficulties – just 20%.22
Homes were more likely than IDPs to report recruitment of care staff to be quite easy or very
easy – 56% and 41% respectively. And while only 40% of LADPs fell into this category,
another 40% reported recruitment to be neither difficult nor easy, far higher than the shares
reported for IDPs and homes.
While these results point to significant problems in recruitment of care workers, our evidence
also reveals that the recessionary conditions of 2008-2009 had in fact made matters easier for
around one third of the care organisations surveyed. The UK unemployment rate increased
sharply from 5.5% to 8.1% between the second quarter of 2008 and last quarter of 2009
(ELMR 2010). After a decade of relatively stable unemployment at around 5-6%, employers
therefore suddenly faced a changed set of external conditions with greater numbers of people
applying for vacancies.
I think there‟s been a real shift with the economic climate. A year ago I would have said very
difficult I think at the moment I‟d say it‟s in the middle. (RD.D.2.CL)
I think it‟s very easy … Since last year I think vacancies have gone down mainly because of
the credit crunch affecting overall everybody. (RD.H.1.B.S)
At the moment I would say a 5, very easy, because we‟ve had such a response for our
vacancies. We‟re having to filter them at the moment because we‟ve had so many, there are
just so many people wanting the post, it‟s not always been like that, it‟s changed.
(RD.HN.4.C.N)
Table III.1. Change in recruitment conditions as a result of the 2008-2009 recession
% of homes
% of IDPs
% of LADPs
% of all
No change
63.2
25.6
28.6
42.0
Some change
36.8
74.4
71.4
58.0
Recruitment easier
34.0
62.9
71.4
51.1
Recruitment more difficult
2.8
11.5
0.0
6.9
Total Responses
38
43
7
88
No response
15
9
3
27
Again, however, the experience was not shared equally among all organisations (table III.1).
Domiciliary providers, both independent sector and local authority, were more likely to
experience an easing of recruitment conditions, probably from a more severe situation of
22
In the last 12 months, 3 LADPs and 2 IDPs did not recruit at all while all homes had recruited new care
workers.
EWERC
Part III. The provider telephone survey
122
shortage than applied to homes prior to the recession. Thus, the gap reported above between
homes and IDPs would have been even wider were it not for the impact of the recession.
As anticipated, the reasons for recruitment difficulties were varied and encompass both
internal organisational factors and external labour market and other conditions. The
responses from providers surveyed suggest that pay is the most common factor (table III.2),
a result of either too many competitor employing organisations offering higher rates of pay
or the inability of the care provider to offer a rate of pay commensurate with people‟s
expectations of the value of the job. More than one in four respondents recorded pay as a
main reason. Pay was an especially common reason among IDPs, accounting for more than a
third of responses. It was also the most common response among care homes. However, it is
significant that it was not reported as a main reason by the LADPs that responded to this
question – a clear reflection of the higher rates of pay offered by local authorities (see III.3
below). The following quotes illustrate the differences:
It is the price that the LA pays – it is low pay. It is the nature of the contract. If they pay us
more we pass it on. (AH.D.4.DS).
No [pay is not an issue]. To be honest that is because in the local authority we pay manual
grade 5 plus 33.5% enhancement for working anti-social - for example for mobile night
workers - plus they get essential car users and mileage. (IL.DIH.1.CP).
A second important reason for recruitment problems concerns the nature of care work.
Respondents told us they believed that for many people the job of a care worker was too
emotionally demanding. They also emphasised the generally poor status of the work, a fact
that was obviously tied to the low pay.
It is very poorly paid and involves a lot of hard work, including both mental and physical,
with a lot of pressure on people, especially with new legislation demands. (RD.D.1.C.S).
This type of work doesn‟t have a particularly valued reputation among a whole lot of people
… You need a terrific sense of … well, you‟ve got to be an angel (RD.D.2.CL).
Aside from pay, the other HR practice that created problems for many care providers was
the working time schedules. This was reported as a factor by twice the number of IDPs as
homes, reflecting the predominance of far more flexible working-time contracts in IDPs.
The 24/7 demands for work, especially the requirement for regular weekend working were a
particular issue for several organisations, an issue we explore further below (section III.4).
Other reasons set out in table III.2 relate explicitly to changes in the external environment,
usually in the immediate locality. These include problems of local competitors – newly
opened supermarkets were often mentioned by respondents – as well as observations of a
„transient community‟ and the frustrating practice whereby some people registered as
unemployed apply for a job primarily in order to satisfy job search requirements.
My bugbear is that people telephone for the paperwork and you arrange 25 interviews and
only 6 show up. They don‟t come. And they only apply so that they can be seen to be
applying to get the benefits. (TE.H.3.AS).
EWERC
Part III. The provider telephone survey
123
Table III.2. Main reasons for recruitment difficulties
% of homes
% of IDPs
% of LADPs
% of all
Pay
19.9
37.3
0.0
27.1
Nature of care work
10.0
7.9
33.3
10.3
Local Competitors e.g. new supermarkets
10.0
9.8
16.7
10.3
Transport costs
10.0
11.7
0.0
10.3
Working time Schedules
6.0
11.7
16.7
9.4
CRB delays
4.0
9.8
0.0
6.6
High or low local employment
8.0
5.9
0.0
6.5
Not suitable/ Calibre of staff
12.0
0.0
0.0
5.6
Location
6.0
0.0
0.0
2.8
People apply so that they can stay on benefit
6.0
0.0
0.0
2.8
Reluctant to train
4.0
0.0
0.0
1.9
Working conditions
0.0
3.9
0.0
1.8
Its a transient community
2.0
0.0
16.7
1.9
Visas
2.0
0.0
0.0
0.9
Can‟t drive
0.0
1.9
0.0
0.9
Childcare
0.0
0.0
16.7
0.9
Total responses
50
51
6
107
No response
3
1
4
8
While the above results concern general recruitment difficulties faced by care providers,
more specific detail can be ascertained by focusing on particular types of job posts that need
to be filled. Around half the sample of care organisations reported specific shortages. By far
the most common shortages were for jobs requiring weekend work and unsocial hours and for
night work (table III.3). The data show a clear divide between care homes and IDPs; specific
shortages were far more likely to be reported among the latter – 77% of IDPs compared with
25% of homes. The difficulty of finding people to fill weekend work and unsocial hours was
reported by more than two thirds of IDPs compared to less than one in ten homes, and night
work problems were reported by 37% of IDPs and 15% of homes. LADPs fell somewhere
between the other two types of care organisation with 40% reporting specific shortages, again
with respect to jobs requiring unsocial hours working.
Given the range of difficulties reported by the surveyed care organisations, it is important to
investigate what types of recruitment and selection practices are utilised, and how practices
vary across different organisations. We address these issues in the following section.
EWERC
Part III. The provider telephone survey
124
Table III.3. Labour shortages for specific job posts
% of homes
% of IDPs
% of LADPs
% of all
Are there any specific shortages?
Are there shortages for weekend work and
unsocial hours?
Are there shortages for night work?
24.5
76.9
40.0
49.6
7.5
69.2
20.0
36.5
15.1
36.5
30.0
26.1
Early morning
0.0
7.7
0.0
3.5
From particular geographical areas
0.0
3.8
0.0
1.7
Trained staff
3.8
0.0
0.0
1.7
Bank Holidays
0.0
1.9
0.0
0.9
Males
0.0
1.9
0.0
0.9
Day shifts as all on specific courses
1.9
0.0
0.0
0.9
Drivers
0.0
1.9
0.0
0.9
Total Responses
53
52
10
115
III.1.2. Recruitment practices: attracting a suitable pool of applicants
Organisations in all sectors of the economy can be expected to use a range of informal and
formal methods to fill vacant posts. The organisations surveyed in the care sector as part of
our study fit with this notion of an eclectic approach. In particular, we find that three
practices were relatively common – the informal practice of advertising vacancies by word of
mouth, the more formal method of paying for ads in the local press and the similarly formal
method of contacting Job Centre Plus. Each of these practices was reported by at least three
in four organisations.
Figure III.2 charts the range of responses for homes and IDPs, ranked by the most popular
recruitment practice for each. Both IDPs and homes appear strongly wedded to the informal
practice of advertising through word of mouth – close to 80% of homes and 90% of IDPs.
One domiciliary provider explained that this involved asking people who worked for her to
„recognise people with the kind of personal qualities we are looking for‟ (UY.D.1.C.L) and
another told us that this informal approach extended to „people literally walking through the
door and asking for a job application‟. It was a less frequent practice among LADPs (just
40%), possibly because of the more formalised processes associated with LA HR
departments. The similarly informal method of posting ads in office or shop windows was
less likely to be reported overall, but nevertheless was a regular practice among one in five
homes and, perhaps surprisingly, almost half of IDPs; the popularity of this method amongst
IDPs is probably explained by the fact that many have a shop front. As might be expected,
given the scale of their organisation, the relatively formal practice of using internal
advertisements was especially popular among LADPs; two in three reported this practice.
Many organisations also retained lists of interested applicants, made up largely of people who
had registered interest at a time when the organisation was not recruiting; close to two fifths
of care homes used such lists and one quarter of IDPs.
EWERC
Part III. The provider telephone survey
125
Figure III.2. Diverse recruitment methods used to fill vacancies for care work
a. Homes
100
90
80
Percentage
70
60
50
40
30
20
10
0
Ra
dio
i
cru
et
afl
en
en
n
me
op
ps
nt
dro
s
e
tm
-in
A
HC
UK
Re
Le
op
Dr
et
loy
ag
da
ge
ys
ta
ts
y
nc
n
ca
es
pli
s
ci e
ap
ow
g
l le
co
in
er
mp
oth
oe
ern
Int
et
Fe
ing
Us
ing
ind
ert
ted
es
ter
nw
tis
f in
to
ei
tic
r
ve
Ad
Lis
No
v
ad
l us
eP
ntr
ing
th
tis
ou
er
dv
fm
al
Ce
a
ss
do
ern
Int
b
Jo
e
Pr
or
W
b. IDPs
100
90
80
Percentage
70
60
50
40
30
20
10
0
Ra
dio
tm
to
ps
en
dro
s
A
HC
UK
i
cru
-in
et
afl
Re
Le
op
Dr
et
ge
s
ay
ta
nd
n
me
ts
y
nc
n
ca
es
pli
s
ci e
ap
en
pe
loy
ag
ow
g
l le
co
in
er
mp
oth
oe
ern
Int
et
Fe
ing
Us
ing
ind
ert
ted
es
ter
nw
tis
f in
to
ei
tic
v
ad
l us
eP
ntr
al
r
ve
Ad
Lis
No
ern
Int
ing
th
tis
ou
er
dv
fm
Ce
do
a
ss
b
Jo
e
Pr
or
W
Note: Total responses: 51 (homes), 51 (IDPs) and 9 (LADPs). Missing responses: 2 (homes), 1 (IDPs) and 1
(LADPs).
Two formal methods also dominate the approach to recruitment among care providers of all
types. First, four fifths of all organisations that responded to our survey said they used adverts
in the local, regional or professional press. The breakdown among type of organisation is
68% of homes, 77% of LADPs and 92% of IDPs. Second, 72% of responding organisations
said they relied on Job Centre Plus as a normal method for filling vacancies. Again, this more
EWERC
Part III. The provider telephone survey
126
formal method was more likely to be reported by IDPs than by homes, some 86% compared
to 60%, respectively. A third formal method that was reported only by a small proportion of
organisations was the use of fee-charging employment agencies; 6% of homes reported this
practice, along with 16% of IDPs and 11% of LADPs.
In addition to the prompts we used in our telephone interviews, managers also told us about
other methods they regularly used. These included the internet, informal drop-ins, leaflet
drops, recruitment open days, UKHCA and the radio.
Certain recruitment methods appear to be more effective than others. Our survey data suggest
that informal word of mouth recommendations and the formal practice of press advertising
are the best ways to fill vacancies, although there is by no means a consensus, or even a
majority, view on this (table III.4). Among our small sample of LADPs, three quarters
favoured formal methods as most effective, with two thirds opting for press advertising. The
views of care homes and IDPs were more varied. Homes were far more likely than either
IDPs or LADPs to favour informal methods; the most common response to our survey
question (43% of homes) was that the informal word of mouth method is the most effective
way to fill vacancies. However, the relatively formal methods of press advertising and Job
Centre Plus were also identified as most effective by 28% and 19% of homes, respectively.
By contrast, IDPs (like LADPs) tended to identify formal practices as most effective; 38%
reported press advertising and 30% Job Centre Plus, compared with around 23% favouring
informal practices.
Table III.4. Managers’ views regarding the most effective method for filling vacancies
% of homes
% of IDPs
% of LADPs
% of all
42.6
23.4
0.0
30.1
4.3
0.0
11.1
2.9
2.1
0.0
0.0
1.0
4.3
8.5
11.1
6.8
Formal methods:
Press advertising
27.7
38.3
66.7
35.9
Jobcentre plus
19.1
29.8
11.1
23.3
Total responses
47
47
9
103
No response
6
5
1
12
Informal methods:
Word of mouth recommendations
Notice in office or shop window
Mixed methods:
Other agencies
Internet, open days, other methods*
Note: * Other methods include the internet, council workforce development and recruitment open days.
A small proportion of providers considered other mixed methods, in the sense of formal and
informal, to be the most effective way to fill vacancies. For example, 2% of homes and 8% of
IDPs believed the internet was the most effective method, while another 2% of homes
believed their local council‟s workforce development initiative was the most effective way.
One LADP reported that recruitment open days were the most effective practice.
EWERC
Part III. The provider telephone survey
127
The recruitment of senior care workers was considered an especially important issue among
managers of organisations responding to our survey. However, the filling of such posts is
unlike the filling of vacant care worker posts since it is more usually filled through internal
promotion, and therefore reflective of the organisation‟s approach to training and career
development for incumbent staff. As one manager told us, „I like to encourage people and
know that I have developed them. If you get someone new, they don‟t know the standards‟
(IL.H.4). In an effort to unpack these differences in approach our survey questionnaire
therefore asked respondents whether they normally recruited externally or from within their
existing staff of care workers.
In fact, the majority of establishments in our telephone interview sample recruited senior care
staff from within their existing staff (table III.5). This is a positive practice insofar as it gives
care workers something to aim for and the prospects of career progression. Only two
organisations out of the total sample of 115 relied wholly on external recruitment to fill
vacant senior care posts. It was far more common for care organisations to recruit from
internal applicants; 56% relied on this method exclusively. In addition, slightly more than one
in three organisations recruited from both internal and external routes. It is notable that 6% of
organisations surveyed did not employ senior care workers and therefore did not provide care
workers an internal opportunity for career progression.
Table III.5. Internal and external recruitment of senior care workers
Existing staff
% of homes
% of IDPs
% of LADPs
% of all
54.7
53.8
70.0
55.7
Externally
1.9
1.9
0.0
1.7
Both from existing staff &
externally
34.0
40.4
30.0
36.5
Don‟t have senior care workers
9.4
3.8
0.0
6.1
Total responses
53
52
10
115
The set of management processes used in recruitment was very standardised among the
different organisations. Nearly all managers who responded to the survey used application
forms requiring a full work history (99%), carried out formal interviews (96%) and relied on
formal job descriptions and person specifications (93%) (figure III.3). In addition, nearly all
organisations required character references – with 88% asking for references after the
interview and 18% prior to the interview.
Once again there is variation by type of care organisation. Around two in three IDPs used
initial telephone screening compared to only around one in three homes and one in ten
LADPs. Another difference concerns the requirement for applicants to produce a CV; this
applied to 61% of homes compared with only 39% of IDPs and 22% of LADPs. Finally, IDPs
and LADPs were twice as likely to use aptitude testing as care homes (43%, 44% and 22%,
respectively).
EWERC
Part III. The provider telephone survey
128
Figure III.3. Features of the recruitment process in homes and IDPs
100
Homes
90
IDPs
80
Percentage
70
60
50
40
30
20
10
0
Application
requires full
work history
Formal
interview
Job
References
descriptions
after
and person
interview
specifications
Initial
telephone
screening
CV
Aptitude
Testing
Informal
interview
Aptitude test References
at interview
before
interview
Aptitude test
at induction
Note: Total responses: 51 (homes), 51 (IDPs) and 9 (LADPs). Missing responses: 2 (homes), 1 (IDPs) and 1
(LADPs).
Table III.6. Alternative practices when local recruitment fails
% of homes
% of IDPs
% of LADPs
% of all
Extend efforts to surrounding areas
Attempt a more national recruitment drive
52.8
48.1
44.4
50.0
18.9
21.2
11.1
19.3
Use other agencies
20.8
11.5
11.1
15.8
Contact other agencies specifically for
migrant workers
13.2
19.2
0.0
14.9
Direct overseas recruitment
17.0
9.6
0.0
12.3
Total No.
53
52
9
114
No response
0
0
1
1
Given the pre-recession difficulties of recruitment, our survey included a question that asked
respondents about their strategies for filling vacancies if unable to recruit locally. Half the
sample reported they would extend efforts to surrounding areas under such circumstances
(table III.6). Use of other agencies was not a popular method, used by just 16%. The option
of contacting agencies, or intermediaries which specialise in providing migrant workers was
also not a very common practice, only reported by 19% of IDPs, 13% of care homes and
none of the LAPDs. However, a surprising 12% of organisations - all from the independent
EWERC
Part III. The provider telephone survey
129
sector - did in fact report recruiting care workers directly from overseas, including 17% of
care homes and nearly 10% of domiciliary care providers.
III.1.3. Selection: choosing the right applicant
While different recruitment methods enable organisations to access varying pools of job
applicants, it is likely that there will be variation in organisations‟ approach to what attributes
among job applicants provide the best fit with the job vacancy. Our survey asked respondents
to identify those attributes among job applicants they considered necessary or desirable. The
question included ten prompts and also allowed managers to identify other factors.
Perhaps unsurprisingly, given the intensive personal contact required in the job of a care
worker, close to nine in ten managers in our sample considered a positive attitude and a
friendly nature to be necessary of job applicants (figure III.4). A further two factors were also
very important necessary factors - availability for weekend work (70% of homes and 66% of
IDPs) and availability for early starts or evening work (66% of homes and 54% of IDPs) –
reflecting the 24/7 demands of work in the care sector. Indeed, all LADPs (not shown in
figure III.4) reported availability for both weekend work and for early starts and evening
work as necessary factors.
Figure III.4. Attributes considered necessary among job applicants
100
Homes
IDPs
90
80
Percentage
70
60
50
40
30
20
10
0
Positive attitude/
friendly
Available weekend
Available
work
earlies/evenings
Own transport
Ability to drive
Care-related skills
Lives locally
Experience caring
for family/friend
Qualifications
(NVQ2+) in care
Note: Total responses: 50 (homes), 50 (IDPs). Missing responses: 3 (homes), 2 (IDPs).
EWERC
Recommended by Formal care work
employee
experience
Part III. The provider telephone survey
130
Table III.7. Attributes considered necessary and desirable among job applicants
a. Homes
% of respondents
Necessary
Desirable
90.0
70.0
66.0
28.0
10.0
6.0
6.0
6.0
4.0
13.7
29.3
27.5
62.7
52.9
51.0
70.6
78.4
52.9
Total No.
50
51
No response
3
2
Necessary
Desirable
88.0
66.0
54.0
28.0
14.0
10.0
8.0
6.0
6.0
39.6
33.3
16.0
40.0
52.0
68.0
74.0
86.0
72.0
64.0
100.0
58.0
61.2
50
2
50
2
Positive attitude/ friendly nature
Availability for weekend work
Availability for early starts or evening work
Skills related to care work
Experience of caring for family member or friend
Recommended by another employee
Formal experience of care work*
Qualifications - NVQ2 or above in care
Lives locally
b. IDPs
Positive attitude/ friendly nature
Availability for weekend work
Availability for early starts or evening work
Lives locally
Skills related to care work
Qualifications - NVQ2 or above in care
Experience of caring for family member or friend
Recommended by another employee
Formal experience of care work*
Own transport
Ability to drive
Total No.
No response
c. LADPs
% of respondents
Necessary
Desirable
77.8
100.0
100.0
55.6
11.1
11.1
0.0
33.3
11.1
11.1
0.0
0.0
33.3
88.9
33.3
77.8
66.7
44.4
Total No.
9
9
No response
1
1
Positive attitude/ friendly nature
Availability for weekend work
Availability for early starts or evening work
Skills related to care work
Experience of caring for family member or friend
Recommended by another employee
Formal experience of care work*
Qualifications - NVQ2 or above in care
Lives locally
Note: *e.g. care home or other home or agency
By contrast, evidence of skills related to care work or qualifications in general care (at NVQ
EWERC
Part III. The provider telephone survey
131
level 2 or higher) were only considered necessary in a small fraction of the independent
sector organisations surveyed. Just one in four (24%) reported skills as necessary and one in
ten reported qualifications. Such factors were instead far more likely to be reported as
„desirable‟ rather than necessary, by two thirds or more of all organisations surveyed. The
results in table III.7 above demonstrate the majority of care organisations do recognise the
value of qualifications in care work, as well as formal or informal experience of care work
and care-related skills (all factors highlighted in italics in the table), but are unwilling to use
these factors to rule out candidates. The exception to this pattern are the public sector
providers. LADPs were far more likely to report care-related skills and qualifications as
necessary factors among job applicants – 56% and 33%, respectively, compared with 28%
and 6% of homes and 14% and 10% of IDPs. On the one hand, this may reflect the lack of an
available pool of ready-skilled job applicants, even during the recession. However, judging
by the comments made by several respondents, it also reflects a genuine prioritisation of
personality attributes over proven skills among public sector LADP managers.
Somebody may come with a string of qualifications but really not be suitable at all. Or,
conversely, zero qualifications but with a lifetime of experience of looking after people that
would be fine. (ON.DIH.1.DP).
Other factors cited as necessary by a small number of organisations were „lives locally‟ (in
fact more than one quarter of IDPs said this was necessary), „recommended by another
employee‟ and „formal experience of care work‟.
The four attributes highlighted in italics in table III.7 refer to skills, qualifications and
experience related to caring work. Across the different providers there was considerable
variation in the extent to which these four skill-related attributes were considered necessary
or desirable among job applicants. Figure III.5 presents the variation among homes and IDPs
using an indicator from 0-8 that assigns 2 points where the provider reported a skill-related
attribute as necessary and 1 point where it was reported only as desirable. Nearly half of both
homes and IDPs score 4 out of 8 on this measure. A surprisingly high share (16%) of IDPs
score 2 or less, meaning that they only reported two out of four skill-related attributes as
desirable or just one attribute as necessary; the same was true of 12% of homes. Only 2% of
homes and 2% of IDPs register the full score of 8, meaning they reported all four skill-related
attributes as necessary among job applicants. Among LADPs, the scores are higher; nearly
two thirds of LADPs score 5 or 6, 13% score 4 and 25% score 3.
EWERC
Part III. The provider telephone survey
132
Figure III.5. Measure of providers’ preferences for skill-related attributes among job
applicants
50%
homes
45%
IDPs
40%
35%
30%
25%
20%
15%
10%
5%
0%
0
1
2
3
4
5
6
7
8
Indicator of provider need for skills and qualifications among job applicants
Note: The four skill-related attributes are qualifications (NVQ level2 and above) in care, skills related to care
work, formal experience of care work and experience of caring for a family member or friend. See table III.7 for
details. 1 point is assigned to each attribute reported as desirable and 2 points to each necessary attribute.
Among all the different attributes that organisations value among job applicants, respondents
were also asked to identify the single most important factor. Unsurprisingly, perhaps,
respondents were most likely to select a positive attitude and friendly nature over any other
factor (table III.8). Two in three organisations cited this factor. All other factors accounted
for fewer than one in ten responses. Nevertheless, among LADPs one in four cited carerelated skills as the most important factor, compared with just 4% of IDPs and 6% of homes.
Interestingly only a handful of respondents considered availability for early starts or evening
work (8%) and availability for weekend work (4%) as the most important factor in applicants
when recruiting. This is somewhat paradoxical as we saw above that many managers reported
staff shortages for weekend work and evening work. Nevertheless, some comments by
managers did highlight this juggling of priorities:
I suppose if the positive attitude and friendly nature presents itself, they‟ve still got to have a
good availability. Just because somebody‟s really really friendly and really really nice, if
they‟ve only got the availability of 10am until 2pm Monday, Tuesday, Wednesday, we are not
going to take them on … So if they say, „Yes, I can start early three days a week because
that‟s all I want‟, and they‟re dead bubbly, then you are going to take them on. Because we
don‟t look for full-time workers. We are looking for people that work - 25 hours is a good
number for people to work. (ON.D.1 DN).
EWERC
Part III. The provider telephone survey
133
Table III.8. The most important attribute required of job applicants
% of homes
% of IDPs
% of LADPs
% of All
Positive attitude/friendly nature
76.6
56.5
62.5
66.3
Availability for early starts or evening
work
Skills related to care work
6.4
10.9
0.0
7.9
6.4
4.3
25.0
6.9
Availability for weekend work
0.0
8.7
0.0
4.0
Recommended by another employer
0.0
4.3
0.0
2.0
Formal experience of care work
2.1
2.2
0.0
2.0
Own transport
0.0
0.0
12.5
1.0
(Other) Reliability
0.0
8.7
0.0
4.0
(Other) Communication skills
4.3
0.0
0.0
2.0
(Other) Willingness to learn
2.1
0.0
0.0
1.0
(Other) Commitment
2.1
0.0
0.0
1.0
(Other) Honesty
0.0
2.2
0.0
1.0
(Other) Understanding
0.0
2.2
0.0
1.0
Total responses
47
46
8
101
No response
6
6
2
14
As well as looking for a particular mix of personal attributes – a friendly nature, a caring
attitude towards elderly people and a commitment to wok different hours – our survey was
also designed to identify whether or not managers also sought to compose a particular mix of
care workers, differentiated by gender, age, ethnicity and so on. One reason care
organisations may seek to do this is to reflect the demographic composition of their users;
male care workers may be in demand by elderly men in need of care and similarly there may
be a demand for care workers from particular ethnic backgrounds. We began by asking
managers if they were satisfied with the composition of their care workforce.
In relation to the numbers of young and old workers, male and female and ethnic mix, most
organisations responding to our survey– over 80% - reported that they were satisfied. The
degree of satisfaction was far higher among care homes – some 96% - compared to 74% of
IDPs and only 40% of the 10 LADPs. Of the 23 organisations that reported dissatisfaction,
we further queried the particular reasons for this (see table III.9). Ten organisations reported a
preference for a more ethnically diverse profile (which may include wanting more white
workers) and a similar number desired more male care workers. Three organisations stated
they wished to have more young workers. The difficulties of extending the recruitment pool
to these particular groups were articulated by some of the managers we interviewed:
I‟d like to see more men in this area of work, I feel frustrated at times that our staff don‟t get
the recognition that they deserve they are considered at the lower end of the scale in terms of
the working classes, … And I‟d like to see a better representation of minorities. Now that‟s
very difficult because of cultural differences and requirements which make it hard to recruit
and also for some of the minority cultures to work in this field. (OM.D.2.DN).
Ethnicity is an issue in terms of recruitment, there are a number of Chinese speaking and
Somali speakers; but this changes and we may lose staff with these languages. Sometimes we
EWERC
Part III. The provider telephone survey
134
can‟t match specific requests. I don‟t know how we have managed to cope because it can be
a problem. (IL.DIH.1.CP).
Men are thin on the ground. We have a lot of male service users who prefer a man to come in
to them. Having male staff limits you, as you can‟t send a male into a female service user.
(IL.D.3 CL).
Table III.9. Reasons for dissatisfaction with the composition of the workforce
% of homes
% of IDPs
% of LADPs
% of all
Happy with composition of
workforce
96.2
74.5
40.0
81.6
Not happy with composition
and would prefer:
More younger employees
3.8
25.5
60.0
18.4
0.0
7.7
28.5
13.0
More men
33.3
53.8
28.5
43.5
More ethnically diverse profile
66.7
38.5
42.9
43.5
Total responses
53
51
10
114
No response
0
1
0
1
III.1.4. Selection problems
In an effort to explore further the consequences of the recruitment and selection context, we
wanted to test the extent to which organisations were forced to hire people who perhaps did
not quite meet the selection criteria. Conversely, mindful of the effects of rising
unemployment during the period of our fieldwork, we also wanted to assess the degree to
which organisations felt they enjoyed the luxury of selecting from a pool of numerous
suitable candidates.
Our first finding concerns the extent to which organisations sometimes hired a person who
was known at the point of hiring to be less than the ideal match for the vacant job post. Quite
surprisingly, more than two in five care organisations in our sample (41%) reported they
occasionally, often or very often employed staff who did not possess as many of the desirable
qualities as they would like (table III.10). Open-ended responses to this question suggest that
organisations sometimes took on people without the desired experience, or without the
desired NVQ qualifications. Others employed the person on a temporary basis or used them
to cover staff on sick leave. The results suggest this was more of a serious problem for IDPs,
17% of which said this situation occurred „often‟. It is possible that the varying responses
relate to labour market conditions, such that those providers experiencing recruitment
difficulties (as reported in Figure III.1) would conceivably be more likely to make a less than
ideal hire. However, interrogation of the data suggest there is not a strong relationship,
neither for homes nor IDPs; those facing difficult recruitment conditions were as likely to
report occasionally or often hiring people without the desirable skills as to never or almost
never hiring such people. Only among homes that reported easy recruitment of care workers
do we find some evidence of an influence, with twice as many saying they never or almost
EWERC
Part III. The provider telephone survey
135
never hired individuals without the desirable skills. Another factor that might help explain the
variation in hiring practices is the provider‟s preference for skills and experience among job
applicants (as reported in Figure III.5 above). Again, there is little evidence of a strong
relationship. And once again only among homes do we find that for those with a medium to
strong preference for skill-related attributes (a score of 4 of more on the 1-8 scale), the
likelihood of never or almost never hiring individuals without the desired skills is twice that
of occasionally or often hiring such individuals.
Table III.10. Percentage of organisations that knowingly hire people who lack the full
set of desirable qualities
% of homes
% of IDPs
% of LADPs
% of all
Very often
Often
1.9
0.0
0.0
0.9
3.8
17.3
0.0
9.6
Occasionally
34.0
32.7
0.0
30.4
Almost never
34.0
15.4
40.0
26.1
Never
26.4
34.6
60.0
33.0
53
52
10
115
Total responses
In contrast a significant minority of organisations did not face problems in attracting
sufficient numbers of suitable care workers and in fact often had to turn away people who
were suitable for the job. Approximately one in three care organisations reported that they
occasionally, often or very often were in the position of having to reject applicants who
would nevertheless be acceptable care workers (table III.11). For one in ten organisations this
occurrence happened often or very often, especially among independent sector and LA
organisations providing domiciliary care. To some extent this finding is likely to reflect the
impact of the recession with an increasing number of people seeking jobs. Nevertheless, the
majority of organisations reported that this happened never or almost never. This finding
suggests that most organisations simply do not experience the luxury of selecting from
several candidates who are all suitable for the job post. At the same time, however, some
organisations may be able to find alternative means of fitting such candidates into the
organisation, as the following quote illustrates:
If we thought we had found somebody good then we would always look at our other care
company because I think if we felt that we had found a genuinely suitable person then we
wouldn‟t want to lose them. (UY.D.2.B.S).
All organisations delivering care to the elderly must apply for Criminal Records Bureau
(CRB) checks on selected job candidates in order to ensure those individuals are eligible to
work with vulnerable adults.23 We investigated two recruitment issues associated with CRB
23
The administrative success of CRB checks has been subject to criticism over recent years. The system was
renovated and relaunched with a new IT system under a contract with the IT firm Capita in 2002, but was
subsequently plagued by problems which led to the delayed opening of schools and unfilled vacancies in many
care organisations.
EWERC
Part III. The provider telephone survey
136
checks – whether or not organisations had not recruited applicants because of delays in the
CRB checks and whether or not applicants had failed CRB checks. In both cases, we were
interested in identifying the extent to which these problems caused organisations to lose
potential recruits over a two-year period.
Table III.11. Percentage of organisations that reject suitable applicants for care work
% of homes
% of IDPs
% of LADPs
% of all
Very often
Often
0.0
1.9
0.0
0.9
5.7
13.5
20.0
10.4
Occasionally
30.2
7.7
50.0
21.7
Almost never
35.8
34.6
20.0
33.9
Never
28.3
42.3
10.0
33.0
53
52
10
115
Total responses
In fact, a majority of organisations, 55% of the 115 surveyed, had experience of not recruiting
qualified job applicants due to delays in their CRB checks in the previous two years. A
smaller share, 36%, had a similarly negative experience as a result of an outright failure of
CRB checks (table III.12a and b). With respect to CRB delays, a far higher share of IDPs
reported problems than homes. Indeed, 28% of IDPs failed to recruit between 11 and 30
individuals in the previous two years as a direct result of CRB delays, and in 2% of IDPs
more than 30 individuals are said to have been lost. A similar pattern is true of reported
problems arising from CRB failures with around half of IDPs experiencing a loss of potential
recruits compared to only 21% of homes.
Many of our respondents took the opportunity as part of the telephone survey to voice
criticism over the administrative process of submitting CRB checks. The following quotes are
illustrative:
This is one of the bones of contention with me. It is a little bit better now. It used to take up to
4 months last year … We consequently lost staff. Now it is a little better and we can get them
in 3 weeks. Others take 8 to 10 weeks. This is just unacceptable. When it comes in they have
found another job outside care. (LK.D.6.CL).
We have a lot apply but they want to start work straight away. As we have a 7-week wait for
CRB we lose people. (HD.D.1).
We have to wait two months and people take other jobs. It is a real problem here. So we now
ask them [job applicants] to foot the bill for the CRB. (AH.D.1.BL).
EWERC
Part III. The provider telephone survey
137
Table III.12. Recruitment failures caused by problems with CRB checks
a. Number of people not recruited in previous 2 years due to CRB delays
% of homes
% of IDPs
% of LADPs
% of all
64.0
28.0
6.0
2.0
0.0
23.3
30.2
16.3
27.9
2.3
50.0
50.0
0.0
0.0
0.0
45.5
30.3
10.1
13.1
1.0
Total responses
50
43
6
99
No response
3
9
4
16
0
1-5
6-10
11-30
Over 30
b. Number of people not recruited in previous 2 years due to CRB failures
% of homes
% of IDPs
% of LADPs
% of all
0
78.8
48.9
50.0
63.8
1-5
19.2
27.7
50.0
24.8
6-10
1.9
12.8
0.0
6.7
11-30
0.0
8.5
0.0
3.8
Over 30
0.0
2.1
0.0
1.0
Total responses
52
47
6
105
No response
1
5
4
10
EWERC
Part III. The provider telephone survey
138
III.2. Turnover and retention
The care sector faces considerable challenges in managing staff turnover and retention.
Estimates for England for 2010 suggest turnover rates as high as 22% for all care workers.
Across the different provider types turnover rates of 24% are recorded in the domiciliary care
sector and among homes with nursing provision and 21% in homes without nursing provision
(NMDS 2010). Such high rates are problematic. Organisations may be forced to deliver care
services without the adequate quota of staff. They will have to commit time and money to
what may feel like a continuous process of managing recruitment and selection. And high
staff turnover clearly limits the ability of managers to cement together an environment where
experience, loyalty and careers add up to a committed staff. In this section, we map the
patterns of staff turnover and staff retention for IDPs, homes and LADPs.
III.2.1. Staff turnover
Evidence from a range of datasets and studies of the care sector suggests there is an acute
problem with staff turnover. In our survey of care providers we sought to provide alternative
measures of turnover, utilising both self-reported, subjective measures, as well as staffing
data on quits and retention among new starters and all care workers.
Figure III.7. Managers’ subjective views about the level of staff turnover
50
45
Homes
IDPs
LADPs
40
Percentage
35
30
25
20
15
10
5
0
very high
quite high
about
right/acceptable
quite low
very low
Note: Total responses: 52 (homes), 52 (IDPs) and 10 (LADPs). Missing responses: 1 (homes).
Figure III.7 presents managers‟ assessments of the level of turnover among their care
workers, disaggregated by type of care organisation. Four in five providers (79%) were
satisfied that the level of staff turnover was acceptable or low. This was especially true of
LADPs, none of which reported high turnover among care workers, and to a lesser extent
among homes, among which just 15% reported high turnover. IDPs were most likely to report
EWERC
Part III. The provider telephone survey
139
high staff turnover – some 31% - and IDPs were the only type of organisation to report „very
high‟ staff turnover. Some of the open-ended answers to our survey provide a glimpse into
the different causes of staff turnover among these IDPs.
We have quite a high turnover. We have some staff who have been with us for 10 years but
some go to a career in nursing. Some are new to the work and they may leave. We had quite a
high level of turnover when the LA contract moved from block to spot last year. It meant that
the work patterns changed and the work became less secure. … Otherwise it is because of the
work times and the low pay. (IL.D.2.DL).
There are obvious problems in comparing subjective opinions about staff turnover; what is
high for one manager may be interpreted as low for another, for example. Hence, we also
collected staffing figures and present below alternative quantitative estimates of turnover
among care workers. The first refers to the ability of the organisation to retain new starters
hired in the previous 12 months. Figure III.8 presents the percentage share of homes, IDPs
and LADPs that registered different levels of retention of new starters. The total number of
responses to this particular survey question is considerably below the full sample of 115,
reflecting the difficulties in providing accurate information on staffing; the data refer to 45
homes, 37 IDPs and 5 LADPs.
Figure III.8. Percentage retention of recruits hired in the previous 12 months
60
Homes
IDPs
Percentage of providers
50
40
30
20
10
0
100%
90-99%
80-89%
70-79%
60-69%
50-59%
40-49%
30-39%
20-29%
Percentage retention of new recruits
Note: Total responses: 45 (homes), 37 (IDPs). Missing responses: 8 (homes), 15 (IDPs). The measure of
retention of new recruits was calculated as the number of new recruits retained divided by the number of recruits
hired in past 12 months.
The key finding is that homes are far more successful at retaining new starters than are IDPs;
nearly 60% of care homes managed to retain all new starters over the previous 12 months
compared to just 22% of IDPs. Nevertheless, a significant proportion of both homes and IDPs
EWERC
Part III. The provider telephone survey
140
reported a failure to retain more than half of new recruits – 22% of homes and 32% of IDPs.
The evidence from LADPs is that new staff retention rates are much higher, although our
evidence is only from 5 respondents.24
Our second quantitative measure estimates the level of staff turnover among care workers
excluding new recruits. Average turnover rates of 18% were recorded for homes, 22% for
IDPs and only 10% for LADPs. Overall 86% of LADPs, 62% of homes and 53% of IDPs had
turnover rates below 20%. At the other end of the scale, a significant minority of IDPs (nearly
one in three providers, 31%) experienced staff turnover in excess of 30%, far higher than the
13% of homes; no LADPs registered such high levels of staff turnover.
Figure III.9. Level of turnover of care workers excluding new recruits
40
Homes
IDPs
Percentage of Providers
35
30
25
20
15
10
5
0
0%
1-9%
10-19%
20-29%
30-39%
40-49%
50-59%
60%
Percentage staff turnover
Note: Total responses: 45 (homes), 36 (IDPs). Missing responses: 8 (homes), 16 (IDPs). The measure of staff
turnover is estimated as the number of care workers who quit in the past 12 months (excluding those recruited in
the past 12months) divided by the care workforce in post twelve months earlier (calculated as the current total
number of care workers minus any new starters still in post plus the number of care workers who quit
(excluding quits by new recruits)).
Our third measure estimates overall total staff turnover by including both the number of new
starter quits and other staff quits in the calculation. The results are reported in figure III.10.
These results show even stronger variation by type of provider with average turnover rates
reaching 31% and 24% in homes and 11% in LADPs. Three fifths of homes (60%) had staff
turnover below 20%, compared to only half of IDPs (51%). All LADPs reported turnover less
than 30% (albeit applicable to a sample of just 7). At the other end, 30% of IDPs reported
very high staff turnover among care workers of 50% or more; the comparable share of homes
is just 13%.
24
Only eight of the ten LAs in the survey had undertaken recruitment in the previous 12 months. Of these eight
we have data for five LADPs. The evidence suggests two of the five LADPs experienced 100% staff retention
and three of the five reported 80-89% retention.
EWERC
Part III. The provider telephone survey
141
Figure III.10. Percentage staff turnover of all care workers
40
Homes
IDPs
35
30
Percentage
25
20
15
10
5
0
0%
1-9%
10-19%
20-29%
30-39%
40-49%
50-59%
60-69%
70-79%
80-89%
90%+
Note: Total responses: 45 (homes), 37 (IDPs). Missing responses: 8 (homes), 15 (IDPs). Measure of total care
workforce turnover in the last 12 months defined as (number of new starters in last 12 months minus number
retained plus number of other staff who left) divided by current number of care workers.
There are many reasons explaining turnover among care workers. Among all care providers,
the most common reason, reported by around one third of organisations surveyed (35%), was
family responsibilities (table III.13). Some managers suggested family issues were a
particular problem given the highly feminised nature of the occupation (OM.HN.2).
However, this reason also interacted with several „push factors‟ related to the working
environment and HR policies of the organisation, particularly the desire for more convenient
working time, which registered as the most important factor among IDPs (33%). In openended answers, managers talked about the difficulties care workers faced working weekends
and long hours while raising young children; for example, at one provider (TE.HI.DL) each
shift was 11 hours long and care workers were required to work alternate weekends. As such,
staff quits to look for a job with more convenient working time was for many workers both a
reflection of inconvenient working hours and family responsibilities.
Leaving for improved job prospects was a relatively common reason. The push factor, „better
pay‟, was cited by 25% of homes and 21% of IDPs (and notably no LADPs), and entering
nurse training was reported by 26% of homes and 14% of IDPs. Also, many care workers
were said to leave to work in another care organisation, for the NHS, local authority or
another sector altogether. Finally, as might be expected, some reasons related to other push
factors, such as dissatisfaction with the manager or other colleagues and lack of support in the
job.
EWERC
Part III. The provider telephone survey
142
Table III.13. Push factors and other reasons for the turnover of care workers
Push factors:
More convenient working times
Better Pay
Unhappy with manager/office
staff/team
Lack of support /no promotion
Other factors:
Family responsibilities
Nurse training
Relocation
Work for the NHS
Work for another care provider
Full-time education
Not suitable – dismissal
To work in a different sector
Car/petrol/travel issues
Health problems
To work for the Local Authority
Job too hard
Don‟t want to/ like to train
Other ambiguous
Total responses
% of homes
% of IDPs
% of LADPs
% of all
15.1
24.5
11.3
3.7
32.7
21.2
1.9
3.9
10.0
0.0
0.0
0.0
22.6
20.9
6.1
3.5
37.8
26.4
26.4
18.8
7.5
13.2
7.5
5.7
3.7
3.7
0.0
1.9
3.7
5.7
30.8
13.5
7.7
11.5
19.2
15.4
15.4
11.5
9.6
3.9
5.8
1.9
0.0
13.5
40.0
10.0
0.0
10.0
10.0
0.0
0.0
20.0
0.0
10.0
10.0
0.0
0.0
20.0
34.8
19.1
15.7
14.8
13.0
13.0
10.4
9.6
6.1
4.3
3.5
1.7
1.7
10.4
53
52
10
115
Note: Question allows multiple answers by each respondent.
EWERC
Part III. The provider telephone survey
143
III.3. Pay and rewards
III.3.1. Level of pay
One of the key issues in the recruitment and retention of the social care workforce is the rate
of pay for the job. For each provider we have identified the minimum, or starting rate of pay
for care workers, and also a „normal‟ rate of pay, which refers to the modal rate of pay in the
organisation for care workers. For example, where most workers were qualified to NVQ level
2 we took the rate paid to this group, but where only a minority were qualified we took the
rate paid to the non-qualified. In some cases where a range was given, we have taken the
mid-point for the normal rate of pay25.
When we look at the distributions of both minimum and normal hourly pay rates for care
workers it is clear that there are two significant dividing lines in the data. The first is the
divide between wages paid by LAs and the wages paid by the independent sector, whether
domiciliary providers or care homes. The average minimum pay across the sample of LADPs
is £8.54 compared to means of £6.40 for IDPs and £6.05 for homes. Similar variation can be
seen with respect to the median level of minimum pay offered: £7.90 in LADPs, £6.35 in
IDPs and only marginally above the national minimum wage at £5.81 in homes. The second
dividing line lies within the independent sector between the voluntary, not-for-profit homes
and the for-profit homes. For example, median pay in voluntary sector homes is £7.55,
significantly higher than the £5.75 median pay paid by for-profit homes. The pay gap is in
part due to the differential proportion of users who are local authority funded since homes
can charge their private clients higher rates and thereby fund higher pay. Our data reveal that
61% of users are LA funded in private homes but only 49% on average in voluntary sector
homes. By way of an economy-wide benchmark for pay, it is notable that the median level of
pay for all female part-time employees in the whole economy was £7.86 in 2009 at the time
of data collection.
Figure III.11 displays the range of minimum pay rates for care workers with box plots that
depict the inter-decile (top and bottom points), inter-quartile (top and bottom of box) and
median pay points (thick horizontal line). It is clear that minimum rates of pay are
significantly higher in LADPs; the range of pay is not presented due to the small sample size.
By contrast, within the for-profit independent sector there is a very high concentration of
minimum pay rates at just above the national statutory minimum wage in both homes and
IDPs. In the not-for-profit voluntary sector, IDPs display a narrow range of minimum pay
rates but homes pay a wider range of rates at a higher level – significantly higher than the
independent for-profit homes. Table III.14 presents the precise share of providers that pay a
25
Where pay data was collected after the upgrading of the national minimum wage in October 2009 we have
deducted the increase of 7 pence from all wage rates. Obviously this is only a rough and ready adjustment to
ensure comparability across time periods as not all rates will have been adjusted upwards. However, this is a
relatively low adjustment and the data would provide a similar picture of relatively low pay, with or without the
7p adjustment.
EWERC
Part III. The provider telephone survey
144
minimum rate of just £6.00 or less. („low‟ or „very low‟). This accounts for 53 organisations almost half of the 111 independent providers that provided the necessary pay data. Moreover,
22% of all independent providers (for-profit and not-for-profit) set their minimum rate at the
level of the national statutory minimum wage (4% of IDPs and 38% of homes).
If we look at „normal‟ pay rates we find an even larger gap between LADPs and the
independent sector with mean normal pay of £9.16 in LADPs and means of £6.65 in IDPs
and £6.31 in homes. Differences in median pay are similarly varied at £8.61 (LADPs), £6.51
(IDPs) and £6.08 (homes). Figure III.12 presents box plots of the pay distributions in a
similar fashion to the previous figure. Again, we see a strong compression of normal pay
rates in the independent sector, particularly among for-profit homes and voluntary IDPs.
Nevertheless, there is a clear differentiation between for-profit and voluntary independent
organisations; median pay is higher in voluntary organisations than for-profit organisations,
whether homes or IDPs. Overall, however, the wage distributions in all parts of the
independent sector are at such a low relative level that there are no overlaps between the
upper decile pay level and the median level of pay in the public sector LADPs. This is also
true of minimum pay rates. Compared to the setting of minimum pay rates, fewer
independent sector organisations paid a „normal‟ rate of pay at the national minimum wage –
9 homes (a 17% share) and no IDPs. But the share of both IDPs and homes paying £6.00 or
less as the normal rate of pay for care work was still substantial at 23 homes (44%) and 10
IDPs (20%) (table III.15).
EWERC
Part III. The provider telephone survey
145
Figure III.11. The range of minimum pay rates for care workers in private and
voluntary sector homes, and private, voluntary and public sector domiciliary care
providers
Notes: The box plots represent the following points of the pay distribution: lowest point (D10), bottom of box
(D25), thick line (D50), top of box (D75), upper point (D90). Only the median pay level is presented for LADPs
because of the small sample size. See table III.14 for sample sizes.
Table III.14. Variation in minimum pay rates
Public
Private for-profit
% of
LADPs
0
% of
IDPs
4.5
% of
Homes
46.3
% of
IDPs
0
% of
Homes
9.1
% of
all
19.8
0
27.3
39.0
33.3
9.1
27.9
Medium (£6.01-£6.90)
11.1
47.7
14.6
66.7
45.5
33.3
High (£6.91-£7.90)
44.4
18.2
0
0
27.3
13.5
Very high (£7.91- £10.90)
44.4
2.3
0
0
9.1
5.4
9
1
44
2
41
1
6
0
11
0
111
4
Very low (£5.73)
Low (£5.74-£6.00)
Total responses
No response
EWERC
Voluntary
Part III. The provider telephone survey
146
Figure III.12. The range of normal pay rates for care workers in private and voluntary
sector homes, and private, voluntary and public sector domiciliary care providers
Notes: The box plots represent the following points of the pay distribution: lowest point (D10), bottom of box
(D25), thick line (D50), top of box (D75), upper point (D90). Only the median pay level is presented for LADPs
because of the small sample size. See table III.17 for sample sizes.
Table III.15. Variation in normal pay rates
Public
Private for-profit
% of
LADPs
0.0
% of
IDPs
0.0
% of
Homes
19.5
% of
IDPs
0.0
% of
Homes
9.1
% of
all
8.1
Low (£5.74-£6.00)
0.0
20.5
34.1
16.7
0.0
21.6
Medium (£6.01-£6.90)
0.0
47.7
39.0
83.3
36.4
41.4
High (£6.91-£7.90)
11.1
25.0
4.9
0.0
36.4
16.2
Very high (£7.91- £10.90)
88.9
6.8
2.4
0.0
18.2
12.6
9
1
44
2
41
1
6
0
11
0
111
4
Very low (£5.73)
Total responses
No response
EWERC
Voluntary
Part III. The provider telephone survey
147
III.3.2. Pay differentials and pay supplements
The care sector appears not only to be characterised by low pay but also by very limited
opportunities for pay progression. This is particularly so among IDPs where 52% paid the
same rate as minimum and normal pay for care workers. In homes the tendency to pay rather
lower minimum rates than in domiciliary care has led, perhaps, to more common provision of
some pay increase between minimum and normal pay, with only 34% not offering any
upgrade. The mean values of the pay differential were only 26 pence in homes and 24 pence
in domiciliary care including those offering no increments. Of those offering some
increments the mean value was 40 pence in homes and 50 pence in domiciliary care. Only 2
homes and 4 IDPs offered increments of £1 or more. The opportunities to progress beyond
„normal pay‟ were usually very limited; in most cases these were limited to opportunities for
promotion to senior care worker or team leader.
We have information on maximum pay levels for senior care workers in 43 cases (15 IDPs,
28 homes). The information suggests there are very wide variations in the increments offered
for seniors. For IDPs and homes the majority paid an extra £1.00 or less (7 IDPs, 20 homes).
Of these, over half (3 IDPs and 10 homes) were paying below 50p, with the lowest rates
being 25p extra per hour. Those offering the very lowest rates for seniors tended to be low
payers for all staff – in 17 of these cases, the normal rate was £6 50 and below, and six of the
eleven were paying the national minimum wage as the normal rate – all of these were homes.
The three IDPs that paid seniors less than 50p extra all paid over £6 50 as the normal rate.
Some of the managers commented on how low the pay enhancements for senior grade staff
actually were:
The amount of workload and responsibility they have on them is a lot.... For a minute amount
of money for the amount of responsibility, it‟s just not worth it. (IL H4 BS).
In fact, as shown in table III.16, fewer than half of the respondents in either homes or IDPs
said that they rewarded experience/length of service with extra pay (38% of homes and 42%
of IDPs). Most of these variations by experience/length of service are limited as has already
been found in the small gaps between minimum rates and normal pay levels. Even fewer (8%
of homes and 4% of IDPs) claimed to have variations in pay based on incremental scales. The
most common factors associated with variations in pay rates were qualifications (over 60% of
homes, and 67% of IDPs) and, for IDPs, weekend work (73% compared to 28% of homes).
Again, these variations tend to be limited with many of the increments for qualifications at
least up to NVQ level 2 more in the range of pence. Of the 25 which specified rates, the
increments ranged from 7 pence to £1.02 per hour above the minimum pay rate; 23 out of the
25 paid under 50p extra, and over half of these paid less than 25p. Even for NVQ level 3,
where rates were specified, some of the increments above minimum pay rates were in the
range of pence. Of five IDPs, two paid 30p or less, and three paid above £1; of six homes five
paid 90p or less and the sixth paid £1.27 above the minimum rate.
EWERC
Part III. The provider telephone survey
148
Table III.16. Main reasons for differences in pay rates for care workers
% of homes
% of IDPs
% of LADPs
% of all
Experience/length of service
37.7
42.3
33.3
39.5
Incremental pay scales
7.5
3.8
40.0
8.7
Qualifications
60.4
67.3
44.4
62.3
Weekend work
28.3
73.1
55.6
50.9
Night work
24.5
32.7
88.9
33.3
Total responses
53
52
9
114
No response
0
0
1
1
Note: Multiple responses possible.
Only one quarter of home managers (25%) cited night work as a source of pay variations
even though all will operate night shifts on a regular basis. A third of IDPs (33%) cited night
work even though not all were engaged in night work, and this suggests that where night
work is undertaken by IDPs a supplement is paid. Some of the providers gave us examples of
supplements for weekend work or night work, but most were a matter of pence. Home
managers also paid less than IDPs for night work. Home rates varied from 20p to £1.60,
while IDP rates varied from 70p to £2.02. The higher rates paid by IDPs may reflect the
unpopularity of being out late in the evening in the community. Where IDP rates were given,
they were commonly for work up until 10pm, although in one case it was for work up until
midnight26.
For weekends, the majority of rates ranged from 8p to £1.45 extra, excluding three outliers
which paid a percentage of the hourly rate for weekend work – in two cases, this was 100%
and resulted in extra pay of over £6 50 per hour. A few organisations (12 IDPs and 1 home)
offered the additional information that they paid higher rates for Bank Holidays. Although
this is likely to undercount the number making such payments, it was notable that amongst
this group not all Bank Holidays were paid for: in one case only Christmas counted, another
only Christmas, Boxing Day and New Year‟s Day27. Among the „other factors‟ associated
with pay differentials cited by providers, the most common were senior or team leader roles,
particularly among homes (30) but also IDPs (13). As we saw in Section III.1.2 (see table
III.5), an overwhelming majority of providers recruited seniors from existing staff or from a
combination of externals and existing staff (only one home and one IDP stated that they
solely recruited seniors externally). These additional payments for seniors thus provided
internal care staff with some limited prospects of pay promotion through upgrading.
A much less commonly cited factor influencing pay was the needs of the client, mentioned
only by 8% of IDPs. Rising dependency levels are increasing the complexity of work but so
26
No information was given on rates for those IDPs offering 24 hour service.
Only three organisations cited the premia paid: in two of the cases double time was paid, in another the rate
was £1.51 above the minimum pay.
27
EWERC
Part III. The provider telephone survey
149
far this is not reflected frequently in pay levels. Indeed only a minority of the IDPs (26%) and
LADPs (38%) that undertook intermediate care/hospital discharge work paid a different rate
for this type of work (table III.17). These findings suggest that pay does not vary in line with
variations in skills required in the actual work tasks, although it should be noted that some
LADPs specialise in this type of work, and these results for the LADPs need to be considered
in conjunction with the generally higher pay rates in local authorities.
Table III.17. Payment of different rates for those providing intermediate care (where
applicable)
% of IDPs
% of LADPs
% of all
Yes
25.9
37.5
28.6
No
74.1
62.5
71.4
Total responses
27
8
35
No response/not applicable
25
2
27
The majority of IDPs did not make a distinction in pay rates between care work and domestic
work but 14% did pay a lower rate for domestic work along with half the LADPs (table
III.18). All those providers paying lower rates to domestic staff were paying a minimum rate
to care staff that exceeded the national minimum wage.
Table III.18. Payment of different rates for personal and domestic work
% of IDPs
% of LADPs
% of all
Yes
13.7
50.0
80.3
No
86.3
50.0
19.7
Total responses
51
10
61
No response/not applicable
1
0
1
EWERC
Part III. The provider telephone survey
150
III.3.3. Pay uprating
Regular uprating of pay was common but not universal. All LADPs had a regular uprating of
pay but 8% of homes and one fifth of IDPs did not have a regular uprating of pay (table
III.19). Failure to increase pay could be a serious source of dissatisfaction which could
impact upon staff retention, as the following quote illustrates:
Well, they [care workers] didn‟t get a pay rise for two years so they weren‟t very happy and a
lot threatened to leave so they [managers] had to take notice. (RN.D.2.CN).
Table III.19. Provision of a regular uprating of pay
% of homes
% of IDPs
% of LADPs
% of all
Yes
92.5
80.0
100.0
87.4
No
7.5
20.0
0.0
12.6
Total responses
53
50
8
111
No response
0
2
2
4
There were some marked differences between homes and IDPs in what triggered an uprating
(figure III.13). The impact of LA fee levels was more important for IDPs with nearly half
(43%) citing this as the most important factor compared to less than one in ten (8%) homes.
In contrast changes in the statutory National Minimum Wage were more important for homes
(52% citing this compared to 20% of IDPs). These findings reflect the higher share of homes
using the National Minimum Wage as a minimum pay rate and the lower influence of LAs on
total income for homes. Profitability was another important factor in uprating but more so for
IDPs than for homes (33% compared to 19%). Performance factors also acted as a trigger in a
significant minority (15% of homes and 14% of IDPs).
Of those homes citing changes to the National Minimum Wage as a main factor influencing
pay uprating, 85% paid under £6.00 and 65% paid the national minimum wage (figure III.14)
compared to 39% for the sample of homes as a whole (see Table III.14 above). In contrast of
those IDPs who cited the National Minimum Wage as a main factor, only 40% had a
minimum rate below £6.00 and only 20% had the National Minimum Wage as their lowest
rate (but this was a higher share than the 4% for the IDP sample as a whole).
EWERC
Part III. The provider telephone survey
151
Figure III.13. Main factors influencing pay uprating in homes and IDPs
60
Homes
IDPs
Percentage of providers
50
40
30
20
10
0
Change in NMW
Completion of
qualifications
LA fee levels
Profitability
Performance
Related
Employee
Request
Note: Total responses: 52 (homes), 51 (IDPs). Missing responses: 1 (homes), 1 (IDPs). Multiple responses
possible.
Figure III.14. Minimum pay rates in homes and IDPs that cited change in the National
Minimum Wage as a main factor in pay uprating
70
Homes
IDPs
Percentage of providers
60
50
40
30
20
10
0
£5.73
£5.74 - £5.99
£6.00 or over
Note: Total responses: 26 (homes), 10 (IDPs). Question only applies to those providers that cited change in the
National Minimum Wage as a main factor in pay upgrading (see figure III.13).
EWERC
Part III. The provider telephone survey
152
III.3.4. Payment for travel time, overtime and training time
Payment for all time spent at work or on work related activities is clearly an important aspect
of working conditions, as is receiving additional premia for working extra hours. The extent
to which the conditions apply to the care staff in our sampled organisations is explored here.
One of the key issues for domiciliary care workers is how travel time between clients is
compensated. The actual time spent travelling may be paid for by travel time being included
in work time or by staff being expected to complete tasks in under the allotted time to allow
themselves time to reach the next client. The variety of practices was indicated by some of
the additional responses to the question on travel costs. One provider paid a flat rate:
We pay 15p per call, whether workers travel by foot, bus, or car, it is the same. (IL.D.3.BN).
Another provider clearly includes a variable element into the work schedule according to
estimated and actual travel times between service users:
We look at the run, and we allow 7 minutes, 10, 15 minutes etc., So it‟s all factored into the
run, so they are paid for the complete time. We pay travel expenses based on the mileage of
the run. (TE.D.1 CN (V)).
Others regard it as a relatively trivial issue due to proximity of services users:
The travel is included in the hourly wage. Because we‟re quite unique here ….because ninety
nine percent of the carers walk. The service users are very close to the office. (RN.D.2.CN).
Travel time for some people – not for foot or bike - if people go out of their normal area to
work we pay for that travel time. We only pay travel costs if they are doing something that the
client needs – for example, taking them to hospital or going shopping for them. If it‟s travel
between jobs, we don‟t pay, but we help with the tax claims. (LK.D.3.DS).
Yet another provider pointed to the problem of comparing rates of pay across IDPs as some
pay a lower rate but pay for actual travel costs and travel time while others pay a higher basic
rate but no compensation for travel time:
Also what our competitors tend to do is to include their mileage cost rates within their basic
rates, which make them look higher when in actual fact they‟re not. (OM.D.2.DN).
With these problems of interpretation in mind, the responses to the question on travel time
suggest that only 20% of IDPs paid any kind of supplement whether flat rate, percentage or in
one case a higher rate for a shorter visits. A higher share, 54%, paid a mileage allowance, or
reimbursed petrol or public transport costs (figure III.15). Those not reimbursing out of
pocket expenses may include those IDPs that rely on „walkers‟. Nevertheless, several said
explicitly that they did not pay petrol or mileage but instead would volunteer to help staff
claim the tax back on their tax returns. Furthermore, 38% of IDPs and 30% of LADPs said
the compensation was included in the hourly rates. However, while in LADPs work time is
organised in continuous shifts without unpaid breaks so that time spent travelling is paid for,
EWERC
Part III. The provider telephone survey
153
IDPs tended to pay just for the scheduled visit time. If travel was undertaken outside these
times it was unlikely to be paid for.
Figure III.15. Payment for travel among IDPs and LADPs
100
IDPs
LADPs
90
Percentage of providers
80
70
60
50
40
30
20
10
0
Supplement (flat
rate/%/higher rate for
short calls)
Reimbursement
(mileage/petrol/public
transport costs)
Included in hourly rate
Note: Total responses: 50 (IDPs), 9 (LADPs). Missing responses: 2 (IDPs) and 1 (LADPs). Multple responses
possible.
Table III.20. Compensation for time spent training
a. Payment for time spent training
% of homes
% of IDPs
% of LADPs
% of all
Yes
88.7
84.6
100.0
87.8
Not all courses
9.4
5.8
0.0
7.0
No
1.9
9.6
0.0
5.2
Total responses
53
52
10
115
% of homes
% of IDPs
% of LADPs
% of all
Yes
77.4
86.5
70.0
80.9
Sometimes
18.9
7.7
30.0
14.8
No
3.8
5.8
0.0
4.3
Total responses
53
52
10
115
b. Time off to attend training
EWERC
Part III. The provider telephone survey
154
Another call on staff time that is related to work but which is not direct caring work is time
spent training. The majority of providers said that staff were paid for training time - all
LADPs paid, as did 85% of IDPs and 89% of homes. Even those that did not pay all the time
may pay some of the time, but 2% of homes and 10% of IDPs said they did not pay for
training (table III.20a). An even higher share of IDPs – as we see in table III.22b below - did
not pay for induction training. When it comes to time off from care duties to attend training
rather than attending in their own time, the pattern was somewhat different with more homes
not always providing time off – nearly one in five (19%) only did so some of the time and 4%
none of the time compared to 8% and 6%, respectively, of IDPs. Around a third of LADPs
also did not always provide time off (table III.20b).
Only a minority of independent providers (26% of homes and 29% of IDPs) ever pay
overtime premia to staff compared to more than two thirds (70%) of LADPs (figure III.16).
Moreover, when this minority were asked whether this applied to all staff, or only those
contracted to work a certain number of hours per week, one out of the 15 IDPs paying a
premium said it was discretionary, one paid it only to TUPE transferred staff, and one only
paid when staff were required to work „out of area‟. Five LADPs referred to overtime premia
that only applied above a certain number of hours – one for over 36 hours, three for over 37
hours and one for over 148 hours in a four week period. Among the 14 home managers who
mentioned overtime premia for extra hours, three said they only applied over full-time hours,
for example, over 37 hours per week.
Figure III.16. Payment of overtime premia to staff working extra hours
80
Homes
IDPs
LADPs
Percentage of providers
70
60
50
40
30
20
10
0
Yes
No
Note: Total responses: 53 (homes), 51 (IDPs), 10 (LADPs). Missing responses: 1 (IDPs).
EWERC
Part III. The provider telephone survey
155
III.3.5. Payment for upfront costs of starting work
There are three elements of upfront costs that staff considering entering care work may have
to pay for; these include the costs of CRB checks, the purchase of uniforms and the cost of
attending induction training if this is not paid for (this latter cost is more an opportunity cost
but there may be also out of pocket costs such as travel or childcare). While most
independent sector providers meet these costs there is a significant minority of providers who
do not (table III.21). This is particularly true with respect to CRB checks, where only one
third of IDPs paid for CRB checks up front with no strings attached and a further 2% paid but
required staff to reimburse the costs if they left within twelve months. A further 12% of IDPs
shared the costs 50/50 and 16% required staff to pay but reimbursed the costs if they stayed.
In more than a third of IDPs (37%) prospective employees had to pay themselves for the
checks. In LADPs, eight out of ten paid for the staff and only one shared the costs 50/50, but
one LA did require the applicant to pay. For homes the situation was more favourable to
potential employees than with IDPs with 64% of homes paying for the check and only one in
four homes (26%) not paying; the remainder either shared the costs (2%) or reimbursed if the
staff stayed (6%).
Table III.21. Percentage of organisations that pay for CRB checks
% of homes
% of IDPs
% of LADPs
% of all
Yes
64.2
33.3
80.0
51.8
50:50
1.9
11.8
10.0
7.0
Employer pays but staff pay if they leave
within 12 months
Staff pay but are reimbursed if they stay
1.9
2.0
0.0
1.8
5.7
15.7
0.0
9.6
No
26.4
37.3
10.0
29.8
Total Responses
53
51
10
114
No response
0
1
0
1
Payment by the employer for uniforms is more common with just under a fifth of homes, just
under a tenth of IDPs and no LADPs saying that staff had to pay for uniforms, although 6%
of homes and 22% of IDPs only provided one uniform and expected staff to pay for extra
uniforms (table III.22a). One IDP provided protective clothing and another gave a clothing
allowance for TUPE transferred staff. All but one home and all LADPs paid staff for
induction training but 24% of IDPs did not pay staff for attending induction. A further two
said they did not pay for part of the training (i.e. initial „orientation‟ and classroom training),
and two more said they only paid if staff stayed in employment for a certain period of time
afterwards (table III.22b). A summary of shares of employers not paying for the upfront costs
of starting work is shown in Figure III.17.
EWERC
Part III. The provider telephone survey
156
Table III.22. Percentage of organisations that require staff to pay for:
a. Uniforms
No
1
Yes
% of homes
% of IDPs
% of LADPs
% of all
74.5
68.6
100.0
74.1
25.5
31.4
0.0
25.9
Total responses
51
51
10
112
No response
2
1
0
3
% of homes
% of IDPs
% of LADPs
% of all
Yes
98.1
68.6
100.0
85.1
Partly
0.0
3.9
0.0
1.8
Yes if staff stay
0.0
3.9
0.0
1.8
No
1.9
23.5
0.0
11.4
Total responses
53
51
10
114
No response
0
1
0
1
Note: including those who only pay for extra uniforms.
b. Induction training
Figure III.17. Percentage of providers not paying for upfront costs of starting work
40
Homes
IDPs
LADPs
35
Percentage of providers
30
25
20
15
10
5
0
CRB checks
Uniforms
Note: For missing responses see tables III.21 and III.22.
EWERC
Induction
Part III. The provider telephone survey
157
III.4. Flexibility, working time and work organisation
While care homes and IDPs in the independent sector offer relatively similar pay levels and
conditions, there are greater differences in the employment context and employment
conditions between homes and IDPs once we consider the organisation of work and working
time. Both segments of the care sector face challenges; in domiciliary care the challenge is to
organise work and working time to fit a fragmented and time-specific demand for care for a
variable set of users located in their own homes rather than in a workplace, and to cover these
demands at least from early morning until evening and into weekends. When asked about
hours of care provision we found that all but seven of the IDPs (87%) provided cover until 10
pm or later with nearly one in four (23%) providing 24/7 cover and one in three (31%)
finishing cover after 10pm. Moreover, seven IDPs (13%) started cover before 7 am. The
LADPs also provided extended cover with all operating until at least 10pm, three out of ten
providing cover until later than 10pm (another saying that in practice they operated 6-11
while in principle it should be 7-10) and three provided 24 hour cover.
For care homes the challenge is always to deliver care on a 24/7 basis but with this being
delivered in a fixed workplace; here the main unpredictable factors are related to bed
occupancy and the needs of the service users on the one hand and the availability of staff on
the other. These differences led to tailored questions being asked as well as common
questions across the two subsectors. We therefore explore these arrangements separately for
domiciliary care and care homes, although drawing in many places on similar questions and
tables.
III.4.1. Flexibility, working time arrangements and work organisation in
domiciliary care
Employment contracts
The first and distinctive characteristic of domiciliary care is the extensive reliance on zero
hours contracts. We were aware that providers may make use of zero hours contracts (Rubery
and Urwin 2010) and that indeed such contracts had also been widely used in LA provisions
until trade unions pressed for better employment conditions (Horrell and Rubery 1991).
When asked about contracts for care workers we found that the practice was overwhelmingly
dominant with 69% of IDPs only offering zero hours contracts to their staff and only 12%
offering all staff some guaranteed hours, with the remainder (20%) offering a mix of zero
hours and guaranteed contracts (figure III.18). This practice of zero hours contracts reflected
the variability and uncertainty of workloads. By comparison, only one of the LA providers
offered a mix of guaranteed and zero hours with all the other LADPs offering only
guaranteed hours contracts.
EWERC
Part III. The provider telephone survey
158
Figure III.18. Types of employment contracts offered to care workers
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Zero hours only
Mix of zero and guaranteed hours
Guaranteed hours only
Note: Total responses: 51 (IDPs) and 10 (LADPs). Missing responses: 1 (IDPs).
Reasons given for offers of guaranteed hours within the independent sector to specific staff
members included the need to retain staff who were, for example, car drivers:
Zero hours only for all staff unless they drive a vehicle, in which case we offer guaranteed hours.
IL.D.2.DL
Or as a means of recruiting and integrating migrant workers:
We had a mix. We offered guaranteed hours to overseas workers for the first year. Then they all
work full time, in fact, excessive hours because they have a very good work ethic. After the first
year, there is no need for guaranteed hours, because they will work full time. (LK.D.3 DS).
The lack of fixed contract hours clearly gave providers discretion in their allocation of work,
and their ability to determine access to enough work seemed in some cases to be used as a
form of control over the staff.
People who are not flexible, they don‟t get so many hours. Now we have more staff we have more
control. It is important. (TE.D.1 CN (V)).
In particular the zero hours contracts left staff vulnerable to loss of work and pay when their
clients went into a home or hospital or died. The provider may seek to replace the work but
does not guarantee so to do if new work is not immediately available.
Zero hours only? All. We provide continuity of care – workers build up service users and if they
lose one, we replace them as quickly as possible. We have picked up ten care plans in the last one
and a half weeks. Before that all the agencies were scrambling for work. It is steady now.
(LKD.6.CL).
EWERC
Part III. The provider telephone survey
159
Working time patterns
Although most staff in domiciliary care were only offered zero hours contracts, in practice
most staff in the domiciliary sector worked more than short part-time hours and many were
involved in long hours working (figure III.19; table III.23). Only 4% of IDPs had the majority
of their staff regularly working less than 16 hours. At the other extreme 59% of IDPs said
short part-time work accounted for less than 10% of all staff (33% having no staff in this
category and 27% up to 10%). Long part-time hours - between 16 and 30 - were more
commonly used, with over 59% of providers having more than 50% of staff in this category
and 17% with ratios of 80% or more. One in four (24%) providers had less than 20% of staff
in this category, including 8% with no such staff, while at the other end 16% had 70% or
more working at least 30 hours. This suggests considerable scope for varying the working
time mix within domiciliary care providers. LA providers were most likely to make extensive
use of long part-time work, with relatively low proportions of either short part-time or fulltime hours.
Very long hours working (over 45 hours) was also far from uncommon in this sector: even
though no provider primarily used long hours work over 38% of domiciliary providers had
some staff working long hours. Even excluding those providers where working very long
hours occurred only on occasions for emergency cover, over 34% of IDPs recorded some
long hours working.
Figure III.19. Proportions of staff working different hours in IDPs
80
Percentage of providers
0%
70
1-10%
60
11-20%
21-30%
50
31-50%
40
51-70%
71-80%
30
81-90%
20
91-99%
10
100%
0
Under 16 hours
16-30 hours
30-45 hours
Usual weekly hours
Note: See table III.23 for responses.
EWERC
Over 45 hours
Part III. The provider telephone survey
160
Table III.23. Working-time patterns of care staff
% of staff
% of homes
% of IDPs
% of LAPDs
% of all
<50
100.0
95.9
100.0
98.1
>50
0.0
4.1
0.0
1.9
<50
58.8
40.8
14.3
47.7
>50
41.2
59.2
85.7
52.3
<50
39.2
67.3
100.0
56.1
>50
60.8
32.7
0.0
43.9
<50
100.0
100.0
100.0
100.0
>50
0.0
0.0
0.0
0.0
Total responses
51
49
7
107
No response
2
3
3
8
Under 16 hours?
16 – 30 hours?
30 – 45 hours?
Over 45 hours?
There is further evidence of extensive engagement by staff in the information on maximum
numbers of days worked. Here 28% of IDPs recorded a seven day maximum working week
and a further 49% had a six day maximum with only just over a fifth having a five days
maximum. In contrast over half of LA domiciliary providers had a five day maximum (table
III.24).
Table III.24. The maximum number of days a week worked by care staff
Number of days
per week
% of homes
% of IDPs
% of LADPs
% of all
3
1.9
0.0
0.0
0.9
3.5
1.9
0.0
0.0
0.9
4
9.6
0.0
0.0
4.5
5
53.8
21.6
55.6
39.3
5.5
0.0
2.0
0.0
0.9
6
23.1
49.0
33.3
35.7
7
9.6
27.5
11.1
17.9
Total responses
52
51
9
112
No response
1
1
1
3
This use of six and seven day maxima reflected the prevalence of weekend working (figure
III.20). Nearly three fifths of independent domiciliary providers and 89% of LADPs said that
all their staff were engaged in regular weekend working. However, there appeared to be some
choice in the way weekend working was organised as around 28% of IDPs had less than half
the staff regularly working weekends.
EWERC
Part III. The provider telephone survey
161
Figure III.20. The percentage of care workers who regularly work weekends
100
Homes
90
IDPs
LADPs
80
Percentage
70
60
50
40
30
20
10
0
0 – 25%
26 – 50%
51 – 75%
76 – 99%
100%
Percentage of staff
Note: Total responses: 50 (homes), 49 (IDPs) and 9 (LADPs). Missing responses: 3 (homes), 3 (IDPs), 1
(LADPs).
Even when an organisation had a policy that all staff should work weekends the reality might
prove different. Some providers claimed that staff were apparently prone to backtracking on
their agreement to work weekends at recruitment.
They work alternate weekends. We try to make them all work weekends, but it is really hard to get
people to work weekends. We have to look closely at applicants. They say that they will work
weekends, then two months in, they say they can‟t work weekends. (LKD.6.CL).
All our carers, when they come for the job, they‟ll do anything. It‟s once they‟ve got in and then
they say, „I can‟t do these evenings, or I can‟t do that day.‟ That‟s when it starts, once they‟re in
the job. Because when they‟re interviewed they are told it‟s mornings, afternoons evenings,
weekends and all that, and it‟s „Oh, yes, it‟s fine, I‟ll do anything.‟ And then you find out that they
won‟t. (ON.D.2 AS).
The problems of staffing weekends led some providers to try a range of different systems:
We struggle to find staff who will work weekends, as everyone wants these off. We did run
alternative weekend work, but now we offer one day at weekends, so that staff have to work
either Sat or Sun to relieve the existing staff and give cover. Some of the extra staff only work
weekends. ( IL.D.2.DL).
Or they recruited specifically for the unpopular time periods:
We‟ve also got carers who just want evening work, so you‟re looking around eight hours a
week for them. And the same at weekends. We‟ve just got weekend workers who just want, you
know, say ten hours a week. (ON.D.3 BN).
EWERC
Part III. The provider telephone survey
162
Working time scheduling
Work scheduling is highly complex in domiciliary care because of the number of clients,
their geographical spread, the need for repeat visits and the fluctuating mix of clients and
demands. In this context there may be tensions between the need to provide continuity of care
for service users - where the same care worker or team of care workers is always provided and the need to organise the care work into a work schedule for individual employees. To tap
into these tensions we asked first about how important it was to provide continuity of care for
service users. All providers responded that it was either very important or important, with
94% of independent providers, in fact, saying it was very important (table III.25). This
suggests that in principle, at least, providers recognize a need to schedule work around
existing allocations to users.
Table III.25. The importance of organising working hours to provide continuity of care
% of IDPs
% of LADPs
% of all
Very important
94.2
77.8
91.8
Important
5.8
22.2
8.2
Neutral
0.0
0.0
0.0
Unimportant
0.0
0.0
0.0
Very unimportant
0.0
0.0
0.0
Total responses
52
9
61
No responses
0
1
1
We then asked about how important it was to schedule work to fit employees‟ circumstances.
Although there was, again, strong support for this being an important factor, with 89% of
IDPs saying it was important, or very important, the share saying it was very important was
significantly lower, at 64%, compared to the 94% who considered continuity of care for users
to be very important (table III.26). The share was even lower for LA providers with only 44%
of inhouse providers saying it was important or very important. These answers may reflect
the changes in LA practice where they have moved from offering domiciliary care workers
fixed hours within a limited window - often school hours - to asking staff to cover hours over
a more extended period including early mornings and evenings.
We explored further the consequences of the variability of demands and the priority to
continuity of care by asking whether staff were able to get work schedules that fitted their
preferences all the time or most of the time. It is likely that they interpreted this question as
referring to the range of what was possible rather than in relation to absolute preferences, as
one provider noted:
I think that‟s a tricky one because people‟s preferences might be working Monday to Thursday
ten till two, but they know that isn‟t an option, so its whether people think the rotas are
reasonable, I mean we get the occasional „I‟ve done more weekends than … ,‟ and that‟s
obviously worth listening to. (RD.D.2.CL)
EWERC
Part III. The provider telephone survey
163
Table III.26. The importance of organising working hours to fit employees’
circumstances
% of IDPs
% of LADPs
% of all
Very important
63.5
22.2
57.4
Important
25.0
22.2
24.6
Neutral
9.6
44.4
14.8
Unimportant
0.0
11.1
1.6
Very unimportant
1.9
0.0
1.6
Total responses
52
9
61
No responses
0
1
1
Figure III.21 shows that the vast majority of IDPs – 98% - said their staff were able to get
schedules that fitted their preferences all, or most of the time, but only a quarter said it was all
of the time, suggesting some requirements for staff to adapt to schedules that do not match
their preferences.
Figure III.21. The overall matching of work schedules with care workers’ preferences
for particular hours
100
Homes
90
IDPs
LADPs
80
Percentage
70
60
50
40
30
20
10
0
All of the time
Most of the time
Some of the time
Occasionally
Note: Total responses: 52 (homes), 52 (IDPs) and 10 (LADPs). Missing responses: 1 (homes).
We also asked IDPs whether they would expect care staff to have to tolerate working longer
than scheduled due to unanticipated needs of service users or to tolerate variations in hours or
location at short notice (figure III.22). On working longer than scheduled only two providers
thought this would never happen and 15% of independent providers and 30% of LA providers
felt it was indeed something care workers would need to tolerate; the majority, however –
over four fifths of IDPs and 70% of LADPs - saw this as only an occasional requirement On
variations in hours or location at short notice 85% of IDPs said that they would expect them
to tolerate it often or occasionally although the majority of these put it down as occasional
EWERC
Part III. The provider telephone survey
164
(77%) and only 8% regarded it as a regular issue. LA providers expected more variability
with 20% saying they did expect staff to tolerate such changes and 70% saying yes,
occasionally.
Figure III.22. The requirement for care workers to tolerate longer working hours or
variations in hour due to unanticipated needs
a. Tolerate longer working hours
100
IDPs
90
LAPDs
80
Percentage
70
60
50
40
30
20
10
0
Often
Occasionally
Never
b. Tolerate longer working hours or variations in hour due to unanticipated needs
100
IDPs
90
80
Percentage
70
60
50
40
30
20
10
0
Often
Occasionally
Note: Total responses: 52 (IDPs) and 10 (LADPs).
EWERC
Never
LAPDs
Part III. The provider telephone survey
165
Table III.27. Staffing arrangements to cover for absences/vacations/unfilled vacancies
% of IDPs
% of Homes
% of LADPs
% of all
Ask existing
staff to work
extra hours
90.4
Use external
agencies
1.9
Use list of staff
available for
temp cover
0
combined with other methods
7.7
0.0
7.7
All using the method
98.1
1.9
7.7
sole method
56.6
3.8
0
combined with other methods
39.7
20.8
34.0
All using the method
96.3
23.9
34.0
sole method
80.0
0
0
combined with other methods
20.0
10.0
10.0
All using the method
100.0
10.0
10.0
sole method
73.9
2.6
0
combined with other methods
23.5
10.5
20.0
All using the method
97.4
13.1
23.5
sole method
Note: Total responses: 53 (homes), 52 (IDPs), 10 (LADPs).
These requirements for flexibility were further exacerbated by the reliance of domiciliary
care providers on their existing staff to cover extra shifts: 80% of LA providers and 90% of
IDPs only used existing staff to cover extra shifts and only one IDP from our sample of 52
used an external agency exclusively for cover. All others relied on existing staff with 8% of
IDPs using a list of temporary staff in addition to existing staff to provide cover. The pattern
for LA providers was similar with all using existing staff and only one combining this with an
external agency and one with a list of temporary staff (table III.27).
To probe further on how flexibility was managed we also asked about how easy or difficult it
was to find staff willing to work extra hours, either on the day itself or with two to three days
notice. The majority of providers found it easy, or very easy to find staff willing to work
additional hours at 2-3 days notice (86% of IDPs and 70% of LADPs). Only 8% of IDPs and
20% of LA providers found it difficult, or very difficult to find staff willing to work
additional hours with this amount of notice (table III.28). Even on the same day, the majority
found it easy, or very easy to find staff to work additional hours (77% of IDPs and 70% of
LA providers). However, the number recording difficulties increased when the notice was
very short with around a fifth of IDPs finding it difficult, or very difficult to find staff willing
to work extra hours on the same day.
The comments from providers indicated that the difficulty in part depended upon how
familiar staff were with the users:
I suppose it depends on what you‟re asking them to do. If it‟s working with someone that they
know, it‟s almost always that they will sort that out between themselves because that‟s, you know,
about your commitment and knowing that person. If you want someone to do something that they
are less familiar with then that might need more discussion. (RD.D.2.CL).
EWERC
Part III. The provider telephone survey
166
It depends on their mood and what you are asking. If it is to work extra time with an existing
client, that might be okay, but if you are asking them to go out for another slot…that might be
difficult. (LK.D.6.CL).
Table III.28. Finding staff willing to work additional hours at short notice
% of IDPs
% of LADPs
% of all
Very easy
9.8
10.0
9.8
Easy/quite easy
76.5
60.0
73.8
Neither difficult nor easy
5.9
10.0
6.6
Quite difficult
7.8
10.0
8.2
Very difficult
0.0
10.0
1.6
Very easy
2.0
0.0
1.6
Easy/quite easy
74.5
70.0
73.8
Neither difficult nor easy
3.9
10.0
4.9
Quite difficult
17.6
10.0
16.4
Very difficult
2.0
10.0
3.3
Total responses
51
10
61
No response
1
0
1
2-3 days notice
Same day
It also varied according to the different ways in which staff might assess the opportunity for
extra work:
People will accept the rota if it‟s got the times that they can work, so they accept it but then they
start to plan other things in the gaps, and then they don‟t want to give those gaps up, rightly so or
wrongly so, depending on your point of view. (ON.D.1 DN).
Sometimes it‟s okay, sometimes not. Before Christmas people want money. If the husband‟s laid
off they want extra hours. It depends. They know holiday pay depends on the amount they work,
so know if they work more their holiday pay goes up. (LK.D.3 DS).
Some providers offered inducements to overcome these problems:
Very easy, we pay enhanced rates, so they are knocking on our door. (LK.D.5 CN (V)).
Work organisation and working time
Behind the working-time patterns and schedules lies the organisation of work and, in
particular, the organisation and duration of visits to clients. All the interviewees said that visit
lengths were tightly defined except for one manager of an LADP who answered no to this
question. We asked managers what was the minimum and average length of a visit and the
modal response to this question was 15 minutes minimum and 30 minutes average where
both figures were given (20 out of 29 responses). Figures III.23a and b show that short visits
EWERC
Part III. The provider telephone survey
167
to clients were the norm. Seven in ten IDPs (68%) had minimum length of visits below 30
minutes (including around 3% with no minimum). This includes 60% of providers reporting a
minimum of 15 minutes. Only 5% of IDPs recorded minimum visits above 30 minutes.
Figure III.23b shows data on average visit lengths, although the data are less complete with a
total of only 28 valid responses. The most popular average duration was 30 minutes (76% of
respondents) with 14% citing an average length of longer than 30 minutes and under 10%
giving an estimate of average duration at less than 30 minutes. A similar pattern was found
for the LADPs, with all giving either no minimum or 15 minutes but average visit lengths
were said to be 30 minutes in five out of the seven cases reporting an average duration, with
the two remaining cases reporting longer averages, at 45 minutes and one hour respectively.
Figure III.23. The minimum and average lengths of visits to clients
a. The minimum length of a visit
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
No minimum
15 minutes
20 minutes
30 minutes
45 minutes or over
Note: Total responses: 37 (IDPs) and 8 (LADPs). Missing responses: 15 (IDPs) and 2 (LADPs).
b. The average length of a visit
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
20 minutes
27 minutes
30 minutes
45 minutes
60 minutes
Note: Total responses: 21 (IDPs) and 7 (LADPs). Missing responses: 31 (IDPs) and 3 (LADPs).
EWERC
Part III. The provider telephone survey
168
This highly fragmented structure of visits is also reflected in the approach taken to minimum
working time periods (table III.29), with four in five IDPs (81%) operating a minimum
working time of only two hours or less (including 63% with no minimum). Only 8% and 4%,
respectively, had minimum work periods of between 2 and 4 hours and over 4 hours. In
contrast LADPs were fairly evenly split between those that had no minimum work period and
those that had minimum work periods in excess of two hours (14% in excess of 4 hours) with
only one case having a minimum between 15 minutes and 2 hours.
Table III.29. Approach to minimum length of work periods
% of IDPs
% of LADPs
% of all
No minimum
62.5
42.9
60.0
15 minutes – less than 2 hrs
18.8
14.3
18.2
2 – 4 hours
8.3
28.6
10.9
Over 4 hours
4.2
14.3
5.5
Depends/varies
6.3
0.0
5.5
Total responses
48
7
55
No response
4
3
7
When asked about how working time was organised, a wide variety of responses was
obtained, in part because the organisation within an individual provider was complex and
varied among staff. One issue was whether staff worked split shifts: overall only 12% of IDPs
and 11% of LADPs said that this was their main pattern of working, with the vast majority
saying they operated a variety of shifts (table III.30).
Table III.30. Types of shift working arrangements
% of IDPs
% of LADPs
% of all
Continuous shifts
7.8
11.1
8.3
Split shifts
11.8
11.1
11.7
Variety of shifts
80.4
77.8
80.0
Total responses
51
9
60
No response
1
1
2
Many referred to the hourglass demands for care with peak demands in morning and
evenings; others divided the work into four main periods - mornings, lunch, teas, bed, and
either allowed staff to work mixes of these periods or joined mornings with lunches and teas
with bed, or allowed for split shifts between mornings and evenings on the grounds that this
suited some staff to have a break in the middle of the day:
They don‟t do continuous shifts. They may do a four hour stint in the morning, you know, with
travel time between the calls, then have a break for a couple of hours and then work from two till
eight in the evening. (RN.D.2.CN).
EWERC
Part III. The provider telephone survey
169
One provider recognised that this practice caused problems as it lead to perceptions that the
working day was very long even if paid hours were much shorter:
Because these people are having, like, four visits a day, the carers are getting tired doing the
four visits because they seem to be at work all the time, even though they get a break in
between. They are thinking, „Oh, I‟ve done a twelve hour day‟ – So what I want to do is do a
morning run where they do the mornings and the dinners, and then they do a tea come bed
run. … So if they do a morning run they won‟t be on till the following evening so they are
getting like a full day, a night and a morning off aren‟t they? (ON.D.2 AS)
One provider had four shifts – two short morning and evening shifts and then two longer
mornings, plus lunch and teas plus evening shifts (i.e. 7 a.m. to 10 a.m., 8 a.m. to 1 p.m., 4pm
to 7 p.m. and 4 p.m. to 10 p.m.). One said they organised work in four to six hour blocks
while seven said they operated a shift arrangement, in some cases involving permanent shifts
but in others rotating shifts. In other cases the working time arrangements appeared to be
even more variable – dependent upon both the mix of users and the availability of care staff.
Four providers referred to the use of computer software to generate the working time
schedules. Patterns of variability were also found in the LADPs, with rotas known at most
one week or in one case two weeks in advance and more variable hours for those engaged in
more specialised work such as EMI or reablement. One LADP tried to overcome the
problems of split shifts by alternating shift patterns:
It depends on availability. Depends. Can be split shifts – depends on carers availability – so it
can be any of these. If there were split shifts we might roster it so that they worked mornings
one week, then evenings the next week. (LK.DIH.1 DP).
The fragmentation of work organisation raises the issue of whether or not staff are paid or not
for a break between service users in their work schedules. Figure III.24 clearly demonstrates
that in general staff are not paid with only 8% of IDPs saying they would provide a paid
break and 88% saying the break would be unpaid.
Figure III.24. Payment of non-travel breaks between service users
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Paid break
Some paid, some unpaid
Unpaid break
Note: Total responses: 50 (IDPs) and 9 (LADPs). Missing responses: 2 (IDPs), 1 (LADP).
EWERC
Part III. The provider telephone survey
170
There are clearly variations between providers, but also among different types of staff within
providers. 4% of IDPs and 22% of LADPs said there was a mixture of paid and unpaid
breaks. Car drivers were more likely to be found replacement work, and all TUPE transferred
staff were more likely to be paid:
We arrange a block of clients. The TUPEd staff are all paid. The „walkers‟ (as opposed to
drivers) are expected to come into the office and work on some training books or do some paper
work in the office e.g. updating the client care plans – we usually can find the drivers other work.
(AH.D.3.CN).
If they are in Respite, we pay them. If there is a huge gap, we try to fill that for them. If they have
a half hour gap, we might make them take half an hour unpaid break. (TE.D.1 CN (V)).
The payment of breaks for TUPEd staff reflects current practice within LADPs where two
thirds (67%) said they would provide a paid break compared to just 8% of IDPs, although
efforts are made to redeploy staff when breaks occur:
If [there is] no work, we bring them into the office or offer them to care schemes to work and
recharge for their time. (LK.DIH.1 DP).
The issue of paid or unpaid breaks appears to be related to the extent to which the labour
force is very local; one factor in the acceptability of the working schedule may be not just
time scheduling but also how manageable the round offered was in relation to distance.
We just try to keep them as locally as possible. When we do the rotas, well, before we send the
rotas out we‟ll make sure they‟re in one area and they‟re not being sent backwards and forwards.
So hopefully that‟ll reduce the amount of petrol they‟re going to be using. (ON.D.3 BN).
It may also be that where there is a close meshing of work with family and home
responsibilities that providers feel able to ask staff to take unpaid breaks and staff may be
willing to accept the arrangements. However, this may restrict the pool of labour supply on
which a provider may easily draw to those where opportunities to return home for part of the
day are at least seen as having some positive benefit.
Only one agency normally organised work in pairs while 28% of IDPs and 10% of LADPs
said care workers worked alone all or most of the time. Over 90% of LADPs and over 70% of
IDPs said work in pairs might be used around half the time to reflect the specific needs of the
user (table III.31).
One particular type of work that may be done in pairs is care in the late evening or night time
We asked whether care workers might be expected to tolerate working late at night on their
own and while the majority of providers said no (64% of IDPs and 70% of LADPs), well
over a third of IDPs said yes or occasionally (37%), as did 30% of LADPs (table III.32).
One factor limiting the use of pairs was said to be the changing mix of clients:
[Care staff work] mostly alone, some doubles. We have some double runs, but it‟s hard to keep
this going as clients change frequently. (LK.D.3 DS).
EWERC
Part III. The provider telephone survey
171
Table III.31. The organisation of care work in pairs or alone
% of IDPs
% of LADPs
% of all
Alone or mostly alone
27.5
10.0
24.6
Half and half; Depends on needs
of service user
70.6
90.0
73.8
In pairs or mostly in pairs
2.0
0.0
1.6
Total responses
51
10
61
No response
1
0
1
The issue of safety of staff – by both area and time of night - was one that some providers felt
was not solely their responsibility:
One of the things that we were discussing only yesterday was the effect of lone working in the
current climate, asking the council whose liability is our staff‟s safety. Is it solely ours or are they
going to share the liability? … But we have actually done [„double-up‟ calls] where we feel that
areas are pretty unsalubrious. We put in two care workers just purely for their safety. (ON.D.1
DN).
Table III.32. Working alone at night as an expected part of domiciliary care work
% of IDPs
% of LADPs
% of all
Yes
11.5
20.0
12.9
Occasionally
25.0
10.0
22.6
Never
63.5
70.0
64.5
Total responses
52
10
62
No response
0
0
0
In addition to the risks associated with night work, particularly alone, there are other risks or
potentially unpleasant or dangerous conditions associated with care work. To tap into this
dimension of work we asked care providers to what extent they would expect staff to tolerate
working in insanitary conditions and to what extent they would be expected to tolerate
working with aggressive service users.
While only one provider said care workers should have to tolerate insanitary conditions on
more than an occasional basis, the frequency of this problem was indicated by the 42% of
IDPs and 70% of LADPs who suggested they would need to tolerate it occasionally (figure
III.25 and III.26).
You wouldn‟t believe the way that some people do live. Obviously what we can do is, we can take
responsibility for that household and ensure that cleanliness is brought up. But it‟s very, very
difficult. You can‟t go in and upset somebody and tell them that they are living in a pigsty. But
you might be able to… So the answer to it is occasionally its bloomin‟ awful. It‟s smelly, it can be
dirty, it can be dark and dingy. The place that they may go to might not be very salubrious.
(ON.D.1 DN).
EWERC
Part III. The provider telephone survey
172
Figure III.25. Toleration of insanitary working conditions
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Often
Occasionally
Never
Note: Total responses: 52 (IDPs) and 10 (LADPs).
Figure III.26. Aggressive service users as an expected part of domiciliary care work
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Often
Occasionally
Never
Note: Total responses: 52 (IDPs) and 10 (LADPs).
Working with aggressive service users was an even more common part of the job with only
15% of IDPs and 10% of LADPs saying that staff would not need to tolerate it and indeed
30% of LADPs regarded it as more than an occasional problem, compared to 11% of IDPs.
EWERC
Part III. The provider telephone survey
173
This may reflect the more specialist nature of LADPs work in some LAs. However, the
majority of both sets of providers said it had to be tolerated occasionally.
III.4.2. Flexibility, working time arrangements and work organisation in care
homes
Employment contracts and working time
Working time in care homes is not only more guaranteed than in domiciliary care but also
more often full-time. Figure III.27 plots the percentage of providers that employ care workers
for different numbers of weekly hours (see, also, table III.23 above). Over three fifths of
responding homes had at least 50% of staff working 30-45 hours and none had a majority
working short part-time hours. Nevertheless, the share of part-time working is significant
considering that these homes need to provide 24 hour, 7 days a week care. Over 41% of
responding homes had more than 50% in long part-time. If we look at the distribution of
homes by shares of long part-time and more full-time hours we find quite a wide variation in
patterns; thus over 40% of responding homes had less than 20% of staff in long part-time
work but at the other end of the spectrum 25% had 70% or more in this type of working time
category Similarly 16% of homes had fewer than 20% in full time work while 44% of homes
had more than 70% in this category.
However, although more workers are in full-time jobs than in domiciliary care, fewer work
very long hours (that is, over 45 hours per week); only 25% of homes had any staff in this
category compared to 38% of IDPs. Excluding those working very long hours only on
occasions for emergency cover reduces the share of homes with anyone on more than 45
hours to 17%. Moreover, under 10% of care homes had a seven day maximum working week
and only 33% had either a six or seven day maximum compared to 77% of IDPs (Table
III.24).
However, when it comes to weekend working it is equally the norm in care homes for all staff
to be regularly involved in weekend work, with 70% of care homes, over ten percentage
points more than IDPs, involving all staff in regular weekend working (see figure III.20
above). The pressures of staffing weekends nevertheless remained considerable. Some homes
sought to solve the problem through stipulations at interview:
They are expected to work weekends. It‟s a 365 day a year job. You know, weekends, Bank
Holidays, Christmas Day because it‟s a 24/7 service, and at interview we ask that question. It‟s
about flexibility.( HD.HN.1.C.LV).
Nevertheless the problems of scheduling sometimes meant that staff might be under pressure
to work more weekends than they had signed up for:
Always difficult at weekends, because I like to give staff alternate weekends off, but sometimes it
is difficult.(OM.HN.2.A.N).
EWERC
Part III. The provider telephone survey
174
Figure III.27. Proportions of staff working different hours in homes
80
Percentage of providers
0%
70
1-10%
60
11-20%
21-30%
50
31-50%
40
51-70%
71-80%
30
81-90%
20
91-99%
10
100%
0
Under 16 hours
16-30 hours
30-45 hours
Over 45 hours
Usual weekly hours
Note: see table III.23 for number of responses.
Working time scheduling
As in domiciliary care the majority of homes (96%) claimed to be able to give staff work
schedules that fitted their preferences all, or most of the time and a higher share of homes –
almost a third rather than a quarter - were able to meet preferences all of the time compared
to domiciliary providers (see figure III.21 above). In homes the problems related not so much
to changes in service users but to the need to cover 24/7 particularly in holiday periods or
when there is a high rate of sickness:
[We have] a four-week rota. It is very difficult to organise. We always try our best to give people
what they want, but at holiday times, it is very difficult. They request, and we try our best. We
rota so that all have the same number of weekends off and the number of hours they want. Some
work nights only, the rest work days, sometimes earlies, and sometimes lates. Staff tend to be very
flexible. If someone leaves suddenly or is off sick, then we are under-staffed. We are flexible, and
they are flexible and will fill in. (TE.H.4 AS).
Care homes, as with IDPs, were primarily reliant on their existing staff for temporary cover
with 57% relying on existing staff only and 96% using existing staff at least in combination
with other methods (see table III.27 above). Only 4% used external agencies as their only
source of cover:
EWERC
Part III. The provider telephone survey
175
It varies. Staff are usually flexible. The new Filipinos are keen to earn money to send home and
they volunteer for extra shifts – they sometimes switch between housekeeping and care work. We
are lucky, but they can all say no to extra work. (LK.H.4 AL).
Other methods were much more common in care homes than domiciliary care, however, with
23% making use of external agencies and 33% using a list of temporary workers.
Work organisation and working time
The main question we asked about work organisation and working time related to first of all
minimum staffing levels and secondly how working time was actually organised. The
adoption of minimum staffing levels was common, with 87% of responding homes claiming
to have minimum staffing levels. Further probing of what these minimum staffing levels
amounted to revealed differences in ratios between day and night shifts (often with further
variations for afternoons and early evenings but, as mornings had the most staff and nights
the least in all cases, we concentrate on the morning to night ratio). Of the 19 cases where
sufficient detail was given of variations across shifts we found that 11 had night ratios in
excess of 50% of the morning shift but in eight cases the night time staffing ratios were half
or less. Some homes gave us the ratios in relation to occupied beds with, for example, the
ratio varying from 1 in 5 in the morning to 1 in 8 at night. In some cases the minimum
staffing ratios were given as a constant over the 24 hours and therefore probably referred to
night time ratios. Quite a number of homes gave ratios not just overall but in relation to
number of senior or qualified staff. These minimum staffing ratios thus clearly create
scheduling constraints both by numbers of staff but also qualifications and seniority. Most
ratios are implicitly related to bed occupancy but adjustments to bed occupancy occur in
rather large lumps as one provider with 27 beds noted that a reduction of occupancy of three
lead to a reduction in staffing levels by a quarter.
Because we‟re three patients down the owner has reduced numbers, reduced [staff] numbers,
so I‟m not too happy about that, but that‟s the way it goes at the moment. …(ON.HN.1 BS).
When it came to shift patterns the homes had different strategies as to whether they used
permanent or rotating shifts with half using rotating shifts and around a third (37%) using
permanent shifts. A mixture of permanent and rotating shifts was used by 14% of homes.
While permanent shifts were often used to meet preferences some homes recognised that this
created problems in reducing staff experience and understanding of the work of the home:
And the shifts, some of the staff here ….work so many nights but we‟re trying to get away
from that and have the rotated shift pattern so that everyone understands what happens 24/7.
(HD.HN.1.C.LV)
Further variations related to length of shifts. Most used a three shift system but at least four
homes operated long shifts of 11 or 12 hours. Two homes offered long days as a choice to
staff. As most involved all staff in working weekends and nights it was only a minority of
EWERC
Part III. The provider telephone survey
176
homes that employed some weekend only staff. Other ways of fitting hours to preferences
included one home that allowed staff to choose their day off. Many also mentioned that
breaks were paid although one said the home did not pay breaks for new staff and another
specified that full-timers were granted a 30 minute paid break but part-timers only ten
minutes.
Table III.34. Use of rotations between shift arrangements in homes
% of homes
Rotate
50.0
Stay on same shift
36.5
Half and half
13.5
Total responses
52
No response
1
EWERC
Part III. The provider telephone survey
177
III.5. Employee development and training
An important element in human resource management is staff development and training. This
starts with induction but continues with opportunities for training and for development
through systematic appraisal systems. We address these three inter-related issues in this
section in turn.
III.5.1. Induction of new staff
When asked about the length of induction training for new staff there was a variety of
responses ranging from one day to six months. However, many respondents distinguished
between an initial induction period of a few days followed by a number of weeks shadowing,
working under supervision, probation and mandatory training courses. Others said the length
of induction could vary according the previous experience and qualifications of the new
recruit, or the length of time taken for the CRB check.
The majority of providers carried out the induction training themselves. Only 3% said the
training was provided by an external training organisation and a similar share reported using
the local authority. A further 10% said the training was provided by themselves and the local
authority, or other organisation, or a combination of all three.
Table III.35 reports managers‟ perceptions of how long new staff need to become competent
in the role. There is a good deal of variation of perceptions between IDPs, LADPs and
homes. Over one quarter of IDP managers said new recruits would be able to do the job as
well as existing staff in one week or less, compared to 15% of home managers and none of
the LADP managers. At the other end of the scale only around a fifth (21%) of IDP managers
thought this would take between one and six months compared with half of the LADP
managers and two fifths (40%) of home managers.
Table III.35. Length of time needed for new staff to do the job as well as existing staff
% of homes
% of IDPs
% of LADPs
% of all
One week or less
15.4
26.9
0.0
19.3
More than one week - up to 1 month
36.5
36.5
30.0
36.0
More than 1 month up to 6 months
40.4
21.2
50.0
32.5
Depends
7.7
15.4
20.0
12.3
Total responses
52
52
10
114
No response
1
0
0
1
Some respondents observed that the length of time taken to become as competent as existing
staff depended on the individual (8% of homes, 15% of IDPs and 20% of LADPs). Previous
EWERC
Part III. The provider telephone survey
178
experience did not necessarily mean that the new member of staff would become competent
in a shorter period of time:
This depends on the person. Some fit in very well. Some with a lot of experience might have
developed poor practice, so sometimes it‟s better for people not to have any experience. (TE.D.1
CN (V)).
Working in a care home would not necessarily prepare someone to undertake domiciliary
care:
It depends what their experience has been because if they‟ve worked in a very sort of institutional
way then it takes a long time to undo that so it depends what the individual experience has been.
(RD.D.2.CL).
III.5.2. Training
All establishments in the survey had some staff trained to NVQ level 2, but there was a wide
variation in the proportions (between 15% and 100%). Table III.36 and figure III.28 show
that attainment of NVQ level 2 was significantly higher in the homes than the IDPs, with
53% of homes having 70% or more staff trained to NVQ level 2, compared with only 33% of
IDPs. On the other hand, over half the IDPs (52%) had fewer than 56% of staff trained to
NVQ2 compared with under 30% of homes.
Table III.36. Proportion of care workers trained to NVQ level 2
% of homes
% of IDPs
% of LADPs
% of all
45% or less
13.7
30.8
22.2
22.3
46 – 55%
15.7
21.2
0.0
17.0
56 – 69%
17.6
15.4
22.2
17.0
70% or more
52.9
32.7
55.6
43.8
Total responses
51
52
9
112
No response
2
0
1
3
Managers were asked how likely they were to meet the Care Standards Act (2000).target of
50% of staff trained to NVQ Level 2. Close to nine in ten homes (89%) and eight in ten
LADPs (80%) had already met this target (figure III.29). Although the majority of IDPs had
also met the target the proportion is lower, at only 65%. However, a further 21% of IDP
managers felt that they would be able to meet the target soon. In line with these findings,
14% of IDPs were experiencing difficulties meeting the target, compared with only one
LADP and just under 4% of homes.
EWERC
Part III. The provider telephone survey
179
Figure III.28. Share of care staff in homes and IDPs with NVQ level 2 by share of
providers in sample (cumulative percentage of providers)
100%
90%
% of staff with NVQ 2
80%
70%
60%
50%
40%
30%
20%
10%
0%
0%
10%
20%
30%
40%
50%
60%
Homes
IDP's
70%
80%
90%
100%
Figure III.29. Likelihood of meeting the 50% NVQ level 2 target
100
Homes
IDPs
LADPs
90
80
Percentage
70
60
50
40
30
20
10
0
Already met
Will meet soon
Experiencing difficulties
Note: Total responses: 52 (homes), 51 (IDPs) and 10 (LADPs). Missing responses: 1 (homes), 1 (IDPs).
We probed this question further by asking the managers who said they were experiencing
difficulties meeting the 50% NVQ level 2 target, what factors were contributing to these
difficulties. The responses are categorised in Table III.37. The two biggest problems for the
IDPs were staff turnover and training-related problems (with providers, assessors or funding)
EWERC
Part III. The provider telephone survey
180
with almost 39% of responses in each of these categories. Problems concerning staff
motivation and pressure of work accounted for just over 22% of responses from IDPs. Staff
turnover and motivation were the biggest problems for the homes, with 38% of responses in
each of these categories. One specifically mentioned having older staff who were very
experienced but did not want to take qualifications. Training-related problems accounted for
one quarter of responses from the care homes.
Table III.37. The factors that make it difficult to meet the 50% NVQ level 2 target
% of homes
% of IDPs
% of LADPs
% of all
Staff turnover
37.5
38.9
50.0
39.3
Staff motivation
37.5
16.7
0.0
21.4
Pressures of work (e.g. scheduling, fatigue)
0.0
5.6
0.0
3.6
Training provider/ assessor/ funding problems
25.0
38.9
50.0
35.7
Total responses
8
18
2
28
No response/not applicable
45
34
8
87
Figure III.30 shows the percentages of staff trained to higher levels – NVQ level 3 or NVQ
level 4. As with the NVQ2,, the proportions attaining these qualifications were significantly
higher in the homes, with 40% having over 20% of staff trained to these levels. The
corresponding figures for the IDPs and LADPs are 16% and 20%, respectively. At the other
end of the scale, only one quarter of homes had 10% or fewer staff trained to these levels,
compared with 59% of IDPs and 60% of LADPs.
Figure III.30. Proportion of care workers trained to NVQ levels 3 and 4
70
Homes
IDPs
LADPs
60
Percentage
50
40
30
20
10
0
10 percent or less
11 – 20 percent
21 – 29 percent
30 percent or more
Note: Total responses: 45 (homes), 50 (IDPs) and 5 (LADPs). Missing responses: 7 (homes), 3 (IDPs), 5
(LADPs).
EWERC
Part III. The provider telephone survey
181
We followed this question up by asking whether any staff actually needed to have NVQ
Level 3 and, if so, which staff, and whether they were recruited externally or internally
trained. Table III.38a shows that 54% of IDPs and 88% of LADPs did need to have some
staff trained to NVQ level 3. The most frequently mentioned role requiring NVQ3 was that of
senior care worker (18 responses). In many cases it was apparent that, on attaining this
qualification, the care worker would automatically become a senior care worker and receive a
pay increase. Other higher level roles were also mentioned as requiring the jobholder to be
trained to NVQ3 level, such as supervisors and team leaders (6 responses) and care
coordinators (6 responses). Some specialised types of care were also said to require an
NVQ3 trained care worker, such as hospital discharge and care for people with specific
medical conditions such as diabetes.
Providers‟ requirements for seniors and supervisors to have NVQ3 were sometimes not
matched by [training] providers‟ willingness to accept initially people who did not already
have supervisory responsibility:
It‟s quite difficult to get them on Level 3 because they don‟t have supervisory responsibility, it can
be difficult to get providers to take them at Level 3. (LK.D.3 DS).
Table III.38. Staffing issues for care workers needing NVQ level 3
a. Requirement for some staff to have NVQ level 3
% of IDPs
% of LADPs
% of all
No
46.2
12.5
41.7
Yes
53.8
87.5
58.3
Total responses
52
8
60
No response
0
2
2
b. Use of external recruitment of NVQ3 trained staff or internal training
% of IDPs
% of LADPs
% of all
Internally trained
66.7
100.0
73.5
Recruited externally
7.4
0.0
5.9
Both
25.9
0.0
20.6
Total responses
27
7
34
No response/not applicable
25
3
28
We asked those managers who said they needed to have some of their care workers trained to
NVQ Level 3 whether these staff were recruited externally or internally trained. The majority
(two thirds of responding managers from IDPs (67%) and all the responding LADP
managers) said they were internally trained. Just over one quarter of IDP managers (26%)
said they would fill these roles both with new recruits and/or internally trained staff. Only 7%
of IDP managers said these roles would be filled exclusively with new recruits (table III.40b).
EWERC
Part III. The provider telephone survey
182
One employer mentioned the difficulty of recruiting people who were already qualified at
NVQ level 3:
Usually [we train staff] internally, as it is very hard to attract people with NVQ 3 externally.
(IL.D.2.DL).
Some IDPs and LADPs provided more specialised types of care, including intermediate care.
Again, we asked managers whether staff providing specialised care needed extra
qualifications (Table III.39). More than half of IDPs (55%) and close to three quarters of
LADPs (71%) that responded said they did not. Where extra qualifications were required,
two respondents said staff would need NVQ level 3, two mentioned shared protocols with
NHS nurses, one mentioned a course on intermediate care provided by the local authority and
others mentioned additional training units such as PEG feeding, risk assessment and
palliative care.
Table III.39. The requirement for staff providing intermediate care to have extra
qualifications
% of IDPs
% of LADPs
% of all
No
54.5
71.4
58.6
Yes
45.5
28.6
41.4
Total responses
22
7
29
No response/not applicable
30
3
33
Managers were asked what training courses were offered to staff and whether they were
optional or compulsory. In each case they were asked whether specific courses were optional
or compulsory and then to identify any other courses which were offered. Table III.40 shows
the results for compulsory courses with the corresponding results for optional courses in
brackets. Firstly, it will be noted that the percentages for „compulsory‟ and „optional‟ total
more than 100 in some cases. This is because some respondents indicated that some courses
were compulsory for some staff and optional for others (e.g. training in „Use of Equipment‟,
which may depend on the needs of the service users that the individual cares for, or the „NVQ
level 2‟ course which may be compulsory for new staff but not for longer serving staff).
Secondly, we know there are some courses which are mandatory for all staff („Health and
Safety‟, „Service User Handling‟ and „Infection Control‟), but the responses for „compulsory‟
for these courses in some cases amount to less than 100%. We assume this is an oversight.
The first five specifically-mentioned courses were offered by all, or at least 90% of
employers, with similar results across the three sectors. Of the other specifically named
courses, „First Aid‟, „Medication Management‟ and „Parkinson‟s Care‟ were more likely to
be compulsory in IDPs than homes, possibly reflecting the fact that those care homes with
nursing would have a trained nurse on duty at all times. NVQ2 was said to be compulsory in
82% of homes, 84% of IDPs and 89% of LADPs. Eighty three respondents mentioned other
compulsory courses. The most frequently mentioned were those related to „Protection of
EWERC
Part III. The provider telephone survey
183
Vulnerable Adults‟ and „Safeguarding‟ (16 homes, 11 IDPs and 3 LADPs), followed by „Fire
Safety‟ (13 homes). Other courses mentioned related to specific conditions or specialised
types of care which some staff may have to undertake, or courses undertaken to comply with
the Skills for Care Common induction standards.
One provider mentioned that more courses were becoming compulsory as the needs of
service users changed:
All staff are now being trained in dementia care as there are many more referrals of those with
dementia and numbers are increasing. (IL.D.2.DL).
Table III.40. Compulsory and optional courses offered (optional courses in brackets)
% of homes
% of IDPs
% of LADPs
% of all
Health and Safety
92.0 (12.0)
97.9 (0.0)
100.0 (0.0)
95.3 (6.5)
Food hygiene
92.0 (14.0)
93.8 (12.5)
88.9 (22.2)
92.5 (14.0)
Service user handling
98.0 (4.0)
100.0 (2.1)
100.0 (0.0)
99.1 (2.8)
Use of equipment
94.0 (6.0)
95.8 (12.5)
88.9 (0.0)
94.4 (8.4)
Infection control
94.0 (8.0)
91.7 (12.5)
100.0 (0.0)
93.5 (9.3)
First aid
72.0 (32.0)
91.7 (8.3)
44.4 (55.6)
78.5 (23.4)
Medication management
52.0 (38.0)
95.8 (10.4)
100.0 (0.0)
75.7 (22.4)
Dementia care
52.0 (48.0)
43.8 (56.3)
44.4 (55.6)
47.7 (52.3)
Diabetes care
16.0 (74.0)
14.6 (75.0)
11.1 (88.9)
15.0 (75.7)
Loss and depression in elders,bereavement
20.0 (72.0)
16.7 (70.8)
11.1 (77.8)
17.8 (72.0)
Parkinson‟s care
4.0 (80.0)
18.8 (72.9)
11.1 (88.9)
11.2 (77.6)
NVQ 2
82.0 (24.0)
83.3 (25.0)
88.9 (0.0)
83.2 (22.4)
When asked which specific courses were optional the pattern of responses reflected the
responses to the question on which courses were compulsory. A wide range of other courses
were mentioned as being optional, including NVQ3 and NVQ4. One respondent said the
courses on offer were too numerous to mention. Optional courses were said to be especially
valuable as staff had specifically requested to do them:
There is lots and lots of training apart from induction. They are sent a questionnaire asking what
they want and there are lists on the training board and they can sign up. It is very fruitful if they
specifically ask for training. They get a lot out of it. (LK.D.6.CL).
Figure III.31 shows that the shares of providers having attained the Investors in People
award, or working towards it, were similar for homes and IDPs, but were only around a third
for all providers. In contrast, the majority (83%) of LADPs had attained the award.
EWERC
Part III. The provider telephone survey
184
Figure III.31. Achievement of the Investors in People Award
100
Homes
90
IDPs
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Yes, or working towards
No
Note: Total responses:45 (homes), 47 (IDPs) and 6 (LADPs). Missing responses: 8 (homes), 5 (IDPs), 4
(LADPs).
III.5.3. Appraisal and staff development
Staff appraisal systems seem to be widely established in independent as well as LA providers
with only one home and one IDP saying they did not carry out appraisals. Most carried out
appraisals annually, with one even saying once every 18 months; a slightly higher percentage
of IDPs (27%) than homes (21%) carried out appraisals more frequently than annually (table
III.43). In over half of cases appraisals were carried out by the manager alone in both homes
(58%) and IDPs (51%) and were involved in the appraisals in over three quarters of homes
(79%) and 59% of IDPs. This close involvement by the manager is reflective of the relatively
small size of the establishments. The higher share of „other‟ staff carrying out appraisals in
IDPs at 41% reflected the more widespread use of care coordinators or team leaders and
supervisors in domiciliary care to manage a more dispersed and indeed often larger
workforce. To probe further on approaches to staff development, we asked how training
needs were identified, first whether they were assessed by appraisal and second if they were
identified by employee request. A sizeable minority answered no to both (14% of homes and
23% of IDPs) and a further 10% of homes only identified needs through employee request.
Overall over three quarters identified needs through the appraisals system, with 56% of those
homes and IDPs using appraisal also using employee requests as a means of identification.
EWERC
Part III. The provider telephone survey
185
Table III.41. Staff appraisal arrangements
a. Frequency of appraisals
% of homes
% of IDPs
% of LADPs
No appraisal or only casual
1.9
1.9
0.0
% of all
Regular but less frequently than annual
0.0
1.9
0.0
0.9
Yearly
77.4
69.2
55.6
71.9
Six months to one year
7.5
5.8
22.2
7.9
3 to 6 months
3.8
17.3
22.2
11.4
More frequently than 3 months
9.4
3.8
0.0
6.1
Total responses
53
52
9
114
No response
0
0
1
1
% of homes
% of IDPs
% of LADPs
% of all
Manager
57.7
51.0
33.3
52.7
Other
23.1
41.2
66.7
34.8
Manager and Other
19.2
7.8
0.0
12.5
Total responses
52
51
9
112
No response
1
1
1
3
% of homes
13.5
% of IDPs
23.1
% of LADPs
10.0
% of all
17.5
Employee request
9.6
0.0
0.0
4.4
Appraisal alone or appraisal plus
employee request
76.9
76.9
90.0
78.1
Total responses
52
52
10
114
No response
1
0
0
1
b. Who carries out appraisals
c. Identification of training needs
Neither
EWERC
Part III. The provider telephone survey
186
III.6. Performance management, job autonomy and employee
voice
Important issues for recruitment and retention are how staff are managed within the
workplace; how performance is managed, the autonomy and discretion offered to employees
and opportunities for employee voice and communication. We consider the telephone survey
data corresponding to these issues in this section
III.6.1. Performance management
The most common practices used for performance monitoring were through the medium of
supervisors in all three types of providers - homes (81%), IDPs (85%) and LADPs (70%). For
IDPs and LADPs we also asked if there was any direct observation of staff and 69% of IDPs
and 80% of LADPs said they did undertake direct observation (figure III.32). We also asked
those involved in domiciliary care whether they used electronic monitoring and 31% said it
was currently in use; however we know from the interview data with LAs that this share is set
to rise. User surveys by providers were used to monitor performance in 29% of homes, 47%
of IDPs and 30% of LADPs. User surveys by the local authority were used by half of LADPs,
but only 6% of homes and 22% of IDPs. However, 74% of homes, 55% of IDPs and 40% of
LADPs said they used other methods to monitor performance. These included investigations
of monitoring, CQC inspections, appraisals and spot checks.
Figure III.32. Types of staff monitoring
a. Homes
100
Percentage of providers
90
80
70
60
50
40
30
20
10
0
No
Yes
Supervisors?
EWERC
No
Yes
User surveys by care
provider?
No
Yes
User surveys by LA?
No
Yes
Other methods?
Part III. The provider telephone survey
187
b. IDPs
100
IDPs
90
LADPs
80
Percentage
70
60
50
40
30
20
10
0
No
Yes
Electronic
monitoring?
No
Yes
Supervisors?
No
Yes
Observation?
No
Yes
User surveys by
care provider?
No
Yes
User surveys by
LA?
No
Yes
Other methods?
Note: Total responses for different questions: 53, 49, 48, 50 (homes); 51, 52, 51, 51, 51, 51 (IDPs) and 10 for all
questions (LADPs).
For some managers electronic monitoring was used solely because of contractual
commitments and they were concerned about the impact on both staff and their own revenues
of moving to paying by the minute or even five minute blocks:
Instead of paying per care call they are only now going to pay per minute. So we are actually
moving now to paying people in five minute pay bands rather then per minute because I think
it‟s a bit childish. So if they do 26 minutes they‟ll get paid 30. So it will be rounded up. But
also if they spend 90% of the scheduled time in a service user‟s home we will also pay the
travel time. So that‟s an incentive for them to keep our income levels high, because the less
they do the less we get and it soon spirals out of existence. (ON.D.1 DN).
Table III.42. Managers’ perceptions of the most effective method for dealing with
performance monitoring
% of homes
% of IDPs
% of LADPs
% of all
Disciplinary only
6.7
12.2
11.1
9.7
„Soft‟ measures plus disciplinary
8.9
28.6
33.3
20.4
Training and „soft‟ measures only
84.4
59.2
55.6
69.9
Total responses
45
49
9
103
No response
8
3
1
12
However, one IDP commented on how it had enabled them to tighten their control of the care
workforce:
Now [performance problems] it is people running late or leaving early before the full amount
of the call. ….We have investigated, and it is usually people arriving late for their first call
EWERC
Part III. The provider telephone survey
188
and then never catching up. They leave early – maybe 15 or 10 minutes early and tell us it is
because the client told them to leave early. We now have a system that they have to call into
the office if the client tells them to leave early. If it‟s someone with dementia we follow this
up; it may be the same person always reporting that their clients tell them to go. Call
monitoring has helped us analyse these issues. (IL.D.1).
Most providers preferred to use „soft‟ measures such as training, one to ones, supporting
staff, changing schedules etc. to deal with poor performance (over 80% of homes, almost
60% of IDPs and over 55% of IDPs), rather than disciplinary procedures (Table III.42).
We also asked what were the most common problems of poor performance (table III.43). The
most frequently mentioned were absenteeism and sickness (18% of homes, 37% of IDPs and
10% of LADPs), timekeeping (8% of homes, 40% of IDPs), and skimping on time spent with
service users (8% of homes, 27% of IDPs and 10% of LADPs). These findings reflect the
nature of work in domiciliary care, where staff usually work unsupervised. Other problems
mentioned were complaints from service users, not following correct procedures, lack of
skills and training, personal or family problems affecting work, poor team working and
language skills.
Table III.43. Managers’ views on the most common problems of poor performance
% of Homes
% of IDPs
% of LADPs
% of all
Absenteeism, sickness
18.0
36.5
10.0
25.9
Timekeeping
8.0
40.4
0.0
22.3
Skimping on time or services provided
8.0
26.9
10.0
17.0
Poor attitude, motivation
20.0
7.7
10.0
13.4
Complaints from service users
0.0
13.5
30.0
8.9
Not following correct procedures
14.0
0.0
20.0
8.0
Lack of skills, training
4.0
5.8
10.0
5.4
Personal or family problems
8.0
0.0
0.0
3.6
Poor teamworking
6.0
0.0
0.0
2.7
Poor language skills
4.0
0.0
0.0
1.8
No problems
12.0
3.9
10.0
8.0
Total responses
50
52
10
112
No response
3
0
0
3
Note: Multiple responses possible.
In their additional comments on the nature of performance problems we encountered a range
of responses, with some attributing the main problems to gaps in training or understanding of
procedures while others felt the problems lay mainly with attitudes:
It‟s about practice issues not using the right techniques with moving and handling and not
following procedure. (HD.HN.1.C.LV).
EWERC
Part III. The provider telephone survey
189
Not understanding professional boundaries, it‟s never meant, it‟s never malicious but most of
the problems that we do encounter tend to be around staff overstepping boundaries.
(OM.D.2.DN).
Another talked about the difficulties of disentangling poor performance from problems of
meeting users‟ expectations:
I think it‟s a bit of both at this moment in time. We have staff going in with guidelines, service
users wanting over and above and we do have a bit of racism and the others are staff not
getting to their shifts on time. (RD.D.1.C.S.).
To link issues of performance management directly back to issues of recruitment and
retention we asked whether providers felt obliged to put up with poor performance because of
problems of staff shortage (figure III.33). As might be anticipated, most said they did not put
up with poor performance (70% of homes, 57% of IDPs and 70% of LADPs) - as to do so
would reflect negatively on their organisation. However, the remaining 30% of homes, 43%
of IDPs and 30% of LADPs admitted that they were forced to put up with poor performance,
at least sometimes.
Figure III.33. Share of providers who said that recruitment difficulties sometimes
forced them to put up with problems of poor performance
100
Homes
90
IDPs
LADPs
80
Percentage
70
60
50
40
30
20
10
0
no
yes
Note: Total responses: 53 (homes), 51 (IDPs) and 10 (LADPs). Missing responses: 1 (IDPs).
Absenteeism featured as a particular concern. The majority of providers (94% of homes, 84%
of IDPs and all LADPs) said they collected figures on absenteeism (Table III.44). Some of
EWERC
Part III. The provider telephone survey
190
the national providers had specific regulations and procedures that were used to manage
absenteeism:
The company does it on a regional basis. After 4 periods of absenteeism, then staff go through
disciplinary proceedings. (IL.D.1 CN).
More than one quarter of organisations surveyed believed rates of absenteeism were quite
high or very high (figure III.34). The evidence suggests the problem is particularly acute in
IDPs (35%), compared to just over 15% of homes. More surprising, however, is the very high
share of LADPs who report high absenteeism – 70% - but this may be related in part to more
generous sick leave provision in the public sector.
Table III.44. The collection of figures on absenteeism
% of Homes
% of IDPs
% of LADPs
% of all
Yes
94.0
83.7
100.0
89.7
No
6.0
16.3
0.0
10.3
Total responses
50
49
8
107
No response
3
3
2
8
Figure III.34. Managers’ views about rates of absenteeism among care staff
60
Homes
IDPs
LADPs
50
Percentage
40
30
20
10
0
Very high
Quite high
Acceptable
Quite low
Very low
Note: Total responses: 53 (homes), 51 (IDPs) and 10 (LADPs). Missing responses: 1 (IDPs); Question asked
was, „What do managers consider rates of staff absenteeism to be?‟ (Q173).
The differences in views as to whether the level of absence was too high, low or acceptable
may reflect different perceptions and attitudes as well as different levels; respondents were
asked to tell us how they measured absenteeism and to give us the data but the methods used
were too variable to report here. One IDP was particularly adamant that absenteeism would
not be tolerated:
EWERC
Part III. The provider telephone survey
191
I don‟t tolerate it. I have had one or two people who are always having sickies. It goes into
their files and I get a pattern. They forget what reasons they have given, and how many days
they have had off, but we write it down. My deputy has had one day off in 20 years, I have had
one week off in 19 years. (TE.H.3 AS).
Others saw absenteeism as a problem related to the age of the workforce and the nature of the
job – including the impact of problems in relationships with users.
Where it is sickness, we have a system of letters and dates that are trigger points. I speak to
them one to one and then it goes to HR. They have not helped much so far. But workers are
old, and they are tired and prone to infection. (AH.D.3.CN).
Absenteeism; [its] low confidence; personal chemistry. (TE.H.2 BS).
Yet others stressed the problems of managing sickness for a dispersed workforce:
Three field care supervisors actually spend time with the staff and we‟ve tried return to work
interviews, but … somebody that works four miles away from here that doesn‟t have a car
finds it very difficult to come in to the office for a half hour to be told that they shouldn‟t be
having sick but, you know, „I‟ve had gastroenteritis‟, what can I do?‟(ON.D.1 DN).
To assess the approach to managing performance we asked about what methods they had
found most effective in managing poor performance. We have recoded those responses into
three categories: those that mentioned disciplinary methods only; those that mentioned softer
measures such as training alongside disciplinary measures and those that only mentioned
softer measures such as training, one to ones, supporting staff, changing schedules and so on.
The vast majority of homes (84%) mentioned only soft measures. IDPs were more varied
with around three fifths only mentioning soft measures but 28% mentioned disciplinary
measures alongside soft measures (with LADPs showing a similar pattern). Only a minority 12% – mentioned only disciplinary approaches.
III.6.2. Discretion and autonomy
Opportunities to exercise discretion and autonomy at work have the capacity both to
contribute both to the quality of the jobs and to the quality of the care provided. However, the
granting of discretion may provide challenges for management, particularly in a context of
tightly specified commissioning. To probe these issues we asked a series of questions related
to both time constraints on tasks and autonomy in tasks. As the work environment is quite
different between domiciliary and care homes we discuss the results in turn (table III.45).
Although all IDPs said that client visits were tightly defined, a majority still expressed the
view that staff did have time to carry out their work to a high standard with 79% saying yes
and a further 17% agreeing that this applied to some extent. In practice only two IDPs said
this was not the case. LADPs were, in fact, less positive with only 60% saying yes, 30%
stating to some extent and 10% - that is, one provider- saying no. There was more recognition
of time constraints on a specific dimension of care, that is developing good relationships with
clients; again although the majority were positive, 15% of IDPs said they were not able to do
EWERC
Part III. The provider telephone survey
192
this and a further 17% only to some extent. For LADPs the shares were quite similar at 10%
and 20% respectively. This aspect of care may be regarded as more voluntary by some
providers but one provider emphasised its importance:
Because they may be the only person that they have seen all day or all week. People are elderly,
lonely, don‟t have any other social contact. They see this as a part of social contact so we do
encourage it. (ON.D.1 DN).
Table III.45. Types of opportunities for staff to improve their performance
% of homes
% of IDPs
% of LADPs
% of all
Yes
90.4
78.8
60.0
82.5
To some extent
9.6
17.3
30.0
14.9
No
0.0
3.9
10.0
2.6
Having the opportunity to put into Yes
practice the training qualifications To some extent
they have gained?
No
94.3
100.0
90.0
96.5
5.7
0.0
10.0
3.5
0.0
0.0
0.0
0.0
Being free to prioritise and carry
out tasks in ways to improve the
quality of care?
Yes
73.6
40.4
60.0
57.4
To some extent
26.4
44.2
40.0
35.7
No
0.0
15.4
0.0
6.9
Having the opportunity to develop Yes
good relationships with service
To some extent
users?
No
94.3
67.3
70.0
80.0
5.7
17.3
20.0
12.2
0.0
15.4
10.0
7.8
Being encouraged to exchange
ideas with other carers of new
ways of working/best practice?
Yes
90.6
84.6
100.0
88.7
To some extent
9.4
11.5
0.0
9.6
No
0.0
3.9
0.0
1.7
53
52
10
0
Having enough time to carry out
the work to a high standard?
Total responses
Both IDPs and LADPs were universally positive about opportunities to put training into
practice within the care work environment with none answering negatively and only one
LADP answering to some extent. An almost similar positive response was found for
opportunities for care workers to pass on ideas to others to improve care. There was more
doubt, however, about whether care staff were free to prioritise and carry out tasks in ways to
improve care; only 40% of IDPs agreed and a further 44% said to some extent with 15%
saying no. None of the LADPs said no and three fifths said yes and two fifths to some extent.
Thus there was some recognition of constraints on the autonomy of care staff to determine
priorities or change ways of carrying out tasks.
The same questions were posed to the home managers. The responses from homes were even
more positive than for the IDPs. There were in fact no negative answers to any of the
questions and the share saying to some extent rather than simply yes fell below 10% in all
cases, except for the question about freedom to prioritise and carry out tasks in ways to
improve the quality of care. Even here almost three quarters of homes said yes (74%) and
EWERC
Part III. The provider telephone survey
193
over a quarter to some extent, with the yes response well above the share of IDPs answering
yes (40%). This apparent lower degree of discretion for domiciliary care applies in a context
where most domiciliary care workers operate unsupervised while care workers in homes are
often working in teams. In a fixed workplace with senior staff always on duty, care home
managers may feel it less necessary to specify priorities and ways of working than in the
unsupervised domiciliary care context.
III.6.3. Employee voice and communication
In contrast to local authorities, most independent sector providers do not recognise trade
unions or follow collective bargaining (figure III.35). In our sample only 15% of homes and
8% of IDPs recognised trade unions. However, voluntary sector providers were more likely
than for-profit providers to recognise unions – 24% and 9%, respectively. But in general,
outside the public sector, opportunities for employee voice depended more on management
initiatives than formal provision for voice.
All the providers in the sample held at least annual staff meetings and over 90% held them at
least quarterly (table III.46). Homes were more likely than IDPs to hold meetings every
month or more frequently. The reason for this was undoubtedly the greater difficulty of
arranging staff meetings for domiciliary care staff who work in the community rather than in
a fixed location but on the other hand the need for staff meetings may be consider greater in
IDPs.
Figure III.35. Union recognition and use of staff attitude surveys
100
Homes
90
IDPs
LADPs
80
Percentage
70
60
50
40
30
20
10
0
Recognise a trade union
Carry out staff attitude surveys
Note: Total responses to the two questions: 53 and 52 (homes); 51 and 52 (IDPs); 9 and 9 (LADPs).
Perhaps reflective of the greater difficulties of direct communication IDPs were more likely
than homes to carry out staff attitude surveys - 83% compared to 58% (figure III.35). Some
EWERC
Part III. The provider telephone survey
194
comments made by interviewees for the telephone survey indicate, however, that these
surveys did not always generate a high response rate.
Yes, but the one I did, no-one filled it in and returned it to me. (IL.H.2).
[Company X] do [undertake a staff survey] after you have been on contract for 9 months. I
am not involved and have no idea of the result. I think that not many responded.
(AH.D.3.CN).
Table III.46. Frequency of staff meetings
% of Homes
% of IDPs
% of LADPs
% of all
Between every three months and yearly
10.0
9.6
0.0
8.9
Between one and three months
44.0
63.5
40.0
52.7
Every month or more
46.0
26.9
60.0
38.4
Total responses
50
52
10
112
No response
3
0
0
3
EWERC
Part III. The provider telephone survey
195
III.7. Summary
In this part of the report we presented a general mapping of the HR practices and employment
conditions in the social care sector, paying special attention to the similarities and differences
between our two main categories of care providers – residential and nursing care homes
(referred to as homes) and independent sector domiciliary care providers (referred to as IDPs)
– as well as a third category of local authority domiciliary care providers (referred to as
LADPs). The results draw on the combined quantitative and qualitative data from our
telephone survey. In exploring the types of HR practices deployed across the sector, the
variety of practices between IDPs, homes and LADPs and the patterns of employment
conditions, this part of the report has set out the descriptive statistics required for the
subsequent more detailed statistical analysis presented in part IV. Therefore, before turning to
the next stage of our interrogation we summarise the key results from this preliminary
mapping exercise.
The six sections of this part of the report were organised around key areas of HR policy and
practice. Beginning with the key area of recruitment practices, the survey evidence
underlined the problems facing all care providers with one in three reporting difficulties
recruiting care workers. IDPs were more likely than homes to report difficulties but were also
more likely to have witnessed an easing of problems during the recession, suggesting that the
gap in experience has narrowed in the last couple of years. Respondents to our survey,
especially from IDPs, believed the most important reason they faced difficulties was the low
level of pay. And the need to fill weekend and unsocial hours shifts was a real challenge for
all providers, but again especially for IDPs, 70% of which recorded shortages in this area.
As anticipated, section III.1 found that care providers use a range of formal and informal
recruitment methods, although homes were more likely than IDPs and LADPs to prefer
informal methods over formal methods. In the selection process, again the data point to a
wide range of practices, with evidence that IDPs were more likely than homes to utilise
aptitude tests and pre-screening telephone interviews. Perhaps surprisingly – although again
this may reflect the recessionary conditions at the time of data collection – providers were
unlikely to use external agencies to fill vacancies. Nevertheless, 17% of homes and 10% of
IDPs had recruited from overseas directly.
While providers sought a wide range of attributes among job applicants, the most common,
reported by nine in ten providers, was a positive and friendly attitude towards care work; this
was said to be the single most important attribute by three in four homes and over half of
IDPs. Availability for weekend work, as well as early and evening shifts, was also required
by a majority of providers, with strong similarity among homes and IDPs. There was a
notable difference of views among public and private sector provider managers such that
LADP managers placed more emphasis on skills associated with care than did providers in
the independent sector. While providers have a clear notion of what they required in a recruit,
a significant proportion – some four in ten – reported occasionally or often having to hire
people (with full knowledge of what they were doing) who lack the full set of desired
EWERC
Part III. The provider telephone survey
196
attributes – a result that is all the more striking given the relatively loose labour market
conditions during 2008-2009. At the same time, a third of providers reported often or
occasionally rejecting candidates who were suitable for the advertised job. This result points
to the likelihood of differential local labour market effects in shaping HR practices, an
important issue that is interrogated in detail in part IV.4. A further external factor that
impinges upon recruitment practices is the need to apply for CRB checks; more than half our
sample of providers had lost one or more job applicants as a result of delays in CRB checks
and a third as a result of CRB failures.
The mapping of turnover and retention conditions in section III.2 showed that while a
majority of providers expressed satisfaction with levels of staff turnover, the data point to
high levels: the turnover of care workers averaged 24% for homes and 31% for IDPs. Homes
were better than IDPs at retaining new recruits but 22% of homes and 32% of IDPs had lost
more than half of their new recruits in the past year. Homes were less likely to report very
high levels of staff turnover; close to a third of IDPs reported turnover of care workers
excluding new recruits of more than 30%. Average rate of turnover, excluding new recruits,
were 22% for IDPs and 18% for homes. Reasons for worker quits are varied and again
differed among homes, IDPs and LADPs. The search for more convenient working hours was
a strong underlying factor at one third of IDPs and the search for better pay at close to one
quarter of both homes and IDPs – although this was not an issue at any of the LADPs in our
survey. Many care workers quit for career reasons, with one in four homes citing nurse
training, and a very common reason was family responsibilities, reported by more than a third
of providers.
The evidence on pay and rewards in section III.3 demonstrates the very low value assigned to
the work of adult care in the UK independent sector and especially so among for-profit
organisations. Homes pay lower minimum rates than IDPs with a third of homes in fact using
the statutory minimum wage, despite its role in the labour market as a floor to wages, not as a
going wage rate. Those paying above the statutory minimum do not pay significantly more –
seven in ten homes and one in three IDPs paid a minimum of less than £6.00 (just 27 pence
more than the national minimum wage). It is notable that no LADPs set such a low minimum
rate for care workers, a reflection of the stronger collective wage bargaining power of trade
union representing care workers in the public sector.
Our analysis of „normal‟ pay rates – the rate paid to most care workers in each organisation revealed very low levels and little variation across independent sector homes and IDPs with
the exception of voluntary sector homes where the average normal pay was relatively high.
At nine of the 52 homes surveyed the normal rate was in fact the same as the statutory
national minimum wage. This finding underlines a more general finding of limited
opportunity for pay progression in these organisations. In more than half of IDPs the
minimum rate paid to care workers is exactly the same as the normal rate. Even where
providers pay more for promotion to a senior care worker, the rate of pay is usually no more
than £1.00 higher. And these employers do little to encourage investment in skills; reward for
the NVQ level 2 qualification in care varied from as little as an additional 7 pence per hour to
EWERC
Part III. The provider telephone survey
197
£1.02 above the minimum rate of pay; indeed, 23 of the 25 providers that offered a higher
rate set an hourly rate at no more than 50 pence higher than the minimum. The results are a
disappointing reflection of the unwillingness and/or inability of these employers to reward
more complex work appropriately.
Regular uprating of pay was common but not universal. Factors influencing the decision to
uprate pay included changes in the statutory national minimum wage, especially among
homes which is directly related to their greater likelihood of setting minimum rates at the
minimum wage floor. Important influences on IDPs‟ uprating of pay, by contrast, included
the level of LA fees and the profitability of the organisation.
There were variable practices for paying travel time to domiciliary care workers. A small
share of IDPs and LADPs (less than one third) paid a supplement; most opted to reimburse
petrol or public transport costs; and a significant share claimed the compensation was
included in the hourly rates. By contrast, there appeared to be a near universal approach
towards paying care staff for time spent training; only around one in ten providers (all in the
independent sector) failed to compensate all training time. However, there is no standard
practice of paying a premium for overtime work. Most LADPs do follow this practice, but
only around a quarter of IDPs and homes. Finally, the data reveal a surprisingly high
incidence of independent sector providers that are unwilling to fund the upfront costs of
starting work, such as paying for CRB checks, uniforms and induction training.
Section III.4 examined HR practices of flexibility, working time and work organisation.
Among IDPs, there is a very strong flexibilisation of employment characterised by very
limited use of guaranteed hours (just one in ten IDPs), strong prioritisation given to user
needs in scheduling work and a near universal expectation that workers must tolerate longer
hours at short notice (occasionally or often). The data suggest providers use work scheduling
as a major form of control over the workforce; the near standard practice (nine in ten IDPs) of
offering zero hour contracts may in part explain the finding that nine in ten IDPs find it easy
or very easy to find staff willing to take extra hours at short notice. Some providers made it
clear that staff were expected to cooperate in variations to schedules if they hoped to be
allocated their desired number of hours in the future. By contrast, the practice of offering zero
hours contracts has been abandoned by public sector providers where nine in ten offer
guaranteed hours.
Behind the working time practices lies the organisation of work, scheduled around visits to
clients. The minimum duration of visits tended to be 15 minutes and the average length no
more than 30 minutes. Three in five IDPs failed to set any minimum working time and a
further fifth set a minimum time of less than two hours. The fragmentation of work into very
short blocks of time created further problems for staff because nine in ten IDPs did not pay
for breaks.
Among homes, care workers were more likely to work full-time than in IDPs and to be
offered guaranteed hours. Nevertheless, there was still a significant share of part-time
working in homes and fewer care workers worked very long hours than in IDPs. Overall, a
EWERC
Part III. The provider telephone survey
198
higher share of homes than IDPs claimed to be able to match employees‟ working time
preferences all of the time, suggestive of a somewhat weaker employer-led approach to
flexibility. A major issue in homes was matching staffing working hours with bed occupancy
with evidence of change occurring in lumps rather than incrementally as homes lost or gained
occupants.
Section III.5 found that most providers were strongly engaged in training provision,
including induction training and training to NVQ levels 2, as well as regular staff appraisals.
Even where staff required NVQ level 3 or 4 skills, three in four providers provided the
training inhouse rather than buy in external provision. There is nevertheless variation in
approach towards staff development. For example, the results suggest IDPs were more likely
than homes or LADPs to believe a newly recruited care worker ought to be competent in their
job within a week‟s induction training. Homes and LADPs were more likely to allow a period
of one to six months for induction. Similarly, attainment of NVQ level 2 qualifications was
higher in homes than in IDPs. More than half of homes and LADPs had more than 70% of
care workers qualified to level 2 compared to a third of IDPs. Also, nine in ten homes had
already met the now abolished national target of having at least half the staff trained to level
2 compared to just two thirds of IDPs. Two key factors explaining the failure to reach the
target were high staff turnover and training related problems such as funding.
The final section III.6 covered inter-related practices towards performance management, job
autonomy and employee voice. Use of appraisals was frequent throughout the sector and most
providers favoured soft over hard methods to improve performance, but poor performance,
including absenteeism, had at times to be tolerated in four out of ten IDPs. With regard to
monitoring, a third of IDPs use electronic monitoring and a significant share of both homes
and IDPs rely on user surveys conducted by both the LA and the care provider. Timekeeping
issues were also a cause of poor performance, again especially notable among IDPs.
The management approach towards encouraging workers to exercise discretion and autonomy
at work is covered in great detail in part V of this report. Here, we only reported the very
basic, descriptive data. Most providers were confident their care workers enjoyed the
opportunity to deliver high quality services, to develop good relations with users and
exchange ideas about good practice care delivery. However, a significant proportion
expressed doubt. For example, more than four in ten IDPs and one quarter of homes believed
workers were not fully able to prioritise and undertake tasks in ways to improve the quality of
care. Also around a fifth of IDPs and LADPs recognised that workers were not fully able to
take the time needed to develop better relationships with service users.
Finally, the survey results confirmed expectations that in the independent care sector the
employment relationship is highly individualised; our survey data suggest only 15% of homes
and 8% of IDPs recognised collective representation through a trade union, albeit with
slightly higher figures among not-for-profit voluntary sector providers. In its place, providers
held staff meetings, with most organising such meetings every one to three months.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
199
IV. The Impact of Organisational,
Commissioning and Labour Market Factors on
HR Practices and Outcomes
This part of the report brings together the various factors identified in the research framework
for the project that could be expected to impact upon the recruitment and retention of the
social care workforce. Following the mapping of HR practices and HR outcomes in Part III,
the analysis here uses statistical methods to interrogate the patterns in more detail. The main
data source used in this part is again the telephone survey of providers but we also
supplement this establishment-based survey with information from interviews with HR
directors or equivalent at the headquarters of ten national chains of providers.
There are six sections to this part of the report, organised as follows:
Section IV.1 presents the organisational characteristics of the sample of providers - by
size, ownership and quality star rating - and identifies the management capacities and
support structures within the independent sector;
Section IV.2 identifies the HR practices adopted by type of provider and creates an
index of „good‟ HR practices by which to compare the range of poor to good HR
practices, including for separate HR practices and for a summary measure;
Section IV.3 uses these indices together with detailed wage data for the providers in
the sample to explore the linkages between LA commissioning practices and good HR
practices and outcomes;
Section IV.4 undertakes a similar exercise in relation to local labour market factors
and explores the association between local pay levels and other measures of local
labour market demand with the likelihood of providers adopting good HR practices
and enjoying good HR outcomes;
Section IV.5 interrogates these divergent influences on HR practices and HR
outcomes through multivariate statistical analysis and considers the relationships for
IDPs and homes between organisational characteristics, LA commissioning practices,
local labour market factors, good HR practices and good HR outcomes;
Section IV.6 explores providers‟ views on the social care policy and commissioning
environment drawing on both the telephone survey and the survey of national
providers at headquarters.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
200
IV.1. Organisational characteristics and the management of
independent sector providers
A key issue for the recruitment and retention of the social care workforce is the capacity of
the independent sector to recruit, retain and manage a skilled and committed workforce, now
that the local authorities have, for the most part, outsourced the majority of service delivery.
The capacities of the independent sector will depend upon their organisational and
management characteristics and their business strategy and position. We thus start this
chapter by identifying the key organisational and market characteristics of our sample of
independent providers and also introduce into the analysis the national chains that we have
interviewed at national level (section IV.1.1). In section IV.1.2 we explore the organisation of
the HR function and associated issues such as approaches to performance management within
our telephone survey of establishments and our survey of ten national companies.
IV.1.1. Organisational characteristics
Table IV.1 shows the key organisational and market characteristics of the telephone survey
sample of 115 providers. The sample of 105 independent providers was relatively evenly split
between homes and IDPs, with 53 and 52 respectively, complemented by interviews with 10
LADPs. Among the 53 homes 56% were offering only residential care and 43% were
offering nursing care.
Size of establishment is often regarded as a characteristic with significant implications for the
management of HR. These implications may be both positively and negatively related to size
with the smaller workplaces more able to manage through informal and „friendly‟ work
relations, which may have positive benefits for retention. Larger establishments may be in a
better position to professionalise HR and possibly to make step changes in volume or quality
of service delivery. However, size of organisation may also matter, with small establishments
as part of larger organisations able to rely on regional or headquarter assistance to
professionalise. As the target sample was specified at local level, it was not possible to
include type of organisation as a specific characteristic - particularly in view of the problems
of securing access discussed in part I (section I.7). However, the sample was reviewed as a
rolling total and, as table IV.1 reveals, it covers a wide range of both size of establishment
and type of organisation. The most frequent size category for homes was 25 to 49 staff while
for IDPs it was somewhat larger, at 50 to 99.
IDPs were also more likely to be part of a chain, particularly national chains (as opposed to
local chains, which are defined as having more than one establishment, but usually less than
ten, situated in one, or in neighbouring local authority areas). Nearly half the sample of
establishments were in fact part of national organisations; this fits with evidence from LAs
and from UKHCA that there has been a marked increase in the role of national organisations,
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
201
particularly in domiciliary care. However, most of the national providers included in the
sample here have been in operation for at least two years and generally longer. Overall only
three IDPs were newly established.
Table IV.1. Organisational characteristics of the telephone survey providers
Size
Chain (local or national) or
single agency
Is it a private, public or
voluntary organisation?
Star rating
Homes
IDPs
LADPs
Total
Total sample size
53
52
10
115
Very small 0-24
15
5
0
20
Small 25-49
24
9
0
33
Medium 50-99
12
24
0
36
Large 100+
2
14
10
26
chain - local
14
10
0
24
chain - national
19
31
0
50
single home/agency
Private
20
11
10
41
42
46
0
88
Public
0
0
10
10
Voluntary
11
6
0
17
1 Star
9
5
0
14
2 Star
31
37
4
72
3 Star
13
10
6
29
How many local authorities
engaged with
1 council only
28
32
10
70
More than 1
25
20
0
45
What proportion of your
service users are local
authority funded
0-25%
13
1
0
14
26-50%
8
3
0
11
More than 50%
Yes
32
48
10
90
25
34
6
65
No
28
18
1
47
3
3
Are any, of your service users
are partly or wholly funded by
the PCT?
What % of beds are currently
vacant?
Missing
0%
13
1-10%
29
More than 10%
What proportion of hours are
done under block and spot
contracts
Missing
< 2 years
Spot only
Mainly spot (>50%)
Mainly Block (50% &
>)
Block only
How long has the
Home/IDP/LADP been
operating?
Do you belong to an
Employers‟ Association?
EWERC
11
Not asked of
homes
Not asked of
homes
Not asked of
homes
Not asked of
homes
Not asked of
homes
Not asked of
IDPs
Not asked of
IDPs
Not asked of
IDPs
Not asked of
IDPs
Not asked of
IDPs
Not asked of
IDPs
25
3
28
3
0
3
12
0
12
5
7
12
7
0
7
0
3
13
29
11
0
3
> 2 < 5 years
8
14
0
22
>5 years
Yes
45
25
35
23
10
2
90
50
No
12
18
5
35
Missing/don‟t know
16
11
3
30
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
202
The majority of homes and IDPs were private, for profit organisations, but Table IV.1 shows
that 21% of homes and 12% of IDPs were run on a voluntary, not-for-profit basis. Less than
half the organisations - 50 out of 115 - definitely belonged to an employers‟ association and
35 said they did not but there was a high share of managers who were not able to answer (30
out of 115). Table IV.1 also gives data on the sample by star rating awarded by CQC. The
most popular category is 2* with 72% of the 115, but 14% are 1* providers and 29% are 3*.
To explore the role of national organisations further, we decided to undertake a separate
survey of 10 national organisations at headquarters level; table IV.2 provides the details of
their organisational characteristics. These also showed a range of different size characteristics
with the number of homes in ownership varying from 40 to over 700 and the number of
branches of IDPs varying from 15 to over 60 (or around 150 if franchised branches for one
national chain are included). All but the smallest of the domiciliary chains operated with a
regional as well as a national structure.
The importance of LAs in shaping the markets for the independent sector is confirmed by the
information for the sample, particularly for domiciliary care where all but four IDPs relied on
LAs for more than 50% of their business. The picture was more mixed for homes where 21
recorded sources other than LAs as accounting for more than 50% of their business and 13 of
these said that LAs accounted for less than a quarter of their activity. The likelihood of
relying primarily on private funding was much higher in some parts of the country than
others. As one home manager commented in a southern location in respect of her owner‟s
policy:
They are unusual in the area as they take local authority people – most don‟t because of the
money. (LK.H.2 AS (V)).
Responses to the question at the end of the telephone survey on levels of fees charged
revealed quite wide differences among some providers between the fees charged to private
clients and those received from the LA especially for homes in all the southern LAs (see
section IV.3.1 for further details).
Concerns over dependence on LAs were expressed by some of the national providers, both
in relation to the low fees paid by LAs and in relation to the likelihood of reduced business
from LAs in the future due to budget constraints. One national provider of homes shared a
presentation on their business plan where it was clearly stated that in the south they were
mainly concentrated on servicing private clients and it was only in the north where their focus
was on relationships with LAs.
EWERC
Part IV. The impact of organisational, commissioning and labour market factors on HR practices and outcomes
203
Table IV.2. Characteristics of national providers
a. Domiciliary care providers
NATDOM1
NATDOM2
NATDOM3
NATDOM4
NATDOM5
Size
Large
Large
Large
Large
Small
National/local terms and
conditions
Local.
Local.
Local.
Local.
Local.
National/local training
and induction
Standard induction.
Standard induction.
Standard induction
Standard induction
Standard induction.
Training company and
local.
Training company- based.
Training companybased
Training company-based
Training company
and local
National recruitment
policies and procedures.
National recruitment
policies and procedures.
National recruitment
policies and procedures.
National recruitment policies
and procedures.
National recruitment
policies and
procedures
Regional structure
Regional structure
Regional structure
Regional structure
Bonus scheme for
managers. Traffic light
system based on quality,
financial and HR targets
For company branch
managers, based on the
contribution of the branch
to the centre
Performance bonus for
managers based on
KPIs (HR and business
targets)
Bonus scheme for managers
based on achieved targets
(KPIs red-amber-green).
Currently emphasis on R&R.
Centralised/decentralised
Performance
targets/bonuses
EWERC
Bonus system for
managers. Targets
on quality, business
Part IV. The impact of organisational, commissioning and labour market factors on HR practices and outcomes
204
b. Care homes
NATHOME1
NATHOME2
NATHOME3
NATHOME4
NATHOME5
Size
Large
Large
Small
Very large
Medium
National/local terms and
conditions
Local.
Local.
National salary scale,
local determination of
position.
National pay rates for
care staff negotiated
with GMB.
Local but aiming to
standardize by region.
National/local training
and induction
Company based with
regional support.
Standard induction.
Training company and
local.
Training company and
area based.
Company and local
based.
Standard induction.
Training company and
local.
Centralised/decentralised
National recruitment policies
and procedures.
National recruitment
policies and
procedures.
National recruitment
policies and procedures.
National recruitment
policies and procedures.
National recruitment
policies and procedures.
Area structure
Regional and area
structure
Regional structure
Regional structure
Regional structure
Performance
targets/bonuses
30%bonus scheme for
managers based on targets set
by themselves – main ones
are marketing, occupancy
and care delivery.
Bonus scope for
managers of 25% based
on financial
performance and
quality.
Quarterly and year-end
bonus scheme for
managers. KPIs for care
and financial
performance.
Bonus for managers
based on financial
performance and
quality (including HR).
Annual bonus for managers
based on Balanced
Scorecard approach (incl.
ability, people management,
finance).
Role of LAs v private
clients
60% of business from LAs
and PCTs. South dominated
by private fee payers but
north more mixed.
Decreasing number of
public funded referrals.
Fee freezes and
reductions from LAs.
90% of business from
LAs and PCTs.
80% of business from
LAs and PCTs.
Pressure on fees.
Looking to grow
private side.
80% of business from LAs
and PCTs. Both under
economic pressure.
Anticipates less business
coming from them.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
205
Sixty of the 105 independent providers dealt with only one LA but 45 were engaged in working
for more than one local authority; for homes this was unsurprising as many placements are
made out of area but nearly 40% of the IDPs also worked for more than one LA. In addition
well over half of the sample did at least some work for the NHS through Primary Care Trusts.
The contract arrangements for the IDPs varied with 28 working on an only or mainly spot basis
and 17 on a mainly or only block basis (7 missing answers). A further indicator for homes of
the state of the market is the number of bed vacancies; here we found a wide range of situations
with 13 recording no vacancies, 29 had vacancies of up to 10% but 11 had vacancies in excess
of 10%.
Box IV.1. National providers’ comments on private versus LA funded clients
The south [of England] seems to be very private fee funding driven, whereas the north is sadly
more blurred and Scotland is a different funding altogether. Recruitment Director, NATHOME1
One of the challenges for us is that a huge proportion of orders come from local authorities and
PCTs. So nearly 80% of our business is from local authorities and PCTs and only 20% from
private paid. So when you look at challenges, I mean, at the moment the sort of fees that one gets
from local authorities and PCTs are significantly lower than the fees that you can charge to
private individuals and, obviously, in the present financial climate, one of the big concerns is
that‟s going to come under even more pressure if those PCTs and local authorities are challenged
in terms of their own budget. Group HR Director, NATHOME 4
I suppose the key business challenge really arises from the state of finances of the country as a
whole. We are certainly noticing fewer public funded referrals. Corporate Services Director,
NATHOME2
IV.1.2. Management in the independent sector
As most IDPs and homes are small at the establishment level, a key issue for the development
of capacity in the sector is the availability of either inhouse expertise or external support - for
establishments that are part of chains. We did not investigate directly the capacity or calibre of
managers via the telephone survey as it would have been difficult to address this subject with
the managers as interviewees and the value of the information collected would have been
questionable. However, we did explore the issue of management capacity and calibre,
including sources of management recruitment and issues of training and turnover, with the ten
national providers. This was seen as a key issue for the quality of the care service, including in
turn the recruitment and retention of the care staff, by both the LA interviewees (see part II)
and by the national providers themselves. Recruitment of managers was identified as
problematic by some of the national providers, leading in some cases to the use of agencies to
search for applicants.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
206
I am finding increasingly that we are having to use recruitment firms because people are not
responding to adverts. Managing Director, NATDOM 5
Others were also stressing the need to standardise and professionalise their recruitment
policies.
Historically, all recruitment, there was certainly no central HR control over it. It was all really
done locally. … And what they have been doing is working with line managers, the area
managers now, to help them with things like home manager recruitment and just simple things
like you know let‟s get an up to date role profile with some competencies and let‟s actually look
at standard things to ask at interviews, things to find out about the person, which we didn‟t
have before. So we‟ve brought a bit more standardisation into that. Group HR Director,
NATHOME 4
There was a particular focus on the development of more standardised, more extensive and
more professional training for managers, to improve retention of the managers in the first place
but also to improve their employee relations skills to improve recruitment and retention of the
social care workforce (see Box IV.2).
Box IV.2. National providers’ approach to training managers
What we‟ve actually tried to do is to pull together a more standardised home manager induction
programme because that had also previously been run largely locally and, to be honest, was a bit
hit and miss in terms of what people got or didn‟t get…. Because when we‟ve been doing some
analysis of turnover, quite a lot of our staff turnover happens within six months or certainly within
the first two years and we think that a lot of that is linked to, are we getting the recruitment right
in the first place? And having done the recruitment, are we inducting and sort of embedding
people into the organisation properly? And right now we‟re probably not.
So our staff turnover, for example, as at November last year, was standing at sort of 27%, 28%
which meant that last year 12,000 left and joined this organisation. That‟s like 1,000 people a
month. …..If you could get to grips with turnover, then actually there would be an enormous
benefit to the business because there would be money to be saved in terms of recruitment fees,
agencies, adverts that sort of thing, but also the amount of time that home managers could have to
actually spend on looking after their residents, as opposed to recruiting and inducting new
people, would be of massive benefit… So we‟ve kicked off a project to run a lot of training in
employer relations issues for home managers, because as a business we haven‟t really invested in
training people beyond what I think of as the operational training. We spend a lot of time and
money on things like NVQs in care but we don‟t do much in terms of management development.
So, a home manager is really running quite a complicated difficult little business and we‟ve done
really very little to equip them to do that. Group HR Director. NATHOME 4
So when [managers] start with the business there‟ll be an induction into the business, who we are,
our values, how we operate and the training and managing teams, managing IT systems,
managing budgets and all the finance. So there‟s a fairly extensive induction covering all of those
areas. We have a directory of training courses available in more specialist areas. So there‟s a
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
207
wide variety of clinical specialist courses, right the way through covering more specialist courses
in finance, HR. So managing people and then through to some just simply looking at management
training and their management expertise. We offer ILM qualifications at both level three and
level four to our managers and we‟re also about to launch an undergraduate level course in
Dementia, which will be available for people to apply For. So there‟s a very wide range of
training. HR Director NATHOME 3
However, while national providers were seeking to improve their policies with respect to
recruitment and development of managers, they were also aware that a dedicated local
manager, or indeed owner, could add to the effectiveness of the organisations through
additional commitment and local knowledge (see box IV.3). However, they also stressed that
many managers of establishments owned by national chains were appointed locally and
brought local knowledge to the post. Overall the national providers felt that they were better
placed to help managers through periods of change and restructuring and that the level of
turbulence in the sector might spell the end for committed, local but less professional
management. However, some still felt that they had not yet built upon the advantages of being
a national organisation offering better and more structured career opportunities to their staff,
including managers.
Box IV.3. National providers’ views on the advantages and disadvantages of being a
national organisation
i) Local has its advantages
What you find with the smaller independent provider is that - local services for local people. And
it is very important for the commissioners that there is that local feel. And when you‟re a national
provider that is difficult. (HR Director, NATDOM 1)
What you tend to find with smaller operations ….is that there is a different emotional connection
to the employer. And higher quality. Because these people have built businesses, what you do find
is that some of the branch managers are of a higher calibre. So some of our best branch
managers have come via acquisitions of small independent providers. (HR Director, NATDOM 1)
What you will find is that us and [a competitor] are less responsive to the local market and the
local providers will be much more aligned in terms of what they‟re offering, against the bigger
providers. So they‟re more nimble it would appear. (HR Director, NATDOM1)
ii) But national organisations have more resource and provide more support for change
I guess we‟ve got more resource to put it in, in terms of training, developing people. And we‟ve
got more of a communication network and we can use tools to help, more than a small business
could. But I think the big challenge with the larger organisations is sometimes the scale of
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
operation is that sometimes there are gaps in getting things done the way you‟d like. And I think
we‟ve done a lot to improve that. But I‟m not sure it‟s small versus large, I think it‟s mixed.
(Managing Director, NATDOM 4)
I think if you‟re a national provider with a good reputation then it‟s so much easier. They‟re still
local; they may be national but they‟re still very local. …. (HR Director, NATHOME 5)
I myself have run a care home for a single provider and I think they do have a battle to get
properly skilled people because you don‟t have the support structure. So it‟s quite a scary thing to
be on your own managing a home (Recruitment Director, NATHOME 5)
Easier [for national providers to recruit] because we can be more competitive with salaries. We
have more resources than smaller business and because we have more branches, we can look at
regional recruitment opportunities as well. (National Recruitment Manager, NATDOM 3)
I think the larger providers, you‟ll certainly see within the next 12 to 18 months, a much more
sophisticated use of things like websites to recruit and pre screen staff and channel them through
to the right branch thus in fact reducing the manpower required to recruit but delivering as good
or better results. So I think there will be a widening there of efficiency but I don‟t see massive
differences at this point. (Commercial Director, NATDOM 2)
iii) Changes to the policy environment may be having particularly negative effects on
small providers
The change to effectively straight line or pro rated, minute by minute charging or payment is
really having a fairly substantive impact on the underlying profitability of domiciliary care
businesses. So at the moment I think, because the recruitment market is benign, the impact has, in
fact, been less dramatic. I think when recruitment gets tighter and the training and recruitment
costs start to lift, that is going to hammer domiciliary businesses and I think where we‟ll see the
pain first will be in the smaller providers. (Commercial Director, NATDOM 2)
I think the challenges for the next couple of years are going to be working within the budgetary
constraints. I think that‟s going to be major issue. I think the implementation of personalisation
will bring its own challenges. I think that [there will be] a lot of turmoil at the smaller provider
level because they will just not be able to cope with all these challenges, I think, that‟s going on.
(Managing Director, NATDOM 5)
Small local providers which are a dying breed with all the legislation and everything else.
(National Recruitment Manager, NATDOM 3)
iv) But national organisations are still not leveraging their advantages
I don‟t think we‟re seeing any of the benefits of being a big national organisation. …So well
designed induction and well designed training programme, some of the things that you could
maybe sell at interview, aren‟t really currently in place. And … we ought to be able to offer a way
of potential career progression than if you go and work in a little local home that‟s only got, I
EWERC
208
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
209
don‟t know 360 staff and that‟s their total business. But because we haven‟t really thought like a
big national employer, we haven‟t actually got all the things in place that you would expect us to
have. (Group HR Director, NATHOME 4)
When we consider management structures at the establishment levels, it is of course the case
that those that belong to chains, particularly national chains, are more likely to have access to
support from a specialist HR department or manager (table IV.3). Around one third of IDPs
and close to half of the homes did not have access to such expertise. However, of those that had
this external support, only 30 to 40 percent reported that this expertise was based either inhouse
or locally with three fifths to two thirds saying it was further afield (table IV.4). Where such
support is available it is said to be very wide ranging by around one third of respondents (table
IV.5). A similar percentage refers to assistance with grievance and discipline while recruitment
and absence management are explicitly mentioned by around one tenth of the respondents
respectively.
Table IV.3. Presence of a specialist HR manager or department
a. IDPs
All
Very
small
&small
medium
large
Local
chain
National
chain
Single
site/agency
1*
2*
3*
% with a
specialist HR
manager or
department
69.2
64.3
70.8
71.4
90.0
83.9
9.1
60
70.3
70
% without
30.8
35.7
29.2
28.6
10.0
16.1
90.9
40
29.7
30
b. Homes
All
Very
small
Small
Medium
& Large
Local
chain
National
chain
1*
2*
3*
100.0
Single
site/
agency
10.0
% with a
specialist HR
manager or
department
52.8
20.0
58.3
78.6
50.0
44.4
54.8
53.8
% without
47.2
80.0
41.7
21.4
50.0
0.0
90.0
55.6
45.2
46.2
However, even among national providers the extent of HR support may be limited. One home
that was part of a national chain commented that monitoring of absence had only really just
started in its organisation.
We‟ve just started doing that, we‟ve got a HR department and all of our staff are required to
complete a return to work form if they‟ve been off sick or off with their children or whatever
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
210
reason then they have to complete that, and so the HR department are starting to collate that
information. (OM.H.1.B.NV).
Table IV.4. Location of the specialist HR manager or department
% of Homes
% of IDPs
Total
On-site
7.1
0.0
3.2
Local
32.1
32.4
32.3
Further Afield
60.7
67.6
64.5
Total responses
28
34
62
No response
0
2
2
Box IV.4 provides examples of the support provided to their branch managers according to the
interviews with national providers at headquarters. Some of the managers interviewed in the
telephone survey revealed how important such external support can be:
We‟ve got now, only in the last 3 months, we have an HR business partner and they‟re CIPD
qualified and she‟s just about saved my life as I was doing it all before. So yes we do have a
specialist, and in fact we did have one person but now that‟s developing into a team. I mean
they don‟t necessarily do all the work but they oversee everything right down to career
development and training that sort of thing. (OM.D.2.DN).
Another manager commented on the importance of external support for non standard activities
such as recruiting migrants:
I am now in a position to recruit foreign nationals, so they give me advice about what I need
for somebody from Poland or Hungary for example. And disciplinary and sickness issues and
they will come up and sit in on interviews with staff if necessary. (AH.D.3.CN).
Table IV.5. Types of support provided by specialist HR manager/department
% of Homes
% of IDPs
% of LADPs
Everything that we ask
31.9
38.6
33.3
% Total
Responses
35.0
Grievance and disciplinary
36.2
25.0
44.4
32.0
Recruitment
8.5
11.4
0.0
9.0
Contracts/Legal/Policy
10.6
11.4
22.2
12.0
Attendance and sickness
6.4
4.5
0.0
5.0
H&S and welfare
2.1
0.0
0.0
1.0
Training
4.3
4.5
0.0
4.0
Immigration
0.0
4.5
0.0
2.0
Total responses
47
44
9
100
No response
8
9
3
20
Note: of those who have a specialist HR manager or department, 53 providers responded (some gave multiple
answers) and 20 providers did not respond.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
211
Box IV.4. HR support services
They all have identified regional support. And again, if you compare the quota of HR people per
head, if you look at the healthcare environment you would invariably be looking at one HR person
per 110 to 140 staff. For us, and we‟ve got the biggest HR resource that we‟ve ever had, and in
the 12 months that I‟ve been in post we‟ve doubled the size of our department, we‟ve got one per
496. So there is access to the support, but I suppose it‟s indicative of the industry. HR Director,
NATDOM 1
From a people perspective, I mean there were only 11 people in the HR team so their impact on
the business was really absolutely minimal. They were doing the best they could in the
circumstances in terms of they were creating policies and management guidelines but actually
being able to engage with management and help them with their people management issues, they
just really weren‟t able to do…..We‟re going to have HR Managers on the ground, three or four
per region, and at the moment we‟ve just got one interim in each region promoting some help, and
then we‟re recruiting for some specialist roles, resourcing, learning and development, employer
relations and so on. So that‟s the second strand. The third strand is what I call people
management framework. Basically, as a business, we have never spent any time saying what kind
of employer do we want to be? What is the deal between us and our employees and if they bring
all their skills and capabilities and competencies to work, what can they expect in return in terms
of things like appropriate working environment, tools to do the job, support to do the job, training
and development, reward and recognition? So we started quite a big piece of work on that. Group
HR Director, NATHOME 4
So specifically with HR we have a central, not a distributed HR team, where any manager can
ring, email for advice, but also that team does a lot of dedicated training on things like disciplinary
and grievance procedures. So every manager will have had the opportunity to have a full day
understanding some basics of employment law, how they translate into our procedures and how we
operate those procedures, and we repeat that to pick up new starters, maybe every six months or
so. Corporate Services Director, NATHOME 2)
We have an HR helpline, which is monitored from our support centre and it‟s an advice line for
managers to call about any operational HR queries. But then in the division there is a HR business
partner to deal with anything that‟s more complex and perhaps to help coaching the manager, an
area manager that needs further support in an issue or the more strategic work. So the immediate
support is available on the end of a phone via the advice line but there is personal contact for the
more complex issues. (HR Director NATHOME 3)
One managerial task that was particularly burdensome for IDPs was the scheduling of work.
This managerial problem was being addressed in some organisations by the application of
software (see example below from a local chain) but we did not collect systematic evidence on
the extent to which there were differences in the use of technology to assist in key managerial
tasks by type of organisation, although this could be an area of interest for future research.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
212
We use the care manager system (computer) and this takes 75% of the nightmare out of putting
together the jigsaw. We assign customers to care workers, and the computer does this
according to whether they are walkers, bike riders, or car drivers. We split [X] into two areas –
North and South and once the jigsaw is in place, using Care Manager, it all seems to work
quite well. Most care workers are flexible. We do some work outside of [X] in the boundaries,
and go into agricultural areas. Care Manager tells us if we are overloading one care workers,
if they say they will only work X number of hours or only up until 12 noon – it doesn‟t let us
overload them with work. LKD.6.CL
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
213
IV.2. HR practices and outcomes by provider characteristics
Part III provided an overview of the range of HR policies pursued by both homes and IDPs. In
this section we explore the telephone survey results for evidence first of variations in HR
strategies by type of provider, focusing on issues of size, ownership, CQC star quality and
public/private or voluntary status. Second, we explore the range of variations in the set of HR
strategies adopted by these individual providers: that is how far we find some providers
adopting sets of good HR practices across the range of dimensions and at the other end of the
spectrum whether there are some providers who have poor or weak HR practices across the
spectrum. Third, we report on providers‟ views on what would do most to improve recruitment
and retention in social care.
To simplify the analyses we have streamlined the questionnaire data as presented in part III by
transforming the variables into indicators, sub-indices and indices, as described in appendix
table IV.A1 and in box IV.5 all taking values between 0 and 1. Depending upon the nature of
the indicator/index, we use the relative level of the mean values to identify whether policies are
more favourable to employees or indicative of more professional and/or high performance
practice (closer to one) or alternatively less favourable to employees or indicative of either
more informal or lower trust HR practices. The direction of measurement for each
indicators/sub index/index is set out in the appendix tables IV.A1 to 4. We include in our
discussion not only the quantitative evidence but also the qualitative material both from the
telephone survey of providers and from our interviews with national providers.
Box IV.5. The dataset
We further divide the data into what we have termed the standardised dataset. This refers to 33
indicators of HR practices and 6 indicators of HR outcomes for 102 providers. These indicators
apply to both homes and IDPs and meet the criteria that missing values should not exceed 10%. A
similar 10% cut off was used to eliminate three providers from the standardised data set. For these
providers and indicators we have then imputed the relatively small number of missing values as the
mean for the sub index across all selected providers (see appendix IV.A.1 for details). The 33 HR
practice indicators have been further subdivided into 18 sub-indices and 6 indices covering pay
levels, pay strategies, recruitment; employee development, working time and work organisation.
The six outcome indicators have been combined into 4 sub-indices and 2 indices covering
recruitment and retention outcomes and skill and training outcomes.
For all other data that we use in the analysis we do not include imputed values. These include in
particular: i) data collected specifically about domiciliary care, due to the difference in the
questionnaire; and ii) turnover data, for which due to the difficulties we had in requesting providers
to give us the detailed information needed to calculate these data we have had to analyse the
turnover data separately and for a maximum of 82 independent sector providers instead of 102 for
the standardised data set. Also for other indicators excluded where the missing values exceeded
10% we have not imputed any values.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
214
IV.2.1. HR practices and outcomes by provider characteristics
Box IV.6 provides an overview of the construction of indicators, sub indices, and indices of
HR practices. We present the full information on variations in HR practices measured by the 18
sub-indices and 6 indices by size, ownership and star category in appendix IV.A.2. We also
provide appendix tables on the individual indicators where significant 28 differences between
types of providers have been identified. These tables present some indicators additional to the
standardised set (those excluded for too many missing variables and some specific domiciliary
HR practices) (see appendix table IV.A3).
Box IV.6. Indices (X) and sub-indices (SI) from the standardised dataset
HR PRACTICES INDICES AND SUB-INDICES:
XPAYLEVELS
SIPAYLEVEL
SIPAYUPGRADE
XPAYSTRAT
SIPAYIMP
SIPAYOPPCAR
XEMPDEV
SIEMPVOICE
XRRPRACT
SIRECRUITPR
SIRECRSELEC
XWT
SIWTSTFFPREF
SIWTWEND
XWO
SIWOTIME
XHRPRACT
28
Index of pay levels
Pay levels
Regular upgrading of
pay
SIPAYUNSOCIAL
SIPAYTRAIN
Pay for unsocial hours
Pay for training
SIPAYUPFRONT
Payment of upfront costs
Index of pay strategies
Opportunities for pay
improvement
Opportunities for career
Index of employee development practices
Employee voice
practices
SIEMPAPP
Employee appraisal
Recruitment and retention practices index
Formality of
recruitment process
Selection by skills,
qualifications or
experience
SIRECRETEN
Role of push factors in
staff quits
Index of working time practices
Work schedules that fit
staff preferences
Weekend working
SIWTLHOURS
Long hours/long weeks
SIWTTOFFTRAIN
Time off for training
Index of work organisation practices
Time discretion at work
SIWODISCRET
Task discretion at work
Overall index of HR practices
Specifically, we calculate the probability that the results we have obtained occurred by chance or not. When we
say that a statistical test is significant at the 95% confidence level, we mean that we are at least 95% certain that a
result is genuine (i.e. not a chance finding), or that there is less than a 5% probability of something occurring by
chance.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
215
Overall the picture is one of limited variation across these different provider characteristics,
certainly when compared to the large differences found between LAs and the independent
sector, as we discuss further below. This puts the discussion of good and bad HR practice
within the independent sector into context; on the whole, as we already saw in part III, few
providers are conforming to standard HR practice, particularly in domiciliary care where
contracts are primarily on a zero hour basis and not all time at work is paid for. With these
caveats in mind, we turn to the evidence of variations by provider characteristic.
Size of establishment
The categories we use for the analysis for size of establishment are different for homes and
IDPs due to differences in the sample distribution: very small and small categories are
separately identified for homes but combined for IDPs and medium and large separately
identified for IDPs to reflect the sample distributions – see table IV.1.
Box IV.7. Significant differences between providers in HR practice indicators by size of
establishment
(Standardised dataset)
Homes:
XEMPDEV:
medium/large establishments significantly higher score on employee development
and voice than small establishments
SIPAYOPPCAR:
SIEMPAPP:
SIWTWEND:
IP15:
IWO4:
very small establishments significantly greater career opportunities
than for medium/large establishments.
medium/large establishments significantly higher utilisation of
appraisals than small establishments
significantly less extensive use/ requirements for weekend working in
small than medium/large establishments (10% sig. only)
very small establishments significantly more likely than medium
/large to offer opportunities for progression to senior care worker
very small establishments significantly more likely than medium
/large to offer opportunities to prioritise and carry out tasks in
ways to improve the quality of care
IDPs:
SIPAYTRAIN:
SIRECRSELEC:
IP13:
IWT4:
IWT8:
EWERC
large establishments significantly more likely to offer time off for
training than the very small and small establishments (at 10% level)
large establishments significantly more likely to use more formal
methods of recruitment than the very small and small establishments
very small/small establishments significantly more likely to pay
for induction than large establishments (at 10% only)
large establishments significantly less likely to have all staff
working weekends than both medium and very small/small
establishments
very small/small establishments significantly less likely than
medium establishments to have higher shares of staff working
long hours
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
216
Looking first at sub-indices and indices we find very few notable differences in HR practices
by size of establishment for either homes or IDPs. For homes some of these relationships were
in the expected direction - for example, larger establishments making more use of appraisals.
But others were more counter-intuitive- such as very small establishments being more likely to
offer opportunities for promotion to senior care workers. Other relationships were significant
but not linearly related to size (see box IV.7). For IDPs again there is some evidence of more
formal HR practices among large establishments particularly with respect to recruitment
methods and time off for training. However, there are also some counter-intuitive findings,
particularly that large IDPs are less likely to pay for induction training. On working time, large
establishments appear to have more freedom not to have all staff working weekends (although
this is the opposite to homes). It should also be noted that we found no significant differences
by size of establishment in relation to the specific indicators that only apply to domiciliary
care.
Ownership
There is perhaps a greater expectation of differences by ownership structure, particularly as the
national chains have made significant advances into the market over recent years and may be
doing this in part on the basis of differences in HR practices.
For homes there are some important differences, but they are not all consistently in one
direction (box IV.8). Three pay variables show significant differences but in two cases national
chains provide the best conditions: they are more likely than single agencies to have regular
pay upgrades and more likely to cover upfront costs of entering work than single homes and
local chains (including specifically being more likely to pay for uniforms), but national chains
are the least likely to pay for unsocial hours. National chains are more likely to have long
working hours or 6 or 7 day weeks (and the indicators on long hours working also shows a
similar pattern). One indicator, one sub index and one index suggested that local chains were
significantly less likely to provide for various types of autonomy at work also showed some
significant differences by but in this case the values were lower of local chains than both
national chains and single home and the overall variation in values were low so these are not
included in the graphics illustrating the most significant variations by indicator.
However, for IDPs there are virtually none of the standardised indicators that show any
significant differences between national chains, local chains and single agencies. National
chains and local chains were more likely than single agencies to carry out staff attitude surveys.
Beyond this indicator which could be expected to be related to organisations with more
resources, the only other indicator showing any significant differences suggested that long
hours working was made more use of by national chains. One indicator not included in the
standardised set due to missing variables was found to have a significant difference: single
agencies were less likely to have the Investor in People award than local chains. Again no
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
217
significant differences by ownership were found in relation to the specific indicators for
domiciliary care.
Box IV.8. Significant differences in HR practice indicators between providers by
ownership
Standardised dataset
Homes:
XWO:
local chains significantly less likely than single homes and national chains (latter
10% sig. only) to provide autonomy over time and task in work organisation
SIPAYUNSOCIAL:
SIPAYUPGRADE:
SIPAYUPFRONT:
SIWTLHOURS:
SIWOTIME:
IP12:
IWT8:
IWO5:
national chains significantly less likely than single homes to make
unsocial hours payments (10% sig.only)
single homes significantly less likely to have a regular upgrading of
pay than national chains (10% sig.only)
national chains significantly more likely than single homes and
local chains (latter 10% sig.only) to pay for upfront costs of starting
work
national chains significantly more likely than local chains (10% sig.
only) to have staff working long hours/ more than 5 days
local chains significantly less likely than single homes and national
chains (latter 10% sig. only) to provide time autonomy in work
organisation
national chains significantly more likely than local chains and
single homes (both 10% sig. only) to pay for uniforms
national chains significantly more likely than local chains to
have staff working long hours (10% sig. only)
local chains significantly less likely than national chains and
single homes to provide opportunities to exchange idea with
other carers
IDPs:
IHR3:
IWT8:
single agencies are significantly less likely than national chains
or local chains (latter 10% sig. only) to carry out staff attitude
surveys
national chains significantly more likely than local chains to
have staff working long hours
Non standardised dataset
IDPs:
IOUT3:
local chains were significantly more likely to have the investor
in people award than single agencies
These limited findings on differences between national chains and more local organisations in
homes, but particularly in domiciliary care, chimes with the information we obtained through
our survey of national providers with respect in particular to pay. All national domiciliary care
providers stressed that they fixed pay at the local level according to the policy of the LA (see
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
218
box IV.9) and in one case even paid different rates to staff in the same branch according to
which LA they were working for under subcontract. There was thus no attempt by any of the
national IDPs to establish a national pay policy. This was also the case in two of the national
chains of homes but two did have a national pay scale, one of which was negotiated with a
trade union and another was working towards that objective. One of the national chains
stressed that location within the national pay scale depended, nevertheless, on local factors.
Some national providers stressed that they did try to standardise on more indirect forms of pay
even if they had to vary actual pay levels in line with the LA.
Even the one national provider that recognised a union did not guarantee either a negotiated
wage increase or pay significantly in excess of the minimum wage as this quote reveals:
This year we had a lot of difficulty with the pay review and we ended up imposing the pay
review because the union were looking for a lot more. We were only paying about 11/2% across
the board. We pay around 10 or 15p an hour more than the minimum wage rate at the moment.
Group HR Director, NATHOME 4
Box IV.9. National providers’ pay strategies: the main influence is the local authority
[Payment for travel time, travel costs] - That‟s generally included in the rates as things which we
do. Depending on the contract and the area, we would pay mileage or travel expenses. But it
varies. Managing Director, NATDOM 5
[Pay] also varies - the contact is with the local authority and they are only willing to pay a
certain amount ... there‟s only so much scope you have to pay to the care workers. So again some
of it is determined by how much you could afford to pay the care workers. Managing Director,
NATDOM 4
We don‟t have any national rates. We have purely local rates, and so some parts of the country
it‟s national minimum wage, in other parts it would be significantly higher than that and London
South East would be the obvious candidate just because that‟s what the market demands. But
also, in London you do get higher fee rates and again, there‟s got to be a match between money
coming in and money going out. Corporate Services Director, NATHOME 2
Local pay - we tried to look at standardising but it‟s impossible. National Recruitment Manager,
NATDOM 3
We can‟t pay the same rates everywhere. Because we get paid differently in different places. But
as a company we have certain basics. So our bank holiday rates are double across the country,
whatever we get paid here. We pay for all the training, it doesn‟t matter what the local
authorities, and we provide uniforms, it doesn‟t matter what the local authority said. Managing
Director, NATDOM 5
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
219
Working time and contract arrangements were also not significantly different on most
dimensions. One branch manager of a national chain indicated that zero hours contracts were
the widely accepted industry norm when s/he described a plan to move to guaranteed hours as
„a bit radical‟.
We are doing an analysis at the moment to see what would happen if we put all of our care staff
on salaries, a bit radical I know but what we are looking to do is to see if it‟s viable…I think
that could ultimately change the face of the social care system and in terms of the status of the
staff it would raise them up (OM.D.2.DN)
However, one of the national domiciliary chains in our national provider survey blamed
variations between LAs for their inability to have standard working time conditions.
It‟s difficult to standardise across the country. For example, you can‟t have a standard start
time. In some authorities they start at 7 in the morning or 8 in the morning and finish at 8 at
night. In others, it‟s 6 to 6. This kind of thing. Managing Director, NATDOM 5
However, one area where we might anticipate more marked difference in the future is in the
use of more formal or systematic recruitment methods. The national chains already had
national recruitment procedures and policy advice but while most recruitment was still done at
local and branch level there was evidence in a number of the interviews of moves towards
providing more active support at regional level. However, this greater centralisation might not
be at the expense of informal methods as we also found some evidence in the case studies of
national chains formalising word of mouth recruitment patterns through the development of
voucher schemes as incentives to staff to recommend new recruits.
Box IV.10. Recruitment of care staff in national providers
[Recruitment previously done at branch level]. But we‟ve changed that model to what we call a
regional resourcing lead network. What it was like was that we would have a recruitment coordinator in each branch, and the recruitment co-ordinator was basically an ex care worker
who‟d done his or her backing and who knew how to turn on a computer. And there was
insufficient technical knowledge and insufficient understanding of the link between capacity and
quality, and capacity in grants. So we changed that and we said, well let‟s remove that model and
put in a career recruiter, so a professional recruiter who would cover a cluster of branches.
They‟re called regional resourcing leads. HR Director, NATDOM 1
So very much it‟s locally engaged with national support. That‟s our philosophy on a number of
things, like when we come on to recruitment and retention, it‟s - again, you can‟t do this centrally
alone. You need the local buy in and local management, owning the situation. Managing
Director, NATDOM 4
it would be a local management decision about who they recruit. We don‟t force the hand of the
local management, we expect they would meet certain criteria and if they want a second opinion
they can involve people from the centre. Managing Director, NATDOM 4
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
220
[Setting up] new Regional Recruitment teams: Branch managers had no time to focus on
recruitment. It was the last of their priorities. They had no time or resources for recruitment so
they were reactive the whole time. Interviews [are held] at branch level - it is down to the
individual manager to make the ultimate decision. National Recruitment Manager, NATDOM3
The personnel manual in the recruitment procedure spoon feeds all of the managers. So here‟s the
steps you take, these are the forms you need to use, here‟s the standard letter, standard contract.
So it‟s all there. Corporate Services Director, NATHOME 2
The need for support to local establishment managers in the area of recruitment is indicated by
this account of the efforts a local chain manager had to go to secure an increased workforce
after a successful tender:
I‟ve had to recruit a lot really especially since January so what I‟ve done is take a PowerPoint
presentation and use that to give people an understanding of what we do, how we do it, our
approach to staff and then they can make an informed decision about whether we‟re a) what
they hear floats their boat in terms of coming to social care but also it‟s about making an
informed decision about the kind of employer we are and if they like how we go about and
present things. Anybody who has responded to the Jobcentre Plus advert or to the newspaper
advert that I put out in January where we said if you can tick some of these boxes or aspire to
tick some of these boxes then we would be interested in talking to you because we are looking
for support workers, we‟re looking for supervisors, we‟re looking for mentors, and so since
January we have had over 600 people make contact with us over the phone, my business
development manager who took the post on the 25th January and started working on the 26th we
have seen over 300 people in small groups of up to a maximum of ten, we have today offered 27
people jobs. (UY.D.1.C.L)
This case illustrates both the sheer scale of the recruitment effort and the management
challenges this poses for single or small chain organisations.
CQC star rating
When we look at HR practices by CQC star rating we find that there is fairly systematic
evidence that 3* homes provide better pay and pay related conditions than 1* and 2* homes (2
indices, 4 sub-indices and 4 individual indicators on pay all show this relationship). However,
when it comes to recruitment practices it is 2* homes that seem to have the best practices and
when it comes to employee voice indicators, 3* homes have less developed practices than
either 1* or 2* homes. There is thus only clear evidence in relation to pay indicators that higher
rated homes have higher quality HR practices (box IV.11).
For IDPs there are no significant indices or sub indices by star rating and those individual
indicators that show some significant differences tend to indicate somewhat counter intuitive
relationships. Thus, although 3* IDPs are more likely to pay extra for qualifications and are
less likely to have all staff working weekends, indicators that we take to be indicative of HR
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
221
quality, they are also less likely to carry out staff surveys. When indicators from outside the
standardised data set are considered, we find that 3* homes are also less likely to pay for travel
or provide paid breaks, although they are more likely to offer a longer minimum work period,
None of this suggests a vey strong relationship between quality of HR practices and the star
rating attached to the IDP.
Box IV.11. Significant differences in HR practice indicators between providers by star
rating
Standardised dataset
Homes:
XPAYLEVELS:
XPAYSTRAT:
XRRPRACT:
XEMPDEV:
3* homes offer significantly higher pay than 1* and 2* (latter 10% sig. only)
3* homes offer significantly better pay strategies than 1* and 2*
1* homes have significantly lower quality recruitment practices than 2* homes
3* homes offer significantly worse employee development and voice practices
than 1* and 2* homes
3* homes offer significantly higher pay than 1* (10% sig. only)
SIPAYLEVEL:
SIPAYUNSOCIAL: 3* homes significantly more likely to make unsocial hours
payments than 1* and 2*
3* homes offer significantly worse employee voice practices than
SIEMPVOICE:
1* and 2* homes
2* homes have significantly better recruitment practices than
SIRECRUTPR:
either 1* or 3* homes
IP1:
3* homes offer significantly higher minimum pay than 1*
IP6:
3* homes significantly more likely to pay more for
qualifications than 1*
IP8:
3* homes significantly more likely to pay extra for weekend
work than 2* (10% sig.only)
IP9:
3* homes significantly more likely to pay extra for night work
than 2* and 1* (latter 10% sig. only)
IDPs:
IP6:
IHR3:
IWT4:
3* IDPs significantly more likely to pay more for
qualifications than 2*
3* IDPs significantly less likely to carry out staff attitude
surveys than 1*
3* IDPs significantly less likely to have all staff working
weekends than 1* (10% sig. only)
Non standardised dataset
IDPs:
IPDOM1:
IWTDOM2:
IWTDOM3:
EWERC
1*significantly more likely to pay for travel than 3*
1*significantly more likely to provide a paid break than 2*
3* significantly more likely to provide a longer minimum
work period than 2* (10% sig.only)
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
222
Public, private or voluntary status
Part III has already provided considerable evidence of the divide between the HR practices in
the independent sector and those prevailing in the local authorities, primarily LADPs. To bring
this information together table IV.6 provides a summary of the overall scores within the six
areas of HR practices and for the overall index of HR practices 29. First of all, in comparing
homes and IDPs, we find that homes score slightly better overall, but the difference for the
summary index is not statistically significant. The only statistically significant difference
between them is in work organisation where homes score more strongly than IDPs; otherwise
differences add at most 0.03 to the score.
When LADPs are considered, not only is the summary index of HR practices for LADPs more
than 19% higher than for the independent sector IDPs they also score on average over 16%
higher than the independent sector homes (table IV.6a). These differences are significant and
the same applies for higher scores for LADPs compared to both homes and IDPs for pay levels,
recruitment practices and employee development. However, for pay strategies, although
LADPs score higher than both homes and IDPs, there is only a significant difference with
IDPs. For working time LADPs score worse than both IDPs and homes (difference significant
only with IDPs), possibly reflecting the problems that LADPs have experienced in moving
their staff from standard hours to more flexible and unsocial hours working, such that they
place more stress on requiring staff to be flexible. For work organisation LADPs score
somewhat better than IDPs but lower than homes (neither difference is significant), suggesting
that these scores reflect the different nature of the work between homes and domiciliary care.
It is notable that voluntary, not-for-profit providers score higher than for-profit providers on all
the indicators of HR practices. Considering the aggregate index for homes and IDPs combined,
the difference between voluntary providers and for-profit providers is statistically significant
and represents a gap of some 10% (Table IV.6b). Two other results are statistically significant:
the score for the index of pay levels is 20 per cent higher for voluntary providers than for
private for-profit organisations (reflecting our analysis in part III); and voluntary providers
score substantially higher on the index of recruitment and retention practices.
Finally, when we look at the indicators that are specific to domiciliary care providers (table
IV.6c), we find again that LADPs are significantly more likely to pay for travel time, to offer
guaranteed hours, to provide a paid break but are significantly less likely to attach importance
to matching staff preferences for working time. Other differences are not significant.
29
In order to produce an estimation for LADPs we imputed 16 missing values out of 280, which represent 5.7% of
total values. This translated as 3 imputed values for the indicator IWT8 (30% of the sample of 10 LADPs), 2
imputes for the indicator IP3 (20% of the sample) and 1 impute for 11 different indicators (10% of the sample).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
223
IV.2.2. HR outcomes by provider characteristics
By HR outcomes we refer to the ability of providers to recruit and retain a skilled and
committed workforce. Thus indicators of HR outcomes relate to ease of recruitment, ability to
retain staff, avoidance of high absenteeism, and ability to meet training targets.
Table IV.6. Differences in indices and indicators of HR practices by provider type
a. X indices of HR practices and outcomes
Homes
IDPs
LADPs
LADPs score
as % of
homes
LADPs score
as % of IDPs
0.61**
(L)
0.63**
(L)
0.90**
(H,I)
147.5
142.9
XPAYLEVELS
Index of pay levels
XPAYSTRAT
Index of pay strategies
0.68
0.65*
(L)
0.78 *
(I)
114.7
120.0
XRRPRACT
Index of recruitment
and retention practices
0.61**
(L)
0.63**
(L)
0.81**
(H,I)
132.8
128.6
XEMPDEV
Index of employee
development
0.58**
(L)
0.59**
(L)
0.77**
(H,I)
132.8
130.5
XWT
Index of working time
0.65
0.64*
(L)
0.55*
(I)
84.6
85.9
XWO
Index of work
organisation
0.95**
(I)
0.84**
(H)
0.88
92.6
104.8
XHRPRACT
Index of all HR
practices
0.68**
(L)
0.66**
(L)
0.78**
(H,I)
116.2
119.7
XRROUTCOMES
Index of recruitment
and retention
outcomes
Index of training
outcomes
0.68**
(I)
0.45**,*
(H,L)
0.58*
(I)
85.3
128.9
0.81**
(I)
0.63**
(H)
0.78
96.3
123.8
XTRAINSKILDEV
b. X indices for public, private for-profit and private not-for-profit providers
Public
Private
Forprofit
Private
Voluntary
Voluntary
score as % of
public
Voluntary
score as % of
private
XPAYLEVELS
Index of pay
levels
0.90**
(F,V)
0.60**
(P,V)
0.72**
(P,F)
80%
120%
XPAYSTRAT
Index of pay
strategies
0.78**
(F)
0.65**
(P)
0.73
94%
112%
XRRPRACT
Index of
recruitment and
retention
practices
0.82**
(F)
0.60**
(P,V)
0.71**
(F)
87%
118%
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
XEMPDEV
Index of
employee
development
Index of working
time
XWT
224
0.77**,*
(F,V)
0.57**
(P)
0.62*
(P)
81%
109%
0.55*
(F)
0.64*
(P)
0.65
118%
101%
XWO
Index of work
organisation
0.88
0.89
0.91
103%
102%
XHRPRACT
Index of all HR
practices
0.78**,*
(F,V)
0.66**
(P,V)
0.72**,*
(F,P)
92%
110%
XRROUTCOMES
Index of
recruitment and
retention
outcomes
Index of training
outcomes
0.58
0.56
0.60
103%
108%
0.78
0.71
0.76
98%
107%
XTRAINSKILDEV
c. Indicators of HR practices
Sample size
IDPs
LADPs
IDPs
LADPs
IPDOM1
Compensation for travel costs/travel time
0.38*
0.61*
51
9
IHRDOM1
Performance monitored by electronic monitoring
0.69
0.80
51
10
IWTDOM1
0.55
0.45
52
10
IWTDOM2
Domiciliary care workers expected to tolerate
variation in hours or location at short notice
Paid break between service users
0.12**
0.78**
50
9
IWTDOM3
Minimum length of a work period
0.23
0.56
45
8
IWTDOM4
0.77**
0.39**
52
9
IWTDOM6
Important attached to organising working hours to
fit employees‟ circumstances
Staff required to work alone late at night
0.76
0.75
52
10
IWTDOM7
Contracts offered to care staff
0.23**
1.00**
51
10
Note: A single * indicates a minimum 90% confidence level (p < 0.1), ** indicates a 95% confidence level (p <
0.05). For table IV.6a, I, H, L are used to indicate differences with IDPs, Homes, LAPDs respectively For table
IV.6b, P, F, V are used to indicate differences with Public, Private for-profit, Private not-for-profit respectively
For the standardised dataset we were only able to include a restricted set of outcome measures
due to problems of missing data on staff turnover. The measures (see box IV.12) include
perceptions of recruitments difficulties (including questions on ease of recruitment and on
presence or otherwise of a labour shortage); perceptions of level of staff turnover; perceptions
of level of absenteeism (data on actual absenteeism was presented by managers in too many
diverse ways to be usable for comparisons); and ability to meet NVQ2 training targets (actual
share trained and position in relation to the 50% targets).
For non standardised indicators we have used three indicators of staff retention: these include
indicators of the share of new recruits retained, of overall staff turnover and of staff turnover
excluding new recruits over the past 12 months (with baseline staff level 12 months
previously).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
225
Box IV.12. Indices (X) and sub-indices (SI) from the standardised dataset
XRROUTCOMES
Index of recruitment and retention outcomes
SIRECDIFF
Recruitment difficulties
SITO
Perceptions of staff
turnover
XTRAINSKILDEV
SIABSENT
Perceptions of
absenteeism
Index of training outcome
Size
For homes, appear larger size to be disadvantageous with respect to HR outcomes. The overall
index for recruitment and retention outcomes shows medium and large establishments faring
significantly worse than both very small and small establishments (box IV.13). Medium and
large establishments also have worse perceived levels of both absenteeism and staff turnover.
Training outcomes are also worse in medium/large homes when compared to very small
establishments. However, recruitment difficulties are perceived to be worse in very small
establishments. For IDPs large establishments also have worse perceived problems of
recruitment and retention but the significant differences are primarily with medium
establishments. This also applies to perceived staff turnover rates and to the presence of labour
shortages. As with homes, very small/small establishments consider recruitment difficulties to
be more severe than is the case for large establishments. None of the indicators on actual staff
turnover in the non standardised data set were found to yield any significant differences with
size of establishment.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
226
Box IV.13. Significant differences in HR outcome indicators between providers by size
Standardised dataset
Homes:
XRROUTCOMES: perceived recruitment and retention outcomes significantly worse in
medium/large establishments than small and very small establishments
absence rates in medium/large establishments significantly
SIABSENT:
worse than in small or very small establishments
perceived turnover rates significantly worse in medium/large
SITO:
establishments than small and very small establishments ( latter
10% sig.only)
SITRAINSKILDEV: training outcomes significantly worse in medium/large
establishments than very small establishments(10% sig.only)
recruitment difficulties significantly worse in very small than
SIRECDIFF:
small establishments ( 10% sig. only)
IDPs:
XRROUTCOMES: perceived recruitment and retention outcomes significantly worse in large
establishments than medium establishments
perceived turnover rates significantly worse in /large
SITO:
establishments than medium establishments
recruitment difficulties significantly worse in very small/ small
SIRECDIFF:
establishments than large establishments
IRC7:
large establishments significantly more likely to have staff
shortages than medium
Ownership
For both homes and IDPs the only significant results relate to training outcomes: for homes the
single homes score highest and have significant differences with both national chains and local
chains but for IDPs it is local chains that score highest and have significant differences at 10%
with national chains and also a higher value than for single agencies although this difference is
not significant. Again the staff turnover data are not significantly related to ownership for
either homes or IDPs (see box IV.14).
Box IV.14. Significant differences in HR outcome indicators by ownership
Standardised dataset
Homes:
SITRAINSKILDEV:
IOUT1:
EWERC
single homes have significantly better training outcomes than
national chains or local chains ( latter 10% sig.only)
single homes have significantly better training outcomes than
national chains
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
227
IDPs:
SITRAINSKILDEV:
IOUT1:
local chains have significantly better training outcomes than
national chains (10% sig.only)
local chains have significantly better training outcomes than
national chains
Star rating
Neither homes nor IDPs recorded any significantly different HR outcomes by star rating.
Public, private or voluntary sector status
Table IV.6a shows that homes have the best and IDPs have the worst scores on the recruitment
and retention index and on the training index with LADP scores falling in between. The
differences are significant on recruitment and retention outcomes between IDPs and both
LADPs and homes, and on training between homes and IDPs.. The better performance on HR
outcomes for homes even compared to LADPs where HR practices were superior to both IDPs
and homes, suggests that it is more difficult to recruit and retain workers in domiciliary than
residential care. That is for the same standard of HR practices the nature of the work in
domiciliary care may lead to worse HR outcomes than in homes. The overall difficulty of the
job may thus be considered to require a higher standard for employment practices in
domiciliary care than residential care. Table IV.6b also shows that HR outcomes in the
voluntary sector are close to or above those in the public sector LADPs, but as our sample of
not for profit organisations is weighted towards homes this result may reflect in part the better
outcomes in general for homes. The voluntary sector scores are clearly better than the for profit
sector, however, and while there is still an issue of oversampling of homes in this case the
results refer to the combined private sector sample of homes and IDPs and is thus more
indicative of better outcomes for the voluntary sector (see section IV.5 for our multivariate
analyses which untangle some of these effects)
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
228
IV.2.3. HR practices and strategies by individual provider
Figure IV.1 shows the range of scores among individual providers by the six indices of HR
practices (separately for homes and IDPs), and figure IV.2 portrays an overview of the overall
HR practices index, comparing homes, IDPs and LADPs. The spread of values for the
individual indices is relatively large, amounting to 42% to 83% of the available value range for
homes and 65% to 83% for IDPs. Only the work organisation index has a range below 50%
and this is only for homes.
The spread of values for the six indices is wider than that found for the HR practices index, the
mean of the six, where the range is only 28% for homes and 33% for IDPs, indicating that there
is some balancing between low and high scores across the range of HR practices for the
individual providers. The range for LADPs is even narrower at 16%; thus not only do LADPs
score higher on average than independent sector providers but also they all tend to be
concentrated towards the top end of the distribution.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
Figure IV.1. Range of scores of providers for the six indices of HR practices
a. Homes
b. IDPs
Note: Standardised data set
EWERC
229
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
230
Figure IV.2. Summary measure of index of HR practices for homes, IDPs and LADPs
IV.2.4. Employer views on the effectiveness of HR strategies
Overall the scope for differences in HR strategies is limited within social care, a condition that
was clear to many of the providers whom we interviewed in the telephone survey. We asked
the providers what HR policies they thought would do most to help recruitment and retention.
The option which was chosen that had the highest percentage of providers at saying it would
improve (over three fifths of independentsector providers) and the lowest share saying that they
had already been able to implement such a policy was „pay increases‟ (Table IV.7). LADPs, in
contrast, felt they had already implemented this policy.
It is clear from these answers that many providers are of the view that they are paying less than
they ought to for care staff. They attribute this to the limited fee levels available for care work.
Well I mean again with the care staff it‟s to do with economics can we afford to do it, because
that is our biggest cost area because even if we just give 10 or 20p extra an hour across our
care staff that is a phenomenal amount of money, and as we‟re a not for profit charity so we‟re
in a difficult situation as our margins are very tight (OM.D.2.DN)
The care staff] should be on eight pound an hour really, shouldn‟t they? No, it‟s true though.
[If I could] pay their wages, I would love to give them that. … And it‟s quite sad you know,
because it‟s a hard job, a tiring job. They‟ve got to have a lot of patience and compassion with
them. (ON.H.2 ML)
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
231
The next most popular HR improvement for homes was recognition of variations in service time of day/weekends/type of care/skill etc. However while many more homes than IDPs felt it
would improve retention (35% to 14%) a relatively high share of both sets of providers (26%
of homes, 21% of IDPs) did not think it would improve matters. The next most popular way of
improving recruitment for IDPs was increased opportunities for internal promotions – but,
while a fifth of IDPs thought this would help, a quarter thought it would not; a fifth of homes
also thought more internal promotion would help and a lower share, 15%, thought it would not,
with the balance made up by a higher share of homes saying they had already implemented this
policy.
There were also mixed views over more flexible hours to suit employee preferences; the
majority thought they had already implemented this policy and those that had not mainly
thought it would not help. Training was the main policy improvement that around four fifths of
all independent sector providers felt they had already implemented; more homes than IDPs felt
there was scope for further improvements but few felt it would not help.
Two policies were relatively unpopular with the providers; the first was improved non pay
benefits where they were more – up to 44% in the case of IDPs - who did not think this would
help. The second was more discretion and autonomy in their job. The homes were much more
likely than IDPs to feel they had already implemented this as a policy but those who had not
were much more likely (2:1) to believe it would not help rather than it would help. Hostility to
increased discretion was very evident from the IDPs: 45% did not feel it would help, only 37%
had implemented such a policy and only 18% felt it would help. LADPs took a similar line,
with two thirds saying they had implemented it and one third saying it would not help. These
views were reinforced by some of our interviewees:
No [more discretion] – this would spell disaster, if you have knowledge of people….if have
variation and don‟t work to a high standard. (TE.D.1 CN (V))
No [more discretion] – that might help but it wouldn‟t help service provision – people would
make the wrong judgements. (LK.D.3 DS)
Well, yes, they are shown how to do the job and how they done is done to the best of their
ability – we don‟t want robots working here. But I wouldn‟t want them straying off the correct
way of doing things. (LK.H.3 BL)
That said, a few commented on the restrictions on autonomy and on time to do a good job that
came from the contracting arrangements.
… it would be nice to give them more autonomy, it‟s dictated by social services. (HD.D.1)
Providers were also given the opportunity to cite other HR policies that they could implement
to assist recruitment and retention. Most of the other responses referred, however, to changes in
external policies (see section IV.5 below for questions that explicitly tapped into external
changes by LAs in particular). The main additional HR policies referred to improving the status
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
232
of the job and making staff feel valued (through recognising staff efforts, arranging social
events, providing mobile phones etc).
Table IV.7. HR policies most likely to improve recruitment and retention
% of homes
% of IDPs
% of LADPs
% of All
20.4
77.6
2.0
49
4
7.7
86.5
5.8
52
0
0.0
100.0
0.0
7
3
13.0
83.3
3.7
108
7
62.0
32.0
6.0
50
3
64.0
30.0
6.0
50
2
12.5
75.0
12.5
8
2
59.3
34.3
6.5
108
7
Would recognising variations in service -time of day/weekends/type of care/skill etc.
improve Recruitment and retention
34.8
13.5
Have already implemented
39.1
65.4
would not improve
26.1
21.2
Total responses
46
52
No response
7
0
12.5
87.5
0.0
8
2
22.6
55.7
21.7
106
9
Would improved opportunities for internal promotion
improve Recruitment and retention
Have already implemented
would not improve
Total responses
No response
19.6
65.2
15.2
46
7
19.6
54.9
25.5
51
1
14.3
71.4
14.3
7
3
19.2
60.6
20.2
104
11
Would more flexible hours to suit
improve Recruitment and retention
Have already implemented
would not improve
Total responses
No response
15.2
67.4
17.4
46
7
3.9
78.4
17.6
51
1
0.0
100.0
0.0
6
4
8.7
74.8
16.5
103
12
Would improved non-pay benefits
improve Recruitment and retention
Have already implemented
would not improve
Total responses
No response
15.0
52.5
32.5
40
13
13.0
43.5
43.5
46
6
14.3
71.4
14.3
7
3
14.0
49.5
36.6
93
22
0.0
66.7
33.3
6
4
13.3
53.1
33.7
98
17
Would improved opportunities for training
improve recruitment and retention
Have already implemented
would not improve
Total responses
No response
Would pay increases
improve Recruitment and retention
Have already implemented
would not improve
Total responses
No response
Would more scope for care workers to exercise discretion over how to provide care?
improve Recruitment and retention
9.3
18.4
Have already implemented
69.8
36.7
would not improve
20.9
44.9
Total responses
43
49
No response
10
3
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
233
IV.3. LA commissioning and contracting and provider HR
practices and outcomes
IV.3.1. The influence of LA fee levels on pay
Domiciliary care
If we plot the level of fees offered by LAs against the normal rates of pay paid by the IDPs in
our survey (Figure IV.3) we find that for IDPs, the level of LA fees is an enabler but not a
determinant of higher pay for care staff. Nevertheless, normal pay rates above £7 an hour were
only found in LAs where the fee level was at least £13 an hour. In Figure IV.4 we plot a trend
line of best fit between the normal rate of pay and the level of LA fees. The implication of the
trend line is that for every pound in increased LA fees, normal pay increases by 19p an hour.
This may not be considered a very good return on higher fees given that that majority of IDPs
costs are labour costs, the worker‟s normal pay rate. For this model, the R2 value is 0.37, which
means that the LA fee level accounts for 37% of the variation of workers‟ pay across providers.
Figure IV.3. A comparison of LA fees and normal rates of pay in IDPs
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
234
Figure IV.4. Trend line of best fit between LA fees and normal rates of pay in
IDPs
£10
y = 0.186x + 4.19
R² = 0.367
Normal rates of pay
£9
£8
£7
£6
£5
£10
£11
£12
£13
£14
£15
£16
£17
£18
£19
£20
LA fees
Homes
For homes there is an even less clear cut relationships between LA fees and normal pay rates.
To provide an estimate of LA fee levels that has more relationship to an hourly wage we have
divided the weekly fee by 40, giving a fee ranging between £8 and £14. Wages paid are low
and relatively similar between £8 and £10 an hour; they are somewhat higher at £12 and £14
an hour though not at £13 an hour (Figure IV.5). Plotting a trend line between fees and normal
pay rates shows that for every £1 extra in fees paid normal pay increases by 14p per hour
(figure IV.6). Not only is this a lower boost to pay even than for IDPs but LA fees also explain
less of the variation in normal pay rates: the R2 value is only 0.20, which means that the LA fee
level accounts for just 20% of the variation of workers‟ pay. For homes a lot of the costs relate
to housing costs not just labour costs so this weaker relationship between fees and wages was
not unexpected.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
235
Figure IV.5. A comparison of LA fees and normal rates of pay in homes
Figure IV.6. Trend line of best fit between LA fees and normal rates of pay in IDPs
£8.5
y = 0.137x + 4.85
R² = 0.197
Normal rates of pay
£8.0
£7.5
£7.0
£6.5
£6.0
£5.5
£7
£8
£9
£10
LA fees
EWERC
£11
£12
£13
£14
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
236
Figure IV.7 plots the level of wage rates in care homes against the percentage of service users
funded by LAs. This shows a tendency for normal pay by provider to be concentrated at the
bottom end of the distribution- under £6 an hour- where the residential home is primarily
dependent upon the LA. Where more than 50 per cent of the business comes from non LA
sources only 18 percent of providers pay at this level compared to 77% of those homes where
more than 85% of the business comes from LA supported clients.
Figure IV.7. Composition of homes paying different normal pay rates by proportion of
LA funding
< £6
£6 - £6.50
> £6.50
8%
18%
29%
36%
64%
15%
27%
53%
77%
36%
18%
18%
<50%
50-70%
71-84%
>=85%
% of service users funded by LAs
These variations in the business are of course linked to the income levels in the area and thus
indirectly to wage levels The evidence we collected on the differences in the prices charged by
providers to private versus LA clients is summarised in box IV.15. The pattern of charging
varied by region for both homes and domiciliary care but many fewer of the IDPs compared to
homes relied on private clients for a significant share of their markets (see table IV.1).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
237
Box IV.15. Comparison of LA and private fees levels
The gap between private and LA fee levels was much greater for homes and especially for homes
located in the southern LAs. This gap was found to be in hundreds of pounds per week- from
£100 to £300 and more in a few cases. In the northern and midlands LAs there was much less
evidence of differences between the LA rate and the rates charged to private residents; several
said they had no private residents and some said they charged the same even though rates were
low. We identified a few examples of higher fees in excess of £100- one in AD where the LA had
said top up fees were rare and another, less surprisingly, in RD where the LA fee was known to be
below the going rate in the area, with those without capacity to pay top ups placed in cheaper
homes located in areas bordering the LA.
The pattern for domiciliary care was more varied with some IDPs even in more depressed and
areas also charging top ups to private clients while some southern IDPs would only add a modest
top up or around £1 an hour or so. Only one IDP said it charged more than a £3 an hour top up to
private clients (one in XD where the private rate was £7.50 above the LA rate). This varied pattern
may reflect tighter pricing policies by LAs in some depressed areas. A few IDPs gave a range of
fees that were lower than the LA rates but these may have included fees for basic cleaning. Only
one in a midlands LA- OM- said they charged less to private clients but several said they charge
the same rate. Practices varied within an LA- for example in one of the low fee LAs IL , three
IDPs effectively charged the same rate to private as well as LA funded clients while a fourth
asked for a top up of £2 an hour.
IV.3.2. HR practices and outcomes by type of LA
We have used two alternative classifications of LA commissioning policy to explore links with
the HR practices and outcomes for independent sector providers. Our first classification
involves the partnership, mixed and cost minimising categories developed in part II of this
report. Our second classification defines categories of LAs according to the level of LA fees.
Table IV.8 provides a summary of the overall X indices by homes and IDPs by the partnership
categorisation and table IV.9 provides a similar summary using the LA fees categorisation. Full
details of indices and sub-indices for the standardised dataset are presented in appendix tables
IV.A11 through IV.A.14.
Partnership, mixed and cost minimising local authorities
To summarize the overall results for the partnership categorisation, a number of significant
differences in sub-indices and indices were found for homes although the direction of the
relationship did not always accord with expectations that partnership would promote good HR
practices or outcomes. However, for IDPs there are almost no significant differences except for
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
238
the summary index of HR practices where providers in partnership LAs score significantly
better than those in cost minimising LAs.
Pay sub-indices and indices were the most frequently found to be significant for homes (box
IV.16); pay levels, pay for unsocial hours, opportunities for pay improvements and the
aggregate Xpay levels all revealed significant differences in the expected direction with
partnerships having the best conditions but the differences were sometimes only significant
with mixed and sometimes only significant with cost minimising LAs. Similar patterns were
found for the individual indicators on normal pay, extra pay for qualifications and for weekend
work. Furthermore, paid time off for training was, contrary to expectations, significantly more
common among providers in cost minimising areas, although the aggregate differences were
not large.
Box IV.16. The significance of LA commissioning strategy (partnership, mixed, cost
minimising) in explaining differences in HR Practice indicators among providers
Standardised dataset
Homes:
XPAYLEVELS:
XEMPDEV:
pay levels significantly higher in partnership than mixed LAs.
employee development and voice practices significantly better in cost
minimising than in partnership or mixed LAs (10% sig.only).
pay levels significantly higher in partnership than mixed and cost
SIPAYLEVEL:
minimising LAs
SIPAYUNSOCIAL: pay for unsocial hours significantly more common in partnership
than mixed LAs
opportunities for pay improvements significantly higher in
SIPAYIMP:
partnership than cost minimising LAs
pay for training significantly higher in cost minimising LAs than
SIPAYTRAIN:
in partnership and mixed LAs (10% sig.only)
weekend working less common/ less of a requirement in
SIWTWEND:
partnership than mixed LAs
staff less likely to be working long hours or long weeks in mixed
SIWTLHOURS:
than in partnership or cost minimising LAs
SIWTTOFFTRAIN: staff least likely to be given time off for training in mixed
compared to partnership or cost minimising LAs (latter 10%
sig.only)
IP2:
normal pay levels significantly higher in partnership than
mixed (10% sig. only) and cost minimising LAs
IP6:
extra pay for qualifications significantly higher in partnership
than mixed LAs (10% sig. only)
IP8:
extra pay for weekend work significantly higher in partnership
than mixed and cost minimising LAs
IP14:
pay for training significantly higher in cost minimising than
mixed LAs(10% sig. only)
IWT4:
staff less likely to be all working weekends in partnership than
mixed LAs
IWT8:
staff less likely to be working long hours in mixed than in
partnership LAs
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
239
IDPs:
XHRPRACT:
significantly higher scores in partnership than cost minimising LAs
IHR2:
frequency of staff meetings significantly higher in cost
minimising than partnership LAs
Non standardised dataset
IDPs:
IWTDOM1:
staff in cost minimising LAs significantly more likely to be
expected to tolerate changes in hours or location at short
notice
The only other sub-index where partnerships were clearly associated with higher HR practice
scores was that related to requirements for weekend working in homes, although providers in
the mixed areas scored the lowest, a pattern reaffirmed in the indicator on share of all staff
involved in weekend working. The sub-index on working long hours and 6/7 days found
providers in partnership and cost minimising LAs to have lower scores than providers in
„mixed‟ LAs. The indicator for working long hours shows a similar pattern with mixed having
the fewest staff in this category. When it came to time off for training, however, those in the
mixed areas scored the lowest. Finally, for employee development and voice we find those in
cost minimising LAs scored the highest, with the score significantly different from both of the
other two categories (box IV.16). This has parallels to the other apparently perverse result
where 3* providers had worse employee voice and development than 1* categories by CQC
(see box IV.1 above).
For IDPs, as we have already noted, it is only the overall HR practices index that reveals any
significant differences and here the pattern is for providers in partnership LAs to have
significantly higher scores than those in cost minimising LAs. Even at the level of indicators
there is only one significant result, with this time providers in cost minimising LAs more likely
to carry out staff attitude surveys.
Box IV.17. The significance of LA commissioning strategy (partnership, mixed, cost
minimising) in explaining differences in HR Outcome indicators among providers
Standardised dataset
Homes:
SITRAINSKILLDEV:
SIRECDIFF:
IOUT1:
EWERC
training outcomes significantly better in mixed than in partnership
or cost minimising LAs
recruitment difficulties significantly worse in partnership than
cost minimising LAs (10% sig. only)
shares of staff trained to NVQ2 significantly better in mixed
than in partnership (10% sig. only) and cost minimising LAs
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
240
When it comes to HR outcomes, again there are no significant results for IDPs. For homes
those in partnership LAs face significantly greater recruitment difficulties than those in cost
minimising LAs and those in mixed LA areas have significantly better training outcomes than
either of the two other types of areas (box IV.17). None of the indicators of actual staff
turnover were found to be related to this classification of LA commissioning.
Table IV.8. Summary indices for homes and IDPs by partnership, mixed and cost
minimising type of local authority (mean values of indices)
a. Homes
All
Partnership
LAs
Mixed
LAs
Cost minimising
LAs
0.61
HR PRACTICES
XPAYLEVELS
XPAYSTRAT
XRRPRACT
XEMPDEV
XWT
XWO
XHRPRACT
Pay levels
Pay strategies
Recruitment & retention
practices
Training & development
0.61
0.67
0.54
(**M)
(**P)
0.68
0.64
0.72
0.65
0.67
0.67
0.58
0.55
0.55
0.66
(*C)
(*C)
(*M P)
0.65
0.59
Working time
Work organisation
Index of all HR practices
0.65
0.95
0.68
0.67
0.94
0.69
0.62
0.96
0.66
0.66
0.93
0.68
Recruitment & retention
NVQ training targets
0.68
0.81
0.68
0.75
0.67
0.94
0.68
0.73
(** M)
(** P C)
(** M)
All
Partnership
LAs
Mixed
LAs
Cost minimising
LAs
0.63
0.65
0.63
0.66
0.68
0.66
0.64
0.65
0.66
0.55
0.60
0.55
XEMPDEV
XWT
Pay levels
Pay strategies
Recruitment & retention
practices
Training & development
Working time
0.59
0.64
0.61
0.64
0.60
0.60
0.55
0.67
XWO
Work organisation
0.84
0.86
0.84
0.78
XHRPRACT
Index of all HR practices
0.66
0.68
0.66
HR OUTCOMES
XRROUTCOMES
XTRAINSKILDEV
b. IDPs
HR PRACTICES
XPAYLEVELS
XPAYSTRAT
XRRPRACT
(** C)
0.62
(** P)
HR OUTCOMES
XRROUTCOMES
XTRAINSKILDEV
Recruitment & retention
NVQ training targets
0.45
0.63
0.46
0.55
0.45
0.73
0.44
0.63
Note: Full details in appendix tables IV.A11 and IV.A12. P, M, C used to indicate difference from partnership,
mixed and cost minimising LAs respectively
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
241
High, medium and low fees local authorities
To explore the influence of LA fees on HR practices and indicators we have collapsed our four
categories of fee levels developed in Part II into three categories. This was to avoid having only
two LAs in each of the very low categories. Note that in comparison to the partnership, mixed,
cost minimising classification we have different measures for LAs between homes and IDPs.
This classification of LA influences revealed many more significant effects for IDPs compared
to the partnership classification above; for homes, the number of significant indicators is very
similar. For IDPs the summary index of HR practices is also still significant, with providers in
low fee areas having significantly lower aggregate HR practice scores than those in high fee
areas; the medium fee areas have a medium score but the difference is not significant.
A high share of the consistent relationships apply to pay indicators (box IV.18). For homes the
pay level, pay improvements and the overall pay index all show significantly higher pay levels
in high fee areas compared to low fee areas. High fee areas are also best for unsocial hours
payments but medium fee areas are the worst. At the individual indicator level we also find
significant differences between high and low fee areas for minimum pay, normal pay and extra
pay for qualifications or weekend work. For IDPs indicators for pay levels and pay
improvements are significantly lower in low fee areas compared to either medium or high fee
areas. Pay for unsocial hours is significantly higher in high fee to low fee areas. Again at the
individual indicator level, we find significant differences between high and low fee areas for
minimum pay, normal pay and extra pay for qualifications but extra pay for weekend work is
lowest in medium fee areas.
Box IV.18. The significance of LA fees (high, medium, low) in explaining differences in
HR practice indicators among providers
Standardised dataset
Homes:
XPAYLEVELS: pay levels significantly higher in high than low fee LAs
pay levels significantly higher in high than low fee LAs
SIPAYLEVEL:
SIPAYUNSOCIAL: pay for unsocial hours significantly more common in high than
medium fee LAs
opportunities for pay improvements significantly higher in high
SIPAYIMP:
than low fee LAs
weekend working less common/ less of a requirement in high than
SIWTWEND:
low fee LAs (10% sig. only)
staff more likely to be working long hours or long weeks in high
SIWTLHOURS:
than in medium or low fee LAs
staff significantly more likely to be able to exercise discretion at
SIWODISCREET:
work in low than in high fee LAs
IP1:
minimum pay significantly higher in high than low fee LAs
IP2:
normal pay significantly higher in high than low fee LAs
IP6:
extra pay for qualifications significantly higher in high than
medium or low fee LAs
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
IP8:
IWT4:
IWT8:
IWO4:
242
extra pay for weekend work significantly higher in high than
medium or low fee LAs
Staff less likely to be all working weekends in high than low or
medium LAs (latter 10% sig. only)
Staff less likely to be working long hours in medium fee than in
high fee LAs
Staff in low fee LAs significantly more likely to be able to
prioritise tasks to improve care than in high fee LAs
IDPs:
XWO:
staff in high and low fee areas significantly more likely to be able to exercise
discretion at work than in medium fee LAs (latter 10% sig. only)
XHRPRACT:
significantly higher scores in high than low fee LAs
pay levels significantly lower in low fee LAs than in medium or
SIPAYLEVEL:
high fee LAs
pay for unsocial hours significantly more common in high than
SIPAYUNSOCIAL:
low fee LAs (10% sig.only)
opportunities for pay improvements significantly lower in low
SIPAYIMP:
fee LAs than in medium or high fee LAs
significantly less likely to have time off for training in low fee
SIWTTOFFTRAIN:
LAs than in medium or high fee LAs
significantly more likely to have time discretion at work in low
SIWOTIME:
and high fee LAs than medium fee LAs
IP1:
minimum pay significantly lower in low fee LAs than in
medium or high fee LAs
IP2:
normal pay significantly lower in low fee LAs than in medium
or high fee LAs
IP6:
extra pay for qualifications significantly higher in high than
medium or low fee LAs
IP8:
extra pay for weekend work significantly lower in medium fee
LAs than in low or high fee LAs
IWO1:
staff in low fee LAs significantly more likely to have time to
carry out tasks to a high standard than in medium fee LAs
IWO2:
staff in low fee LAs significantly more likely to have time to
develop relationships than in medium fee LAs
Non standardised dataset
IDPs:
IOUT3:
IHRDOM1:
significantly more likely to have investors in people award in
medium than low fee LAs
significantly more use in low fee LAs than medium fee LAs
For homes, as with our partnership classification above, we again find the potentially
inconsistent results that high fee areas score best on not requiring full weekend working but
worst on the share with long hours and working 6 or 7 days (box IV.18).30 One relationship
30
These results are confirmed at the indicator level for the share working weekends and for long hours working
although the significant difference is only between medium and high fee areas in this instance.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
243
works in a potentially perverse direction with low fee areas offering significantly higher worker
discretion and autonomy than high fee areas (particularly in relation to opportunities to
prioritise tasks) but the differences in aggregate scores are small.31
Table IV.9. Summary indices for homes and IDPs by low, medium and high fee paying
local authority (mean values of indices)
a. Homes
All
Low fee
LAs
Medium
fee LAs
0.55
0.59
High fee
LAs
HR PRACTICES
XPAYLEVELS
Pay levels
0.61
(**H)
0.69
(**L)
XPAYSTRAT
Pay strategies
0.68
0.66
0.66
0.73
XRRPRACT
Recruitment& retention practices
0.61
0.56
0.61
0.67
XEMPDEV
Training & development
0.58
0.60
0.60
0.53
XWT
XWO
Working time
Work organisation
0.65
0.95
0.65
0.95
0.63
0.95
0.66
0.93
XHRPRACT
Index of all HR practices
0.68
0.66
0.67
0.70
XRROUTCOMES
Recruitment & retention
0.68
0.69
0.61
0.70
XTRAINSKILDEV
NVQ training targets
0.81
0.86
0.95 (** H)
HR OUTCOMES
(** H)
0.68
(** M L)
b. IDPs
All
Low fee
LAs
Medium
fee LAs
High fee
LAs
HR PRACTICES
XPAYLEVELS
Pay levels
0.63
0.60
0.61
0.68
XPAYSTRAT
Pay strategies
0.65
0.59
0.68
0.68
XRRPRACT
Recruitment& retention practices
0.63
0.56
0.65
0.66
XEMPDEV
Training & development
0.59
0.54
0.60
0.62
XWT
Working time
0.64
0.58
0.68
0.63
XWO
Work organisation
0.84
0.87 (* M)
XHRPRACT
0.75
0.91
(**L *H)
(** M)
Index of all HR practices
0.66
0.62
(** H)
0.66
0.70
(** L)
XRROUTCOMES
Recruitment & retention
0.45
0.39
0.51
0.43
XTRAINSKILDEV
NVQ training targets
0.63
0.71
0.67
0.49
HR OUTCOMES
Note: Full details in appendix tables IV.A13 and IV.A14. H, M, L are used to indicate significant differences with high,
medium or low fee LAs respectively
31
The results detailed in appendix table IV.A13 show mean aggregate scores of 0.93 (all homes), 0.96 (Low fees
homes), 0.93 (Medium fees homes) and 0.89 (High fees homes).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
244
For IDPs low fee area providers are significantly less likely to provide time off for training
than either medium or high fee LA providers. The two remaining practices that are significant
relate to work organisation – namely, time allowed to complete tasks and form relationships
(SIWOTIME) and the aggregate work organising index (XWO). However, here the main
finding is that providers in medium fee LAs are less likely than those with either higher or
lower fees to provide sufficient time for high quality work (box IV.18). At the individual
indicator level the significant differences in either time for carrying out tasks or time to develop
relationships are between low and medium fee LAs only. None of the specific domiciliary
variables were found to be significantly related to fee levels. Among the other non standard
indicators, for IDPs medium fee LA providers were more likely to have the investor in people
award than low fee LAs.
Providers explicitly identified the level and form of LA fee as a major factor in their HR
practices decisions. For example one provider explicitly linked the upgrading of staff pay to
whether or not there was an upgrade in fees paid by their LA.
They [the LA] haven‟t offered enough over the last year, so we have not upgraded staff for 18
months. Prior to that they got one regularly each year. (LK.D.3 DS).
Another regarded their decision not to pay mileage as a direct reflection of the lack of a
mileage allowance in the LA fee.
I do think care workers should be paid more than what they do get paid, especially because
they don‟t pay mileage, it‟s very difficult. And they are needed, you know, care workers are
essential. So I think if they did contribute towards mileage that would be definitely beneficial.
(ON.D.3 BN).
However, for some providers it is the general change in labour market conditions - for
example, the increased legal minimum holiday entitlements – that have increased costs.
This year and last year, it was an increase in holiday hours, because we‟ve got a large staff and
staffing costs are about I think 70% of our turnover and so increased holiday hours makes a big
difference to that so what we‟ve had to do in considering this year and last year, so holiday
hours have gone up from 4 times your contracted hours to 5.6, which is obviously quite a leap.
(RD.H.3.A.L)
As most independent sector providers are operating at the bottom of the set of employment
conditions, any raising of minimum standards for the labour market as a whole is likely to have
a disproportionate effect on the organisation and it is not clear that LA fees are always
upgraded in line with such changes to minimum labour market conditions of employment.
With respect to HR outcomes, we found that among homes, providers in high fee areas had the
worst outcomes in regard to meeting NVQ training targets; medium fee area providers
performed the best but there were significant differences between both low to high and medium
to high fee area (box IV.19). These findings are confirmed by each of the indicators making up
the sub-index - that is, the measure of the actual share of staff trained to NVQ level 2 and the
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
245
likelihood of meeting the 50% NVQ level 2 target. For IDPs the only outcome variable to be
significantly associated with LA fees was that relating to subjective evaluations of staff
turnover which were worse in low fee areas. This is perhaps the first result indicating that more
positive commissioning might act to provide better absolute outcomes (where results are in the
opposite direction, LA commissioning may still be helping if the alternative of a low fee might
be even higher turnover).
For homes, high fee areas had the best overall turnover rates but none of the paired
comparisons by fee level were significant. For IDPs the share of new recruits retained was
significantly lower in low fee LAs compared to medium fee LAs, and the average for high fee
LAs was similar to that for medium fee LAs even if there was not a significant difference (box
IV.19). Other staff turnover indicators did not yield any significant results.
Box IV.19. The significance of LA fees (high, medium, low) in explaining differences in
HR outcome indicators among providers
Standardised dataset
Homes:
SITRAINSKILLDEV:
IOUT1:
IOUT2:
training outcomes significantly worse in high than medium or low
fee LAs (latter 10% sig.only)
shares of staff trained to NVQ2 significantly higher in medium
than high fee LAs
providers in high fee areas significantly less likely to
meet NVQ target than in medium (10% sig.only) or low
fee areas
IDPs:
significantly worse perceptions of staff turnover in low
fee paying LAs than in medium fee areas
SITO:
Non standardised dataset
IDPs:
IRT2:
EWERC
Share of new starters retained significantly lower in low
fee to medium fee LAs (10% sig.only)
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
246
IV.4. Labour market conditions and provider HR practices and
outcomes
IV.4.1. The influence of local labour market conditions on pay
Figure IV.8 compares the level of normal pay in our sample of providers to the median hourly
pay for female part-time workers in the specific LA labour market. LAs listed along the
horizontal axis are ranked by the level of the local labour market median female part-time pay
rate (from high to low reading from left to right). The first point to observe is that for the two
LAs with the highest local median rates (AW and RN), the relative level of normal pay for care
workers in the surveyed providers is the lowest for all the providers in our sample. A second
point to observe is that, where pay levels reach a high percentage of the local labour market
female median rate or even exceed it, this applies to only some of the providers in the area so
that the effect is to spread out the ratios, suggesting wide variations in pay strategies between
providers. This mirrors the findings for local labour market fees (section IV.3.1) that not all
providers react in the same way either to LA fees or to local labour market conditions.
Figure IV.8. Providers’ normal pay for care workers by LA, relative to the local market
median for female part-time workers
110%
100%
90%
80%
70%
13
14
UY
IL
12
ON
11
TE
10
RT
9
OM
8
LK
7
RD
6
AD
5
AH
4
HD
3
XD
2
RN
1
AW
50%
0
60%
Note: The different points on the vertical lines represent the ratio of normal pay for each provider organisation to
the median hourly pay for female part-time workers in the specific local authority labour market.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
247
In general we can observe a high concentration of pay levels between 75% and 90% of the
relevant median. This finding underlines the low level of pay in the sector as the median level
of female part-time hourly pay is only 65% of male full-time hourly pay at the national level.
There are only 6% of providers paying above the local labour market median for female parttimers and only16% paying above 90%. At the other end of the spectrum 21% of the sample
paid below 75% of the median and all providers in one LA, classified as a „cost minimising‟
LA but located in a high wage area (outer London), paid rates below 60% of female part-time
median pay.
IV.4.2. The influence of local labour market conditions on HR practices and
outcomes
To explore the impact of local labour market conditions on HR practices and outcomes we use
the combined measures of labour market demand and local labour market pay conditions
developed in part I (see section I.7 and appendix table I.A1 and appendix figure I.A1).On this
basis we have divided the LAs into weak, medium and strong labour demand.
Labour demand leads to the highest number of significant differences between providers for
homes, although for IDPs variation in LA fees (section IV.3.2) generated a wider range of
significant results. Not all relationships are in predictable directions but most suggest that
providers do have to improve their HR practices when located in local labour markets
characterised as strong demand areas. Table IV.10 summarises the results for the different
summary indices.
For homes, labour demand is significantly associated with four overall indices: for pay levels,
working time and the summary index of HR practices it is the strong labour demand areas
where the scores are highest. By contrast, the index for work organisation suggests that
discretion at work is lower in strong demand areas, perhaps suggesting that workers are more
under pressure in these areas (box IV.19). There are less strong relationships at the aggregate
index level for IDPs: only the index for work organisation is significant but here it is the
medium demand areas that offer less discretion than either weak or strong demand areas.
Notably no significant differences among IDPs in different local labour markets were found for
the overall HR practices index even though they were found for LA fee levels (see box IV.15
above).
Local labour market demand is significantly related to pay levels for both homes and IDPs. As
anticipated, pay levels are highest in strong demand areas. For homes the main differences are
between strong and weak areas32 while for IDPs it is low wages in weak demand areas relative
to both medium and strong demand areas that stands out. Unsocial hours payments are also
more common in strong demand areas and this time for both homes and IDPs the main
32
The sub-index measures for pay levels among homes are 0.46 (strong demand areas), 0.31 (medium) and 0.20
(weak) (see appendix table IV.A15).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
248
differences are between strong demand and other areas. Homes also record significant results
for pay upgrade opportunities and the overall X pay levels index also has significant
differences between both strong and medium with weak demand areas. At the indicator level
both homes and IDPs record minimum and normal pay to be lower in weak demand areas and
extra pay for weekend work to be higher in strong demand areas, although the exact pattern of
significant differences varies. For homes extra pay for qualifications is also significantly higher
in strong demand areas but for IDPs there is a somewhat perverse result that staff are more
likely to have to pay for their own uniforms in medium compared to weak demand areas. There
is also one significant result for a pay indicator that applies specifically to IDPs (IPDOM1),
which suggests that those providers in strong demand areas are more likely to pay for travel
than those in medium demand areas.
Box IV.19. Significant differences among providers in HR practice indicators by
labour demand (weak, medium, strong)
Standardised dataset
Homes:
XPAYLEVELS:
XWT:
pay levels significantly lower in weak than medium or strong demand areas
working time arrangements significantly better in strong than weak demand
areas (10% sig.only)
XWO:
opportunities to exercise discretion significantly lower in strong than in weak or
medium (10% sig.only) demand areas
XHRPRACT:
overall high practices score significantly higher in strong than medium or weak
demand areas.
pay levels significantly higher in strong than medium (10%
SIPAYLEVEL:
sig.only) or weak demand areas
SIPAYUNSOCIAL: pay for unsocial hours significantly more common in strong than
weak demand areas
SIPAYUPGRADE: regular pay upgrading less common in weak than strong or
medium demand areas.
weekend working less common/ less of a requirement in strong
SIWTWEND:
and medium than weak demand areas
staff more likely to be working long hours or long weeks in strong
SIWTLHOURS:
than in weak demand areas
staff significantly less likely to be able to exercise discretion at
SIWODISCREET:
work in strong than in medium or weak demand areas
working time significantly more likely to be matched to employee
SIWTSTFFPREF:
preferences in weak than strong demand areas
SIWTTOFFTRAIN: staff significantly more likely to be given time off for training in
strong compared to weak demand areas
IP1:
minimum pay significantly higher in strong than weak
demand areas
IP2:
normal pay significantly higher in strong than weak demand
areas
IP6:
extra pay for qualifications significantly higher in strong than
weak demand areas (10% sig.only)
IP8:
extra pay for weekend work significantly lower in weak than
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
IWT4:
IWT5:
249
strong or medium demand areas (latter 10% sig. only)
staff less likely to be all working weekends in strong than
medium or weak demand areas
availability for weekend work more likely to be a recruitment
requirement in weak than strong or medium demand areas
IDPs:
XWO:
opportunities to exercise discretion significantly lower in medium than in weak
or strong demand areas
pay levels significantly lower in weak than medium or strong
SIPAYLEVEL:
demand areas
pay for unsocial hours significantly more common in strong
SIPAYUNSOCIAL:
than medium or weak demand areas
significantly more likely to have time discretion at work in
SIWOTIME:
weak and strong than medium demand areas
IP1:
minimum pay levels significantly lower in weak than medium
or strong demand areas
IP2:
normal pay levels significantly lower in weak than medium or
strong demand areas
IP8:
extra pay for weekend work significantly higher in strong than
medium demand areas
IP12:
staff significantly more likely to have to pay for uniforms in
medium than weak demand areas (10% sig.only)
IWT4:
staff less likely to be all working weekends in strong and
medium (10% sig.only) than weak demand areas
IWO1:
staff in medium demand areas significantly less likely to have
time to carry out tasks to a high standard than in weak or
strong demand areas
IWO2:
staff in medium demand areas significantly less likely to have
time to develop relationships than in weak or strong demand
areas
Non standardised dataset
IDPs:
IPDOM1:
IHRDOM1:
IOUT3:
IWTDOM5:
staff significantly more likely to be paid for travel time in
strong than medium demand areas
significantly more use of electronic monitoring in weak than
strong demand areas
significantly more likely to have investors in people award in
medium than strong demand areas
minimum lengths of visits significantly more likely to be
longer in medium than strong demand areas
For IDPs there are few strong relationships with local demand conditions other than for pay.
The only other HR practice areas for IDPs to reveal significant differences at the sub-index
level are those related to work organisation (as found for LA fee levels, box IV.17) and again
here it is the medium demand area that scores significantly worse than strong or weak demand
areas (a finding mirrored in two of the individual indicators in this area, IWO1 and IWO2, box
IV.19). With regard to working time, the indicator on staff working weekends suggests that it is
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
250
more common among providers in weak labour demand areas for all staff to be working
weekends. Another finding from the specific domiciliary indicator list suggests that minimum
lengths of visits tend to be longer in medium than strong demand areas. Finally, IDP providers
in medium labour demand areas are more likely to have the Investors in People awards than in
strong demand areas.
For homes weak demand areas were less likely to provide time off for training than strong
demand areas and this relationship was significant.33 We also find a series of working time
indicators that are significant, including the overall working time index, XWT. However, the
directions of effects are mixed. The summary index for working time suggests working-time
arrangements are significantly better in providers located in strong than weak labour demand
areas (although only at the 10% level, table IV.10). Strong and medium labour demand areas
are significantly less likely to require all weekend working than weak demand areas. This is
demonstrated by the sub-index, SIWTWEN, as well as by the individual indicators on the share
of care workers working weekends (IWT4) and the recruitment requirement for weekend
working (IWT5) that also suggest that weak areas are more likely to impose this requirement.
On other measures, however, homes in weak labour demand areas score better – specifically,
on matching working time preferences, on long hours and 6/7 day working. Homes in strong
labour demand areas also score worse than medium or weak demand areas on two work
organisation variables: namely, the sub-index of the extent of discretion allowed in the job and
the summary index of work organisation (box IV.19).
Finally, we find that certain HR outcomes are associated with labour demand conditions in the
local labour market (box IV.20). Achievement of NVQ targets, captured in our sub-index of
training (SITRAINSKILLDEV), is negatively associated with labour demand: for homes it is
weak demand areas that have better training outcomes than those in medium or strong demand
areas but for IDPs it is more that strong demand areas have by far the worst outcomes. For
IDPs, medium labour demand areas were also significantly less likely to perceive problems of
absenteeism than was the case in weak or strong demand areas. As with our analysis of
variation in local authority commissioning arrangements (section IV.3.2), the results again
reveal no significant relationship between differences in labour demand and actual staff
turnover levels.
33
The scores on the 0-1 sub-index are 0.93 (strong labour demand) and 0.76 (weak labour demand), with a
significant difference at the 5% level (table IV.10).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
251
Table IV.10. Summary indices for homes and IDPs by labour market conditions (mean
values)
a. Homes
All
Strong
demand
Medium
demand
Weak
demand
0.69
(**W)
0.71
0.65
0.57
0.68
(**W)
0.91
(**W *M)
0.70
(**M W)
0.64
(**W)
0.69
0.57
0.64
0.67
0.97
(*S)
0.69
(**S)
0.50
(**S M)
0.65
0.59
0.54
0.60
(**S)
0.97
(**S)
0.64
(**S)
HR PRACTICES
XPAYLEVELS
Pay levels
0.61
XPAYSTRAT
XRRPRACT
XEMPDEV
XWT
Pay strategies
Recruitment & retention practices
Training & development
Working time
0.68
0.61
0.58
0.65
XWO
Work organisation
0.95
XHRPRACT
Index of all HR practices
0.68
Recruitment & retention
NVQ training targets
0.68
0.81
0.71
0.72
(**W)
0.62
0.76
(*W)
0.68
0.94
(**S *M)
All
Strong
demand
Medium
demand
Weak
demand
0.67
0.66
0.65
0.57
0.66
0.87
(* M)
0.68
0.61
0.63
0.66
0.56
0.68
0.72
(**S W)
0.64
0.59
0.66
0.57
0.63
0.57
0.88
(** M)
0.65
0.44
0.46
(**W *M)
0.50
0.73
(* S)
0.43
0.78
(** S)
HR OUTCOMES
XRROUTCOMES
XTRAINSKILDEV
b. IDPs
HR PRACTICES
XPAYLEVELS
XPAYSTRAT
XRRPRACT
XEMPDEV
XWT
XWO
Pay levels
Pay strategies
Recruitment & retention practices
Training & development
Working time
Work organisation
0.63
0.65
0.63
0.59
0.64
0.84
XHRPRACT
Index of all HR practices
0.66
Recruitment & retention
NVQ training targets
0.45
0.63
HR OUTCOMES
XRROUTCOMES
XTRAINSKILDEV
Note: Full details in appendix tables IV.A15 and IV.A.16. S,M.W are used to indicate significant difference from
strong , medium and weak demand areas respectively.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
252
Box IV.20. Significant differences among providers in HR outcome indicators by
labour demand (weak, medium, strong)
Standardised dataset
Homes:
SITRAINSKILLDEV:
IOUT1:
IOUT2:
training outcomes significantly better in weak than medium(10%
sig.only) or strong demand areas
shares of staff trained to NVQ2 significantly higher in weak
than strong demand areas
providers in high fee areas significantly less likely to meet
NVQ target than in medium (10% sig.only) or low fee areas
IDPs:
SITRAINSKILLDEV:
SIABSENT:
IOUT1:
IOUT2:
EWERC
training outcomes significantly worse in strong than
medium(10% sig.only) or weak demand areas
significantly worse perceptions of staff turnover in weak and
strong demand areas than in medium demand areas (latter
10% sig.only)
shares of staff trained to NVQ2 significantly higher in weak
than strong demand areas
providers in strong demand areas significantly less likely to
meet NVQ target than in weak demand areas
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
253
IV.5. Internal and external environmental factors associated with
good HR practices and HR outcomes
The above sections have investigated the way in which the quality of HR practices and
outcomes among homes and IDPs vary by a range of key factors, including organisational
characteristics (the size and ownership status for example, considered in part IV.2), LA
commissioning environment (level of fees and partnership orientation, for example, considered
in part IV.3) and local labour market conditions (considered in part IV.4). Considering each set
of factors in turn, our analysis so far suggests a number of significant associations between
these internal and external factors and the propensity of providers to adopt good HR practices
and enjoy good HR outcomes. To explore these associations further, this section reports the
results of multivariate statistical analyses. The first set of analyses was designed to identify the
factors associated with the adoption of good HR practices. The second set aimed to explore the
relationships between environmental factors, organisational characteristics and good HR
practices on the one hand, and good HR outcomes on the other.
IV.5.1. Exploring the factors associated with the adoption of good HR practices
In this section, our aim is to identify, using multivariate analysis, those factors that help explain
differences among homes and among IDPs in the quality of different HR practices –
specifically, pay practices, recruitment and retention practices, employee development
practices, working time practices and work organisation practices. In line with our over-arching
analytical framework for this project (figure I.1) our proposition is that these HR practices are
likely to be influenced by key external environmental factors that vary across provider and
local authority, namely the commissioning and contracting practices of LAs and local labour
market conditions. In addition, we know from our analysis above (section IV.2), as well as
from an extensive literature on the factors shaping the design of „HR bundles‟ (eg. Kepes and
Delery 2007, Purcell 1999), that organisational characteristics of the sample of providers are
likely to influence the ability and willingness of providers to adopt better HR practices. As
such, we also include factors such as size, ownership and profit-making status.
We carried out two types of multivariate analysis. First, we undertook a cluster analysis based
on the standardised dataset of HR practice indicators in an attempt to identify distinctive
clusters among homes and IDPs in their approach to HR. However, the cluster analysis
produced relatively unstable and not very distinctive groupings and is therefore not presented
here.
The second type of multivariate analysis consisted of a number of regressions. We used the
method of backwards regression. Details of this method along with explanatory notes for our
style of presentation of regression results are included in appendix IV.A3. In order to
investigate the effects of environmental and organisational factors on the different HR practices
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
254
we entered seven independent variables consisting of two LA commissioning variables (three
for homes), two labour demand variables and three organisational characteristics. Box IV.21
provides the full details of each independent variable. The labour demand variables consist of a
measure of local labour market demand and the median level of pay for all female part-time
workers in the local labour market, both derived from national statistics (see section I.7.1 and
appendix table I.A1 and appendix figure I.A1). There are also two LA commissioning
variables, the categorisation of partnership, mixed or cost-minimising LA (as derived in part II
above) and the actual fee level paid to the provider.
Box IV.21. Description of the dependent and independent variables used in the regressions on
HR practices
For each regression the effects of a number of independent variables were tested on the different
HR practices among homes and IDPs separately. The six HR practices variables, plus a summary
index variable, are as follows (see, also, box IV.6 above):
HR practices:
XHRPRACT: Overall summary index of HR practices
XPAYLEVELS: Index of pay levels
XPAYSTRAT: Index of pay strategies
XRRPRACT: Index of recruitment and retention practices
XEMPDEV: Index of employee development practices
XWT: Index of working time practices
XWO: Index of work organisation practices
And the seven independent variables (eight for homes) are as follows:
LA commissioning variables:
Details of measure:
partnership=3, mixed=2, cost minimising=1
Partnership LA
Actual £ fee levels
LA fee levels
For homes only, the proportion of service users
% dependency on LA
LA funded
Labour demand variables:
Local labour demand
Female part-time pay
Organisational characteristics:
Size
Ownership: national chain,
local chain, single establishment
Private for profit or voluntary
sector
EWERC
Scored 2 to 6
Actual £ median pay rates for locality
Actual size, number of employees
National chain is the reference category
Voluntary sector is the reference category
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
255
The regression results are presented from two models in each case. This is because there is a
high correlation between two independent variables, LA fee levels and local labour market
demand34. Consequently we ran the regressions twice - first with the LA fees but not labour
demand (model i) and again with the labour demand variable, omitting the LA fees variable
(model ii).
Tables IV.11 and IV.12 present the results for IDPs and homes, respectively. We only report
here the results for those indices of HR practices where the explanatory power of the
independent variables is relatively strong, using the measure of the adjusted R2 as a benchmark
(see IV.A.5).
For IDPs, several environmental factors and organisational characteristics appear to have a
significant association with the quality of HR practices (table IV.11). As anticipated, the local
authority commissioning policy appears to have a strongly significant influence on HR
practices. Both LA fee levels and the partnership orientation of the LA have a positive and
significant influence on HR practices. The partnership variable has a significant positive
association with the summary index of HR practices (model ii), the index for pay levels (model
i) and the index for pay strategy (model ii). And the LA fee level variable has a similarly
positive and significant relationship with the summary index (model i) and the pay strategy
index (model i). For IDPs, therefore, HR practices are significantly associated with the local
authority environment. Relations with a more partnership-oriented and high fee paying LA, as
opposed to a cost minimising and low fee payer LA, are beneficial for the adoption of better
HR practices.
Three organisational characteristics are also helpful in explaining the variance of HR practices
among IDPs. These are whether or not the IDP is a private profit-making organisation (as
opposed to a not-for-profit IDP), whether or not it is part of a local chain (rather than a national
chain) and the size of organisation. Holding all other factors constant, HR practices in profitmaking IDPs are inferior to those in the voluntary not-for-profit sector. The results presented in
table IV.11 suggest this result is significant for the summary X index (models i and ii) and for
the index of pay strategy (models i and ii), with confidence intervals of more than 99% in all
cases. Being part of a local chain, on the other hand, exerts a positive influence on the index for
pay strategy (model i) compared to IDPs that are part of a national chain. The size of workforce
of IDPs has a negative effect, insofar as larger IDPs are significantly associated with a worse
index for pay strategy (models i and ii).
Local labour market factors appear to play a less important role in explaining variance of HR
practices among IDPs. The variable for female part-time earnings exerts a significant positive
effect on the index for pay strategy (models i and ii), such that IDPs in areas of relatively high
female part-time earnings are more likely to register a better index for pay strategy.
34
LA fee levels are highly and positively correlated to local labour market demand factors, with a coefficient r =
0.66, which is also highly significant at p < 0.001.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
256
Table IV.11. The effects of environmental factors and organisational characteristics on
different indices of HR practices for IDPs
a. Summary index of HR practices (XHRPRACT)
i) With LA fees
Partnership LA
LA fee levels
-Single establishment
Private for profit
--
Coefficient
Significance
0.23
0.24
n.s.
*
0.17
-0.46
n.s.
***
ii) With labour demand
Partnership LA
-Female part-time pay
-Private for profit
Size
Coefficient
Significance
0.32
**
0.19
n.s.
-0.45
-0.169
**
n.s.
Coefficient
Significance
0.22
n.s.
0.18
-0.22
n.s.
n.s.
Coefficient
Significance
0.32
**
0.31
-0.19
-0.30
0.20
-0.37
**
n.s.
**
n.s.
***
Note: OLS regression, sample 50 (IDPs). Adjusted R2 of 0.32 (model i), 0.32 (model ii).
b. Index of pay levels (XPAYLEVELS)
i) With LA fees
Partnership LA
Female part-time pay
-Private for profit
Coefficient
Significance
0.334
0.13
**
n.s.
-0.20
n.s.
ii) With labour demand
Partnership LA
-Local labour demand
Private for profit
Note: OLS regression, sample 50 (IDPs). Adjusted R2 of 0.11 (model i), 0.12 (model ii).
c. Index of pay strategies (XPAYSTRAT)
i) With LA fees
-LA fee levels
Female part-time pay
-Size
Local chain
Private for profit
Coefficient
Significance
0.24
0.24
*
*
-0.30
0.23
-0.39
**
*
***
ii) With labour demand
Partnership LA
-Female part-time pay
Local labour demand
Size
Local chain
Private for profit
Note: OLS regression, sample 50 (IDPs). Adjusted R2 of 0.31 (model i), 0.31 (model ii).
For homes, the overall results of the regression models suggest that the same environmental
factors and organisational characteristics (plus the additional measure of dependency on LAs)
offer weaker explanatory power for the variance of HR practices (table IV.12). Moreover, the
LA commissioning environment appears to play a less significant role in influencing HR
practices in homes than in IDPs. This is most apparent for the summary index of HR practices
where we find neither the LA fee variable nor the LA partnership variable appear as significant
variables. These variables are nevertheless both significant (strongly significant in the case of
LA fees) for the index for pay levels for homes (model i). The regression suggests a 99%
confidence interval for the result that homes contracting with high fee paying LAs have a
significantly higher index for pay levels. The result for the LA partnership variable runs
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
257
counter to the result for IDPs since it suggests a negative association (albeit at a less strong
level of significance than our result for IDPs).
Like IDPs, a key variable is the private for-profit organisational characteristic. When a home is
a private sector profit-making organisation, its summary index of HR practices and its index of
pay levels are significantly worse than those for voluntary sector homes (models i and ii).
Another organisational characteristic, the size of the home, is negatively associated with the
index of pay levels, which compares to its negative influence on pay strategy for IDPs.
A key difference with the results for IDPs is that the local labour market factor of median
female part-time earnings emerges as an important variable for explaining the variance in the
summary index measure (models i and ii). The results suggest that the higher the pay for
women in part-time jobs in the local area, the better the overall measure of HR practices in
homes. This factor is not significantly associated with pay levels in homes (although it exerts a
positive influence in model ii), but does display a strongly significant association with the
index of pay strategy (models i and ii) and the index of recruitment and retention practices
(model ii); neither result is reported in table IV.12 due to the low overall explanatory power of
the regression models.
Table IV.12. The effects of environmental factors and organisational characteristics on
different indices of HR practices for homes
a. Summary index of HR practices (XHRPRACT)
i) With LA fees
-Female part-time pay
-Size
Private for profit
Coefficient
Significance
0.32
**
-0.15
-0.28
n.s.
**
ii) With labour demand
Coefficient
Significance
-0.13
0.25
0.24
-0.14
-0.27
n.s.
*
n.s.
n.s.
**
Coefficient
Significance
-0.21
n.s.
0.12
0.45
-0.14
-0.25
0.14
-0.35
n.s.
**
n.s.
**
n.s.
**
Partnership
Female part-time pay
Local labour demand
Size
Private for profit
Note: OLS regression, sample 52 (homes). Adjusted R2 of 0.15 (model i), 0.15 (model ii).
b. Index of pay levels (XPAYLEVELS)
i) With LA fees
Partnership
LA fees
--% dependent on LA
Size
Local chain
Private for profit
Coefficient
Significance
-0.29
0.50
*
***
-0.14
-0.31
0.19
-0.35
n.s.
**
n.s.
***
ii) With labour demand
Partnership
-Female part-time pay
Local labour demand
% dependent on LA
Size
Local chain
Private for profit
Note: OLS regression, sample 52 (homes). Adjusted R2 of 0.36 (model i), 0.41 (model ii).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
258
The regression results provide a surprisingly contrasting set of explanations for the two indices
of pay practices for IDPs and homes. In terms of the conventional measure of explanatory
power (the adjusted R2), the selected environmental factors and organisational characteristics
provide a relatively good explanation of the variance of pay levels among homes but a poor
explanation for IDPs. Indeed the opposite holds for the index of pay strategies where we only
report the results for IDPs since the regression models for homes had very poor predictive
power.35 For homes, three factors have a significant negative association with the index for pay
levels (model i) - being a private sector organisation (a 99% confidence level), being in a
partnership LA (only a 90% confidence level) and being of large size. LA fees work in the
anticipated opposite direction with higher fees having a positive and strongly significant effect
on pay levels. Two other variables remain in but are not significant: that is, being in a local
chain compared to a national chain which has a positive effect on pay and having a high
dependency on the LA for clients which has a negative effect. Model ii yields very similar
results except that the significance of the partnership variable disappears and local labour
demand has a strongly positive and significant effect, providing an effective substitute for LA
fee levels (as anticipated given its strong positive correlation).
These relatively plausible results, where fee levels and labour demand have strong positive
effects on pay levels, are not replicated for IDPs. Nevertheless, for IDPs partnership does have
a positive impact on pay levels (significant in model i). No other variables are significant;
median female part-time pay in the area has a positive effect on the pay level index (model i)
while being a private sector organisation has the usual negative effect (models i and ii).
In terms of the index of pay strategies, for IDPs we find the same negative influence of
organisational size and being a private for-profit organisation (strongly significant for models i
and ii) as we found for the index of pay levels for homes. Positive effects derive from the
labour demand variable, median female part-time earnings, along with LA fees and being a
local chain rather than a national chain. Partnership-oriented LAs also have a positive and
significant association in model ii.
The regression models generated poor levels of prediction for four indices of HR practices,
namely recruitment and retention practices employee development, working time and work
organisation. For all four indices the adjusted R2 measure consistently fell below 0.2.
In sum, these multivariate statistical results lend support to one of the main propositions of this
research, namely that the LA commissioning environment plays a strong and significant role in
shaping the quality of HR practices. IDPs that contract with high fee paying LAs and
partnership-oriented LAs display a better overall index of HR practices than other IDPs. And
for homes, while the LA commissioning environment does not appear to be associated with the
35
For the regression estimating the effects on the index for pay levels the adjusted R2 measures for homes are 0.36
(model i) and 0.41 (model ii) and for IDPs are 0.11 (model i) and 0.12 (model ii). For the regressions on the index
for pay strategies the measures of R2 for homes are 0.07 (model i) and 0.07 (model ii) and for IDPs, 0.31 (model i)
and 0.31 (model ii).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
259
overall measure of quality of HR practices, it has a strongly significant association with pay
levels such that those homes contracting with high fee paying LAs are more likely to register a
high index of pay levels than other homes. Conditions in the local labour market also matter;
homes in areas where the median pay for women in part-time employment is relatively high are
likely to provide high quality HR practices; for IDPs the same variable has an important,
similarly positive, association with the index of pay strategy. And finally, certain
characteristics of the organisation also facilitate our explanation of variance of HR practices.
The size of the workforce and the for-profit status appear to exert a negative effect on key HR
practices among both IDPs and homes, and IDPs that are local chains benefit from a higher
index of pay levels than IDPs that are part of national chains.
IV.5.2. Exploring the factors associated with good HR outcomes
In addition to exploring the factors associated with the quality of HR practices, we also used a
similar regression method to interrogate HR outcomes. Again, following the analytical
framework set out in part I of this report, we sought to test the impact of the external
environment – the type of LA commissioning and the local labour market context – and
organisational characteristics (as above). In addition, given that the bundle of HR practices
deployed in a particular organisation is likely to have a significant effect on the quality of HR
outcomes, we expanded the number of independent variables to include the seven indices of
HR practices (see appendix table IV.A17).
Drawing on the data from the telephone survey of providers, we constructed four measures of
HR outcomes that exploit both the subjective views of managers and the quantitative workforce
data. A first measure of recruitment and retention outcomes (XRROUTCOMES) is an
aggregate index of managers‟ subjective views about recruitment difficulties, staff turnover and
staff absenteeism. A second measure of training outcomes (XTRAINSKILDEV) combines
workforce data on the proportion of the care workforce qualified to NVQ level 2 and
managers‟ views about the future likelihood of their training at least 50% of their staff. The
third and fourth outcome measures are alternative quantitative measures of staff turnover – the
overall staff turnover rate for care workers (RT3) and the turnover rate excluding new recruits
(RT9).36
Tables IV.13 and IV.14 present the results for the first two measures of HR outcomes –
recruitment and retention outcomes and training outcomes – for IDPs and homes, respectively.
Across all regressions, the equation of association between the selected independent variables
and outcome variables provides a relatively low level of explanation; the adjusted R2 varies
from 0.10 to 0.29. Nevertheless, a number of variables appear to be significantly associated
with variation in these two HR outcomes.
36
While we have near complete data from providers for the first two outcome measures, it proved very difficult to
obtain reliable staff turnover data and as a consequence we have run regressions on smaller samples than we
would have liked – 37 IDPs and 45 homes.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
260
A first finding is that a key set of HR practices represented by the index of working time,
which reflects a mix of indicators such as the requirement for weekend and long hours working
and time off for training, exhibits a strongly significant and positive association with
recruitment and retention outcomes for IDPs (table IV.13). In both models (i and ii), this
finding suggests that the more IDPs are able to offer attractive (and less demanding) working
time schedules the better are the outcomes for recruitment and retention. Here is strong
evidence, therefore, that recruitment and retention outcomes can be shaped through attention to
what is perhaps one of the most important areas of HRM in IDPs given the complex nature of
work schedules. Two further significant variables are the organisational characteristics of size
and ownership. IDPs that are part of a local chain (model i) are significantly associated with
recruitment and retention outcomes that are higher than those of national chain providers. The
size of a provider‟s workforce tends to lower HR outcomes (models i and ii) with larger
providers significantly associated with lower scores for recruitment and retention compared to
smaller IDPs. As might be anticipated, strong local labour market demand appears to have an
adverse impact, with IDP managers in areas of strong labour demand more likely to register
negative views about recruitment difficulties and staff retention.
Table IV.13. The effects of environmental factors, organisational characteristics and HR
practices on indices of HR outcomes for IDPs
a. Index of recruitment and retention outcomes (XRROUTCOMES)
i) With LA fees
--Size
Local chain
XWorking Time
Coefficient
-0.31
0.22
0.35
Significance
**
*
**
ii) With labour demand
Coefficient
Significance
0.26
-0.29
-0.30
0.20
0.39
n.s.
*
**
n.s.
***
Partnership
Local labour demand
Size
Local chain
XWorking Time
Note: OLS regression, sample 50 (IDPs). Adjusted R2 of 0.20 (model i), 0.22 (model ii).
b. Index of training outcomes (XTRAINSKILDEV)
i) With LA fees
-LA fees
-Local chain
XPay Levels
XEmployee
Development
Coefficient
Significance
-0.31
**
0.29
0.15
0.14
**
n.s.
n.s.
ii) With labour demand Coefficient Significance
Partnership
-Local labour demand
Local chain
XPay Levels
--
0.17
n.s.
-0.49
0.27
0.14
***
**
n.s.
Note: OLS regression, sample 50 (IDPs). Adjusted R2 of 0.14 (model i), 0.20 (model ii).
Being part of a local chain is also significantly associated with better training outcomes among
IDPs (models i and ii). In other words, holding all other variables constant, IDPs that are
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
261
members of a local chain are more likely than national chain members to report high levels of
NVQ trained care workers and/or to have high expectations about the share of staff who will be
trained. The variable that registers the strongest significance is the local labour market demand
variable (a 99% confidence interval). As with recruitment and retention outcomes (and also
similar to our evidence on pay strategies, above), labour demand displays a negative
association: IDP managers in areas of high labour demand are significantly less likely to report
favourable training outcomes compared to IDPs in areas of weak labour demand. This might be
considered surprising since providers in areas of high demand facing strong competition for
labour might be expected to seek to improve the bundle of employment conditions on offer to
workers, including the opportunities for skill formation. However, what appears to be
happening is that where providers experience poaching of skilled workers, they are less
inclined to invest in training provision or their investments may not yield as high outcomes due
to higher rates of staff turnover. A further surprising result concerns the nature of association
between LA fees and training outcomes for IDPs. While our results for HR practices above
suggest a clear positive association with the level of LA fees to providers, here we find instead
a negative association. The result is confirmed by a correlation test on the two variables which
shows a negative correlation, -0.29, significant at the 95% level.
The results for homes suggest the same independent variables provide a very weak explanatory
model for the measure of recruitment and retention outcomes but a relatively strong
explanation for the index of training outcomes (table IV.14). Only one variable is significantly
associated with recruitment and retention outcomes among homes, that of workforce size. As
with IDPs, the larger the home the worse are managers‟ views about recruitment difficulties
and retention outcomes (models i and ii). More variables are associated with the measure of
training outcomes; also, the results are the same for models i and ii due to the weak explanatory
value of LA fees and local labour demand. Homes that are single establishments are
significantly more likely to be associated with better training outcomes compared with national
chains. Competition for female labour in areas with relatively high levels of median earnings
for part-time jobs has the apparent effect of reducing training outcomes among homes, much
like the labour demand measure for IDPs. And, like our results for IDPs, we find a strongly
significant (99% confidence level) and positive association between the training outcome and
the set of HR practices that constitute our index of work organisation. Thus, training outcomes
are likely to be better in those homes that have a positive approach towards giving staff the
time to deliver quality care and to develop relations with users, as well as the opportunities to
exercise discretion in improving the way they work. This may suggest that when time is
squeezed in general, so are opportunities for training.
The regressions for the third and fourth measures of HR outcomes, namely overall staff
turnover (RT3) and staff turnover excluding new recruits (RT9), draw on a more restricted
sample of respondents to the telephone survey(37 IDPs, 45 homes) due to difficulties in
obtaining detailed turnover data from all respondents (see section I.7 and III.2). The results
explain a very high proportion of observed variance among IDPs (the adjusted R2 measure is
greater than 0.60 for both measures) but a comparatively lower proportion of variance among
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
262
homes (with R2 values of around 0.20, similar to the above results).37 Corresponding with this
overall finding, the regressions suggest that many more variables are significantly associated
with measures of staff turnover in IDPs than is the case for homes. Table IV.15 presents the
results for IDPs with separate columns identifying those factors that are significantly associated
with a lower rate of staff turnover and those associated with a higher rate of staff turnover. We
only present the results for model i (with LA fees and without the variable for local labour
demand) since the results from model ii are equivalent for the total staff turnover measure and
very similar for the measure of staff turnover excluding new recruits. Full details of
coefficients for the independent variables are in appendix table IV.A20.
Table IV.14. The effects of environmental factors, organisational characteristics and HR
practices on indices of HR outcomes for homes
a. Index of recruitment and retention outcomes (XRROUTCOMES)
i) With LA fees
Size
X Pay Levels
X Pay Strategy
X Employee
Development
X Work Organisation
Coefficient
Significance
ii) With labour demand
Coefficient
Significance
-0.26
0.19
-0.19
-0.23
*
n.s.
n.s.
n.s.
Size
X Pay Levels
X Pay Strategy
X Employee Development
-0.26
0.19
-0.19
-0.23
*
n.s.
n.s.
n.s.
0.14
n.s.
X Work Organisation
0.14
n.s.
Note: OLS regression, sample 52 (homes). Adjusted R2 of 0.10 (model i), 0.10 (model ii).
b. Index of training outcomes (XTRAINSKILDEV)
i) With LA fees
Female part-time pay
Local chain
Single establishment
Private for profit
XPay Strategy
XRecruitment&Retention
practices
XWork Organisation
Coefficient
Significance
ii) With labour demand
Coefficient
Significance
-0.27
0.20
0.34
-0.19
0.17
-0.19
**
n.s.
**
n.s.
n.s.
n.s.
-0.27
0.20
0.34
-0.19
0.17
-0.19
**
n.s.
**
n.s.
n.s.
n.s.
0.35
**
Female part-time pay
Local chain
Single establishment
Private for profit
XPay Strategy
XRecruitment&Retention
practices
XWork Organisation
0.35
**
Note: OLS regression, sample 52 (homes). Adjusted R2 of 0.29 (model i), 0.29 (model ii).
A clear finding for IDPs is the significance of association between a range of HR practices and
the two measures of staff turnover (table IV.15). However, good HR practices appear to have
both positive and negative effects. For the measure of total staff turnover (RT3), four good HR
37
Unlike the above regressions, the models testing the staff turnover measures used indicators of HR practices
rather than the summary index measures. As such, many more independent variables were entered as potential
explanatory factors (see appendix table IV.A.20).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
263
practices are associated with lower staff turnover and three good HR practices are associated
with higher staff turnover. For the measure of staff turnover excluding new recruits (RT9) we
find a significant association between four good HR practices and low turnover and between
five good HR practices and high turnover. We must remember that the regression results only
provide a test of statistical association, not cause and effect. As such, the apparently
contradictory findings may be interpreted as demonstrating, on the one hand, that good HR
practices in many organisations tend to encourage relatively low rates of staff turnover and, on
the other hand, that high staff turnover may induce some organisations to improve their HR
practices (in an effort to improve staff retention).
Those practices associated with higher staff turnover among IDPs include regular uprating of
pay (RT3 only), paying for CRB checks, using formal recruitment methods, fitting work
schedules with employees‟ circumstances (RT9 only) and offering guaranteed hours contracts
(RT9 only). The indicator on formal recruitment methods could feasibly work in the opposite
direction to what we anticipated, if for example recruitment by word of mouth leads to more
committed staff. However, it is very difficult to come up with any explanations why the other
four practices could do anything other than tend to reduce staff turnover. This suggests that the
direction of cause and effect is likely to run from HR outcome to HR practice. In other words,
IDPs in contexts where staff turnover is a particular problem are more likely to implement
better HR practices in an effort to improve staff commitment to the organisation.
The HR practices associated with lower levels of staff turnover among IDPs are opportunities
for pay increases, payment for weekend work (RT9 only), recognising a trade union, selecting
new recruits who have care skills and qualifications (RT3 only) and provision of time off for
training. The first and third of these variables are highly significant (as defined by a 99%
confidence interval), such that those IDPs that offer opportunities for care workers to increase
their pay and those that recognise collective representation by a trade union are strongly
associated with lower rates of staff turnover.
The external environment and organisational characteristics play a lesser role in shaping staff
turnover compared to our other measures of HR outcomes presented above. Both larger size of
provider and the partnership orientation of the local authority only appear as significant in the
regression on the measure of staff turnover excluding new recruits where we find both
measures are associated with high staff turnover. The level of female part-time pay in the local
area is associated with relatively low levels of total staff turnover (RT3 only).
For homes the regression results suggest the relationship between HR practices and staff
turnover measures is more straightforward, albeit revealing a far smaller list of significant
variables (table IV.16). Just two indicators of HR practices are significantly associated with
staff turnover and in both cases the regression results suggest good practice is associated with
lower staff turnover. Just like IDPs, those homes where managers value caring skills and
experience among job applicants are more likely than other homes to enjoy low staff turnover.
For the measure of staff turnover excluding new recruits (RT9) a further indicator of HR
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
264
practice, the share of staff who regularly work weekends, also displays a significant
association. Here, the results suggest that those homes where a smaller proportion of care
workers regularly work weekends enjoy lower staff turnover, excluding new recruits.
Table IV.15. Factors associated with higher and lower measures of staff turnover in IDPs
a. Total staff turnover (RT3)
Factors that reduce staff turnover
Factors that increase staff
turnover
LA commissioning environment:
--
--
Labour market demand:
Higher female part-time pay (**)
--
Organisational characteristics:
--
--
HR practices:
Pay upgrading opportunities (***)
Recognition agreement with trade
unions (***)
Skills and qualifications desirable
among job applicants (*)
Time off from care duties to attend
training (*)
Regular uprating of pay (***)
Employer pays for CRB checks
(***)
Use of formal recruitment methods
(***)
b. Staff turnover excluding new recruits (RT9)
Factors that reduce staff turnover
Factors that increase staff
turnover
LA commissioning environment:
--
Partnership (***)
Labour market demand:
--
--
Organisational characteristics:
--
Larger Size (*)
HR practices:
Pay upgrading opportunities (***)
Extra pay for weekend work (**)
Regular uprating of pay (**)
Employer pays for CRB checks
(***)
Use of formal recruitment methods
(***)
Work schedules that fit staff
preferences (**)
Offering guaranteed hours contracts
(**)
Recognition agreement with trade
unions (***)
Time off from care duties to attend
training (**)
Note: see Appendix table IV.A20 for details.
As with IDPs, the local labour market appears to have limited association with variation in staff
turnover rates with the exception of female part-time pay which has a negative association with
total staff turnover. A distinctive result for homes is the differentiation between private for
profit organisations and voluntary not for profit organisations. The former are significantly
associated with higher levels of staff turnover on both measures, total staff turnover and
turnover excluding new recruits. For homes, therefore, the private for profit status is negatively
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
265
associated with three of our four HR outcome measures, a result that serves as a cautionary
warning to further advances in the role of private sector providers in delivery of health and
social care. The opposite association is found for the organisational characteristics of single
establishment (compared to national chain homes); single establishment homes are
significantly more likely to register lower staff turnover.
Table IV.16. Factors associated with higher and lower measures of staff turnover in
homes
a. Total staff turnover (RT3)
Factors that reduce staff
turnover
Factors that increase staff
turnover
LA commissioning environment:
--
--
Labour market demand:
Female part-time pay (**)
--
Organisational characteristics:
Single establishment (*)
Private for profit (*)
HR practices:
Skills and qualifications desirable
among job applicants (**)
--
b. Staff turnover excluding new recruits (RT9)
Factors that reduce staff
turnover
Factors that increase staff
turnover
LA commissioning environment:
--
--
Labour market demand:
--
--
Organisational characteristics:
Single establishment (*)
Private for profit (*)
HR practices:
Skills and qualifications desirable
among job applicants (*)
Lower % of staff regularly
working weekends (*)
---
Note: see Appendix table IV.A21 for details.
In summary, through the method of multivariate analysis this section has demonstrated a
number of statistically significant associations between factors in the internal and external
environment and the likelihood of IDPs and homes implementing good HR practices and
enjoying good HR outcomes. Our guiding framework for analysis was figure 1.1 from part I of
this report, which presents the key factors likely to influence the HR approach of care
providers. Several findings deserve highlighting. In relation to the adoption of HR practices,
the notion that the quality of LA commissioning (specifically higher fees and a partnership
orientation) is associated with better HR practices was confirmed for the summary index of HR
practices among IDPs and for the index of pay levels for homes. However, these positive
influences interact with several other factors that are more difficult to shape through strategic
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
266
policy action. In particular, conditions in the local labour market (especially the median level
of female part-time pay in the locality) display a significant association with the variation in
our measure of pay strategy practices among IDPs and the summary index of HR practices
among homes. Also, two organisational characteristics have a significant impact; smaller
providers and not-for-profit providers are more likely than larger providers and for profit
providers to implement good HR practices.
Our analysis of factors associated with HR outcomes points very strongly to the significant role
of HR practices, especially among IDPs, suggesting a possible linear cause and effect
relationship from internal and external factors through to HR practices and then to HR
outcomes. However, as we have argued, in some cases good HR practices may be induced by
pressure from local labour market conditions, in an attempt to reduce very high levels of staff
turnover. As a consequence not all good HR practices are associated with better HR outcomes.
Nevertheless, the results did highlight a significant association between IDPs‟ use of better
working time practices and better recruitment and retention outcomes, as measured by our
summary index of recruitment and retention conditions. Moreover, a bundle of good HR
practices in IDPs - good pay practices (opportunities for pay upgrading and paying a premium
for weekend work), trade union recognition, appreciation of care skills and care experience
when selecting new recruits and provision of time off for training – is associated with low
turnover among care workers. Those good HR practices what were found to be associated with
higher turnover included some basic employment conditions such as regular uprating of pay,
employer paying for CRB checks, fitting work schedules with employees‟ circumstances and
offering guaranteed hours contracts, suggesting that employers may only provide some of the
basic employment protections when required to do so by high labour demand and associated
turnover levels. Likewise, the association of formal recruitment methods with higher turnover
may reflect either a need to extend recruitment beyond informal networks in areas of high
demand or alternatively that more informal methods yields more stable and committed
employees.
Among homes fewer HR practices are identified as significant. Nevertheless, it is notable that
good work organisation practices, such as encouraging discretion in the job and facilitating
time to undertake caring duties, are associated with high scores on our training outcome
measure for homes. Two other HR practices are associated with lower staff turnover rates in
homes - the identification of care skills when selecting good recruits and the facility for some
staff to avoid regular weekend working.
For both homes and IDPs certain organisational characteristics also matter in explaining
variation in HR outcomes, namely: the smaller the provider the better the summary index of
recruitment and retention outcome; national chain providers appear to have worse training
outcomes than single establishment homes and than local chain IDPs; and not-for-profit homes
enjoy better staff turnover than for profit homes.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
267
IV.6. Providers’ views on the social care policy and commissioning
environment
IV.6.1. Providers‟ attitudes towards and experiences of local authorities
We asked providers how they would rate their relationships with the LA on a five point scale
from very good to very poor: 81% of care homes and 87% of IDPs regarded their relationship
as either very good or good and only 6% of homes and 6% of IDPs regarded their relationship
as poor or very poor, the rest remaining neutral. Despite this relatively low level of variation in
answers to the question, when we compute average scores by individual LA we do find some
relationship between our classification of LAs and providers‟ responses concerning their
relationships with the LA.
Table IV.16. Measure of providers’ satisfaction with LA relationship
(1-5 scale, very poor to very good)
IDPs
average score
Homes
average score
All
average score
Partnership LAs:
AH
LK
RN
UY
XD
4.6
4.3
4.5
4.7
4.2
4.5
4.2
4.7
3.0
4.4
4.6
4.3
4.6
4.4
4.1
Mixed LAs:
AD
OM
ON
RT
TE
4.5
4.3
4.2
5.0
5.0
3.5
4.7
3.5
3.3
3.0
4.0
4.6
3.9
4.3
4.2
Cost minimising LAs:
AW
HD
IL
RD
4.7
3.2
3.7
3.7
4.5
4.0
3.8
4.5
4.6
3.6
3.0
4.1
Providers in cost minimising LAs tend to display lower satisfaction with their relationship with
the LA for domiciliary care than among providers located in partnership or mixed LAs. 38 Table
IV.16 shows that among IDPs, the level of satisfaction was lowest in three cost minimising
LAs – HD, IL and RD. Scores for homes were more varied with three mixed LAs - ON, AD
38
The one exception is the cost minimising local authority AW where relationships with providers were reported
as relatively good.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
268
and RT – recording the worst scores but two of the cost minimising LAs also receiving below
average satisfaction ratings.
A number of quotes from the providers during the telephone interviews underscore the
complexities of categorising relationships with the LA. Some made a distinction between their
relationship with their immediate points of contact and their relationship with those making
policy decisions. Others pointed to differences in their relationships with different grades or
levels of staff.
The difficulty is it needs to be qualified because they have a contracts officer and we get on
very, very well with her. Her boss, great guy, get on well with him. But when we‟ve got an
issue we have absolutely no way into the council to make any difference. …..when we‟ve got
particular issues they don‟t want to know. ……So that‟s the difficulty of dealing with a public
authority. You just can‟t get there to where the decisions are made. The bureaucracy doesn‟t
allow you to do it. (ON.D.1 DN).
I think its best to speak of the last couple of years because before that it wasn‟t so wonderful, I
think that sometimes its about there are some very capable people there and some team leaders
who aren‟t so good, so probably some problems with communication following things up and
that is often around safeguarding issues. (RD.D.2.CL).
Another distinction made was between the personal relationship and their satisfaction with
funding:
With regard to funding when I said we had a good relationship, well they don‟t meet our
funding requirements. (RD.HN.4.C.N).
Work relationship is fine, but it is the funding issue. We are the lowest paid authority. (IL. H.
4).
Past poor relationships were apparently forgiven if new policies provided more financial
support:
I think it‟s probably a lack of support in the past. But what has improved is training. It‟s had a
huge impact for us because it‟s saved us a fortune off our training budget. (RD.H.3.A.L).
Some providers clearly had a negative view of the role of the LA:
I think the experience we get in nursing homes is it‟s kind of almost like a policing of us rather
than a supportive, or work together. (ON.HN.1 BS).
Yet others attributed problems to the policies of central government rather than the LA itself:
But then again, they‟re on a budget aren‟t they? It‟s the government, it‟s not them. (ON.D.2
AS).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
269
Specific problems identified ranged from a tendency to impose the latest policy fads or
concerns on providers, regardless of its relevance or priority, to insistence on contract
compliance even when LAs had been informed of recruitment difficulties and staff shortages.
[Its] pressures that senior management put onto you, you know it‟s other people‟s agendas …
So no matter what you‟ve got planned if they say, because of an issue in another unit, every
member of staff has to be refreshed in, oh I don‟t know „Violence at work‟ …then your training
plan just goes out of the window. It means that you‟ve got to get everyone on that training.
(HD.HN.1.C.LV).
[It‟s the] contract – [there‟s] no cap on it. They are aware we have recruitment problems and
we don‟t have enough staff, but they refuse to stop forcing work on us because it is part of our
contract. In other words, it‟s, „You have the contract and it is your problem‟. (HD.D.1).
Recurring themes among the national providers in discussing their relationships with LAs were
first the variation between LAs, with only one national provider saying they did not find much
variation. Others stressed differences in approach to communication; differences in the
administrative details of contracts and commissioning practices (leading to great waste and
duplication); and above all differences in pricing strategies. These include differences in the
fixed fees:
Local authorities will sometimes fix in the contract what the price should be. So I suspect they
haven‟t necessarily market tested whether you can get care workers at some of those rates. So
there are some anomalies there. You‟d like to think that before they came up with the charge
rate they maybe had a view of what they saw in terms of care worker retention and pay. But I
wouldn‟t like to say that always happens…… Managing Director, NATDOM4
And differences in their implementation of policies which affect the overall profitability of the
business:
If you look at some of the requirements, and this is where it gets implicated by local authorities,
the advent of call monitoring, electronic call monitoring. ….Some councils have a greater
rigour to that. Some councils will tell you when they expect the calls to be done. So there‟s
degrees of flexibility, or not, in there. I think the other thing is some local authorities will pay
mileage and visit fees, and some won‟t. Some will fund all sorts of training to support you.
Increasingly that‟s diminishing. You see less and less people willing to fund care worker
training so it‟s down to the providers really. (Managing Director NATDOM4).
Some LAs give us the contract then move the goalposts, for example by introducing call
monitoring. It is a difficult thing to do mid-contract. Some dictate to you what system to use –
it is always a strain on the budget. Because of the different LAs, we find it difficult to
standardise. (National Recruitment Manager, NATDOM3).
Some aggressive pricing strategies were, according to some national providers, jeopardising the
supply of care services. Some national providers stressed that although they would
accommodate to local demands they would not do so at the expense of minimum standards set
by the company.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
270
So for us it‟s not about flexing completely. It‟s actually about making sure that we have got the
safeguards we want in our business. So we will always enforce the minimum standards that we
see and hopefully they‟re higher or the same as the local authority requires. …We know we can
be efficient and competitive in terms of our price, but for us, we will walk away from contracts
if we think that the local authority is going for cheap and cheerful and basically putting lives at
risk. (Managing Director, NATDOM4).
Some LAs were said to be inconsistent between quality and price, expecting „the highest level
of service but want[ing] to pay per minute‟ (Managing Director, NATDOM5). A further
problem identified was that some LAs wanted to,
…run your business for you. They insist on the structure of the branch. They tell you you have
to have certain people in place, and if you don‟t they reduce the hourly rates that you claim.
Micro-management and minute billing. We can only claim for every minute of care we provide
and we can only pay the carers those minutes. (National Recruitment Manager, NATDOM3).
One specific way in which LAs seek to develop relationships with providers is through
provider forums. Most LAs hold provider forums and this is confirmed by the finding that only
9% of independent providers said their LA did not hold a providers‟ forum. Table IV.17 shows
that of the 88 providers who responded to a question about their own attendance at forums,
65% said they always or mostly attended the forums. There was a notably lower attendance
among the providers located in our „cost minimising‟ LAs than was the case for the
partnerships or the mixed category LAs. Of the 77 who expressed a view on the usefulness of
the forums, around 65% considered them to be very useful or useful. Those located in cost
minimising LAs were most likely to consider them not very useful or a waste of time,
accounting for 18% of all providers in these LAs.
In one LA, LK, the provider forum had apparently broken down and relations between the
independently run homes and the LA had only been restored through formation of an
association of independent care providers to re-establish dialogue with the LA. Members of the
association were now invited to sit on committees and had opportunities to communicate with
councillors:
We have managed to get very good dialogue with them; we communicate a lot better. From
time to time, there might be a few difficulties where they reject things out of hand, but on the
whole, it is innovative, there are not many counties that have this sort of joint partnership. I sit
on the scrutiny committee of the council for special care and that is a voice – it is useful for
informing councillors about what is actually going on. In the past, councillors hadn‟t a clue.
(LK.HN.1 BS).
One national provider commented on the very different approaches to managing forums across
LAs reflecting different degrees of interest in communication with and listening to the concerns
of the care providers:
We deal with some 30 different authorities and I see 30 different examples of local authorities.
What I would call good authorities are the ones who organise regular provider forums. They
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
271
consult all the providers, pretty much in advance, or at least keep them informed as to what
they‟re thinking. Also [they] facilitate meetings between providers, so that they can hear a
consensus view. And [they] are quite happy to accept challenges from providers, and also to
listen. And quite often you find that over a period of time they implement what you have said.
…Then there are the authorities who pay lip service to it. Just try and do the minimum to meet
up with CQC requirements. Say, „Oh yes we are consulting and blah, blah, blah‟ - whatever.
And then there are others who just don‟t do anything. And yet at the same time they impose
things without any commercial awareness as to the impact this would have on the providers. ...
They don‟t seem to connect up the building of the capacity and the building of the service, with
the changes in the rules and the regulations. (Managing Director, NATDOM5).
Table IV.17. Provider views about LA providers’ forums
a. Frequency of provider attendance
Always
Mostly
Occasionally
Never
Partnership LAs
50.0%
26.5%
14.7%
8.8%
Mixed LAs
44.8%
17.2%
20.7%
17.2%
Cost minimising LAs
32.0%
20.0%
24.0%
24.0%
All LAs
43.2%
21.6%
19.3%
15.9%
Note: Total responses 88, missing 17 (excluding LADPs).
b. Usefulness of forums
Very useful
Useful
Sometimes
useful
Not very
useful
Waste of time
Partnership LAs
23.3%
33.3%
36.7%
3.3%
3.3%
Mixed LAs
32.0%
44.0%
20.0%
0.0%
4.0%
Cost minimising LAs
27.3%
36.4%
18.2%
13.7%
4.6%
All LAs
27.3%
37.7%
26.0%
5.2%
3.9%
Note: Total responses 77, missing 28 (excluding LADPs).
The comments confirm the prevalence of very different approaches to building relationships
with providers identified in our own interviews with the selected LAs.
Providers were also asked what, if any, changes in the LA‟s commissioning and contracting
arrangements would do most to assist them in recruiting and retaining a stable and motivated
workforce. A list of options was provided (three items common to both homes and IDPs and a
further two items added for IDPs) and multiple answers were accepted. A rise in LA fee levels
was the most popular option, chosen by 55% of homes and 58% of IDPs. This view was also
forcibly endorsed by at least one manager of an LADP.
For the life of me I do not know how you can offer a service for somebody when all you receive
is ten and a half quid an hour. … A woman set up a cleaning firm in [this area]. She charges
twelve quid an hour at the front end. Her office is her living room. There‟s only her and her car
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
272
and she has a number of cleaners that she sends out. For that she charges twelve quid an hour.
We‟re asking people to provide personal care services, with all that that involves, at ten and a
half quid an hour. We have to pay a lot more, frankly, if we want a good quality service that
meets the national minimum standards in a robust way that provides the level of care that
people deserve. We have to pay a lot more for it. (AD.DIH1.DP).
The option of more variation in price by service user or for homes by type of accommodation
was selected by 31% of homes and 34% of IDPs. One home called for „much higher pay rates
for those with mental health problems‟ (RD.H.3.A.L). However, one IDP felt everyone was
underpaid so that the only way forward was better funding all round.
No I think care, whether we‟re going in to give somebody a bath or care to someone being
commoded or providing support to someone through cooking and domestic help, it all places
the same demands on carers, the same training levels and the same conditions that they are
working under, so it needs to be better financed. (RD.D.1.C.S).
There was more variation in the third option – a more integrated approach by the LA to service
delivery- with 37% of IDPs selecting this change compared to only 21% of homes. The
additional items asked of the IDPs were also selected by over a third of IDPs: that is, there was
fairly widespread support among providers for more scope to determine how care is delivered,
higher guaranteed volumes of work and more time for a service user. However, those not
selecting the option on guaranteed volumes may have sided with the provider who said that
block contracts were squeezing out space for those not selected to be block contractors or
preferred providers.
Some more specific issues were raised under the „other changes‟ category. Some of the
comments related to specific policies of their LA: for example, one home (TE.H.2) was
concerned about a five to ten year lock-in written into their contracts. One home asked for
„More clarity, openness and honesty‟ (XD.D.2). Among IDPs, the concerns related to the lack
of attention to people in the tendering process - according to the respondent at one IDP
RN.D.3) the LA commissioner needed to follow the guidelines in this respect - and others
talked about the lack of attention to quality of life of users and the fact many users were lonely.
One provider thought LAs should pay mileage (ON.D.4) and another that they should be
speedier in their response (RT.D.2). Some providers asked for changes that went beyond the
individual LA; for example one home called for registration for care staff to raise their profile
(XD.H.3) and others raised concerns about complexities of the funding arrangements or about
restrictive regulations on admissions to care homes.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
273
IV.6.2. Providers‟ attitudes towards and experiences of monitoring systems
Through our telephone survey, we asked providers about their experience of monitoring
systems. Questions were designed to cover both the role of the LA in monitoring and of the
role of Care Quality Commission (previously known as the Commission for Social Care
Inspection).
Role of the LA in monitoring providers
The providers were asked what importance they thought the LA placed on provider HR
policies (table IV.18). Around 43% said that it was very important and a further 44% somewhat
important, leaving only 14% of respondents who said their LA attached no importance to it.
This share was highest among the mixed category of LAs and it was the providers in the cost
minimising LAs that had the highest shares saying the LA considered their HR practices to be
very important – at 50%. One provider in a cost minimising LA, however, made the comment
that there may be greater interest in compliance with regulations than in supporting the
providers to improve their HR practices.
Well that‟s it they … love lots and lots of paper work and love giving lots of rules and
regulations but then never support you to obtain them or keep up with them or stuff. We have
tendered for work with them but sometimes its just unrealistic in terms of demands made by
them. (RD.D.1.C.S).
Table IV.18. Provider views about the importance the LA places on providers’ HR
practices
Very important
Somewhat important
No importance
Partnership LAs
36.0%
56.0%
8.0%
Mixed LAs
44.8%
34.5%
20.7%
Cost minimising LAs
47.4%
42.1%
10.5%
All LAs
42.5%
43.8%
13.7%
Note: Total responses 73, missing 32 (excluding LADPs).
The survey also included a question about whether the provider‟s LA was directly involved in
monitoring or whether the LA relied on the Care Quality Commission to monitor its providers.
Table IV.19 shows that around four fifths of providers said their LA was involved directly and
just one fifth said the LA relied completely on the CQC. The involvement in monitoring was
somewhat higher in the partnership LAs at 85% but LA involvement was higher in costminimising than in mixed LAs.
Comments from the providers suggest that the amount and frequency of monitoring varies and
that LA practice may be inconsistent over time:
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
274
[The LA] does do some monitoring. … They come in and check policies and procedures. but
that‟s probably happened just once in the last five years. (RD.H.3.A.L).
[The LA] had stopped active monitoring, but now restarted. (LK.D.3 DS).
Certainly there is a lot of monitoring. [The LA] is very much better than they were I have to
say. (OM.D.2.DN).
They are very strict and visit the branch regularly and take away care workers‟ time sheets for
audits regularly. (HD.D.1).
[The LA] doesn‟t do any [monitoring], but I think that it will do in the future. We have had to
send our policies, procedures, training policies, etc. (TE.H.4 AS).
Table IV.19. The role of the LA and CQC in monitoring providers
LA direct role
CQC only role
Partnership LAs
85.4%
14.6%
Mixed LAs
71.4%
28.6%
Cost minimising LAs
81.5%
18.5%
All LAs
79.6%
20.4%
Note: Total responses 103, missing 2 (excluding LADPs).
Many provided examples of the types of monitoring that LAs were engaged in. The areas that
were mentioned frequently were recruitment processes and turnover or training. Only one
mentioned equality and diversity policies and some implied that most of the monitoring was
done at the tender and contract stage. One provider said that not only was the LA involved a lot
in monitoring HR, including looking at their HR policies, but they had also provided them with
access to some advice from an employment law firm
For some providers the involvement of the LA as well as CQC was too much:
The day of the cancelled interview [with the research team], they were in all day. I wish they
would talk to each other [CQC and LA], it is exhausting. (IL.H.4).
There is too much inspection. The company come in, the LA, CQC. What I want from the
company is for them to say that I am doing OK, and leave me. CQC is fine, but sometimes it
seems as though there is too much. (IL.H.3).
These views were held by some national providers who saw the active involvement of LAs in
quality monitoring as unnecessary duplication and increasing problems at defining and
adopting a consistent policy.
I think some of them [LAs] decide to have a much greater involvement with inspection of the
services that they‟re commissioning, which we think is duplication because there is the CQC
that is charged with making sure quality is right in everything. (Corporate Services Director,
NATHOME2).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
275
Where we can have issues is around, from an HR perspective, it is around some of the policy
stuff. Whereby we‟re having to double train people because we have, say, issues around,
someone has a separate medication policy, and we from a CQC perspective have to do it one
way, and then we have to do it again another way from a local authority perspective. So it can
be a little bit of a struggle sometimes, where the local authority will insist on a certain type of
training taking place, which is not necessarily part of the National Minimum Standards or
anything mandatory. (HR Director, NATHOME5)
The results presented in table IV.20 suggest that over 70% of providers were satisfied or very
satisfied with CQC quality standards but that satisfaction rate fell to below 58% when asked
about satisfaction with CQC quality rankings. A very high share of those ranked one star were
unsurprisingly dissatisfied and nearly 27% of those ranked 2 star were also not satisfied. Even
7% of the 3* establishments expressed dissatisfaction.
A repeated theme among the providers was a concern over the consistency of CQC ratings.
Inconsistency was attributed both to variability among inspectors and to false impressions due
to snapshot inspections.
Well I think that the standards are a very good thing but I‟m not altogether sure about the
Commission because I think that they‟re quite sort of inconsistent. I think that some of their
inspectors are inconsistent but the standards are good. (UY.D.2.B.S).
I think it would be better if it was done over a length of time rather than just a snapshot of that
day that they‟ve come in. (HD.HN.1.C.LV).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
276
Table IV.20. Providers’ attitudes towards the Care Quality Commission
a. Satisfaction with the CQC’s set of quality standards
Very
satisfied
Satisfied
Neutral
Dissatisfied
Very
dissatisfied
Partnership LAs
28.3%
52.2%
13.0%
2.2%
4.4%
Mixed LAs
21.1%
42.1%
26.3%
5.3%
5.3%
Cost minimising LAs
32.3%
35.5%
19.4%
9.7%
3.2%
All LAs
27.0%
44.4%
19.1%
5.2%
4.4%
Note: Total responses 115.
b. Satisfaction with the CQC’s system of quality ranking
Very
satisfied
Satisfied
Neutral
Dissatisfied
Very
dissatisfied
Partnership LAs
19.6%
37.0%
26.1%
6.5%
10.9%
Mixed LAs
18.4%
34.2%
29.0%
10.5%
7.9%
Cost minimising LAs
25.8%
38.7%
19.4%
12.9%
3.2%
All LAs
20.9%
36.5%
25.2%
9.6%
7.8%
Note: Total responses 115.
c. Belief that the individual provider star ranking is fair
Yes
No
1 star rating
28.6%
71.4%
2 star rating
73.2%
26.8%
3 star rating
92.6%
7.4%
All providers
72.3%
27.7%
Note: Total responses 112; missing 3.
Similar concerns over consistency were also expressed by national providers (see box IV.22).
A further problem was the focus of the CQC on those rated adequate or poor with less frequent
inspections for those seeking to improve from good to excellent; for some national providers
this made it difficult to apply pressure to raise standards. Some of the national providers were
operating their own audit and monitoring systems both to raise standards and to ensure that
their homes or IDPs were ready for CQC inspections (box IV.22).
Suggestions from the telephone survey respondents as to how to change or improve CQC
monitoring included the following:
Less attention to paperwork and more attention to people - „particularly for people who don‟t
speak [they need to] use more skilful communication with people and their families.‟
(RD.D.2.CL);
More focus on the needs of users through „sight of detailed care plans‟ (AH.D.3.CN);
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
277
More focus on building relationships, „to encourage organisations to meet standards and to
work together with the Care Quality Commission to aim for higher standards right across the
board‟. (OM.D.2.DN);
More „listen[ing] to what we are saying‟ and „less tend[ency] to treat all the homes the same.‟
…. so that „what is deemed necessary in a big home where there might be different staff on
each day‟ might not be in a small home where managers see and talk to their staff every day.
(RD.H.3.A.L);
Change to the ranking system to use the 5* system used by the hospitality industry on the
grounds that „I wouldn‟t stay in a two star hotel‟ (LK.H.3 BL).
Box. IV.22. The views of national providers towards care standards
i) Burden of regulatory compliance
The challenge is to meet the increasing expectations and burdens of regulations, of training, within
a fee rate which is declining, or not increasing at the same rate. (Managing Director, NATDOM5).
ii) Effectiveness of CQC
I think they are in such a state of flux. I think what I‟m not satisfied about is the lack of consistency.
Different inspectors have different approaches, so that‟s one thing. Not satisfied at the rate at
which the inspectors are changing. (Managing Director, NATDOM5).
We actually go quite far beyond CQC standards through quality. So we like to feel that because
we‟re doing that we should be pretty much compliant with anything CQC would do. I think that‟s
been borne out by the results of our audit inspections. I guess the complexity of that is that
sometimes you are dependent upon the inspectors. Good day, bad day, or focus [on a ] particular
area. (Managing Director, NATDOM4).
I think for us, we have our internal audit team as well looking at different things. So for us, the
combination of the two works well. Our internal quality audit is, I think, harder than the CQC was
and I think, in terms of people and motivation, the thing that‟s the most difficult with CQC is that
they‟re not going to be assessing their good and excellent services. They‟re focusing on the poor
and adequates, which means it‟s difficult to get a good service to excellent at the moment. (HR
Director, NATHOME3).
The biggest problem we have is inconsistency. We have what I think is a relationship provider,
which is a senior manager at their headquarters. But that person has no executive power over the
inspectors all over the country. And we will get an inspector in one part of the country saying you
know, you‟ve got to do xyz because regulation say so. And we‟d say, well that‟s not how we read it,
with all due respect, it‟s not like how the CQC read it, and sometimes it will lead to a debate and
others it will lead to, „I‟m inspector here, you do as you‟re told‟, or whatever. (Corporate Services
Director, NATHOME2).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
iii)
278
Activities to improve outcomes
What we‟ve done is we‟ve now got a regulation team which helps managers. Sometimes we don‟t
evidence the good things we do well and I think it‟s taking that turnaround of „you‟re good at this;
lets show it‟ and we sometimes don't have the evidence, because it‟s very evidence led and they‟re
constantly trying to move to an objective type of regulation. But it‟s getting our managers and
supporting them to get the training records. Sometimes it is happening but it‟s how you evidence the
things that are happening. (Recruitment Director, NATHOME1).
Every region now has a head of service quality and they have reporting to them, a team of service
quality inspectors too, who do exactly that; they go into the homes, inspect them and rate them
internally and help them come up with action plans to address any issues, and then there‟s a team of
service quality advisers who actually go into the homes and help them implement plans, coach and
support the home manager. … Rather than waiting for CQC to come and tell us here‟s a problem,
we‟re aiming to identify those kinds of things for ourselves and then we can take action so that by
the time CQC come we can either say, „Yes, we know we‟ve got problems and this is what we‟re
doing about them‟, or we‟ve actually tackled them and in fact CQC are looking at something rather
better. (Group HR Director, NATHOME4).
In addition to asking providers about their satisfaction with care standards, we also asked them
to identify which of the CQC standards they found the most challenging. Table IV.21
aggregates all the answers covering the four most challenging standards for homes and IDPs
separately. This reveals that the care standards that are the most difficult to meet vary between
homes and IDPs, related to the nature of the service. Thus, for IDPs the most challenging
standard was to ensure „service users are protected from abuse, neglect and self-harm‟,
presumably as a consequence of the fact that IDP service users are located in their own homes
and are only seen intermittently and by mainly one member of staff. For homes the most
challenging standards is ensuring that „service users find the lifestyle experienced in the home
matches their expectations and preferences and satisfies their social, cultural, religious, and
recreational interests and needs‟. The difficulty in meeting this standard in part relates to
differences in expectations among service users as one home manager commented:
I don‟t find any of them [care standards] challenging; this is my job, so professionally I should
be able to meet them. Maybe the one … to do with their [users‟] perceptions. They may expect
to be tied to the bed and fed bread and water, or [they may] expect three staff in the room,
chandeliers and champagne for tea (IL.H.4).
The standards that relate to staffing issues - including training, skills or performance appraisal
(asterixed in the table) - were mentioned only by a minority of providers, accounting for 16 out
of 92 responses among homes and for 14 out of 96 among IDPs. But of course many of the
standards are implicitly dependent upon quality care staff, especially in the IDPs.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
279
Table IV.21. CQC care standards most difficult to meet for homes and IDPs
(aggregate scores for the top four most difficult to meet care standards)
Home care standards
Service users find the lifestyle experienced in the
home matches their expectations and preferences
and satisfies their social, cultural, religious, and
recreational interests and needs.
Service users, where appropriate, are responsible
for their own medication and protected by the
home‟s policies and procedures for dealing with
medicines.
Service users‟ health, personal and social care
needs are set out in an individual plan of care.
Staff are trained and competent to do their jobs*
Rank
(no. of
homes)
1 (18)
Domiciliary care standards
Service users are protected from abuse,
neglect and self-harm
Rank
(no. of
IDPs)
1 (18)
2 (10)
Policies and procedures on medication
and health related activities protect service
users
2 (16)
3 (7)
Service users receive a consistent, wellmanaged and planned service
The risk of accidents and harm happening
to service users and staff is minimised
Service users know and benefit from
having staff who are supervised and
whose performance is appraised
regularly*
Service users treated with respect, valued
and right to privacy upheld
3 (13)
6 (5)
Care needs individually assessed
7 (6)
6 (5)
Health, safety and welfare of service users
is promoted and protected
The well-being, health and security of
service users is protected by the agency‟s
policies and procedures on the recruitment
and selection of staff
Service users know that staff are
appropriately trained to meet their
personal care needs*
Service users, relatives and
representatives are confident that their
complaints will be listened to, taken
seriously and acted upon
8 (5)
3 (7)
Service users‟ needs are met by the numbers and
skill mix of the staff*
5 (6)
Service users assessed and referred solely for
intermediate care helped to maximise their
independence and return home.
Service users are helped to exercise choice and
control over their lives.
The home is run in the best interests of service
users
Service users receive wholesome, appealing,
balanced diet and pleasing surroundings at times
convenient to them
6 (5)
No service user moves into the home without
having his/her needs assessed and assured that
these will be met.
The health, safety and welfare of service users and
staff are promoted and protected
9 (4)
Service users are in safe hands at all times
Service users‟ financial interests are safeguarded
Service users maintain contact with
family/friends/representatives and the local
community if they wish.
Service users are protected from abuse
Service users feel they are treated with respect and
their right to privacy upheld.
Service users‟ health care needs are fully met
Service users are supported and protected by the
home‟s recruitment policy and practices
Service users live in a safe, well maintained
environment
Service users live in a home run and managed by a
person who is fit to be in charge, of good character
and able to discharge his or her responsibilities
fully
12 (3)
12 (3)
14 (2)
9 (4)
9 (4)
14 (2)
14 (2)
14 (2)
18 (1)
18 (1)
18 (1)
Note: * Care standard relating directly to HR issues such as staffing levels, skills, training and performance
appraisal.
EWERC
4 (10)
5 (9)
6 (7)
8 (5)
8 (5)
11 (4)
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
280
IV.6.3. Providers‟ attitudes towards, and experiences of, policy developments
likely to affect social care
Providers were asked to comment on two policy developments with potential implications for
the social care market. One was whether the new regulations limiting non EU migrants would
affect their ability to recruit sufficient or sufficiently skilled care staff. Most answering said
either that they had not used migrants or that, while it would have been of concern in the past,
the recession meant it was no longer a key issue. However, one or two providers expressed
rather high levels of concern. For example, one home said it was „our biggest concern‟
(LK.HN.1BS) and another home in the same area had engaged a solicitor to help them obtain
the right certification to enable them to continue to recruit. One home in the HD LA was
concerned that some of their existing staff would fail to get the right number of points required
to stay on.
IDPs were also asked about what problems or opportunities they anticipated as a result of an
increase in direct payments and individual budgets. Some saw this as an opportunity to
improve the quality of care as users might be able to trade volume of care hours against quality:
I think too many LAs focus far too much on price rather than quality, as much as they say that
they do, we know that they don‟t. I think it‟s really sad that the local authorities are in that
situation, they can‟t choose the best care because they can‟t afford the best care so that needs
to change. I think the government needs to recognise that people deserve to choose. Some may
want more hours at a lower price and lower quality of service and if that‟s what they want then
that‟s fine. But equally they should be given the opportunity to choose better quality, maybe less
hours but a more costly service because that‟s what they want for their circumstances, at the
moment people are not getting that choice. (OM.D.2.DN).
Two national providers of domiciliary care also talked about the need to upgrade the quality of
both their staff and services:
Traditionally a lot of domiciliary care provision has been set up around national minimum
standards and that‟s the scope of the ambition. For us, what we need to do is try to look further
forward and to adjust our workforce and the skills of our workforce and the way we reward our
workforce and develop them in accordance with the provisions of personalisation. (HR
Director, NATDOM1).
As a company we are looking at changing the way we recruit - having service user involvement
in recruitment and training - and the services we provide [we are] going to have to extend and
offer more variety. We have a company strategy on this. (National Recruitment Manager,
NATDOM3).
By and large concerns over personalised budgets were prefaced with comments that the
providers - both local and national - supported the idea of personalisation in principle but they
had a range of concerns over practicalities. A first set of concerns related to poaching of staff
and guarantees of payments as some had already experienced difficulties in extracting payment
from individual budget holders.
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
281
Another one we had and we used to provide a serious amount of care for her, two carers four
times a day. Very, very difficult to get payment off her. Direct payments team weren‟t interested
whatsoever. They constantly advertised behind our backs for PAs for her. We lost one of our
staff to her. We‟d CRB‟d her, inducted her, introduced her, we lost her. So that was another
one. (ON.D.1 DN).
I think it‟s just the sheer organisation of getting the money in, [compared to] having a block
contract where we invoice once a quarter, same amount every quarter. (RD.D.2.CL).
These concerns were also echoed by the national providers:
And because if the cash is given to the individual and the individual has to spend the cash and
pay the providers, and then the providers have to take a credit risk on that. Whereas if I‟m
dealing with London Borough XX for example, I can - at least I know that if I‟ve done a proper
bill they will pay me, I don‟t have to worry about the local authority going bust. (Managing
Director, NATDOM5).
Other concerns related to the potential for abuse, if families took the money but didn‟t provide
the care and the problem of an individual personal assistant providing cover. Some were
concerned about personal assistants not being trained or subject to CRB checks, an issue also
taken up by national chains who were concerned about the lack of minimum standards for
personal assistants and the unfairness of holding agencies responsible for meeting a whole set
of standards while allowing individuals to take up work under personalised budgets without
training or CRB checks (see box IV.23). National providers raised another set of concerns over
how the system was being implemented and administered in practice, including the differences
in approach between LAs and the consequent complexities, administrative costs and shifting of
responsibilities onto users or agencies.
Box IV.23. National providers’ views about the implementation of personalised budgets
i) Actions by LAs
As a principle I have no quibbles with [direct payments]. The problems I envisage are the rates of
payments. Some of the local authorities are paying, in terms of direct payment, the rate is lower than
what they would pay an agency. … So if you are paid less than, you have a choice. Either you have to
top up the £11 to buy the service from the agency or you have to employ a personal assistant – a
local, your neighbour or whoever is doing that. (Managing Director, NATDOM5).
The challenge is that every single local authority seems to want to do things differently. If you look at
direct payments. Sometimes people are being paid a lot less than they would if they were getting care
provided through social services. Sometimes they get paid more. And the whole mechanisms by which
that funding is arranged and agreed and how it‟s processed can be quite complicated. So you‟ve
really got to know the local area to know how they process a direct payment. (Managing Director,
NATDOM4).
What I see is authorities seeing individual budgets as a way to effectively cut a substantial amount of
inhouse financial administration because they‟re not laying contracts, they‟re not having to deal with
the invoices coming through, reconciling invoices and timesheets etc., etc. I think they see it as a
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
282
fairly large financial incentive, a large financial incentive to pursue individual budgets. I think the
other aspect is I see the direct payment level is often set substantially below the prevailing contracted
rate. So not only are they saving because they‟re chucking out financial administration. (Commercial
Director, NATDOM2).
ii) Actions by central government
All the registered providers have this problem that personal assistants are not CRB checked. They do
not always pay their National Insurance or tax or whatever. And they cannot provide holiday cover,
and they are not trained. … Having gone round and setting up a registered service, and everybody is
going through the registered process, all the providers, we‟ve got to meet minimum requirements,
you‟ve got all these conditions. To then say, actually we‟re going to have a whole lot of people who
can provide service as a personal assistant. It just doesn‟t work. That‟s one big problem. And I don‟t
know how much the local authorities are spending on administering the direct payment service.
(Managing Director, NATDOM5).
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
283
IV.7. Summary
Building on the mapping of results presented in Part III, this part of the report interrogated the
findings from the telephone survey in more detail using a mix of statistical techniques and also
further explored qualitative interview data from provider managers, including senior HR
managers from the headquarters of ten national chains of providers. The six sections explored
step by step the patterns of effects of organisational characteristics, local authority
commissioning and labour market conditions on HR practices and HR outcomes experienced
by social care providers. Here, we summarise the key findings of each section.
We began by identifying the organisational characteristics of the sample of 115 providers
included in the telephone survey, supplemented by additional details for ten national chains
that also probed the pros and cons of being a national chain. The sample includes a wide range
of organisations characterised by size, ownership type (including nearly half as part of national
chains), public/private/not for profit status and CQC star rating, as well as by business
conditions such as percentage of bed vacancies, role of block contracts and reliance of service
users on LA funding. The extent of management support for HR practices was found to be
stronger in national and local chain providers, with less than one in ten single establishment
providers benefiting from a specialist HR manager. Nevertheless, only a third of all providers
had support available locally or on-site.
Given these different provider characteristics, section IV.2 analysed the statistical relationship
between size, ownership, CQC star rating and public/private/voluntary status and the variety of
HR practices and outcomes, drawing on a specially constructed, „standardised‟ dataset from the
telephone survey. Central to our analysis is the use of carefully defined indices and sub-indices
of HR practices and HR outcomes. These establish a standardised measure of quality for
defined HR practices such as pay levels, employee development, recruitment and retention and
working time, and for defined HR outcomes, including recruitment and retention, training and
staff turnover. Our objective was to identify those characteristics that are associated with good
practice and good outcomes. Key results include the following:
Homes, IDPs and LADPs:
- there is very little overall difference in use of good HR practices between homes
and IDPs, but the public sector LADPs register significantly higher on four out of
six indices, especially pay levels and employee development;
- homes deliver better HR outcomes than IDPs or LADPs despite the better HR
practices in LADPs, suggesting that the nature of domiciliary care work requires a
higher standard for HR practices;
Size differences:
- there are mixed effects of size on HR practices by size of establishment (among
other findings, examples include larger homes making more use of appraisals,
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
284
smaller homes being less likely to require weekend working, and larger IDPs more
likely to offer time off for training);
- large homes and large IDPs tend to have worse recruitment and retention outcomes
than smaller providers as measured by management perceptions, and more training
outcomes but there are no significant differences by size in quantitative measures of
staff turnover;
Ownership differences:
- national chain homes are more likely than other ownership types to have staff
working long hours and long weeks, and least likely to pay premiums for unsocial
hours, but more likely to provide regular pay uprating;
- there is limited evidence of differences among IDPs by type of ownership and this
fits with the qualitative interview data, which highlights local design of HR
practices, such as pay-setting for example, among national chains;
- single establishment homes score better on training outcomes than chains and local
chain IDPs score better training outcomes than national chains;
CQC star rating differences:
- homes with a CQC 3* rating provide significantly better pay and pay-related
conditions than 1* and 2* homes, but worse employee development and voice
opportunities;
- 3* IDPs are more likely to pay for qualifications than 2* IDPs; 3* IDPs are less
likely to have all staff working weekends than 1* IDPs.
Public, private and voluntary sector status
- Public sector LADPs score higher on most indicators of HR practices than both
homes and domiciliary care with working time and work organisation the two
exceptions where homes score higher, suggesting that these are affected by the
nature of domiciliary care work. Voluntary organisations score higher than for
profit independent sector providers, particularly on pay levels, although this may
reflect the higher share of private clients among voluntary sector homes in our
sample (see part III.3).
- The public sector LADPs do not score better on HR outcomes than homes, despite
better HR practices. The low outcome scores for all in domiciliary care suggests that
a higher standard of HR practice is required for similar HR outcomes in domiciliary
compared to the home sector. The voluntary sector has better outcomes than the
private sector and similar to the LADPs but the sample of voluntary sector
organisations is skewed towards homes.
Evidence from the interview data underlined the relatively limited variation in quality of HR
practices among independent sector providers. A willingness to pay more to care workers was
constrained by a perceived inability to raise revenue through charging higher LA fees.
Managers identified several HR practices as possible levers to improve recruitment and
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
285
retention outcomes but tended not to value improving workers‟ discretion at work or their nonpay benefits.
A second set of results identified the impact of the LA commissioning environment on quality
of HR practices. The interview data suggest LA fees play an important role in determining the
level of care workers‟ pay. However, our analysis shows that while higher fees facilitate the
payment of higher pay they do not guarantee higher pay. For IDPs, for every £1 increase in
hourly fees, the rate of pay increases on average by just 19 pence and for homes by just 14
pence. Reliance on LA funding among homes does appear to dampen pay rates; the greater the
share of LA funded clients the greater the likelihood of them paying care workers very low
rates of pay. As with pay levels, there is positive, albeit relatively weak, support for the idea
that LA fees positively influence the quality of HR practices. The results suggest higher fee
paying LAs support a higher score for the summary index of HR practices for IDPs, as well as
a higher index of pay levels for homes. The quality of other HR practices is higher on average
in high fee areas but differences are not found to be statistically significant. Fee levels offered
limited explanatory value for differential HR outcomes, with the exception of training
outcomes being surprisingly worse in high fee areas than in medium or low fee areas.
Using the categorisation of local authorities as adopting partnership, mixed and cost
minimising approaches to contracting for elderly care services (from part II of the report), we
found that these differences offered some value in explaining differences among homes but not
for IDPs. Among homes contracting with partnership-type LAs, most sub-indices of pay
practices scored higher and weekend working was less likely to be required. At the same time,
however, homes in cost minimising areas were most likely to have adopted good employee
development and voice practices. Like fee levels, this categorisation of LAs offered limited
value in explaining differential HR outcomes, with the exception of training outcomes in
homes (better in mixed LA areas) and recruitment difficulties in homes (worse for those in
partnership areas than in cost minimising areas).
Section IV.4 presented a similar analysis of HR practices and outcomes considering the effects
of local labour market conditions rather than LA commissioning. A first significant finding is
that in their approach to pay setting, just as we found with LA fee levels, not all providers
respond to local labour market pay levels (at least with respect to median pay levels for female
part-time workers in the LA area) in the same way. Around a fifth paid below 75% of the local
median, one in six paid above 90% of the median and the rest in between.
Using the more general categories of strong, medium and weak labour market demand
(developed in part I), the findings point to a tendency for providers to respond to strong labour
market conditions by improving their HR practices. For homes, this is particularly true of the
indices that measure the quality of pay levels and working time, as well as the summary HR
practice index. Other sub-indices support these findings, including greater use of pay practices
that reward unsocial hours and lesser requirement of regular weekend working in homes
located in strong labour demand areas. Two counter-intuitive results, however, are that these
same homes are also less likely than others in less strong labour demand areas to implement
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
286
good work organisation practices (such as encouraging workers to use discretion to manage the
timing and tasks of care duties) and less likely to match working time with employee
preferences. For IDPs, several results follow those for homes, including the measures of good
quality practices towards pay levels, payment for unsocial hours and the requirement for staff
to regularly work weekends - all of which are better in strong labour market areas. The results
for the measure of work organisation are again counter-intuitive, this time suggesting that IDPs
in strong and weak labour demand areas implement better work organisation practices than
IDPs in medium demand areas. The labour market appears to shape HR outcomes also. In
particular, achievement of NVQ targets is negatively related to labour demand, with an
especially strong penalty effect on IDPs in strong labour demand areas. This may be an
indication of poaching of qualified workers in tight labour markets, a problem than is not
confined to the social care sector.
While sections IV.3 and IV.4 usefully illuminated the direction and significance of associations
between organisational characteristics and environmental factors on the one hand and HR
practices and outcomes on the other, section IV.5 applied multivariate statistical methods
(backwards regression models) to interrogate these associations further. The headline findings
for IDPs are as follows:
a partnership, high fee paying LA environment is positively associated with good HR
practices, yet does not display a strong association with measures of HR outcomes
(with the exceptions of two counter-intuitive results that partnership LAs are associated
with high staff turnover on one measure and high fee paying LAs are negatively
associated with training outcomes);
local labour market factors play a role insofar as female part-time pay levels are
positively associated with the quality of pay strategies, the measure of local labour
demand is negatively associated with recruitment and retention outcomes and areas
with high female part-time pay have lower staff turnover;
several organisational characteristics explain some of the variation in HR practices and
outcomes, including:
- IDPs with for-profit status and of a larger size are more likely to have poor quality
HR practices;
- local chain IDPs benefit from a higher index of pay strategies than national chain
IDPs and better recruitment and retention outcomes (subjective measure) and
training outcomes;
and a number of HR practices are associated with good HR outcomes in IDPs,
including:
- good working-time practices (such as not requiring weekend and long hours
working and providing time off for training) are positively associated with
recruitment and retention outcomes (both subjective and quantitative measures);
- a recognition agreement with trade unions is strongly associated with lower staff
turnover;
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
287
- and the practices of providing pay upgrading opportunities, paying a premium for
weekend work and identifying skills and qualifications among job applicants are all
associated with lower staff turnover;
Given the complexity of the organisation of care work it is no surprise to find that some results
point in unanticipated directions. In particular, our regressions on the two quantitative
measures of staff turnover suggest that several good HR practices are associated with worse
outcomes. Examples include regular pay uprating, paying for CRB checks, use of formal
recruitment methods and offering guaranteed hours contracts. In these cases the cause and
effect may run the other way – that is, only in conditions of high staff turnover are managers
persuaded to introduce basic employment conditions and protections such as guaranteed hours
contracts.
The headline results for homes offer a similarly interesting and varied set of findings, as
follows:
the character of the LA commissioning environment has only a limited association with
quality of HR practice, with the important exception of high fee paying LAs being
strongly and positively associated with good pay level practices;
local labour market factors play a strong role through the level of female part-time pay
in the locality registering a strong positive association with quality of HR practices yet
worse training outcomes, and local labour demand is positively associated with quality
of pay level practices;
three organisational characteristics figure in the explanation of differentiated HR
practices and outcomes:
- larger size homes are associated with worse pay level practices and worse staff
turnover (quantitative measure)
- private, for-profit homes are very strongly associated with worse HR practices,
including pay level practices;
- single establishment homes have better training outcomes than national chain
homes;
and, finally, the quality of HR approach towards work organisation practices is strongly
and positively associated with training outcomes.
In the final section we assessed providers‟ views on social care policy and the commissioning
environment in order to provide a more nuanced account of relationships between providers
and LAs and to assess views about planned policy developments. Most providers rated their
relationship with LAs as good or very good. However, providers in cost minimising LAs
generally displayed the lowest levels of satisfaction. The quality of relationships depended on a
variety of factors such as the expertise of LA partners, satisfaction with the funding
arrangements, approach to communication and (unwelcome) involvement in providers‟
business decisions. One important mechanism to strengthen relationships was LA providers‟
EWERC
Part IV. The impact of organisational, commissioning and labour
market factors on HR practices and outcomes
288
forums. However, providers in cost minimising LAs were least likely to find these useful and
experienced the least frequent attendance.
Providers identified particular changes in commissioning arrangements that might improve
recruitment and retention. The most popular change was a rise in fee levels, followed by
greater variation in price by service user and, especially among IDPs, a more integrated LA
approach to service delivery. Other specific changes identified included a greater role for
providers to determine how care is delivered, higher guaranteed volumes of work and more
time for a service user.
Most providers believed LAs attached importance to their HR practices (especially recruitment
practices and training provision), with around four in ten saying this was very important for
LAs. General monitoring of providers tended to be undertaken directly by the LA, with only a
fifth or so reporting sole monitoring by the CQC; where both were involved in monitoring this
was sometimes perceived as excessive. More than two thirds of providers were satisfied with
CQC quality standards but only slightly more than half the quality rankings; most of those
dissatisfied were providers with a one star rating. Providers‟ suggestions about how to improve
CQC monitoring include greater focus on user needs, strengthening relationships with
providers, better communication and recognition of diverse provider practices.
Finally, providers expressed a number of concerns with respect to the new policy of direct
payments and individual budgets. Most supported the principle of personalisation of care but
voiced doubts about the practicalities, including problems of poaching of staff and managing
the multiple invoices for payments, as well as concerns about the lack of training and CRB
checks for new personal assistants.
EWERC
Part V. Recruitment and retention in the care sector: a case study
approach
289
V. Recruitment and Retention in the Care
Sector: A Case Study Approach
The aim of the case studies was twofold: to explore the HR practices of care sector providers
in more detail, in particular by exploring how these were experienced by care workers; and to
explore and understand some of the personal motivations and expectations of those who enter
the sector. These perspectives, we believe, provide insights into how providers could put in
place HR practices to facilitate smoother entries into the sector and foster longer term
commitments to care work.
Given the impact of LA commissioning and contracting on the HR practices of providers we
selected four local authorities with very different commissioning arrangements. The four LAs
include two from the north of England and two from the south, and include one very low
paying LA (IL), one low paying LA (ON), one medium paying authority (RN) and one high
paying (XD). Two (XD and RN) were classified as having commissioning environments that
typified a partnership arrangement. IL fitted the cost minimisation classification and ON
pursued a mixed approach (indeed it changed approach towards more cost minimisation
during the period of study-see part II above).
Within each LA, we carried out five case studies of providers: two domiciliary care, two care
homes and one local authority provider (in three cases a local authority based domiciliary care
provider and in IL a local authority owned home). We have used a simplified coding system
for the providers included in this case study sample; the relationship between the codes used
here in part V and those used for the same providers in the wider telephone survey are
outlined in appendix table V.A1. We ensured the provider organisations spanned a range of
different types and sizes and included national chains, local chains and not-for-profit
organisations. Qualitative interviews with care staff and senior care staff were used in
conjunction with the survey data already collected and reported in parts III and IV. The case
study data played a central role in the methodology of the project to provide more in-depth
data on range of areas including:
firm level practices and their impact on recruitment and retention in the care
sector;
the characteristics and experiences of care workers including their entry into
the sector, their desire to stay or leave, and the levels of satisfaction with key
aspects of their employment;
the linkages, where they exist, between commissioning practices, employer
practices and job quality issues for care workers;
differences, where they exist, between the views of established staff and those
of new recruits to gauge potential problems in retention in the sector;
Part V. Recruitment and retention in the care sector: a case study
approach
290
linkages, where they exist, between the provision of good quality care and
good quality care jobs
This part of the report is organised as follows. Section V.1 introduces each LA‟s approach to
commissioning and provides comparisons across the four LAs of key indicators of HR
practices within the five providers per LA included in this part of the study. These
comparisons focus on pay and benefits, working time, work organisation and training and
development. Key HR outcomes relating to recruitment and retention are also compared.
Two detailed comparative case studies of national providers are also presented; in each case
we have included two branches of the same national chain among our 20 case studies and
each branch is located in a different LA with contrasting commissioning strategies and
contracting practices. These case studies provide insights into the relative importance of LA
commissioning practices over company policy in shaping HR practices. In this first section
the analysis draws on data from the telephone survey of managers, building on our analysis in
parts III and IV.
The subsequent sections analyse the issues from the care worker perspective. We identify key
themes that emerge from interviews with care workers across all 20 case study organisations
in the four local authorities. Section V.2 explores care workers‟ perspectives on recruitment
into care work, while section V.3 considers the factors influencing retention among the care
workers. Section V.4 considers care workers‟ perspectives on the key HR practices related to
pay and working time while section V.5 considers their perspectives on the organisation of
care work and how this impacts on the quality of care they can provide. Section V.6
completes this exploration by looking at perspectives on and experiences of training and
development practices. Section V.7 concludes. Although most of the analysis draws on
qualitative data, it has also been possible to quantify some of the responses as nearly 100
interviews were carried out, 88 with care staff. Thus the case studies provide both some indepth data and some more general insights into care workers‟ perspectives, an area of research
which has been relatively neglected.
Part V. Recruitment and retention in the care sector: a case study
approach
291
V.1 Case studies in four local authorities: exploring the impact of
commissioning and contracting arrangements
V.1.1 Introducing the local authorities
The following four boxes give an overview of the LA commissioning environment in the four
local authority case studies, identifying the aspects of each that had led to their subsequent
categorisations as partnership (for XD and RN), mixed (for ON) and cost minimising (for IL).
Box V.1. Partnership local authority XD
The XD local authority is based in the south of England and covered rural as well as urban areas. Its
commissioning approach could be regarded as typifying a partnership approach that put HR issues at
the heart of contracting. It was a high paying LA with fees ranging from £16 per hour to £28 per hour
for domiciliary care and a relatively large inhouse facility covering over 40% of care provision. The
independent sector fees were raised in response to providers asking for a higher fee to remunerate the
staff properly to encourage retention. The LA had also moved to block contracts (for 11 providers
although 24 still provide spot services) in response to provider feedback that recruitment and
retention was being hampered by the lack of guaranteed hours. Overall the LA had adopted an
approach of enabling independent sector domiciliary care providers to offer similar terms and
conditions as those enjoyed by staff in the internal service. For example, they claimed to be only
accepting tenders for organisations that paid workers £7.00 per hour but some of our case study
organisations were paying lower rates. However, to offset some of the costs of paying higher fees
they had introduced electronic monitoring which changed the way of invoicing and was deemed to be
more efficient. According to published data this LA also had the highest average fee of our 14 LAs
for external home providers (note the interview data suggested a somewhat lower fee) and had in fact
moved out of residential care provision by transferring its homes to one voluntary organisation with
the result that more than half the provision is based on block contracts. It did not have any quality
enhancements for higher quality homes but said it would only normally make placements in homes
rated 2* or 3* by CQC and never in zero rated homes. Top up fees were relatively common and most
clients in local homes were not LA funded.
Box V.2. Partnership local authority RN
The RN local authority case study is based in the south of England. Overall it had adopted a
strategic approach to promoting quality by offering quality enhancements to domiciliary care
providers for meeting HR targets (and requiring these to be spent on staff bonuses or incentives,
training or team building) and in adopting a fair commissioning strategy for care homes which
should in principle involve no placements in homes which do not achieve a 2* or 3* CQC ranking.
Fees were also higher in homes meeting higher quality standards. However, this strategic approach
was adopted in conjunction with a policy of only paying a medium-level fee of £13.10 despite
being a relatively high wage area and not paying travel time on the grounds that a district provider
would get 55% of the work in their contracted area. Extra payments were, however, made for
Part V. Recruitment and retention in the care sector: a case study
approach
292
weekend work. RN contracts with ten preferred providers and the key performance indicators
(KPIs) that IDPs were expected to meet to receive additional payments included keeping turnover
less than the national average, ensuring continuity of care and the take up of work; meeting NVQ
training targets etc. RN had not introduced electronic monitoring and was piloting outcome-based
care with one of the case study providers. RN also commissioned jointly with the NHS. This joint
commissioning was proving more of an obstacle than a support for the fair contracting policy as the
NHS commissioners were said to be still keen to explore ways of keeping prices down while the
LA had come to a view that this would only lead to low quality. However, the fair commissioning
strategy had not been fully implemented due to a shortage of homes with good or excellent ratings
in the area. Fees paid by RN for home placements were rated as high but top up fees were relatively
common but not universal. RN only provided short term residential care in LA owned facilities but
had only a low share of block contract beds in the independent sector. LA funded clients were a
minority in most care homes.
Box V.3. Mixed case study local authority ON
The ON local authority is based in the north of England. The commissioning approach of this LA
contained strong elements of both cost minimisation and partnership. ON espoused a partnership
approach in its discussion of its relationship with providers and up to and including the time of the
interview at the LA, there was substance to the claim that it had taken steps to ensure that IDPs
paid for travel time, by paying a higher fee for short term visits and monitoring IDPs to ensure
travel time was paid for. It also symbolically paid double time for bank holiday working. However,
it combined this approach with a relatively low fee level of £11.17 and during the course of the
project had discontinued the practice of paying more for short visits as a consequence of
introducing electronic monitoring and indeed instead was introducing a system of paying only far
actual minutes spent at the user‟s home. ON had moved to single pricing for domiciliary care some
years ago to try to prevent poaching of care workers between providers. It now had ten preferred
providers and 7 spot contractors. For homes ON only provided a low level of fees and was still
engaged directly in the provision of both long term and short term care but most of the provision
was joint with the NHS around intermediate care. It paid a little more for homes with Investors in
People awards and was considering a wider quality enhancement framework. Top up fees were
found in some but not all homes and the LA was aware sometimes private residents subsidised
those funded by the LA, who are often a minority of residents.
Box V.4. Cost minimising local authority IL
IL is based in the north of England. We have classified this LA as a cost minimising LA in part on
the grounds that it paid very low fees for both domiciliary care (£10.78 per hour) and also for care
homes (the lowest of the 14 LAs) with no quality uplifts. The LA used spot contracts except in one
case where a provider had been awarded a block contract to provide the hospital discharge service.
There was a set price for domiciliary work of £10.78 per hour with few variations and no increases
for bank holidays. There were no enhancements for short visits and the move away from block
contracting had also removed payments for travel time. A premium payment for higher quality care
Part V. Recruitment and retention in the care sector: a case study
approach
293
had also been removed on the grounds that all providers now met the quality threshold. The LA
contract managers considered that the shift from block to spot contracting had affected recruitment
and retention of staff but commissioning policy was developed independently from contract
management in this LA. With respect to care home placements the LA paid a very low fee and
despite being a low wage area anticipated that most LA-funded residents would still be asked for top
up fees. Although over 40% of placements were under block contracts to the independent sector,
these were said to be political and historical legacies and were being phased out. The LA itself was
only involved in short term care. The LA had a strong quality framework for monitoring IDPs and
care homes but this was not linked to any financial incentives.
V.1.2. Pay practices of providers by local authority.
Comparison of key indicators relating to pay (see table V.1) shows that although there is some
relationship between LA commissioning price and the wages paid by providers, such that pay
rates are marginally higher in the high fee compared to the low fee areas, with pay rates
hovering around the level of the national minimum wage (£5.73) in both IL and ON
providers. However, pay levels were only slightly higher in southern locations despite much
more generous fee levels: for example in one national chain fee levels were £4 to £5 an hour
higher in the southern than in the northern LA but wage levels were only 25 pence per hour
higher (see table V.1 to compare pay levels between XDDom1 and ONDom2). In another
national chain fee levels were around £2 an hour in the higher compared to the lower fee LA
but wage levels were only about 50 pence higher (see table V.1 to compare pay levels
between RNDom1 and ILDom1). This evidence suggests that national chains are not passing
on more favourable commissioning practices by improving employment conditions in the
sector and instead pay wages that are further down the local labour market wage hierarchy.
Table V.1 Pay practices across the case study providers
Normal pay rates £
Area
XD
RN
ON
IL
Case 1
Case 2
LA case
Home
7.34
6.50
Dom
6.50
7.26
Home
6.60
6.50
Dom
6.51
7.14
Home
6.21
5.73
Dom
6.05
6.25
9.13
Home
5.73
6.08
11.82
Dom
6.00
6.00
8.41
11.11
Travel Payments 2
Unsocial hours
payment1
Case 1
Case 2
LA case
Case 1
Case 2
LA case
Y
Y
Y
DK
Y
M
T
T
N
N
Y
Y
Y
N
N
T
N
N
Y
Y
N
N
N
T
N
N
Y
N
Y
N
N
1
Y – Yes; N- No; DK – Don‟t know
T – Time; M-mileage only; N-none
2
The case study organisations are typical of the providers surveyed in stage two of the project
in that pay varies according to provider type. The LA inhouse providers all pay higher rates of
Part V. Recruitment and retention in the care sector: a case study
approach
294
pay, all pay for travel time and all but one pay enhancements for unsocial hours and in
contrast the lowest paying providers are care homes, particularly in the cost minimising and
mixed LAs.
The data relating to travel payments and unsocial hours also shows the influence of the LA
commissioning environment. None of the IDPs in RN paid travel time or mileage which is
consistent with RN‟s policy not to pay travel time. In contrast the IDPs in XD paid a mix of
travel time and mileage, although where only mileage was paid the manager reported that in a
rural area the lack of payment for travel time was still a reason for recruitment and retention
problems. Only care homes in XD paid extra to care staff working unsocial hours; all other
care homes offered no enhancement. Significantly, the two providers in IL that paid
enhancements for unsocial hours did so because one was an LA care home and the other
ILDom2 had been awarded the LA hospital discharge contract.
V.1.3. Working time practices of providers by local authority
There is mixed evidence as to the impact of the LA commissioning environment on the case
study providers‟ working time practices. If we firstly look at the type of contracts on offer,
table V. 2 shows only two out of eight IDPs (XDDom2 and ILDom2) offered guaranteed
hours and these had block contracts with the LA. While this shows the LA enabling good
practice in these cases, the data on other dimensions of working time show just as many
variations within LAs as across LAs.
Table V.2 Working time practices across the case study providers
Maximum working
week1
Area
XD
RN
ON
IL
Case 1
Case 2
Home
6
6
Dom
6
5
Home
7
6
Dom
7
6
Home
5
5
Dom
7
6
Home
5
5
Dom
7
6
LA case
Case 1
Case 2
M
M
M
A
M
M
M
M
M
M
5
A
7
5
5
Contracts3
Match staff
preferences2
LA case
Case 1
Case 2
LA case
M
Z
G
G
S
Z
Z
G
M
M
Z
Z
G
A
M
M
A
M
Z
ZG
1
Days
A-all; M-most; S-some of the time
3
Z- zero hours; G- guaranteed hours; ZG- mixed
2
Three quarters of the 20 case study providers said they matched preferences most of the time.
Four reported that they matched preferences all of the time and three of these were in IL and
ON, the non partnership authorities. One LADP in RN said they only matched hours some of
the time; this is in line with a general finding that those working for LADPs have less
Part V. Recruitment and retention in the care sector: a case study
approach
295
flexibility in terms of choosing their hours compared to those working for independent
providers possibly because LADPs have moved from 9 to 5 type work schedules to very
flexible ones, related to their more specialist re-ablement work. This means they pay much
less attention to employee preferences compared to the past.
The type of provider is an important factor in explaining variations in the maximum working
week. LADPs all had a maximum working week of five days although the LA care home had
a maximum working week of seven days. However, some of the lowest paying homes in IL
and ON only had a five day maximum working week. There was thus no obvious bundling
together of poor pay practices with poor working time practices or indeed good with good;
nor indeed any systematic trade-off between good working time and poor pay, for example.
There were also no patterns relating to this and the LA strategy; so although no providers in
XD had a maximum working week of seven days in the partnership, two providers in RN, the
other partnership LA, had a policy of maximum seven day working. In this area company
policy appears to the key factor shaping HR practice.
V.1.4. Work organisation of providers by local authority
We compared the case study providers across three indicators of work organisation. Not only
were these indicators expected to reveal the influence of LA commissioning and provider
practices on how care work is organised but they could also be expected to have an impact on
the quality of care jobs and on the quality of care for service users. The first two indicators tap
into the opportunities to use discretion to prioritise tasks and develop good relationships with
service users (see section I.4 for the links between these aspects of work organisation and the
quality of care). The third indicator relates to the use of electronic monitoring which is linked
directly to LA commissioning practices.
Table V.3 gives a breakdown of this data for each case study provider. Nine out of twenty
managers reported that care workers were free to prioritise tasks, six of the nine being from
care homes. However, no provider in XD said yes to this and our analysis of the manager
telephone survey data from the case study providers suggest that there are conflicting views as
to whether increasing care worker discretion was a good or bad HR practice. These findings
mirror evidence in part IV (section IV.2) that managers did not consider changes to work
organisation as a mechanism to improve recruitment and retention. The quoted responses in
box V.5 from one provider manager in ON sum up the reservations some managers have
about giving care workers the opportunity to prioritise tasks to improve quality care,
especially those working for IDPs where such freedom may have cost implications if
electronic monitoring is in place. However, as we have seen in section I.4, a certain amount of
flexibility is deemed to be an important factor in service users‟ definitions of quality care and
managers appear to have a view that runs counter to such perspectives where the focus instead
is on following contracting requirements and care plans.
Part V. Recruitment and retention in the care sector: a case study
approach
296
Table V.3 Work organisation across the case study providers
Freedom to prioritise tasks in
ways that improve the quality
of care1
Opportunities to develop
good relationships with
users1
Electronic
monitoring2
Case1
Case2
Case1
Case2
LAcase
Case1
Case2
LAcase
Home
SE
SE
Y
Y
Dom
N
SE
N
Y
Y
Y
Y
Y
Home
Y
Y
Y
Y
Dom
SE
SE
SE
Y
SE
N
N
N
Home
Y
Y
Y
Y
Y
Dom
SE
N
Y
Y
Y
Y
Y
Y
Y
Home
Y
Y
SE
SE
Y
Y
Dom
Y
SE
Y
Y
N
N
Area
XD
RN
ON
IL
LAcase
SE
Y
1
Y - Yes; N – No; SE - Some extent
Y - Yes; N – No
2
Box V.5 Work organisation that encourages discretion: a manager’s views on whether
it is a good or bad practice?
Q. Are staff free to prioritise and carry out tasks in ways that they feel will improve the quality of
care?
A. No. We have to stick to a care plan which is provided by social services, and we have to do the
tasks that are on there.
Q: [So they have to do that in a strict order]?
A: They do, yes. If anything else is required by the service user they have to phone up and let us
know first. (ONDom2, manager)
Providers were more positive about care workers‟ opportunities to develop good relationships
with service users. Sixteen out of twenty providers said care workers were able to do this.
There appeared to be no obvious relationship between this and the LA commissioning
environment although the only provider that said this was not possible, XDdom1, had also
said care staff were not free to prioritise tasks. It would seem in this provider there was
limited discretion and ability to develop good relationships and both could be related to
electronic monitoring. An interview with a care coordinator at the provider suggests this is the
case.
I would say [the job of a care worker is] more difficult [than in the past] and generally that‟s
because of the paperwork involved as well…..Because they‟ve got to write more and more,
that‟s more and more details, spend more time looking at the plan. With the log in, log out,
obviously it‟s not taking into account how long it takes to actually get in the house. Because
they‟re paid by the minute. Plus when they leave, you phone out, and then Miss Bloggs turns
Part V. Recruitment and retention in the care sector: a case study
approach
297
round and says, “Oooh dear, could you just put the bin out?” And then they‟ve got to do that.
And then you‟ve got to say,:”Alright, I‟ll see you again”, and ... get out past the lock up and
obviously none of that‟s taken into account with the log in, log out (XDDom1, Care
Coordinator, age 38, 3 yrs in post)
Table V.3 shows that electronic monitoring was in use in the two LAs - XD and ON- that
specified its use in its commissioning. This use of electronic monitoring did appear linked to
perceived lower levels of discretion for care workers as the only IDPs that said workers had
no freedom to prioritise tasks to improve quality of care were XDDom1 and ONDom2. These
providers were also part of the same national chain so this may either have been a general
company policy to limit care worker discretion or alternatively a company policy in response
to electronic monitoring in those specific LAs that used this practice to ensure care workers
were able to carry out the commissioned tasks in the designated time. However, it is notable
that all providers in ON reported that staff could develop good relationships, even though
electronic monitoring was also in place.
Overall the case-study findings suggest those working in IDPs have less discretion to
prioritise tasks as the majority report this was possible only to some extent. Thus company
policy, the LA commissioning environment and the nature of the work may all play a part in
explaining why work organisation takes the form it does in specific providers.
V.1.5. Training and development of providers by local authority
A comparison of some of the key indicators relating to training reveals the limited influence
of the LA commissioning strategy on this aspect of HR practice.
Table V.4 shows that some of the lowest paying case study providers in local authorities with
the lowest fees perform particularly well on meeting statutory requirements relating to
training. This fits with the overall findings from the telephone survey that training outcomes
were worse in high fee areas ( see part IV, section IV.3). In contrast two of the case study
providers in RN had not met the NVQ level 2 target even though they had been set KPIs by
the LA relating to training targets. The case study care homes were more likely to have NVQ
level 2 qualified staff although this could reflect increased opportunities for care workers to
complete any associated paperwork in the workplace rather than a stronger commitment by
providers to meeting statutory requirements and training.
The payment for time spent in induction training and length of induction are also indicators of
providers‟ commitment to training. The XD partnership authority stands out with induction
training paid by all providers, ranging from a minimum of four days to a maximum of three
months. However, other trends do not relate to the LA commissioning environment. Induction
training was more likely to be both longer and to be paid for in all care homes across all four
local authorities. Company policy may also explain differences in policies towards induction.
For example, XDDom1 and ONDom2 were part of the same national chain and both offered
four days induction training.
Part V. Recruitment and retention in the care sector: a case study
approach
298
Table V.4 Training and development across the case study providers
Area
XD
RN
ON
IL
Home
Dom
Home
Dom
Home
Dom
Home
Dom
Length of induction1
Paid induction2
NVQ attainment level3
Case 1
Case 2
Case 1
Case 2
Case 1
Case 2
3
3
Y
Y
3
2
1
2
Y
Y
1
3
3
3
Y
Y
4
4
1
1
L
N
1
1
3
3
Y
Y
4
4
1
1
3
N
Y
Y
1
4
4
1
3
2
Y
Y
Y
4
3
4
3
2
Y
Y
2
3
LA case
2
2
LA case
Y
Y
LA case
1
4
1
1: 4 days or less; 2: 5 days to 2 weeks; 3: More than 2 weeks
Y – Yes; N – No; L – paid later if staff stayed
3
1: Up to 45%; 2: 46% to 55%; 3: 56% to 69%; 4: 70% or greater
2
V.1.6. Comparing national providers in different LA environments
Boxes V.6 and V.7 compare the HR practices in place in provider organisations that were part
of the same national chain but located in different LAs. These two national chain case studies
can illuminate the impact of LA commissioning versus company policy on HR practices as a
whole and on specific elements of HR practices as the case study establishments are located
in LAs that span southern and northern locations and partnership, mixed and cost minimising
commissioning and contracting practices.
Box V.6. A comparison of a national providers’ domiciliary care establishments in a
partnership and cost minimising local authority (RNDom1 and ILDom1).
Background: Both RNDom 1 and ILDom1 were part of the same national chain and were rated
2*by CQC. RNDom1 was based in a partnership authority that paid medium level fees and
ILdom1 was based in a cost-minimising authority that paid very low fees. Both providers found
recruitment easy and had turnover between 10-20%. RNDom1 reported staff shortages in contrast
to ILDom1 that reported no shortages.
Pay: RNDom1 paid £6.51 with enhancements in contrast to its equivalent in IL which paid £6.00
with no enhancements. Thus LA fee levels were higher in RN by around £2 an hour but wages
paid were only 51 pence more in the RN branch than in the IL branch. Not only is there only a
limited increase in line with LA fee levels but also the stronger labour demand in RN compared to
IL has had limited impact in raising wage levels, as is perhaps indicated by the greater staff
shortages in the RN branch. High unemployment in IL may be enabling providers to pay very
close to the NMW without much impact on recruitment and retention. RNDom1 also paid
enhancements for weekend work: this was in line with the RN commissioning policy of paying for
weekend work as well as with perhaps pressure from strong labour demand. Of the nine providers
in RN that were surveyed in the telephone survey, seven out of nine providers paid enhancements
for weekend working and five out of nine paid enhancements for evening work. In contrast, in IL,
only three out of nine of the providers in the telephone survey offered enhancements for weekend
Part V. Recruitment and retention in the care sector: a case study
approach
299
working and only one offered enhancements for evening work. In IL there was no commissioning
policy encouraging unsocial hours payments.
Working Time: Both providers had a six day maximum working week. However, there were
differences in relation to efforts to match staff preferences; ILDom1 reported matching staff
preferences all of the time whereas RNDom1 reported to do so only most of the time.
Training: Both providers had short paid inductions, although in RNDom1 this was not paid
initially but only if staff stayed. ILDom1had met the NVQ target but RNDom1 had not done so.
Work Organisation: Electronic monitoring was not in place in either LA but the two providers
differed in terms of whether care staff were able to prioritise tasks and develop good relationships.
ILDom1 reported this was the case whereas RNDom1 where reported only to some extent.
Summary: It would appear that the commissioning environment, combined to some extent with
local labour market factors, has an influence on pay practices, particularly unsocial hours
payments. Other dimensions of HR practice appear to be more influenced by company policy
rather than the commissioning environment. In some cases variations in responses between the
two branches may also be a result of managerial discretion at branch level. For example, even
though electronic monitoring was not in place in either location the two branch managers reported
very different approaches to care workers‟ discretion and to payment for induction.
Box V. 7 A comparison of a national providers’ domiciliary care establishments in a
partnership and mixed local authority (XDDom1 and ONDom2)
Background: Both XDDom 1 and ONDom2 were part of another national chain and were both
rated as 3 * providers by CQC. Both reported staff shortages. XDDom1 found it neither easy nor
difficult to recruit whereas ONDom1 found it quite easy. However, ONDom2 had much higher
staff turnover at over 30% compared to 10-20% in XD.
Pay: XDDom1 paid £6.50 while its northern counterpart ONDom2 paid £6.25 with a weekend
enhancement of 22p. However, fee levels were £4 to £5 an hour higher in the southern LA than in
the northern LA location so this 25 pence extra shows a very marginal impact of LA
commissioning practices on pay levels offered. XDDom1 also paid mileage, possibly a reflection
of its rural location and XD‟s willingness to pay a higher fee in rural areas. ONDom2 was in a
more urban location. However, both paid enhancements for unsocial hours and ONDom2 was
atypical in doing so if we compare this with the other data collected in the telephone survey from
providers in ON. Only three out of nine providers paid an enhancement for weekend work and
only one out of nine paid extra for evening work. In this sense ONDom2 had put in place a pay
practice that was not typical of those on offer by other providers despite limited LA fees and this
may show the influence of company policy. The LA in ON did pay extra for bank holidays but had
discontinued other unsocial hours payments.
Working Time: Both providers had a 6 day maximum working week and matched worker
preferences most of the time.
Work Organisation: Both providers said care staff could not prioritise tasks to improve the
Part V. Recruitment and retention in the care sector: a case study
approach
300
quality of care and this could be related to the impact of electronic monitoring which was in place
in both LAs.
Training and Development: Both providers had four days paid induction training and neither had
met the NVQ level 2 target. However, the high level of staff turnover at ONDom2 is likely to have
been an obstacle to meeting training targets, but the same did not apply to XDDom1.
Summary: In this case the LA commissioning environment had limited influence on pay
practices. A much higher fee led to only a marginal difference in wage levels, although the
payment of mileage may be related to commissioning practice. Work organisation was also shaped
by commissioning practices since the requirement to use electronic monitoring, as in both these
LAs, limited the freedom of providers in this area. However, in the areas of training and working
time it would appear that it is national firm policy that is primarily shaping HR practices.
The two comparative case studies suggest that the policies of national chains are playing a
significant role in both shaping HR practices and in limiting the actual impact of favourable
commissioning and contracting practices on employment terms and conditions. This
reinforces the picture presented in part IV as well as from the evidence from the case study
providers in these four LAs. A key finding is that the LA commissioning environment may be
an enabler of better practice but there are variations between providers in the extent to which
they respond to more favourable commissioning practices. Furthermore, although there is
variation in practices across providers, this variation is around a very low level of basic
employment conditions and protections. However, we also need to consider the possibility
that national providers are cross subsidising providers in low fee paying LAs where they
may be making losses through retaining higher margins in higher paying LAs. If this were to
be the case, and national providers‟ overall profits are either low or even negative, then the
key driver of low pay can still be said to be LA commissioning
V.1.7. Overview of HR outcomes for providers by local authority
Drawing again on evidence from the telephone survey, we can assess the performance of the
case-study providers with respect to HR outcomes, measured by various indicators of
recruitment and retention. Table V.5 presents the HR outcomes for the 20 providers and
shows that there is no straightforward relationship between practice and outcomes.
The data on HR outcomes show that ten out of 16 independent sector providers considered it
easy or very easy to recruit care workers. Two of the four providers in the low paying IL LA
reported it to be quite difficult or very difficult to recruit but this was not replicated in ON, the
other low pay area where all providers considered it quite easy or very easy. Perhaps
surprisingly the LA providers were the most likely to respond that it was neither easy nor
difficult or quite difficult (all three LA case studies for which we have responses). In contrast
there was a majority view among independent sector providers that they did face specific
labour shortages. This applied to nine out of 16 and seven of these were IDPs out of a total of
eight IDPs. The two LADPs in high wage areas also felt they faced specific labour shortages.
Part V. Recruitment and retention in the care sector: a case study
approach
301
We have two measures of staff turnover, one the overall rate and one excluding turnover
among new recruits. On both measures the two case study IDPs in ON stand out as
experiencing very high levels of turnover, although the rates are particularly high when new
recruits are included. However, beyond these two providers, turnover rates were more
variable within than between LAs even for the independent sector providers but this was even
more the case if the LA providers are considered where turnover rates were low in the three
LAs for which we have data. If we look in detail at overall turnover rates in these providers
and compare them to the national average turnover rate for care workers of around 22% ( see
part I.5 (Eborall et al. 2010)) we find that only the two IDPs in ON have rates above this
level and of the rest the majority (seven out of thirteen ) are clustered slightly below this level
in the range 18% to 22%. Of the six with rates below 18%, five are homes and only one is an
IDP. However, they are drawn from all four LAs. This suggests that to the extent that
partnership LAs are associated with better HR practices, at most these are tending to alleviate
otherwise very high turnover rates.
Table V.5 HR outcomes across the case study providers
Ease of
recruitment1
Area
XD
RN
ON
IL
Case1
Case2
QE
N
Dom
N
QE
Home
VE
N
Dom
QE
N
Home
QE
VE
Dom
QE
QE
Home
QE
VD
Dom
VE
QD
Home
LA
case
Specific staff
shortages2
Staff turnover rate
excluding new
recruits 4 %
Case1
Case2
Case1
Case2
21
17
23
17
11
MD
14
MD
19
12
20
13
18
22
16
15
16
5
11
5
Case1
Case2
N
Y
Y
Y
N
Y
Y
Y
N
N
QD
Y
Y
N
101
56
6
48
21
6
N
N
N
N
19
6
MD
19
7
MD
N
Y
19
18
MD
4
N
QD
LA
case
Level of staff
turnover in the last
12 months3 %
Y
Y
LA
case
6
7
LA
case
5
7
1
VD - very difficult, QD - quite difficult N - neutral QE - quite easy VE - very easy
Y- Yes N- No
3
for definition see Appendix IV.A1.4 IRT3 MD= missing data
4
for definition see Appendix IV.A1.4 IRT9 MD= missing data 4
2
The data on HR outcomes show that ten out of 16 independent sector providers considered it
easy or very easy to recruit care workers. Two of the four providers in the low paying IL LA
reported it to be quite difficult or very difficult to recruit but this was not replicated in ON, the
other low pay area where all providers considered it quite easy or very easy. Perhaps
surprisingly the LA providers were the most likely to respond that it was neither easy nor
difficult or quite difficult (all three LA case studies for which we have responses). In contrast
there was a majority view among independent sector providers that they did face specific
labour shortages. This applied to nine out of 16 and seven of these were IDPs out of a total of
eight IDPs. The two LADPs in high wage areas also felt they faced specific labour shortages.
Part V. Recruitment and retention in the care sector: a case study
approach
302
We have two measures of staff turnover, one the overall rate and one excluding turnover
among new recruits. On both measures the two case study IDPs in ON stand out as
experiencing very high levels of turnover, although the rates are particularly high when new
recruits are included. However, beyond these two providers, turnover rates were more
variable within than between LAs even for the independent sector providers but this was even
more the case if the LA providers are considered where turnover rates were low in the three
LAs for which we have data. If we look in detail at overall turnover rates in these providers
and compare them to the national average turnover rate for care workers of around 22% (see
part I.5 (Eborall et al. 2010)) we find that only the two IDPs in ON have rates above this level
and of the rest the majority (seven out of thirteen) are clustered slightly below this level in the
range 18% to 22%. Of the six with rates below 18%, five are homes and only one is an IDP.
However, they are drawn from all four LAs. This suggests that to the extent that partnership
LAs are associated with better HR practices, at most these are tending to alleviate otherwise
very high turnover rates.
Moreover, not all „good‟ HR practices may induce lower turnover. For example, some
managers from case study providers suggested that extensive induction and high levels of
training could be a reason for some turnover, particularly of trained staff.
Some do [leave]. Social care is quite popular at the moment. Rehab assistants. Usually NHS offer
better terms and conditions than we do. That‟s my latest one, I‟ve got one of my NVQ 3 girls
going. But often it‟s for advancement. Because we put people through NVQ 2 and then NVQ 3,
which is a springboard to higher positions. (XDHome1, Manager).
I think, to be quite honest, because we train our care assistants up to NVQ3 as much as possible,
and when they‟ve got their [NVQ] three then we encourage them to try to do better. Now, some
come back „cos the grass isn‟t greener, you know, but quite a few have gone to hospital and
whatever and doing their training. (ONHome1, Manager).
This reveals why HR outcomes are not directly related to HR practices; not only will local
labour market factors play a role but also internal policies to train and develop staff may
increase their external opportunities. Furthermore, the personal motivations of care staff and
their experiences will also be a big part of the story of recruitment and retention in the care
sector and while they will be shaped by these organisational and local labour market factors
they will not be determined by them. An analysis of the case study interview data will now
follow and we will look at care worker attitudes and motivations towards the job and areas of
HR practice in more detail.
Part V. Recruitment and retention in the care sector: a case study
approach
303
V.2. Care workers’ perspectives on recruitment
Drawing now on the interviews with care workers, we explore the attitudes and experiences
of care workers, focusing specifically in this section on the process of recruitment, including
why people entered the care sector and how they heard about care job vacancies. We also
highlight any findings that relate to specific HR practices that may make some providers more
attractive to potential recruits than others. Appendix table V.A2 provides information on the
employment roles of the 98 respondents; 88 were directly involved in care work while a
further 10 had a variety of roles in supporting care work. For much of the analysis the sample
is limited to the 88 care workers but where relevant we use the whole sample. In this section
because all 98 interviewees were recruited as care workers, our analysis draws on data from
the whole case study sample.
V.2.1 Factors that influence entry into the care sector
All interviewees were asked why they had chosen to work in the social care sector as a care
worker. It was possible to identify four dominant factors that shaped entry;
the nature of the job and the search for meaningful work
the influence of family and social networks
the opportunity for a change of direction/career
the search for convenient working time.
The nature of the job and the search for meaningful work
Previous research has shown that „making a difference‟ and doing a job that involves helping
others is important to those working in the care sector and for many of the interviewees it was
simply this that was given as the reason for entering the sector. For many care work was a job
that gave the opportunity to be engaged in satisfying and meaningful work, often in contrast
to previous work they had done (box V.8).
Box V.8. Care work as an opportunity to make a difference and do meaningful work
I think I originally chose it because of the satisfaction it gave me, and to actually see the outcomes
for individuals, which I think was very rewarding for me as an individual. (RNLADP, Service
Manager, age 45, 21 yrs in post)
When I was made redundant [from retail] for the third time, I knew that I didn‟t want to work in
retail any more after all these years, I wanted to do something a bit more meaningful, that give me
more satisfaction from a human point of view (RNDom2, Care Worker 3, age 57, 6 months in post)
I wanted to do something where I actually was making a difference. I had, for example I had one job
where for half a day I worked in tele-sales, cold calling, and I left at lunchtime. It‟s the only job I‟ve
Part V. Recruitment and retention in the care sector: a case study
approach
304
ever walked out on, because it‟s just a horrendous job and I did not want to do something like that.
(RNDom2, Care Coordinator, age 24, 3 yrs 6 months in post)
I just think it‟s nice to be able to help somebody that can‟t do anything for themselves or can‟t do a
lot for themselves, it‟s just a good feeling to see that you‟ve done something for them, you know, it‟s
an achievement. (ONDom2, Care Coordinator 1, age 54, 2 yrs in post)
Just wanted a career change. It‟s very monotonous [office work], I mean office work is very well
paid, but it‟s not all about money. You know, it‟s job satisfaction. I like the buzz here, it‟s very nice.
It‟s a nice environment and I‟m very much a people‟s person, that‟s why I‟m good at what I do.
(RNHome2, Care Worker 1, age 54, 1 yr 10 months in post)
Some care workers identified the distinctive characteristics of care work in homes compared
to IDPs, or vice versa, and used these distinctions to describe why one type of work was
chosen over the other (Box V.9). For some working for IDPs, the unsupervised nature of
domiciliary care work meant they felt autonomous, an attribute that was very attractive to
them. They also liked the idea of moving around between different places and meeting
different people. In contrast some of those working in care homes had worked for domiciliary
care providers in the past and found it too rushed and had chosen to work in care homes.
Older workers in particular said working in one place was less tiring while younger workers
with no access to transport also chose care homes.
Box V.9. The advantages and disadvantages of working in IDPs
The advantages
Being my own boss, because I‟m obviously out on my own most of the time. I occasionally go out with
other care workers, on double-up runs, but mostly I‟m on my own. So I‟m my own boss as such.
(XDDom1, Care Worker 2, age 37, 2 yrs in post)
You‟re all the time in different places…And I‟m bored when I‟m sitting in one place, so that‟s why.
(RNDom2, Care Worker 1, age 22, 10 months in post)
It‟s something different on your own, you‟re not in one place, somebody watching you while you‟re
working all time, you‟re out and about…..You meet different people. (ONDom1, Care Worker 1, age
48, 3 yrs in post)
The disadvantages
Too much pressure [in domiciliary care providers]. I mean because you didn‟t have the time, like say
if you had to do their dinner for „em[users], it‟s like you‟re rush, rush, rush, don‟t have time to talk to
„em, time to get their dinner, you know, how you want it, and then you‟re off to your next one
then….No, I didn‟t like it, it wasn‟t me. (ONHome2, Care Worker 1, age 47, 8 yrs in post)
I didn‟t fancy home care because of the transport and I don‟t drive. (ILHome2, Care Worker 4, age
29, 3 weeks in post)
Part V. Recruitment and retention in the care sector: a case study
approach
305
The influence of family and social networks
The case study approach allowed us to contextualise responses about the attractiveness of care
work to this group of workers. This revealed first of all the importance of family and social
networks in influencing these decisions. Thirty-six out of 88 care workers (and 38 out of the
whole sample of 98 interviewees) cited informal experiences of looking after elderly relatives,
neighbours or children as the main motivating factor when deciding to enter care work (box
V.10). This is an important finding because it meant that 40% of our sample of „stayers‟ and
new recruits had some knowledge about what the job involved before they entered the
organisation. Seventeen of these were working for IDPS compared to 15 who were working
for care homes (including four who were working for the LAhome). Four out of 15 care
workers working for LADPs cited this as a motivating factor.
Box V.10. Informal experience of caring for family and the elderly
Why did you choose to work in the social care sector?
Basically because it‟s all I‟ve done, personally, through my life, if you know what I mean….I‟ve
never done it officially but I‟ve done it unofficially with family members...My Nan, my granddad and
my son. (ILDom1, Care Worker 2, age 34, 8 months in post)
It‟s something that I‟ve wanted to do for a long time but I just felt I wasn‟t ready. You know when the
children have grown up and that. And then I was looking after my father in law who has got
dementia and he is in a nursing home. So I helped my mother in law with him a lot. And went round
and was helping her. And when it came to changing him, because he was incontinent, it was me that
actually did it, and I didn‟t think twice about doing it. My mother in law, she couldn‟t do it. And it
was from that and then quite a few people over the years said, you‟re quite good with old people.
Why don't you work with them. (XDHome1, Care Worker 3, age 44, 3 yrs in post)
Because I obviously care for my children, so I‟m already used to caring. And with care work what
we do is very similar to looking after children basically, apart from obviously adults. So I was used
to it. So I thought well it‟s the best job really for me to do. And I enjoy caring. So, it‟s my sort of job.
(XDDom1, Care Worker 2, age 37, 2 yrs in post)
No, it weren‟t just the hours. I mean I looked after an elderly neighbour once, I used to like go in
every day and see to her and I thought I‟d always fancied doing something like that. (ONDom1,
Care Worker 1, age 48, 3 yrs in post)
Related to this was also the influence of family and friends on entry into care (box V.11).
Two thirds of the interviewees (64 out of 98 interviewees) mentioned that family or friends
worked in care and 11 of these stated that this was the main influence on why they entered
care while the majority recognised that this knowledge of the care sector through personal
contacts influenced their entry in some way. Quite a few of the new recruits we interviewed
were younger workers who had family members, often mothers, working in the care home or
the IDP they were working for. Many care workers cited being encouraged by family
Part V. Recruitment and retention in the care sector: a case study
approach
306
members and friends to do the job and others recognised that being surrounded by care
workers influenced their decision to enter.
Box V.11: The influence of family and social networks on entry into care work
Our [sister-in-law] loves it, she kept saying, „It‟s, just perfect for you, you would just love it.‟ And
she was right. (ONDom1, Care Worker 4, age 43, 5 months in post)
I spent a lot of time with my Nan, like I say, my Nan worked in care for about 30 years. So often
when I was at her house I‟d hear different things from when she was out working. It‟s just kind of,
they didn‟t push me into care, but I think it‟s something that I‟ve wanted to do, hearing stories from
my Nan and my aunty. (ONDom2, Care Coordinator and Care Worker, age 26, 5 yrs in post)
My mum done it, my Nan done it first, obviously, then my mum‟s been doing it for about ten years.
She started off as a cleaner and then become a carer in her home and she‟s been there for ten years.
My cousin was working in my old home which I got a job in and then my sister was like, „Oh, I‟ll
come and join you too.‟ So she come into it…..My mum said, „Give it a go.‟ But I was just like I need
to do something, I just can‟t be bothered to do hairdressing any more. And I couldn‟t hack working
in a shop or things like that, so I just thought, oh. Everything‟s worth a try, ain‟t it, you don‟t know if
you‟re gonna like it or not until you try it. (RNHome2, Care Worker 3, age 21, 3 months in post)
Yes. My mother was a nurse, so yes. And she had a lot of experience in that area…Yeah. I think it
did [influence me] because she introduced me to care and she was quite passionate about what she
did as well, so I think it did have a big influence on my future. (RNLADP, Service Manager, age 45,
21 yrs in post)
Therefore many of the care workers had already had experience of informal care in the home
and knew what the job entailed. In relation to recruitment, this meant that on entry into the
sector many already had a reserve of tacit knowledge and skills that had been built up through
informally caring or having close relationships with those who did the job. How this relates to
the recruitment process will be discussed in the next section.
Care work as a new direction
Many of our interviewees talked about their entry into the care sector as a „career change‟. It
was often a result of a „push‟ factor into the sector; for example a change in personal or work
circumstances such as redundancy and divorce. The case study interviews allowed us to see in
practice how the recessionary effect, as discussed in Section III.1, eased recruitment
difficulties for providers. Of the 50 care workers who had entered the care sector in the last
two years, nine mentioned they had been actively looking for work before they started their
Part V. Recruitment and retention in the care sector: a case study
approach
307
current post and five of these had been made redundant39. Others had simply decided they
wanted to leave a job, often higher paid, that they were dissatisfied with and it was the „pull‟
factors of training and opportunities that made the sector attractive. Providers that emphasised
training and careers either in the advert or in interview were more successful at attracting
those who wanted a career in care. For these, working as a care worker was a stepping-stone
to something else or an opportunity to gain training and qualifications.
Box V.12. Care work as a new direction
I‟d been made redundant for nearly seven months. I found the job through a newspaper but a friend
of mine that was working for the same company had got made redundant at the same time, she‟d
applied here as well. And so I follow in the footsteps basically. (XDLADP, Care Worker 2, age 55, 4
months in post)
I was made redundant, sort of. And then approaching 50, I felt this was a good job that I could do
efficiently and well. (XDDom2, Care Worker 1, age 53)
I just wanted a complete career change. I didn‟t want to go in another factory. I just wanted
something totally different. And it is. (XDLADP, Care Worker 3, age 52, 7 yrs in post)
Well, I was obviously looking and came to my interview and like had an interview with Gloria and
she was like very helpful and like 'cos I came with no experience was more willing to give me the
experience I needed. Cos quite a lot of other place I applied for are a bit dubious with no
experience…..More helpful, more willing to sort of teach me and train me, very nice place.
(RNHome1, Care Worker 2, age 19, 6 months in post)
Because I am studying mental health nursing. So it‟s like a way of getting into nursing, so I know
how to care about people. Getting experience first…..I was just walking past. When I came in, I
asked them if they were going to train me, so that I know what I was going to do. (XDDom2, Care
Worker 3, age 28, 4 months in post)
Convenient working hours
The final dominant factor that shaped entry into the sector was the search for work that fitted
family circumstances or other interests. Ten interviewees identified the hours on offer in the
care sector as the main reason why they entered. As box V.13 makes clear, some care workers
were able to negotiate very convenient hours for themselves but often these were not
representative of the hours of work across the sector as they might involve limited weekend
work and hours that fitted around home commitments. Thus those expressing satisfaction
were doing so more with respect to their own specific hours, than those that typified the
sector. It is important to note that the care worker who chose to work for the inhouse service
39
The issue of redundancy and job insecurity prior to the care workers taking up their current position was not
part of our initial investigation and there were no specific questions relating to this. Therefore it may be the case
that at the time of the interviews recent redundancy may have been more common than the data suggests.
Part V. Recruitment and retention in the care sector: a case study
approach
308
because the hours fitted in with school hours may not have been able to negotiate these hours
if she was a new recruit and the types of hours she mentions are no longer typical. Indeed
others referred to the hours as a reason for deferring entry into the sector. The use of zero
hours contracts was mentioned; a lack of guaranteed work meant that anyone who was reliant
on a wage to bring up their family could not take a risk on the unpredictable hours on offer.
Therefore the case study interviews show that the pattern of working hours in the care sector
are far from being a „pull‟ for everyone.
Box V.13. Care work and working hours: a help and a hindrance in attracting a wider
pool of candidates
Why did you enter the care sector?
Because it is something to do with when you are both full-time and you have to juggle around the
time with looking after your kids and then the time working full-time as well. So it took me three
years to decide I need to get into the kind of job that would suit our time and schedule. Because a
clerical job is normally like office hours. It is not flexible enough. …I laid down my cards to [the
manager] - we have got the schedule ready, my wife and myself. And then I told him already when I
applied for this job, I can only work in the afternoon, …. (XDHome1, Care Worker 2, age 31, 6
months in post)
I'm in a new country and this is the second job I‟ve had, and I‟m really a clothing designer,… I like
how flexible the time is, so I can say that yes, I‟m available to work these days, and also .. I think
that was the main one but I enjoy working with people also but I would have to say being flexible
with my hours was the main reason [I entered the care sector]. (RNDom2, Care Worker 4, age 32, 2
weeks in post)
I left my job [at the hospital] because it was weekends and it was a split shift, so I literally done from
the seven till one and then had to go back and do five till ten, so it was giving up every weekend. And
then this one, when you were home helps you could start at nine and finish at two thirty, so I could
take my children to school and pick my children up from school, which I feel is an important thing to
do. (RNLADP, Care Worker 4, age 46, 20 yrs in post)
But the variability in the hours had been a pull away from the sector in the past for other care
workers
I‟ve wanted to do this forever but because I‟d two kids I couldn‟t, because of the hours (…) and I
was a single parent, so I needed a steady wage and steady hours. Which you don‟t get steady hours
in this job. (ONDom1, Care Worker 4, age 43, 5 months in post)
I‟ve always wanted to work with the elderly but whilst my daughter was younger, you can‟t easily do
the different shift hours. but once she got old enough I just said, well I‟m getting out of this, and
came into caring. (XDLADP, Care Worker 3, age 52, 7 yrs in post)
Part V. Recruitment and retention in the care sector: a case study
approach
309
V.2.2. Role of employers versus employees in access to information on care job
vacancies
The case studies were designed to investigate the recruitment process from the employee
perspective. In particular we wanted to know how people heard about care jobs and if they
were responding to a formal vacancy (employer-led recruitment) for a care job or whether it
was through informal means (employee-led).
Table V.6 shows that 45% of the interviewees heard about the job via informal means,
referred to here as employee-led recruitment, while 55% entered through formal practices or
employer-led recruitment. This pattern applied to both IDPs and care homes but three quarters
of those entering LAs did so through formal practices. Similarly, around three fifths of those
working for national chains or for single homes or agencies were recruited formally but this
only applied to 13% of the people who worked for a local chain.
Table V.6 Employer-led and employee-led recruitment
Sample
No.
Employee -led
Recruitment (%)
Employer led
Recruitment (%)
Domiciliary
40
43%
58%
Homes
38
58%
42%
LADP/ LA Home
20
25%
75%
Local authority
20
25%
75%
Local chain
16
88%
13%
National chain
48
40%
60%
Single home
14
43%
57%
98
45%
55%
a. By type of care provider
b. By Organisation Type
Totals
Formal recruitment in the case study interviews included press advertising or radio
advertising, placing an advert in a shop window, using the job centre or an employment
agency or advertising on the internet. Only three people mentioned finding out about the job
via the internet. We found that those looking to enter the care sector as a career change were
influenced by particular HR practices rather than informal knowledge and reputation.
Providers who emphasised training in advertisements made themselves attractive to a pool of
recruits that wanted a career in care and LA providers that emphasised secure employment,
quality of care and the adherence to strict procedures were also attractive to the care workers.
Employee-led recruitment took a number of forms; for some it involved ringing around
homes to see if there were vacancies or walking in to the office of the provider and asking if
there were any jobs. The most common way employee-led recruitment took place in practice
was through informal social and family networks; when care workers were asked how they
heard about the job or vacancy it was often friends or family who already worked for the
Part V. Recruitment and retention in the care sector: a case study
approach
310
agency that passed on knowledge about vacancies and shortages in specific providers and
encouraged them to apply. This informality was found across all four LA areas regardless of
the age profile in each case study local authority. This supports the survey findings that a
significant share of providers (43% of the managers in care homes, 23% of managers of IDPs
but none of the LADPs) found word of mouth recruitment to be the most effective method of
recruitment. The lower share among IDPs may in part reflect the higher share of national
chains in the IDP sample who made more use of formal methods.
Employee-led recruitment in practice
Box V.14 shows the ways employees can take the initiative and enter the care sector without
seeing a formal advertisement about a vacancy. The role of informal networks is central in
this process. Linked to this theme of networks is the localised nature of recruitment in the care
sector. Informal networks were effective because care workers worked in a very localised
area. This meant that chance encounters with friends who worked in the care sector could be
the way knowledge about opportunities was passed on. Fifty-seven out of 88 care workers
reported that they lived in or close to the area they worked 40. It meant that shop window
advertising and simply walking past providers who were visible was an effective way for
providers to recruit.
Box V.14. Employee-led recruitment in practice; informal and local knowledge
Informal networks and word of mouth recruitment
I got divorced and needed a change of direction; I fell into care as I needed a job and a friend
suggested [ILDom2]. I had heard about [ILDom2] and its reputation – there are now 4 providers in
[IL] and this is the leading one. (ILDom2, Senior Care Worker 1, age 39, 8 months in post)
Yes it was through my sister - actually one of our friends told us about the jobs here. And she also
works here. (XDDom2, Care Coordinator and Care Worker, age 23, 1 yr in post)
I heard good things from the person that worked here, and they pay better than some of the other
agencies, and those are the two factors… They‟re more organised than some of the other ones.
(RNDom2, Care Worker 4, age 32, 2 weeks in post)
Well, sort of when I first applied with [the agency] because my friend that works in this section had
put my name forward to them that‟s where I was offered the work. (RNLADP, Care Worker 3, age
43, 2 yrs 6 months in post)
I wanted to do it all the time but I thought it was hard to get into, and then a friend who I worked
with in the shop where I worked, her sister worked here, so it was like by word of mouth. So I just
40
However care workers had very different definitions about what travel-to-work distances constituted being
close to where they worked. For example, some care workers who lived three or four miles away from where
they worked responded that they did not live close to the area where they worked while others defined this
distance as being close to work.
Part V. Recruitment and retention in the care sector: a case study
approach
311
came along and just asked if there was any jobs going. (ONHome2, Care Worker 3, age 42, 2 yrs in
post
A friend that I‟d worked with in my other job and I saw her when I was out shopping and I said,
„You know, I‟ve had to give it up because of my back.‟ And she said, „Well, this is just a little rest
home that I work in.‟ And I thought, well, yeah, I can manage that. (RNHome1, Senior Care Worker,
age 54, 6 months in post)
So I decided, I thought right, perhaps I‟ll go to a nursing or residential home. So I just randomly just
rang all the nursing homes around like here, I think St Luke‟s. So I just randomly rang….I got an
application form from four of them, and then got an interview for two of them. And then I sort of
liked it here. So…It just seemed more friendly. (XDHome2, Care Worker 4, age 44, 3 yrs in post)
Well, I‟d applied for two, both care companies, and I got jobs at both, but the office for this one was
nearer to me than the office for the other one, so, and I was accepted first by [ONDom1] so I came
here. (ONDom1, Care Worker 3, age 49, 4 yrs in post)
Voucher schemes to encourage the use of existing care workers‟ social networks recognise the
pool of potential recruits that can be tapped into via existing employees. Three of our case
study organisations operated a voucher scheme (XDDom1, ONDom2 and ILDom1) which
involved offering, on average, a £50 bonus payment for employees who introduced a friend to
the sector which was paid once the person who introduced had worked more than 40 hours.
Interestingly these were national chains and the majority of the people we interviewed who
worked for these organisations were recruited formally (table V.6). However, it would appear
that national providers are increasingly recognising that word of mouth recruitment has been
operating quite well for many local providers and they are seeking ways of integrating this
recruitment practice into more formal systems.
In many respects this is unsurprising. It could be argued it is a more reliable method than
others, as the tacit knowledge that is gained from having family members and friends in the
sector manages the expectations of those entering the organisation and this may increase their
propensity to stay. It is also a reliable form of entry from the employee perspective. The
reputation of providers and knowledge about the employer is passed on by existing employees
which is an invaluable source of information when care workers are choosing between
providers. However, an increased focus on informal recruitment methods may have
implications for expanding and diversifying recruitment into care as we discuss in section
V.7.
Suitability of job applicants and the emphasis on informal experience and skills
We also asked all interviewees to describe their experiences of the recruitment process and
what skills and qualities the provider had looked for when they applied for the job. In line
with the general telephone survey findings reported in part III, all the independent case study
organisations identified a positive attitude and friendly nature as the most important factor in
assessing the suitability of a job applicant for a care job. The views of the LA providers were
Part V. Recruitment and retention in the care sector: a case study
approach
312
more mixed with two LADPs reporting a positive attitude was the most important factor and
one LADP41 (ONLADP) saying skills for care were the most important factor. Interviewees‟
accounts of the recruitment process (box V.15) show how providers value the informal skills
built up through experience of caring in the home. Many of the unqualified interviewees
appreciated being judged on this rather than formal qualifications.
Box V.15. The recruitment process and the stress on informal skills
There wasn‟t nothing on qualifications but it was all, because, like I said, mine‟s all basically down to
personal experience…… And like when they seen what I‟d done with family members and that it was
basically the same, it was the same as the job, if you know what I mean. (ILDom1, Care Worker 2,
age 34, 8 months in post)
My mum had dementia towards the end of her life. So I understood how that affects people as well. So
I had some sort of insight into that as well…..I told them about my dad and I told them about my
mother‟s situation towards the end of her life. And I suppose because I‟d been down that road already
and I knew the insights into what the job could probably be throwing at me, then they seemed to be
more than happy that I could probably cope with it………I don‟t remember them saying that you need
this and this, and they needed ... ….I suppose they took it on face value on my general attitude on
things like that. And I think to a certain extent that is a better way to look at people. Because I applied
for numerous amounts of jobs and I think to a certain extent because of my age as well, people
weren‟t looking at me. (XDLADP, Care Worker 2, age 55, 4 months in post)
No. They just asked what my exam results were. Which I couldn‟t remember. It was a very long time
ago. And apart from that, no. I had the interview and they didn‟t seem to want anything special.
(XDLADP, Care Worker 1, age 50, 3 yrs in post)
41
The ILLADP also said skills for care were most important but this was not included in the cases studies as it
was LAHome that was studied
Part V. Recruitment and retention in the care sector: a case study
approach
313
V.3. Care workers’ perspectives on turnover and retention
In this section we examine the intentions of the care workers we interviewed to stay with their
current employer and to stay in the sector and the reasons given for these intentions. The
problems of examining turnover from a sample of interviewees that does not include „leavers‟
has been discussed in section I.8. Nevertheless, through our case studies we explored those
aspects of care work that the interviewees did not like and also their perceptions and
experiences of why new entrants to care work may leave. Together these provide us with
some insights into the cause of staff turnover and staff retention.
V.3.1. Care workers‟ intentions to stay or to quit
Table V.7 gives a breakdown of the case study interviewees‟ intentions to quit: 89% of the
sample intended to stay in the social care sector and over half (54%) said they would expect
to be working for their current employer in five years time. Half of those working for care
homes (19 interviewees, all of whom were care workers) said they intended to stay with their
employer compared to only 38% of those working for IDPs (15 interviewees, 13 of whom
were care workers). Among those working for LAs, 90% intended to stay (16 of the 18
stayers being care workers). A further 4% of all interviewees said they probably would stay,
leaving 27% who said they did not expect to stay and 15% who were unsure.
Table V.7. Care staffs’ intentions for employment over the next five years
Sample
No.
Yes
(%)
Probably
(%)
Unsure
(%)
No
(%)
39
38
5
20
35
care homes
38
50
5
16
29
LAs
20
90
0
5
5
all types of providers
97
54
4
15
27
38
89
0
5
5
care homes
36
86
0
6
8
LAs
20
90
5
0
5
all types of providers
94
88
1
4
6
a. With current employer in 5 years?1
Workers in:
domiciliary care
b. In Social Care in 5 years? 2
Workers in:
domiciliary care
1
One missing response- domiciliary care worker
workers
2
missing responses- 2domiciliary care workers, 2 care home
Out of 26 who said they intended to leave, 22 were care workers and they gave a number of
reasons for intentions to quit. Working for the NHS and nurse training were the reasons most
often given for leaving. Low pay was only cited by one care worker as a reason to leave,
although the better pay in the NHS may mean that when care workers stated they intended to
Part V. Recruitment and retention in the care sector: a case study
approach
314
leave for the NHS, pay could be a factor shaping this choice. Pay is certainly an important
factor cited by managers as reported in part III. A quarter of respondents in the management
survey also identified working in the NHS as a reason why care staff leave (see section III.2)
but in many instances our case study data suggests that care workers were not actively
seeking work in the NHS. Instead it was often presented as an aspiration for the future, often
discussed in quite vague terms. The case study below gives an indication of the ambiguity of
some of the care workers‟ responses when they identified leaving the sector to work for the
NHS (box V. 16).
Table V.8 Reasons for care workers’ intentions to leave
Workers in all
provider types
(%)
19.2
Domiciliary
care workers
(%)
21.4
Care home
workers
(%)
18.2
Work for the NHS
19.2
7.1
36.4
Move to home country
7.7
To work in a different sector
11.5
14.3
Lack of support /no promotion
7.7
14.3
More convenient working areas
3.8
7.1
Better Pay
3.8
7.1
Work for another care provider
3.8
7.1
To work for the Local Authority
3.8
7.1
Retirement
3.8
Total responses
22
Nurse training
Workers in LA
care providers
(%)
18.2
100.0
9.1
12
9
1
Box V.16. Case study ONHome2: the ‘pull’ factor of the NHS
Summary
This provider was in an LA classified as „mixed‟ according to its commissioning practice and staff
reported high levels of job satisfaction despite being dissatisfied with staff shortages and low pay.
All care workers felt supported by their manager and one was studying for her NVQ 3. There were
opportunities to progress in the care home; for example, the manager had asked two of the staff if
they wanted to become senior care workers but they were undecided as to whether they would like
to do this because of the extra responsibility for little extra pay. Although they were happy many
aspired to move into working for the NHS in the future although they did not seem to have any
concrete ideas about how they would go about this.
Will you still be working for your current employer in 5 years time?
Possibly be here or I‟ve even considered hospitals and stuff like that, to sort of, well, I‟ve done this
for twenty five years, if I don‟t do it now I won‟t do it, type of thing. But on the whole I‟m content
where I am at the moment so if I was to move it would be …It would be something like the NHS.
(ONHome2, Senior Care Worker, age 43, 5 yrs in post)
Part V. Recruitment and retention in the care sector: a case study
approach
315
I think I‟ll still be in the caring profession, but I would like to work in the hospital. That‟s what I
want to do. (ONHome2, Care Worker 3, age 42, 2 yrs in post)
No. I don‟t know. Hospital, I hope. (ONHome2, Care Worker 1, age 47, 8 yrs in post)
I‟ll still be in this kind of job, whether it‟ll be in this place or not, I don‟t know. (ONHome2, Care
Worker 2, age 26, 3 yrs in post)
How I feel now I‟d like for to stay here, definitely…..but I say I‟d look at hospitals, that‟s in a
couple of years that I‟d look at the hospital. I‟m not ready for anything like that yet, definitely not.
(ONHome2, Care Worker 4, age 24, 6 months in post)
The patterns with respect to intentions to stay or quit were relatively mixed, with 58% saying
they would stay or probably stay and 42% saying they would definitely leave or were unsure.
Nevertheless the fact that only 27% of those we interviewed definitely intended to quit may
be influenced in a large part to the high level of job satisfaction reported by the care workers.
To explore these issues further, we also asked directly about what the job of a care worker
involved on a daily basis, what they liked and disliked about their job and also the nature of
their relationships with service users. All 88 care workers said they enjoyed their work. All
highlighted the rewarding nature of the job related to helping people, working with the elderly
and building relationships with service users. Care workers spoke with passion and
enthusiasm about their work and were clearly committed and dedicated to providing a good
quality service to users (box V.17). Significantly, they used their discretion in forming their
relationships with users and spoke of the need to adapt the ways they interact with different
users to provide a quality service.
Box V.17. High levels of job satisfaction: making a difference and building
relationships
They‟re elderly, they‟ve had their life and you‟ve got to make their last years or whatever as
comfortable as possible. To me, I would treat them as if they were my family. I mean some have
challenging behaviour but you just deal with it. You don‟t get aggressive with them, you just keep on
a level par with them. I mean some you can have a bit of banter with, some you can‟t, you know
which to step back from. But no, I love the job. Love it. (ONHome2, Senior Care Worker / Deputy
Manager, age 60, 9 yrs in post)
And you have to be understanding, you have to be able to understand your clients and make sure
that they understand you. And you need to be able to - not change so much with different people but
you know how you can talk to one client and how you can‟t talk to another. Everyone‟s different and
you just have to find a way with everybody. (XDDom2, Care Coordinator and Care Worker, age 23,
1 yr in post)
Making a difference to people‟s lives – making an impact – it could be a sociable thing, a wink of the
eye, a joke, any form of communication with them. If I don‟t get the wink from this man I know he‟s
not comfortable – and then I make him comfortable and then he winks. It‟s giving them something
Part V. Recruitment and retention in the care sector: a case study
approach
316
back for me. (ILDom2, Senior Care Worker 1, age 39, 8 months in post)
You go and someone can be very depressed the first time you meet him or her and then you going on
your days it can cheer them up, so you get job satisfaction. You know, I‟ve had clients that are
bedridden and now they‟re walking with a Zimmer because they‟ve had that encouragement. ..So it‟s
a lot of job satisfaction really, and it‟s very, very rewarding. (ONDom1, Care Worker 2, age 33, 6
months in post)
Levels of satisfaction were shaped by different aspects of the job, depending on the type of
provider they worked for (box V.18). Those working in homes identified the family
atmosphere of working in a care home and working as part of a team as one of the aspects of
the job they enjoyed. In contrast, those working for IDPs identified the autonomy of being
able to work unsupervised and not working in one place as one of the most enjoyable aspects
of their job42. Those working for LADPs also enjoyed working in different places and spoke
in terms of „working in the community‟ and focused on the challenging and rewarding aspects
of the re-ablement role that many of those working for the inhouse service were now involved
in.
Box V.18. Working in different types of providers brings different sources of job
satisfaction
Care Workers in IDPs
It‟s something different on your own, you‟re not in one place, somebody watching you while you‟re
working all time, you‟re out and about. (ONDom1, Care Worker 1, age 48, 3 yrs in post)
I feel as though I‟m my own boss, sort of like going around, and I feel as though I‟ve like helped
people, you know. (RNDom1, Care Worker 1, age 41, 11 months in post)
you‟re going in and making, you are making a difference to somebody. The only person they might
see that day. I just like chatting with them, socialising with them, just doing anything that I can to
help keep them in their own homes. (RNDom1, Care Worker 2, age 51, 2 yrs in post)
Care workers in care homes
I just think it‟s like loads of grans and granddads, it‟s like really close and family; and it‟s nice to
help people. It‟s just a nice thing to do; it‟s something to give back isn‟t it really. It‟s like having lots
of nans and granddads, and you all have different ways to talk and to interact with them, and you
know how they feel and you can make them happy and vice versa, if I‟m having a down day, they can
bring me up. It‟s just nice. (ILHome1, Care Worker 3, age 23, 3 yrs in post)
It‟s nice when you see a smile on the resident‟s face. It‟s nice helping, it‟s nice when you make a
difference to someone, it‟s like a family atmosphere as well. (ILHome1, Senior Care Worker, age 38)
I like that it‟s a small residential home. So everybody is looked after on a personal level. And the
42
Note two of the quotes are from RNDom1; further details on this case study are given in box V.32
Part V. Recruitment and retention in the care sector: a case study
approach
317
team that you work with have been here a long time so they know the residents and you get to know
them and you know their abilities. So you can help - if they need help and they can help you. It‟s a
good team. (XDHome2, Care Worker 3, age 26, 2 months in post)
Care workers in LADPs
I like the challenge of, there‟s nothing worse to me than when I‟ve got a client that you can‟t get to …
do what you know is, what is good for them, you know what I mean? I get a real sense of achievement
when I can get them to do something that they‟ve never wanted to do. You know, even if it‟s just like
having a wash, you‟d be amazed how many just won‟t wash, and when you can get a relationship with
them where they trust you, 'cos at the end of the day they don‟t wanna have somebody washing them,
because it‟s perhaps a final admittance that they need help, and when you can finally get them to let
you help them, I enjoy that. I enjoy, you know, the achievement of it. There‟s nothing more frustrating
to me than when I can‟t get somebody to help themselves really. (ONLADP, Care Worker 3, age 43,
14 yrs in post)
I love meeting people, I like the fact that you‟re not stuck in one place, you are actually out and about
in the community with clients that are not, you‟re not just in a care home, for instance, you are out in
the community with clients. (ONLADP, Care Worker 1, age 22, 11 months in post)
It‟s rewarding, it‟s challenging. Yeah. It‟s rewarding and it‟s challenging and I like the colleagues
that I work with. (RNLADP, Care Worker 4, age 46, 20 yrs in post)
I like people. I must admit I do, I like it, especially now if we‟re managing to get them sort of on their
feet more than they were before. I don‟t know, I can‟t imagine doing anything else, to be honest,
although I don‟t particularly wanna say I‟m gonna do it till I‟m 65, I can‟t imagine me doing
anything else. (RNLADP, Care Worker 2, age 45, 15 yrs in post)
This gave us a more complete picture of why, despite the low pay and uncertain hours, it was
only a minority of care workers who intended to leave. As we have seen, motivations to enter
the sector were often related to the nature of care work; being able to help others, to make a
difference, to do meaningful work and to build on rewarding personal experiences of informal
care in the home. Motivations to enter the care sector are important to understand because
these reveal the expectations about the job of those entering the sector. This has a direct
impact on levels of retention. It is often whether the organisation and the job can fulfil
expectations that determine job satisfaction and consequently whether people will stay or
leave. The descriptions above of care workers‟ feelings about their jobs reveal that in many
cases the role did fulfil care workers‟ expectations.
Part V. Recruitment and retention in the care sector: a case study
approach
318
V.3.2. Factors that may contribute to turnover
Insight into causes of turnover can be gleaned from responses to questions about those aspects
of the job care workers did not like (table V.9). Forty-two percent of the care workers
interviewed said there was nothing they disliked about the job. Of those who did report
aspects of the job they did not like, issues relating to pay (including the lack of compensation
for time spent travelling between users) and working time were most often mentioned. This
suggests that dissatisfaction is often related to the way care work is managed rather than the
job itself.
Table V. 9 Aspects of the job care workers were unhappy with
% of care
workers
Nothing
42.0%
Low pay / Lack of travel pay
19.3%
Working time
10.2%
Difficult clients
9.1%
When clients deteriorate / die
9.1%
Being asked to cover/absent staff
6.8%
Stressful/Chaotic/Exhausting
4.5%
Short staff
3.4%
Lack of autonomy / time
3.4%
Unpleasant parts of the job
2.3%
Travelling between users
1.1%
No promotion opportunities
1.1%
Not working in preferred geographical areas
1.1%
Working with agency carers
1.1%
Language difficulties
1.1%
More paperwork
1.1%
Increased Privatisation
1.1%
Expectations of male carers (to do heavy work)
1.1%
More responsibility and threat of litigation
1.1%
Total respondents =88
Part V. Recruitment and retention in the care sector: a case study
approach
319
Perceptions of why staff leave
The care workers were also asked why in their experience new recruits into care work may
tend to leave. Two main issues were mentioned: the nature of the job and the unpredictability
of working hours.
With respect to the nature of the job, many of the care workers said that those who enter,
particularly younger people, did not know what the job entailed and it was for this reason
many new recruits left quite quickly (box V.19). This contrasted with the personal
experiences of many of those we interviewed, who, as already mentioned, had experience of
informal caring in the home and/or had contacts working in the care sector before they entered
the sector. This meant they had some prior knowledge of what the job entailed. Their view
was that new recruits often expected it to be more like the traditional „home help‟ role and
those who left often had found the job to be more complex than they had expected.
Box V. 19. The nature of the job as a reason for staff quits.
I don‟t think they[new recruits] come into it with their eyes open. They don‟t think about what
domiciliary care involves, it‟s the old, I think they still think of the old home helps, when it was a bit
of cooking, a bit of cleaning, keeping them company, that‟s what they thought it was. You can tell
them what domiciliary care involves, but until they actually see it themselves then they don‟t actually
realise, and that‟s where we hit the problems. They go through all their theory training in the
classroom, you send them out, and I think that‟s when reality hits (ONDom2, Senior Care Worker 2,
age 36, 1 yr 6 months in post)
I think a lot of them went, especially young girls who are18, I think they come into it thinking it‟s
you‟re just gonna go in and make someone‟s tea and then they realise it‟s not that. You‟re gonna see
some distressing, you know, sights, especially when you go on double-ups, and they can‟t hack it, so
they‟ll go. It‟s not for them. (ILDom2, Care Worker 4, age 37, 7 yrs in post)
Mainly because .. a lot of it comes from the way you‟re paid, doesn‟t it. If you‟re not paid enough for
a job then people don‟t see it as a proper job, it‟s just a little part-time thing that people do. That‟s
how people see it a little bit. And that we just go round making cups of tea for people. (RNDom1,
Care Worker 3, age 50, 1 yr in post)
Another reason put forward by care workers for staff quits was the unpredictability of
working hours and the pressure to do extra hours because providers were often short staffed.
As we have seen in section III.4 a very high share of independent sector providers and LADPs
said it was easy, or very easy to find staff willing to work additional hours at short notice and
by and large providers tend to depend on existing staff to cover shortages. However, what the
survey did not tell us is that this could be a reason for staff turnover. Indeed, pressures to
change working-time arrangements had made one care worker leave her previous provider
(box V. 20).
Part V. Recruitment and retention in the care sector: a case study
approach
320
Box V. 20. Unpredictable working time as a reason for staff quits.
I mean it‟s not as easy as people think it is. I mean it‟s not a nine to five job, you know, it can be
unsocial hours, you do get mithered a lot from our end, 'cos you know, work has got to be covered. It
doesn‟t matter how many staff we‟ve got off there‟s still the amount of people to look after, and I
think a lot of 'em, you know, they get fed up of being pestered. It‟s not a job you finish, you go home
and you‟re left alone till t‟ next day. You try not to bother people but if work needs covering then you
have to mither 'em. (ONDom2, Senior Care Worker 2, age 36, 1 yr 6 months in post)
I was working from very early in the mornings, never .. they used to pester me night and day to work,
and when you‟ve got children you‟ve gotta have some time to yourself and I was never left alone so I
got alternative employment. (RNLADP, Care Worker 3, age 43, 2 yrs 6 months in post)
But it‟s mostly because of the hours [why people leave]. If you‟ve young families this job wouldn‟t
suit. (ONDom1, Care Worker 4, age 43, 5 months in post)
Part V. Recruitment and retention in the care sector: a case study
approach
321
V.4. Care workers’ perspective on pay and working time
V.4.1 Pay and travel time
Data was gathered on care workers‟ attitudes towards pay as well other paid benefits such as
enhancements for unsocial hours working and travel pay. We have seen that 19% of care
workers identified dissatisfaction with pay as an aspect of their job they did not like but we
have also shown that it was not cited as a reason to leave the sector, although it could be
argued the attraction of the NHS is linked to the better pay on offer in the health sector.
We asked all care workers whether they thought the pay they received for the job they do was
reasonable. Table V.10 gives a breakdown of care worker perceptions of their pay and shows
that out of a sample of 88 care workers, 35% thought the pay was reasonable, 64% thought it
was not reasonable (1% unsure). Those working in care homes were most likely to perceive
the pay as unreasonable; only four care workers out of 36 (11%) thought their pay was
reasonable.
Table V. 10 Care workers’ perceptions of pay as reasonable
Sample No.
% saying pay is
unreasonable
59
% who don’t
know
0
Domiciliary care
34
% saying pay is
reasonable
41
Care homes
36
11
86
3
LAs
18
72
28
0
All types of providers
88
35
64
1
By contrast 72% of care workers employed by LAs perceived their pay to be reasonable
comparing it favourably to the pay on offer in the independent sector. Significantly, it was not
only the basic rate of pay that was discussed by those working for LADPs; all of the LAPDs
in our sample paid for travel time and paid mileage and this was intrinsically linked to care
workers‟ positive perceptions (box V.21).
When IDPs followed similar practices, interviewees were likely to be more positive. For
example, in XDDom2 pay practices mirrored LAPDs; they paid mileage and travel time and
also good enhancements for unsocial hours. Three out of four care workers perceived their
pay to be reasonable in this organisation.
Of those who perceived their pay to be fair, there was often a reference to good weekend
enhancements. This varied by local authority: in XD, every provider paid enhancements for
unsocial hours but in RN and ON, while domiciliary care providers paid enhancements for
weekends, care homes did not. In contrast in IL, the cost minimising LA, three providers did
not pay enhancements including one IDP (see section V.1). Table V.11 shows that there was
a relationship between the LA the care workers worked in and the likelihood they perceived
the pay as reasonable. In the partnership authorities where fees were higher nearly half of the
care workers interviewed perceived pay to be fair (45% in RN and 48% in XD) compared to
Part V. Recruitment and retention in the care sector: a case study
approach
322
only 23% of care workers in IL. Care workers working for IDPs in the high fee paying
partnership LA of XD were more likely to consider their pay to be reasonable compared to
those working for IDPS in other LAs.
Box V. 21. LADP care workers’ attitudes to pay and non-pay benefits
I would say yes [it is reasonable] I know that they [the council] look after their staff better than the
private company, they pay better, their conditions are better, you know. (ONLADP, Care Worker 3,
age 43, 14 yrs in post)
Our pay is very good for what we do. I‟m not saying it‟s a piece of cake but when you compare our
pay to, especially private sector, we‟re very well paid… There‟s hundreds of agencies out there that
I could work for but their pay is far less than ours, and we have other perks as well, like travel.
(RNLADP, Care Worker 2, age 45, 15 yrs in post)
'Cos you see them advertising and I know people that are working, and on the whole a lot of them
are on like £6.50 an hour, and the main problem with agency and with us as well is they don‟t get
paid their travel time. So in between calls, whereas I know my next call now from here is about eight
miles away, nine miles away. Now, if I didn‟t get paid for that and I‟m in a traffic jam for half an
hour, 45 minutes I‟ve lost 45 minutes pay. So you‟re behind. (RNLADP, Care Worker 2, age 45, 15
yrs in post)
Regardless of which local authority care workers worked in, those working in care homes
thought their pay was unreasonable. Furthermore, the perception of pay as unreasonable in IL
shows that those working in local labour markets characterised by high unemployment were
just as likely to think the pay was unreasonable as those working in higher wage areas as the
quotation below shows;
I think we‟re grossly underpaid. I think we‟re in the firing line for all the mucky jobs and grossly
underpaid….It‟s minimum wage. It is a minimum wage city, isn‟t it. (ILDom1, Senior Care Worker
1, age 50, 1 yr 8 months in post)
Table V.11 Care workers’ perceptions of pay by local authority area
Number of care workers who perceived their pay to be reasonable
By LA
%
IDPs
Homes
LA providers
All
ON
2
0
4
6
29
RN
3
2
4
9
45
IL
3
1
2
6
23
XD
6
1
3
10
48
All 4 LAs
14
4
13
31
35
Part V. Recruitment and retention in the care sector: a case study
approach
323
Among the 56 people who said their pay was not reasonable for the work they do, a number
of themes arose in their discussions (box V.22). One of the striking findings was the absence
of any discussion of the employer‟s role in determining low pay. Rather, care workers talked
about the undervalued nature of care work in general and some appeared to accept a trade-off
between rewarding work and well paid work.
Box V.22. Independent sector care workers attitudes to pay and non-pay benefits
I just think it‟s a badly paid profession, it always has been and nobody‟s doing anything about it to
make it any better. I always think if they paid more money they‟d get a higher calibre of people
coming through anyway. (RNDom1, Care Worker 3, age 50, 1 yr in post)
I think it [the pay] should be a little bit more. But, like I say, I love the job, so I mean it‟s not an
issue with me…. (ON.Dom1, Care Worker 3, age 49, 4 yrs in post)
Working as a care assistant is generally not particularly well paid, but … to a certain extent the
reward is the job itself…. Knowing that you‟re able to make a difference to people‟s quality of life by
being there and doing your job properly. (RNHome2, Care Worker 4, age 48, 1 yr in post)
Yeah. I mean my son‟s in [ retail store], stacking shelves and he‟s on like £8 an hour. But it‟s not the
type of job that you can work for money, it‟s a job that you‟ve gotta like and love. (ILHome2, Care
Worker 1, age 50, 2 yrs 6 months in post)
Yes [it is reasonable]. I find that I like the work more, I like getting up of a morning and coming to
work more than I did previously. (ILHome1, Care Worker 1, age 30, 1.15 months in post)
Yeah. I think, I think maybe, I think pay would be a question if you didn‟t like what you were doing. I
think when you enjoy what you‟re doing, it‟s a bonus. (ILDom1, Senior Care Worker 2, age 45, 1 yr
6 months in post)
This data would appear to support the idea that care workers are „prisoners of love‟, accepting
low wages because of altruistic motivations and the intrinsic rewards of the job (see section
1.4). However, while the evidence suggests that some do accept the low wages because of
compensating rewards, these findings also need to be put into the context of care workers‟
previous work histories that have shaped their expectations about wages and job quality. The
majority of the sample had worked in low paid, low skilled jobs in sectors such as retail,
hospitality, administration, and factory work. These jobs were low paid and often described as
monotonous. In contrast care work was found to be more interesting and rewarding than their
previous jobs. It is the limited range of opportunities available to unqualified workers in
general that led the low pay in care work being at least tolerated as the opportunity to have
both higher pay and interesting work did not appear to be an option.
These influences can be illustrated when we look at younger workers‟ perceptions of pay (box
V.23). Half of the total sample of under 30s in the sample felt the pay was reasonable
compared to just over a third of the whole sample. Those who did consider it reasonable
tended to relate their experience in care work to their low expectations, based on their
Part V. Recruitment and retention in the care sector: a case study
approach
324
earnings in the past rather than to specific organisation policies. It is also notable that pay
tends not to rise with experience in care work, so younger staff may be more likely to
consider the pay reasonable than those with many years of experience in the sector.
Box V.23. Young people and perceptions of pay
Well, for my age it is, yeah. It‟s not too bad. (RN.Home1, Care Worker 2, age 19, 6 months in post)
Yes. I‟m not really bothered about how much I get paid. Because I feel rewarded because of what
I‟ve done. But the pay is fine, yes, it‟s alright. (XDDom1, Care Worker 1, age 18, 8 months in post)
It is more money, yeah .. in a nursery you would think you‟d get paid a bit more money …they‟re
putting their children‟s lives in your hands, you would think that you‟d get paid more, but you don‟t.
So it‟s nice to come here and feel like, you know, 'cos you get paid a little bit more you actually feel
you‟re being a bit more valued. Like they actually appreciate what you‟re doing. (RNDom2, Care
Worker 2, age 24, 1 yr in post)
Some care workers did voice criticisms of their employer‟s policy on pay and a minority
linked the pay to the commissioning practices of the local authority. As discussed above,
when policies about pay were discussed, it was often in relation to enhancements or travel pay
rather than the basic pay. It was the lack of these that was often at the centre of discussions
about pay when people perceived it to be unreasonable (box V.24).
Box V. 24. Lack of travel pay as a source of dissatisfaction
You‟re not getting paid for your distance you walk to, each (…) house, people‟s houses, just for what
you‟re doing….And I think you should get paid for your distance (…), 'cos that‟s all in your job.
….Because we have to go out to various places and pay bus-pass fares and things. And I don‟t see
why we should have to pay to go to work, if you know what I mean. (ILDom1, Care Worker 3, age
25, 1 week in post)
I‟d like to get paid from the time I start to the time I finish, instead of being paid just for the calls I
do. For example, I was out for 5½ hours yesterday in the evening. But I only got 3½ hours pay.
Because of all the travelling here, there and everywhere, by the time I leave home and the time I get
home, I was out for, as I say, 5½ hours. Which is a bit of a shame, because it‟s two hours of my time
that I‟m not getting paid for. And I do think to myself, oooh, that‟s the worst part of the job I
think…Our manager has tried putting it forward but it‟s up to social services, and they say “No,
we‟re not going to give you any more money”. So she can‟t give us any more money. (XDDom1,
Care Worker 2, age 37, 2 yrs in post)
The quotations in box V.24 show how some workers made links between the LA
commissioning environment and the lack of travel pay. The impact of commissioning
practices was also becoming increasingly felt through the implementation of electronic
monitoring. This was in place in two of the case study LAs and one care worker raised the
Part V. Recruitment and retention in the care sector: a case study
approach
325
issue of how this was affecting her pay because she may be told by service users to leave their
homes before she is scheduled to leave (see box V.25). As this practice spreads and becomes
more commonplace care workers may become more directly conscious of the role of the LA‟s
practices on their pay. Although electronic monitoring practices are designed to monitor
providers, the inevitable outcome is increased monitoring of care workers with potentially
negative impacts on their take home pay.
Box V. 25. Electronic monitoring and the impact on pay
So you only get paid for what you clock in for. So if you‟re there ten minutes, you only get paid that
ten minutes. …..Even if they say, “You can go now, I‟ve done everything, there‟s nothing else for you
to do. There‟s no point in you staying. You get on dear and get on with your other jobs”…..So you can
think you‟re getting a five hour shift and you actually end up only doing 3½ hours, because some of
the clients don‟t want you to stay, (XDDom1, Care Worker 2, age 37, 2 yrs in post)
This discussion of pay shows that dissatisfaction with pay alone is only part of the story when
trying to explain recruitment and retention difficulties. Pay may deter people from entering
care work and even among those who have entered, such as our sample of care workers, the
majority consider their pay to be unreasonable. Nevertheless, the majority wanted to stay in
the sector and with their employer. To understand this commitment further, other HR
practices relating to working time, work organisation and training are examined to see what
bundles of practices and trade-offs between particular advantages and disadvantages of the
job help create the group of „stayers‟ that our sample represents.
V.4.2 Working time
We have already discussed the somewhat conflicting findings relating to working time and
recruitment. Although working hours on offer in the care sector can be both a reason to enter
the sector and a reason to defer, in practice only nine care workers identified issues relating to
working time as an aspect of the job they were dissatisfied with.
Table V.A3 in the appendix gives a breakdown of the working hours of our sample of
interviewees. This shows that over half of the sample (54%) worked full-time hours (between
30-45 per week): this applied to 58% of interviewees in IDPs and 63% of those in care homes.
Although there were only 20 interviewees in the sample working for the LAs, these tended to
work fewer hours than those working in the independent sector: only 30% worked full-time
hours and 70% worked long part-time (16-30 hours per week). None of those working for an
LA worked over 45 hours compared to 18% of those in IDPs and 5% of those in care homes.
Although the sample is too small to generalise from, these figures suggest that social care is
far from a short hours, part-time work sector.
To explore the care workers‟ views on working time, we asked whether they were working
the hours they preferred, why they preferred these hours and if their employer was able to
Part V. Recruitment and retention in the care sector: a case study
approach
326
match their work schedules with their preferences. In the telephone survey five case study
managers said they matched care workers working time preferences all of the time, 14 said
they matched them most of the time and one LADP said they only matched preferences some
of the time. Care workers were in fact more positive about their working time arrangements.
Seventy-two out of 88 care workers said their working hours matched their preferences. Of
those who said they did not work hours that matched their preferences, the majority were new
recruits who wanted more hours, or disliked the fragmented and unsocial nature of the hours.
Eight said they had no preference or reported that they worked contracted hours which
implied limited choice over hours but they did not give any indication whether these were
preferred hours or not. Significantly, out of the eight care workers that reported they did not
work their preferred hours, five of these worked for LAs (out of a sample of 20 LA care
workers). This gives some support to a trend that was discussed in section V.1 where care
workers working for LADPs appear to have less working-time flexibility compared to those
care workers working for other providers. New recruits in particular who were often hired to
provide cover for holidays and sickness could work very varied hours. Many of these care
workers wanted to build up a round of clients and wanted more work. Dissatisfaction over not
being given enough hours could lead to the newly recruited thinking about leaving the
organisation because of the impact on their pay (box V.26).
Box. V. 26. New recruits dealing with the unpredictable and fragmented working time
in the care sector
I asked for 40 hours a week and I‟ve only been getting 21…..Yeah. Because I‟d rather have, do you
know what I mean, set hours like I thought it was, but when they, you know what I mean, when
you‟re starting they‟re not set out like that, they‟re just all different, so that was a problem for me.
I‟m a bit unsure whether to stay here or what. Gonna get back in touch with [employment agency].
(ILDom1, Care Worker 3, age 25, 1 week in post)
I need to work a certain number of hours in a week and I can only go on for like a certain length of
time and if I‟m not getting those hours then there‟s no point in me staying. (RNDom2, Care Worker
4, age 32, 2 weeks in post)
It can fluctuate quite a bit. I find it quite hard sometimes when I‟ve got a gap in the day that‟s over
eight hours. Like this morning I was getting people up. Then I‟m not on until around about 20 past 7
tonight when I‟ve got to go back out again. And I find it very hard. I find it - because you‟re just
winding down. The body‟s winding down and then you‟ve got to - and I‟m looking at the clock from
5 o‟clock on, just keep looking at the clock because you don‟t want to miss that. Because you have to
go out and do double ups and things like that. (XDLADP, Care Worker 2, age 55, 4 months in post)
Oooh, it can vary. I‟ve got 12 permanent hours I do a week and then I cover sort of hours for people
on holiday, things like that, and I can be doing about between about 18 to about 40 hours a week.
Sometimes more. (RNHome1, Care Worker 2, age 19, 6 months in post)
Sometimes I can do 25, sometimes 35, sometimes 40 or 50, depends on how much staff we‟ve got.
(ILDom1, Care Worker 2, age 34, 8 months in post)
Part V. Recruitment and retention in the care sector: a case study
approach
327
However, for some the fragmented hours were the reason why they entered the sector and
stayed. The split shifts in particular could fit in with school times if family or friends were
available to cover in the evenings and some older workers preferred them. Yet for others, the
hours were seen to be incompatible with a family life and, as we have seen in the recruitment
and retention discussion, they could be the reason for not delaying entry or for leaving the
sector.
Some care workers felt very dissatisfied with the practice of providers using existing staff to
cover shortages and the unpredictability involved in being asked to do hours at short notice.
One care worker was employed in an organisation with a very high turnover rate and there
was a sense that existing staff were constantly being asked to cover. She believed new staff
who did not like saying no to their new employer were doing too many hours and this made
them leave (box V.27). Another one talked about how difficult it was working unpredictable
hours;
Box V.27. Care workers not achieving work-life balance
..they‟re always ringing you up asking you to do extras all the time, can you do this, can you do that,
'cos somebody‟s rang in, you see. They‟ve just asked me now, 'cos it‟s my weekend off. I work every
other weekend and she just said, „Do you want to work this weekend?‟ I said no. ……I mean when
they [new recruits] first start they don‟t like saying no….They think, oh well, they‟ll think I‟m no
good at the job, so they end up doing all these extra hours what they don‟t really wanna do.
(ONDom1, Care Worker 1, age 48, 3 yrs in post)
I feel this is a hard job – you get attached to people, and it‟s a lot of care, and a lot of people can‟t
do it. It‟s like you are not appreciated, it‟s hard working, and its long hours, it‟s not fitting your job
round your life, it‟s fitting your life round your job. You don‟t know what you are doing one day to
the next hours wise. (ILHome1, Care Worker 3, age 23, 3 yrs in post)
However, for others the offer of more hours and the ability to earn more money by working
extra hours was the attraction of the job and the only way they could earn a living wage, thus
enabling them to stay working in the sector. The quotations in box V.28 are from care
workers working long hours, often over 45 hours a week. The opportunity to build up a
weekly wage through additional hours may be a further factor why a third of workers
considered their pay to be reasonable, despite the very low hourly rate of pay.
Box V.28. Long hours working to earn a living wage
It is the hardest profession, it is not reasonable. I wouldn‟t go for a £7 (an hour) job through
because I love this job. It is poor. I have to work an extra 20 hours per week to earn a salary – there
is no recognition as a profession. (ILDom2, Senior Care Worker 1, age 39, 8 months in post, 40-50
hours a week).
It‟s long days. I mean I started at quarter to seven this morning and I won‟t be finished till half
seven, quarter to eight tonight. I‟m off in the afternoon and then I‟m back on at three. If you‟ve got
Part V. Recruitment and retention in the care sector: a case study
approach
328
kids you just couldn‟t do it. -I work every hour they give me. …This is my first weekend off in about
six, seven weeks, I‟ve always done a bit of overtime for them. I‟m cream-crackered (ONDom1, Care
Worker 4, age 43, 5 months in post, 40-60 hours per week – 6.45 am – 7.45 pm).
But I used to do, that‟s what I‟m used to, you see. In my old home I used to do 72. But the thing is
you get used to earning a certain amount of money and if you cut that down to, say you‟re
contracted to 36, you think, oh God, how can I survive on that? (RN.Home2, Care Worker 3, age 21,
3 months in post, 48-60 hours a week).
'Cos if you want they‟re flexible, if you wanna do more overtime, if you wanna earn more money
there is more money sometimes there to be earnt. (ILDom1, Care Worker 1, age 29, 1 yr 6 months in
post, 30 hours a week)).
Yes. If I didn‟t do weekends, I wouldn‟t make up my money. (XDDom2, Care Worker 1, age 53, time
in post unknown).
For some care workers, therefore, satisfaction with hours may underpin their decision to stay
in the sector. Many talked of a trade off between hours that fit in with their needs and
circumstances and low pay, the former being the most important factor in their job choice at
this point in their lives. Fundamentally, while in many discussions of pay the employer was
not identified as a key agent, in respect of working hours a manager who showed flexibility in
hours scheduling was highly appreciated (box V.29).
Box V. 29. The ‘good employer’ as the one who matches working time preferences
They‟re really, really good. Yeah, we can choose our hours, and they‟re also very good, 'cos I look
after my mum and they‟re really good here if I‟ve got a hospital appointment or something like that
with her, they‟re absolutely brilliant with me. (RNHome2, Care Worker 2, age 56, 2 yrs in post)
And also it‟s like here they‟re very good, I‟ve a got a five year old and because my husband works in
the NHS, they‟re very good about swapping my hours around. I go to the person who does the rotas,
which has all come through Nick as well. It‟s not just me, there‟s other people with children that
need to change their hours and they really accommodate us. They work out who‟s on holiday and
they change your hours, so they are very good like that. (XDHome1, Care Worker 3, age 44, 3 yrs in
post)
We don‟t have guaranteed hours, so we only get what we‟re given. But the co-ordinators are
excellent. They do actually try and give us what they can and help us out. A very good team, very
good office. The ladies are lovely. (XDDom1, Care Worker 2, age 37, 2 yrs in post)
Part V. Recruitment and retention in the care sector: a case study
approach
329
Care coordinators realised how important this was for care worker satisfaction;
It‟s very important to us[that staff get preferred hours]. We don‟t work people outside their
availability unless they agree to work. If we wanted someone to do any extra, we would always ask
them, we wouldn‟t just give them work… Everyone, when they start, they fill in availabilities and
we do not work people outside these‟. (XDDom2, Care Coordinator and Care Worker, age 23, 1
yr in post)
Hours become important in recruitment and retention if we look at intentions to quit; a crosstabulation of the data demonstrates that those who were unhappy with their hours were more
likely to intend to leave their current employer (table V.12). Four of the eight people who said
they were unhappy with hours were likely to quit their employer and three out of five of the
care workers on contracted hours with no choice also said they would not be with their current
employer or were unsure if they would be.
Table V.12 Satisfaction with working hours by intention to stay with current employer
Sample No.
Intending to be with current employer in five years
% of care workers
Yes
Probably
Unsure
No
Happy with hours
72
56%
6%
17%
22%
Unhappy with hours
8
50%
0%
0%
50%
No choice offered*
5
40%
0%
40%
20%
No Preference
3
67%
0%
0%
33%
Total
88
55%
5%
16%
25%
*These interviewees did not say whether they were happy or unhappy with their hours
The above discussion has shown the idiosyncratic nature of the hours worked by care
workers. They are a result of a negotiation between the manager or care coordinator and the
care worker and what is a push factor for one care worker (getting asked to do too much
cover, getting split shifts) is a pull factor for others (getting the extra hours they need, getting
some wanted gaps in the day). In general in our case study organisations across all LAs the
providers‟ requirements for flexibility were met by staff and it would appear to be the case
that managers were by and large also meeting staff‟s requirements for flexibility.
Part V. Recruitment and retention in the care sector: a case study
approach
330
V.5. Care workers’ perspective on work organisation and the
quality of care
Managers‟ perspectives on whether the current system of work organisation was allowing
work to be carried out to a high quality standard were collected in the telephone survey. In
section V.1 we discussed the management perspectives on aspects of work organisation that
we have identified as particularly important in creating both good quality care jobs and
opportunities for care workers to deliver good quality care. This revealed that managers of the
IDP case studies, in particular, perceive there to be some limitations on workers‟ freedom to
prioritise and carry out tasks in ways to improve the quality of care. They also perceive some
restrictions, but not as many, on care workers‟ opportunities to develop good relationships
with service users. Nevertheless, the majority of the care workers we interviewed identified
the relationships with service users as a key source of job satisfaction, and many others
identified the autonomy they had as a reason why they liked the job. These divergent views
suggest there are some contradictions between managers‟ and care workers‟ accounts of how
work was organised. This section will explore these contradictions in more detail.
In the case studies we explored the extent to which care workers felt they were able to deliver
the best quality care. We asked about the concrete ways they could use their discretion to
improve the care they provided and also their ability to develop good relationships with users.
We were also able to explore the impact of the LA commissioning environment by
interviewing care workers who worked in LAs where electronic monitoring was in place. As
section V.1.6 has shown, managers from two IDPs that were part of the same national chain
but located in different LAs (XDDom1 and ONDom2) reported that care workers had low
discretion and that there were also some limitations on care workers being able to develop
good relationships. Both were in LAs where electronic monitoring was in place. We were
particularly interested in care workers‟ perspectives in these cases and if this LA policy and/or
provider policy shaped their experiences of work and their ability to deliver good quality care.
Boxes V.30 and V.31 use some of the qualitative data collected from care workers in
XDDom1 and ONDom2 to illustrate their experiences of discretion and relationships with
users.
Box V.30. Case study of XDDom 1: care worker perspectives in a ‘low discretion’
national provider in a partnership LA
Manager and coordinator perspectives: Staff do not have the freedom to prioritise tasks and do
not have time to spend time talking to service users. There are time constraints on staff delivering
the best quality care because of electronic monitoring and the increased paperwork this brings.
Management reported that although electronic monitoring is a good management tool they were
dissatisfied with the practice of using minute-to-minute invoicing.
Part V. Recruitment and retention in the care sector: a case study
approach
331
Care worker perspectives:
Time constraints but workers feel they can overcome these
Sometimes I find I haven‟t got enough time. But if that is the case and I find I go in there three or
four times, I found that I‟m taking more than the half hour I‟m given, then I will let the office know
and they‟ll ring social services, and say, this lady‟s going to need extra time, because our care
workers are taking longer. So it gets changed that way. As long as you open your mouth and say,
they‟ll do something about it. If you don‟t say anything, nothing will get done. So you have to speak
out and say. (XDDom1, Care Worker 2, age 37, 2 yrs in post)
There‟s always time. You make the time. And if it means you run over a few minutes then you run
over. But then on some calls you can only be there 10 minutes and it‟s a half an hour call. So you
do make up a bit of time. So you do what you have to do and I always say, is there anything I
should be doing. Even if it‟s not in the care plan. It might be put the washing on the bed, or put the
washing on the line. You do it. I don‟t see why people don‟t do it. I have terrible issues with people
who don‟t even do the basics like wash up and empty bins and things. (XDDom1, Senior Care
Worker, age 42, 3 yrs in post)
Task autonomy: changing the way you do things
Yes. Sometimes [I do change], yes. You‟ve got to remember, a lot of old people are set in their
ways as to how they want it to be. So that‟s how it is. But if you‟ve got an idea that can make their
life easier, they are open to it. But it depends if they like it or not. And you have to go with them.
It‟s freedom of choice. They choose, or their family chooses if they‟re not in the position to choose.
(XDDom1, Senior Care Worker, age 42, 3 yrs in post)
I‟ll just do it [if she finds an easier way to lift a client] And then I‟ll make a note of it in the care
plan, and then next time I speak to them [the office] I‟ll say, oh well I tried this, but everybody has
their own way. And if you‟re on a double up run, you both do it differently. But you work together.
As long as your aim is the same purpose at the end of it, you just do it. (XDDom1, Senior Care
Worker, age 42, 3 yrs in post)
Opportunities to develop relationships
Yes. I think it‟s vital that you go in and you speak about you. I don‟t think you should go in
miserable. And I know we all have bad days. But I think you should go in there upbeat and chat.
And talk about different things. …I‟m always talking about my family. My daughter did a sky dive
and one of the ladies I visit, sponsored her, so I took photos in to show her, even though she[the
user] ended up in hospital. …Because some of those people don‟t see anybody. They don‟t go out.
They sit in that house 24/7. So by talking about something completely different I think it‟s nice for
them. (XDDom1, Senior Care Worker, age 42, 3 yrs in post)
Box V.30 shows that in XDDom1 electronic monitoring does not seem to have affected
opportunities for care workers to develop relationships and „go the extra mile‟ in the way
managers and coordinators believed it had (although it did have an impact on pay, see section
V.1.2). The care coordinators were very aware of the issues that arise with electronic monitor-
Part V. Recruitment and retention in the care sector: a case study
approach
332
Box V.31. Case study of ONDom2: care worker perspectives in a ‘low discretion’
national provider in a mixed LA
Manager and coordinator perspectives: Staff do not have opportunities to prioritise tasks but are
able to develop relationships with users. There was a reluctance to encourage staff to exchange
ideas and best practice but continuity of care was considered to be very important and the manager
said time was built into care packages for care workers to be able to have time to develop good
relationships.
Are staff encouraged to exchange ideas with other care workers about new ways of working or best
practice?
A: Only at staff meetings, but obviously we have to be made aware of it first because it has to get
authorised, they wouldn‟t be allowed to just change things (ONDom2, Manager)
Care worker perspectives:
Lack of task autonomy
I think sometimes what annoys me, it‟s sort of your hands are tied a lot of the time, because we‟re
commissioned by social workers we can only do what they instruct us to do, and sometimes we‟re
the ones who are seeing service users on a daily basis and we‟re seeing what they need, and
sometimes it‟s not always easy to get them what they need, and I think that‟s frustrating. There‟s a
lot of red tape you have to go through. (ONDom2, Senior Care Worker 2, age 36, 1 yr 6 months in
post)
Not really, no [freedom to prioritise tasks]. 'Cos we have a care plan in each house we‟re stuck to
that care plan. But if someone‟s needs have changed we‟re told to ring the office and they get the
authorisation from social services then. (ONDom2, Care Coordinator and Care Worker, age 26, 5
yrs in post)
Time constraints and developing relationships
I don‟t feel we‟ve always enough time for to spend. Sometimes, if you‟ve a lot of service users to see
in a day, you can‟t give them the time they need. And I think that‟s the biggest constraint. You are
on a tight schedule because, you know, …
Q: Is there any way you can get that changed in terms of asking for a longer visit or …?
A: Well, it‟s not always … 'cos sometimes, you see the social workers assess the length of a visit on
what they need doing, but sometimes they don‟t take into consideration that they might just want
somebody to sit and chat to. (ONDom2, Care Coordinator and Care Worker, age 26, 5 yrs in post)
Continuity of care
You do build up, good relationships with some of your clients when you see them on a regular
basis. So you see them, you know, getting better, you can see some getting worse. It is a rewarding
job, that's why I do it. (ONDom2, Care Coordinator and Care Worker, age 26, 5 yrs in post)
'Cos we try and keep the same carer to the same service user. Keep it structured, which is a good
thing. (ONDom2, Care Coordinator 1, age 54, 2 yrs in post)
Part V. Recruitment and retention in the care sector: a case study
approach
333
ing (see section V.1) and when there are issues related to too little time these seem to resolved
with the LA. This could be the result of the good relationship between the LA and the
provider, rated four out of five in our survey. Although managers expressed the view that
there should be more time to sit with care users, in fact relationships are developing well in
this case often at the discretion of the care worker. Fundamentally it would appear that care
workers have more discretion than managers perceive them to have and the inherent
autonomy in domiciliary care may mean that care workers are able to be more flexible and
develop better relationships than the HR practices in theory would allow. As it is these aspects
that are cited as the source of their job satisfaction, it is unsurprising they are willing to invest
time and energy in building and deepening these relationships with users.
A contrasting picture emerges in ONDom2 as care workers‟ experiences would appear to
support manager perspectives. The lack of autonomy and reluctance to go beyond the care
plan echoed the management perspective. This organisation had a high level of turnover and
this combined with the unsupervised nature of domiciliary care work might be one possible
reason why the provider did not encourage discretion if many of the care workers were new
recruits and inexperienced. There was continuity of care but care workers reported time
constraints on their freedom to spend time with users which was not recognised by managers.
Electronic monitoring was not mentioned as a problem by the care workers specifically, but
the tight schedules that they said did not allow time to talk to users might have been a result
of this.
It is also useful to contrast these care workers‟ experiences with those who worked for
providers who reported different outcomes for care staff in terms of discretion and
relationships with users. Box V.32 gives the perspectives of some care workers working for a
provider in a partnership LA which sets KPIs relating to continuity of care. Box V.33 then
looks at the perspectives of those working for a provider in a cost minimising authority where
levels of discretion were reported to be high. We find that although the opportunities to
develop good relationships were there only to some extent, the manager did encourage care
workers to share ideas.
In box V.32 extracts from interviews with care workers show that the emphasis on continuity
of care at the LA and provider level is implemented in practice and shapes the care workers‟
experience of work. There are some limits on task autonomy but there were high levels of
satisfaction expressed by those working for this provider. It was a low paying provider
compared to other providers in RN but the care workers valued „being their own boss‟, being
unsupervised and caring for regular service users. In terms of delivering good quality care, it
would appear that care workers were able to do so because of the stress on continuity of care
and their ability and confidence to use their discretion and go „beyond the care plan‟.
Research with users shows that this kind of flexibility is valued by users (see section I.4) and
a shift to outcome-based care can have the effect of sanctioning some of the discretionary
behaviours care workers have been carrying out without little recognition in the past.
Part V. Recruitment and retention in the care sector: a case study
approach
334
Box V.32. Case study of RNDom1: care worker perspectives in a partnership LA that
emphasises continuity of care
Manager perspective: KPIs and incentive payments relating to continuity of care were built into
contracting arrangements. This provider was also piloting outcome-based care for the LA which
would move away from a task and time-oriented approach. The manager identified continuity of
care as very important but reported that workers could only prioritise tasks and develop
relationships to some extent. Outcome-based care was, however, providing more scope for care
workers to exercise discretion over how to provide care .
„Continuity of care is essential…It‟s one of our KPIs to the local authority, is continuity of care‟.
(RNDom1, Manager)
Care worker perspectives:
Task discretion
I go straight to the care plan and look at the tasks that are allocated, and then it‟s using a bit,
working round commonsense, what is appropriate and what isn‟t, and just say „Is there anything
else that you need me to do?‟ That‟s not perhaps on the care plan but within reason. (RNDom1,
Care Worker 2, age 51, 2 yrs in post)
Not being able to follow things through, if something needs to be done you have to hand back to the
office. I‟d quite like it if I could phone up the social worker and speak to them myself, and that sort
of business. Which I might be able to do soon if they let me be team leader. (RNDom1, Care Worker
3, age 50, 1 yr in post)
Autonomy and relationships
I like it because I‟m on my own and I‟ve got nobody breathing down my neck all the time and I just
feel that, you know, you are, it sounds a bit clichéd, job satisfaction, rewarding (RNDom1, Care
Worker 2, age 51, 2 yrs in post) (see Box V.18 for additional quotes)
Continuity of care
It‟s generally if you build up a relationship. When you‟ve got a regular service user, I do a lady
that I go in to five mornings a week for an hour, and then I do an hour and a half with her doing
her domestic, so it‟s continuity really. (RNDom1, Care Worker 2, age 51, 2 yrs in post)
Outcome-based care
There‟s a bit of both now because they‟re bringing in a different type of care plan where they can
choose a little bit more of what they [the user] have, rather than a set one that we‟ve always
had…..We make sure everything that we‟re supposed to be doing‟s done but there‟s loads of other
jobs that we do and a lot of that‟s in our own time…
Q: What kind of things?
A: Go to post office for them and post letters, pick up shopping, papers, newspapers, fish and chips.
(RNDom1, Care Worker 3, age 50, 1 yr in post)
Part V. Recruitment and retention in the care sector: a case study
approach
335
Box V. 33. Case study of ILHome1: care worker perspectives in a ‘high discretion’
provider in a cost minimising LA
Manager perspective: The manager reported that staff were free to prioritise tasks and were able
to develop good relationships to some extent, although she recognised this was often when they
worked on other tasks. They were encouraged to share ideas with her and continuity of care was
very important.
„When I asked for ideas/suggestions at a meeting, they didn‟t say anything, but I asked them to
write it down. We got some good suggestions, and when they were less shy, we got more. We try
them out‟ (ILHome1, Manager)
Care worker perspectives:
Time constraints on tasks
Sometimes you‟re, you know, obviously rushed off your feet and it can get quite hectic. (ILHome1,
Care Worker 1, age 30, 1.15 months in post)
They do [tasks] get done, just it is rushed a little bit. Like hoisting and things like that, and getting
them all to their meals. (ILHome1, Care Worker 2, age 21, 6 months in post)
Time constraints on developing relationships with users
No, not always, they sometimes think you can spend all day with them, but realistically, you can‟t
and sometimes they want it there and then – you learn to get out of that, you explain we have 42
residents and we can‟t possibly do that, especially if you have only five staff on. If it‟s full, it can be
hard. (ILHome1, Care Worker 4, age 30, 6 yrs in post)
Management support to exercise autonomy
[ Q. (How much) Are you able to introduce new approaches on your own to improve the quality of
care you provide? ]
A.
Well, it depends. I‟d ask the supervisor or [the manager] anyway, just to see what their
opinion is. (ILHome1, Care Worker 2, age 21, 6 months in post)
A. I would discuss this first with a supervisor. (ILHome1, Care Worker 4, age 30, 6 yrs in
post)
In the case study of ILHome1 there would appear to be some discrepancy between the
management perspective and that of the care workers. The manager did not mention that staff
shortages were affecting work organisation in contrast to the situation described by her staff
although she did recognise that relationships often had to be developed while care workers
were doing other tasks. However, the care workers identified problems when the service users
wanted them to stop all other tasks and devote time specifically to their relationship needs.
Care workers felt they could use their initiative but only if supported by management.
Fundamentally, it would appear that, despite the manager‟s best intentions, time constraints
Part V. Recruitment and retention in the care sector: a case study
approach
336
were affecting the quality of care that staff were able to provide. Interestingly, although this
group of workers experienced time constraints as a source of frustration, the care workers
working in this provider cited pay as the aspect of work they were dissatisfied with and they
linked it to the fact that the job was „very hard work‟. This would suggest that dissatisfaction
with low pay can increase when work organisation and staff shortages mean care workers‟
experience their daily job as rushed and hectic.
Part V. Recruitment and retention in the care sector: a case study
approach
337
V.6. Care workers’ perspectives on training and development
In this section we look specifically at how training and development practices of providers
can affect recruitment and retention. This section will firstly give an overview of the level of
qualifications attained by the sample of interviewees and identify any trends relating to the
commissioning environment and type of provider. We then go on to discuss the care workers‟
views on training and their aspirations for development and promotion. These are discussed
in relation to their effect on intentions to stay with their employer and in the sector.
V.6.1 Experiences of training
Levels of qualifications
Table V.13 gives an overview of the NVQ levels of all of the interviewees across the case
study providers. The share of interviewees with NVQ level 2 qualifications ranged from 53%
in IDPs, 61% in care homes and 85% in LA providers. There were fewer differences in the
shares with NVQ level 3, with 35% of those in IDPs, 34% of those in care homes and only
25% of those in LA providers with this qualification. Those working in LAs pursuing cost
minimisation or mixed strategies were more likely to have NVQ levels 2 and 3, RN had the
lowest number of staff with NVQ level 2. We found only one example of a more obvious
relationship between commissioning strategy and level of training; the high proportion of
NVQ level 3 trained staff in ILDom2 was the result of the block contract they had with the LA
for hospital discharges that stipulated care staff working on this contract should be trained at
this level.
Table V.13 Qualification levels of interviewees
NVQ2
Total
Yes
(%)
Due to
start
(%)
NVQ3
Yes
NVQ4
Nursing
qualification
Yes
UK
Non-UK
(%)
Due to
start
(%)
(%)
(%)
(%)
Working in:
Domiciliary
40
53
10
35
3
0
3
0
Care homes
38
61
8
34
5
5
3
8
LA providers
20
85
0
25
0
10
0
0
All provider types
98
62
7
33
3
4
2
3
ON
25
68
8
56
0
8
4
0
RN
22
55
5
27
0
5
5
5
IL
26
69
0
38
0
0
0
0
XD
25
56
16
8
12
4
0
8
By LA
Part V. Recruitment and retention in the care sector: a case study
approach
338
Experiences of training and links to retention
Our interview data revealed that in general the new recruits and more established care staff
reported positive experiences of training. Induction was perceived as useful by the majority of
the sample, including both new recruits and stayers. Induction can be the first signal to an
employee about the value the employer places on its workforce and can also provide the staff
with a realistic introduction to what the job of a care worker involves, thereby the likelihood
of staff quits where new recruits find the job to be different to expectations. Some of our
case study organisations prided themselves on the training they gave and workers appreciated
the opportunities this brought to help them do their job well (box V.34).
Box V. 34. Positive experiences of training
They do push us to learn more, which is good. And training wise we got all the training that we
need. ...It‟s very helpful, yes they‟re all very helpful, all the training. Made us more confident in
what we are doing. Like manual handling, we become more confident. With dementia training we
become more confident about dealing with people with dementia. We get to understand them and we
become better in the care that we are providing. (XDHome1, Care Worker 2, age 31, 6 months in
post)
Well the training is just absolutely brilliant. The best. It really, really is. It‟s all practical as well
as theory. ….I think [the manager‟s] trying to encourage everybody to do the NVQ. Because it is
interesting, you learn a lot from it. (XDHome1, Care Worker 4, age 32, 2 yrs in post)
Well, I‟ve taken loads of courses. I‟ve taken a lot of courses in dementia. So I‟m really interested in
dementia. Yes. I‟ve been lucky. I‟ve gone on a lot of courses. If I‟ve been interested in something,
they found a course that will cover it. (XDLADP, Care Worker 3, age 52, 7 yrs in post)
While low pay was rarely seen to be the fault of the employer, opportunities for training led
care staff to think of the organisation they worked for as a „good employer‟. Box V.35 gives
examples of care staff working for very low paying providers discussing the reasons why they
value the training opportunities they have been given. These staff often had no or little
opportunity for pay progression when they have completed training, so financial reward was
not the motivator. Significantly, these workers had no or very few formal qualifications and
valued the opportunity given by a sector that offers a rare opportunity for unqualified workers
to gain a qualification.
Box V. 35. Care workers and training: a chance to gain qualifications
I did my NVQ 1. I did that in caring here. And that‟s about it really. I‟m gonna try do my NVQ2. I‟ve
no qualifications with school. Just what knocks me back on that at the minute is like my reading and
writing, so I‟m gonna try and get round, I was at college at one point doing it, it‟s only through me
not going to secondary school through my accident. …And with me having my accident my
confidence went….and I was a bit like behind with my reading and my writing and I didn‟t think that
Part V. Recruitment and retention in the care sector: a case study
approach
339
I could ever get the chance, and then [the manager] give me the chance and I loved it. (ONHome2,
Care Worker 4, age 24, 6 months in post)
I‟ve got my NVQ2, I‟m in the middle of doing my level three, I‟m also doing a safe medication
course as well. Unfortunately I didn‟t get no GCSEs or anything at school. Well, I‟ve just, I started
off as a carer and I‟ve worked my way up as a senior, and I think up to now that‟ll be like the highest
I can get in this place here, but I wouldn‟t mind like going further up, like management or even
owning my own home or something like that…. If I had the opportunity I would definitely take it,
yeah. (ONHome2, Care Worker 2, age 26, 3 yrs in post)
They do tend to give everybody a chance here, which is nice. They‟re not judgemental and they‟ll
listen, 'cos I‟ve been here and been listened to, you know, so …And they do do a lot NVQ levels with
the skills for life, English and Maths, so they‟re helping people that are perhaps from a
disadvantage, do you know what I mean? (ONDom1, Care Worker 2, age 33, 6 months in post)
Some care staff identified negative aspects of training, relating to the time it took and their
lacked of basic reading and writing skills. However, more often any negative views about
training related to it being too theoretical and class-based which fitted in with the positive
accounts given above where training is valued because it can be put into practice (see box
V.36).
Box V. 36. Preferences for practical induction and training
We did the training downstairs and it was just someone going over basically all the information
about Plan and stuff like that….I found it a little bit useful, but I‟m the sort of person that learns
from actually going out and doing the job and not sitting …. I mean the only time that she showed us
a bit of information and we had to do it for ourselves is when we were learning to do the hoists and
stuff like that. I preferred my shadowing, even though I didn‟t get to do much 'cos I‟m just observing,
I still got to see it from that point of view. (RNDom2, Care Worker 2, age 24, 1 yr in post)
I found the training, because I went straight into training, confusing. Because I‟d never done the
job. It was alright the first day, that was interesting. But by the end of two weeks it was psh, psh, psh
- going over my head. I hadn‟t been out in the field….I think it would have made more sense if you‟d
have done a bit of training, gone out in the field, and shadowed, seen how things worked and
progressed and you could slot what you‟ve just learnt into what you‟re seeing in practice. And then
go back and do a bit more training. (XDLADP, Care Worker 2, age 55, 4 months in post)
There were also many examples of staff who were happy with the training they received but
who wanted more specialist training that was not related to meeting statutory regulations but
related to the needs of specific users they cared for. In particular dementia training was
mentioned by care staff as a form of training many would like the opportunity to have (see
box V.37).
The data across all case studies show that in general care staff valued the training on offer and
this was particularly the case when they were able to train in areas that were relevant to the
Part V. Recruitment and retention in the care sector: a case study
approach
340
specific needs of users. When employers offered extensive training, care staff often came to
define their employer as a „good employer‟. However, positive perceptions about training did
not necessarily mean that care staff wanted to progress to more senior levels.
Box V. 37. Learning opportunities that are user-led rather than regulation-led
I‟d like to do both the Alzheimer‟s and the dementia, 'cos I have been to a few clients who have got
that. (IL.Dom2, Care Worker 2, age 20, 3 weeks in post)
There are other areas that I‟ve not been trained for that I would be interested in
doing…..Alzheimer‟s and dementia and Parkinson‟s. And now we‟ve someone that‟s got MS and
I‟m interested in that as well. So - and it all helps to understand. (XDLADP, Care Worker 4, age 58,
11 months in post)
Then I‟ve had different individual training at certain houses, depending what the client needs. Some
people you have to be trained to do certain tasks. We have a lady where she had a peg feed, where
you feed her internally with liquid. I was taught how to do that. There‟s a lady who has liquid
medicine. We have to be taught to do that. We‟re not allowed to just go and give liquids. We‟ve got
to be trained. (XDLADP, Care Worker 1, age 50, 3 yrs in post)
I‟d like, well, we do a dementia course but I‟d like to go further into it..More depth, you know, more
understanding about it. (ONHome2, Care Worker 3, age 42, 2 yrs in post)
I‟ve had medication training in the other place I used to work, had it all the time. But I‟d like
dementia training especially, I think, because dementia, it‟s a thing everybody can suffer with, isn‟t
it, quite a scary thing (RNHome1, Senior Care Worker, age 54, 6 months in post)
V.6.2 Development and opportunities training
Restricted career ladders have been identified as a reason why it is difficult to recruit and
retain in the social care sector and the importance of linking training with career ladders has
been identified. Because of the methodology used in the project, we are unable to say whether
the lack of development and career opportunities have been deterring people from entry.
However, in relation to retention we are able to look at whether the care staff we interviewed
had aspirations to progress and if this shaped their intention to stay or quit working for their
provider. We asked all care staff whether they would like to progress in the organisation.
Thirty care workers out of 88 said they wanted to progress, 57 said they did not and one was
unsure. There were no trends relating to type of provider or age, with older workers just as
likely to want to progress as younger workers.
Of those that wanted to progress, some interesting trends can be observed. Firstly, seven out
of nine men wanted to progress; the two men who did not want to progress were in their 50s
and 60s and said they were too old. For the men who wanted to progress, a lack of
opportunities to do this was a reason to leave their employer in the future (see box V.38).
Part V. Recruitment and retention in the care sector: a case study
approach
341
However, as men made up a very small minority of our sample it is difficult to generalise and
the attitudes of men in care work must be a key area of future research.
Box V. 38. Development opportunities as a retention factor for men
The only way that I can explain it is that I asked - because obviously I‟ve got an NVQ 2, I said to her
[the manager] basically, everybody else is doing their NVQ 2, so I would like to do my NVQ 3. And
[she] turned round and says, we don‟t let you do your NVQ 3 because we cannot promote you.
That‟s not a good excuse really…obviously because of that reason I won‟t stay here. But yeah I
would stay in social care. (XD.Dom2, Care Worker 2, age 32, 1 yr in post)
I wanna do, I‟m thinking about doing my [NVQ] level four after Christmas, or I would really like to
do my RMA [Registered manager‟s award].…I either wanna do like the manager‟s side or I‟d like to
go to university and become a mental health nurse, so sort of like one of the two…..if I got to like a
point within the home where I thought I‟m not gonna get any further, I would have a look around
and if an opportunity come up then I would take it. (RNHome2, Care Worker 3, age 21, 3 months in
post)
Secondly, many who said they wanted to progress did so while anticipating barriers to doing
so. While the lack of part-time positions in professional occupations has been highlighted as a
barrier to women‟s progress, it would appear that in this female-dominated occupational
group there is little room for part-time senior positions, or at least this is the perception of care
workers (box V.39).
Box. V.39. Obstacles to progression
I became a senior, and that was hard work, but with my life the way it is with my young children, I
decided that I couldn‟t keep the devotion up as a senior, so I went back down to being a carer, so
I‟m doing that now….It‟s not a lot more work, it‟s just the company do put a little bit more pressure
on you, because you‟re a senior. They think that you should - well they don‟t think, but they expect
you to take calls on because you‟re a senior, they expect you to take the calls, and it‟s very, very it‟s quite hard. And with young kids I just found it too much. (XDDom1, Care Worker 2, age 37, 2
yrs in post)
I think moving up to senior, it‟s just the hours that stop me doing that, because I can‟t work enough
– I‟m not flexible you see. (ILHome1, Care Worker 4, age 30, 6 yrs in post)
The reasons care workers reported for not wanting to progress were threefold; firstly the
limited reward for a senior post that involved a lot more responsibility and stress; secondly
the opinion that a senior role involved taking care workers away from the job of caring; and
thirdly family responsibilities and circumstances that meant they could not work the hours
required to do a senior role. Interestingly, some had been offered senior roles and declined
Part V. Recruitment and retention in the care sector: a case study
approach
342
them or had had them in the past but returned to a care worker post because they either felt it
was too much work or preferred to be caring for users (box V.40).
Box V.40. Care staff rejecting opportunities for progression
I could. I was offered the job of a senior but I think, it‟s not even a pound extra an hour, so I will not
take on the responsibility of this whole home for that sort of money. (RNHome2, Care Worker 2, age
56, 2 yrs in post)
I was actually a senior carer, I was the first senior carer here, but all the responsibility of all the
phones and all this I didn‟t want, so I chose to go back to be a carer because I enjoy the job, I love
the job, you know, in the field, it‟s a totally different job. (ONDom1, Care Worker 3, age 49, 4 yrs in
post)
I suppose I could be a supervisor, but there‟s not that much, I could go to supervisor and I think that
would be it. Yes, and no, the amount of work load and responsibility they have on them is a lot. I
can see that because that‟s what my mum does. For a minute amount of money for the amount of
responsibility, it‟s just not worth it. (ILHome1, Care Worker 3, age 23, 3 yrs in post)
These comments (box V.40) shows that the increased responsibility associated with a senior
role was difficult for many with families, especially when it was paid poorly and took care
workers away from the direct care of service users. As we have seen, job satisfaction was
largely derived from working with users. As such, the reluctance of some care workers to
progress seems related to the perception that a more senior role would involve more
paperwork and less caring (see Box V.41). It is also worth noting that there was very limited
interest among the care workers we interviewed in taking up roles as personal assistants.
Sixty-three care workers were asked whether they would be interested and of these 44 said
they would not even consider it, while only ten said they were interested and a further four
said possibly (five said they did not know). The majority of care staff expressed the view that
they would not even consider a job as a personal assistant but ten of the 63 who were asked
did say they might be interested. The minority of care workers who would consider it
mentioned that one-on-one work of this kind could potentially be more rewarding and would
also have the benefit of being less rushed than their current role. However, for the majority of
care workers the one-on-one nature of the personal assistant role was not appealing. Many
mentioned how it would be emotionally draining to care for only one user and many felt they
would become too involved and be unable to cope. They identified aspects of their current
jobs they would miss if they were to become a personal assistant, including opportunities to
meet lots of different people, being able to move around autonomously and have the support
of managers and colleagues. Some would not consider it because they wanted the „back-up‟
of management and working in a team and they also anticipated increased job insecurity in
such a role if work was reliant on specific users.
Part V. Recruitment and retention in the care sector: a case study
approach
343
Box. V.41. Progression as a move away from hands-on caring
It‟s not, it‟s more about paperwork at senior and medication. They do do care and that but I‟d rather
be caring and more hands-on, definitely. (ONHome2, Care Worker 4, age 24, 6 months in post).
I don‟t know if I would [like to progress], because then you don‟t get to do the care. See I like the
care. (XDDom1, Senior Care Worker, age 42, 3 yrs in post).
No. I do .. because the next level up from me would mean giving my care up, you see. The next level
up from me is a coordinator, which is office based. So I do like being out on community, so for to
move up I‟d have to have sort of reached that stage where I don‟t want to actually do hands-on any
more, so to speak. (ONDom2, Senior Care Worker 2, age 36, 1 yr 6 months in post).
I suppose if we went to … be senior carer or whatever, that entails an NVQ3, I don‟t wanna be in an
office. I just don‟t. I don‟t, I wanna be on the floor. (ILLAHOME, Care Worker 2, age 49, 21 yrs in
post).
In summary, positive experiences of training may improve retention in the sense that care
staff felt valued by their organisation. Crucially it was also another means to ensure they were
providing good quality care to users, a key source of job satisfaction. Case-study data also
revealed why a lack of career opportunities may not necessarily be a reason to leave the job or
the sector. Care workers valued hands on caring and opportunities for progression typically
represented a move away from this. Moreover, the more senior roles demanded very high
responsibility with very limited improvements in pay. The examples of care staff that prized
training in the low paying organisations shows the importance of recognising how employees
can feel valued and supported by employers, even if in receipt of a low wage. However, we
have shown this depends on the experiences and expectations of the particular care worker
and we cannot assume this group is typical. For example, in order to expand the potential pool
of applicants, for example to men or to women with more qualifications and career options,
these potential new recruits might be less willing to make the trade off between opportunities
to gain qualifications and low pay. If this is the case, the creation of senior posts that are both
more rewarding financially and that do not involve such a leap away from care work, possibly
involving more specialist care roles rather than only supervisory roles could help to make care
work a more attractive opportunity for those who both wish to enter the sector to care but also
to have opportunities to develop and progress.
Part V. Recruitment and retention in the care sector: a case study
approach
344
V.7 Summary and conclusions
In section V.1 we compared the HR practices of providers across the case study LAs. This
overview found variations among providers in the same LA as well as across LAs. The LA
commissioning environment appears to have more influence on some aspects of HR practice
more than others: for example pay and the nature of contracts offered to care workers were
related to being in a higher fee paying LA, but the improvements were only marginal. In other
aspects such as training and working time, firm level policies are even more significant with
limited effects from the LA commissioning and contracting. Using case-study data to
compare and contrast the practices put in place by the same national providers located in
different LAs shows we find that the policies of national chains are playing a significant role
in both shaping HR practices and in limiting the actual impact of favourable commissioning
practices on employment terms and conditions. These findings suggest that the LA
commissioning environment may be an enabler of better practice but there are variations
between providers in the extent to which they respond to more favourable commissioning
practices. Furthermore, although there is variation in practices across providers this variation
is around a very low level of basic employment conditions and protections.
Sections V.2 to V.6 explored the experiences and perspectives of care workers and identified
a number of trends. The recruitment process in the social care sector is characterized by a high
degree of informality, particularly in the independent sector. Care workers‟ informal
experiences of caring in the home often lead them to want to do the job and care workers use
family and social contacts and networks who are already working in the care sector to access
information about the nature of jobs and vacancies. Employers are complicit in this
informality and in some ways actively encourage it. Providers identify attitudinal qualities
rather than formal skills as the most important factor when assessing the suitability of
candidates and some national providers are trying to formalise the use of „word of mouth‟
recruitment by using voucher schemes which reward existing care staff with a bonus if they
introduce a friend to the job.
We found that just over half of interviewees anticipated that they would still be working for
their current employer in five years time and 85% intended to stay working in the social care
sector. Only 10% of care workers working for LADPs intended to leave their current
employer. Of those who intended to leave their current employer, going to work for the NHS
and/or undertaking nurse training were the reasons most often given. However, only 27% of
interviewees said they definitely intended to leave. This may be considered unsurprising
because the case study revealed high levels of job satisfaction. All 88 care workers enjoyed
their work, in particular the rewarding nature of the job, helping others and relationships with
service users were given as reasons for high levels of satisfaction. Care workers working for
IDPs also mentioned the autonomy the job brings as a reason for enjoying the job.
However, care workers also reported low satisfaction with pay. Fifty-six care workers out of
88 believed their pay to be unreasonable and there was particular dissatisfaction with the lack
of travel pay and pay for unsocial hours. They also had concerns that the spread of electronic
Part V. Recruitment and retention in the care sector: a case study
approach
345
monitoring might reduce their total reward still further by restricting paid work time to time
actually spent in people‟s houses rather than at work. In contrast those working for LAs
expressed high levels of satisfaction with their pay, in part because they were aware of the
poor conditions in the independent sector.
Care workers were more satisfied with working time. Many had entered the sector because it
offered convenient working time and 72 out of 88 care workers said their working hours
matched their preferences, although care workers working for LADPs were less likely to work
their preferred hours. Care workers who did not work hours that matched their preferences
were more likely to intend to leave their current employer, although we cannot say whether
this was a direct reason for their intention to leave. Care workers, especially new recruits,
were working variable and unpredictable hours to cover shortages and holidays and the
idiosyncratic nature of the hours worked by care workers was a key finding. Hours were
highly fragmented and did not conform to standard family friendly working time and this had
led some to defer entry into the sector in the past. While the care workers we interviewed
were in general happy with their working hours, the hours suited care workers with very
specific needs and circumstances who often needed to work locally.
In general the new recruits and more established care staff reported positive experiences of
training and the offer of training had attracted some into the sector. Opportunities for training
led care staff to think of the organisation they worked for as a „good employer‟. Significantly,
these workers had no or very few qualifications and they valued the opening for unqualified
workers to gain a qualification. The provision of training and development opportunities
appeared to be an important way in which providers could show care staff that they were
valued. There were some contradictory findings relating to care workers‟ aspirations to
progress. On the one hand the limited opportunities for progression were not perceived as a
problem because many care workers said they did not want to progress, although this was not
true for the small sample of men interviewed. However, one of the reasons the female care
workers gave for not wanting to progress was that senior jobs involved far more extra
responsibility for limited extra reward. Another important factor was that senior roles also
involved taking them away from the hands-on care that was key to their job satisfaction.
The findings on work organisation revealed some contradictory results. We particularly
focused on care workers‟ opportunities to prioritise tasks to improve quality care and their
opportunities to develop good relationships with service users. While some providers reported
care workers had low discretion and also faced constraints in developing relationships, care
workers accounts revealed care workers continue to use discretion despite some constraints
in time and continue to be flexible and go „beyond contract‟. The extent of discretion varied
by context. Thus a national provider operating in LAs that had put in place electronic
monitoring was found not to offer much scope for discretion. However, a case study of a
provider operating in an LA that had established KPIs relating to continuity of care for
providers was found to allow care workers much more scope to go beyond contract. The
opportunity to develop relationships with users allowed room for discretion and in this sense
care work was not found to fit the standard classification of low paid, routine work.
Part V. Recruitment and retention in the care sector: a case study
approach
346
This finding that care workers do use discretion to improve the quality of care and develop
relationships is important because research on users‟ perspectives shows that the attitudes of
care workers and their relationships with care users are central to users‟ definitions of quality
care. In particular care workers‟ willingness to be flexible and do jobs beyond those stipulated
in the care plan are of particular importance alongside a caring attitude. This definition of
good quality care fits into the definition of a good quality care job as defined by the care
workers themselves. Those care workers who reported high job satisfaction referred to the
importance of the relationships they developed with users.This fits with evidence from other
studies ( see discussion in part I and TNS 2007). The importance of relationships to both
care workers and users thus reveals a complementarity between user and care worker
perspectives and between understandings of good quality jobs and good quality care.
347
VI. Research Findings and Conclusions
In this final part of the report we return to our original research questions (see section I.5) and
provide a summary of the findings. We conclude by using the insights gained from our nine
empirical research questions and the three stages of the research project to address our final
policy-related research question. That is, in the light of our findings, we consider the
prospects for the recruitment and retention of an expanded and higher quality social care
workforce in the future under current and emerging conditions and suggest where the key
policy challenges may lie if these workforce objectives are to be realised.
VI.1. The local authority commissioning environment
1. How do those in the local authorities responsible for commissioning and/or
contracting make sense of the multiple, changing and potentially
contradictory pressures on commissioning policy?
Our qualitative interviews with key actors responsible for commissioning and contracting in
the 14 selected local authorities (LAs) revealed the multiple and potentially conflicting
influences on commissioning practices. Social care commissioning takes place within the
wider local authority and is thereby influenced by the specific council‟s organisational and
political environment. At the same time it is shaped by the longer term policy agendas for the
development of social care. Approaches towards commissioning were found to be influenced
by competing agendas, including on the one hand the need to support providers and develop
the supply base and the imperative, on the other hand, to take costs out and control price, even
in a context of pressures to drive up the quality of care delivered. Further competing agendas
stemmed from whether commissioning would in the future continue to be dominated by LAs
or either undertaken jointly with the NHS or devolved to users.
While commissioning in all LAs was being pulled in competing directions, differences could
be identified between LAs in both the preferred strategic approaches taken by their
commissioners and in what they were actually doing to implement these approaches. In
particular there were marked differences in the emphasis placed on developing partnerships
with independent providers and in the emphasis placed on strategies to reduce costs. We
classified LAs on the basis of both actual fee levels paid and on their commissioners‟
espoused views and policies on partnership to distinguish between three types of LAs: those
that are partnership focused; those focused on cost minimisation; and those falling into a
mixed category. This classification was found to have some resonances with the national user
satisfaction scores as recorded by LAs, with the cost minimising LAs assessed by users as
providing less good quality care than the partnership or mixed categories. The cost
minimising category included LAs from different regions and labour market conditions,
348
indicating that their classification was a reflection of a particular policy stance by the LA
rather than a reflection of other local conditions. However, the partnership category included
mainly LAs that faced strong local labour market demand while the mixed category was also
more mixed in characteristics. Some of the mixed category LAs topped the user satisfaction
scores and in one case LA directly employed staff in a 3* rated unit provided a high share of
domiciliary care services, suggesting perhaps that it is share of services outsourced as well as
commissioning strategies towards the independent sector providers that may influence user
satisfaction scores.
While we have provided a categorisation of the commissioning and contracting strategies of
the LAs, a triangulation of the various sources of information on LA strategies and
approaches casts some doubts on the coherence, stability and long term sustainability of some
of these apparent differences in commissioning and contracting stances. Above all there was a
very high rate of change in commissioning policies, some of them implemented during the
course of our project. This rate of change reflected both the changing commissioning
environments and the recognition of potential contradictions between some of the LAs‟
objectives and their current commissioning approach. In some cases the problem was a
perception that their policy was not working (higher prices for rural domiciliary providers
were not being passed on to the workforce) or that their policy might lead to too high costs in
the future (where uprating of fees was guaranteed in the contract as an indicator of
partnership). In one LA the commissioners were planning to use new policy agendas such as
personalisation to push through changes that they had found difficult to legitimize in the past,
such as LA withdrawals from routine domiciliary care. Such double-edged policy initiatives
created problems in developing stable and coherent classifications of the approach taken by
the LA. Among the LA commissioners there was considerable awareness that following short
term and budget driven competitive tendering was undermining the scope for long term
strategic developments but cost pressures and rules on competition policy stood in the way of
a more strategic approach. Furthermore, working with the NHS was identified by some as a
means towards a more strategic approach but for others it had become a source of short term
inconsistencies: for example, where the NHS in the locality created obstacles to policies of
reducing admissions to residential homes or to developing quality rather than simply pricebased commissioning strategies. Past commissioning strategies were also hampering some
LAs in developing current policies and practices. This particularly applied to those LAs that
had effectively ended domiciliary care direct provision in the past. These LAs faced a large
cost legacy in the form of TUPE transferred staff to independent providers but also lacked an
inhouse facility to facilitate the development of re-ablement services and provide training
support to local providers.
Thus, although the LAs did adopt different commissioning strategies and approaches, these
did not necessarily provide sufficiently stable and coherent signals for independent providers
to have the confidence to use them as a basis to develop different approaches to managing the
social care workforce. Even when a policy decision had been taken to provide a higher
quality approach, there were concerns that this might leave them exposed to higher costs than
other LAs which could prove difficult under future funding regimes. That is, the LAs were
349
not sufficiently autonomous from central government policy to be able to develop coherent
and stable strategic approaches that would not be easily destabilised by changes in central
government policy, as well as by other local policy decisions.
2. What are the variations and trends in the specific characteristics of LA
commissioning and contracting practices, from price and contract to quality
monitoring and provider relations?
We found significant variation in the specific practices adopted by LAs with respect to
commissioning and contracting, particularly in the case of domiciliary care, but these
differences again were, as already suggested, subject to a high degree of change. The
variations between LAs and the changes within LAs can be best analysed by taking
commissioning of domiciliary care and care home placements separately.
In domiciliary care the majority of service hours had already been outsourced in all LAs and
there were further plans to outsource in six of the eleven where outsourcing was still below
90% of service hours. There were no plans to TUPE transfer LA staff and most LAs felt that
this would not be cost effective. Moreover, most were planning to keep some inhouse
provision and the high levels of outsourcing also coincided with a strong tendency towards
greater specialisation within the remaining LA provision with only four still undertaking
routine domiciliary care work. Nevertheless there were wide variations in the extent of
involvement of the independent sector in specialist work (see table II.1).
One of the major trends identified was a move away from block contracts towards a set of
preferred providers, in part as a cost efficiency measure to reduce risks of paying for unused
hours but also in preparation for the personalisation agenda. One LA described their new
preferred provider systems as a „new block‟ contract, that is involving similar commitments to
block but without minimum guaranteed hours. However, the trends were not uniform as five
still used block contracts and two had recently moved to such contracts. These new preferred
provider arrangements almost always included an increased use of national providers. The
LAs‟ commissioning staff often expressed some concerns about the effect of the increased
role for national providers but nevertheless still included more in their preferred provider list
and in only a few LAs were concerns expressed about the need to maintain local agencies on
the list particularly where they were associated with serving particular communities. All
divided up their preferred providers or block contractors by geographical area but some used a
number of providers per area while others used only one or a main and subsidiary providers.
Many LA commissioners were concerned about the impact of personalisation on the survival
of these arrangements which they saw as essential to reduce costs and keep travel time to a
minimum.
350
Pricing strategies did vary between LAs with six setting a fixed fee per hour before the tender
with all providers contracted at that rate while eight LAs fees varied by providers according to
their tender price. The trend appeared to be more towards a fixed fee and in practice the
variations between fees were limited even when they could vary in theory. Not only did the
average fee paid to IDPs (excluding those with TUPE transferred LA staff) only range from
£10.45 to £14.50 for 13 LAs but the range among providers within a locality rarely exceed £2
to £3. One LA was an exception on both counts with a range from £16 to £28. In addition to
a trend towards a fixed fee there was a general trend towards a simple flat rate fee for
whatever hours were worked (several had recently phased out higher fees for shorter visits
and very few paid anything extra for unsocial hours or bank holidays) and also with limited or
no differences by the needs of the user. Likewise fees were paid for service hours and not for
travel time, although some allowed for higher prices from IDPs operating in rural areas. This
simplification of the fee structure was driven by the interests of transaction costs at the LA
level and the implications for wages and for incentives towards taking on more complex or
more unsocial hours work for either the providers or the employed staff did not seem to be
actively considered. Likewise the move towards use of electronic monitoring was primarily
driven by the interest of reducing costs and ensuring clients received their full visits; the
impact on the staff employed appeared not to be a prime consideration. While most LAs
undertook some form of quality monitoring of IDPs, which also included some monitoring of
HR practices, only two provided quality incentives for IDPs to either improve the quality of
their care or the quality of their HR practices.
Commissioning practices with respect to care homes tended to be primarily on a spot contract
basis. Twelve of the 14 LAs still provided some residential home care inhouse and ten had
some block purchase contracts with independent sector homes but most placements were spot
contract with independent sector homes, usually according to the preferences of the user. LA
commissioners were clearly aware that they had less ability to influence the behaviour of care
home providers especially in those areas where a large share of clients were self funded.
Variations in fees for residential care were much wider than for domiciliary care between LAs
and reflected regional variations in housing costs, not just wage costs. However, the level of
fees set also reflected political priorities. In some LAs there was an explicit commissioning
strategy of setting a care home fee at a level where it would not be necessary for an LA
funded client to pay any top-up fees unless they had a special room of some kind. In other
LAs commissioners anticipated that most residents would be asked to pay top-up fees.
Perhaps because of the difficulty of influencing care homes, more LAs had introduced quality
enhancements for homes, with six currently offering quality premia and some others planning
to introduce them. As with domiciliary care, many LAs were actively engaged in monitoring
homes but fewer had developed their own quality frameworks for homes. However, where
they were in place they had potentially more impact because they were linked to a qualitybased fee framework.
351
The selected LAs also were, for the most part, engaged in actively supporting independent
sector providers through training partnerships. Nine had current partnerships with the
independent sector and others supported training through opening up LA training to the
independent sector. However, those that had outsourced all their domiciliary services were
less likely to be engaged in training and in some cases LAs discontinued training provision
when sources of central government money for training support dried up, thus providing
another example where changes in central government policy may lead to rapid changes in
LA policy. Although all LAs held forums with providers these were more common with IDPs
than with homes. Moreover there was evidence of variations in activity within the forums in
part linked to the tendency or otherwise for local providers to become organised and engaged
in dialogue with the LA commissioning and contracting staff.
352
VI.2. Explaining the variety of HR policies and HR outcomes of
providers
3. What is the current state of HR practices and outcomes in the sector?
The need to map the current state of HR practices and outcomes arises largely out of the
context of radical transformation in the organisation of social care services for the elderly,
characterised by a near complete shift from local authority provision to independent private
sector and voluntary sector provision. As a consequence, there are multiple forms of provider
organisations currently engaged in delivering elderly care, of varying size, diverse ownership
configurations (such as single establishments, local and national chains) and distinctive profit
and not for profit business strategies. Moreover, without a guiding national framework for
employment conditions and HR practices (as provided across much of the public sector
through national framework agreements), there is enormous potential for variety and diversity
in the quality of HR practices. To address the research questions about what factors influence
HR practices and outcomes, therefore, this project constructed an original dataset on the
characteristics, context, practices and outcomes of provider organisations – including
domiciliary care providers, care homes and local authority inhouse providers of domiciliary
care (referred to throughout this report as IDPs, homes and LADPs, respectively). An
important contribution of our dataset is its incorporation of quality measures of a raft of HR
practices and outcomes, encompassing recruitment, working time, pay and work organisation
among others.
The overall mapping of HR practices and HR outcomes presented in part III, and
complemented by the case-study findings in part V, yielded the key finding that the quality of
HR practices across the whole of the independent private sector is clustered at the poor end of
the spectrum of potential HR policies and that there remain notable problems in recruitment
and retention, despite much of the survey having been conducted after the start of the
recession. Some systematic differences were found between homes and IDPs but the major
differences in quality of HR practices were between the independent and the public sector,
although voluntary sector providers offered better conditions than the private sector. However
in our sample a high share of the volunaty providers were residential homes operating
predominately with private clients rather than LA funded clients. The evidence suggests that
there are significant problems of recruitment and retention in the independent sector.
Although most providers judged recruitment to be relatively easy in the recession period,
IDPs in particular faced difficulty meeting their needs with nearly 70% recording shortages
for weekend and unsocial hours work. Much of the recruitment is informal although more so
in homes than IDPs and LADPs ,and all tended to rely on recruiting workers with positive and
friendly attitudes, with only LADPs placing importance on previous skills related to care
work among job applicants. and IDPs were most likely to emphasise availability for early
mornings, evenings and weekend work. Staff turnover averaged 24% for homes and 31% for
IDPs. Homes were better at retaining new recruits but 22% of homes and 32% of IDPs had
353
lost more than half of their new recruits in the past year. Even excluding turnover among new
recruits, turnover rates were still 22% for IDPs and 18% for homes.
Responses to these problems by providers have been limited. Overall the independent sector
provided a poor set of employment conditions, whatever the characteristics of the provider.
Thus, the potential for variations in HR practices by type of provider were marginal within
our dataset, although these could still, as we see later, make an impact on recruitment and
retention outcomes. These poor conditions were particularly notable with respect to pay. Pay
levels in the independent sector were clustered within a band for the most part no more than
£1 above the then national minimum wage of £5.73 with limited opportunities for upgrading
even for those who acquire NVQ qualifications at level 2 or even 3. The practice of uprating
pay on a regular basis was not universal and in homes was more influenced by changes in the
statutory national minimum wage while in IDPs the main factor was change in LA fee levels
and profitability.
Not only did we find basic pay levels to be low in the independent sector particularly among
for profit organisations but we also found that other elements of the reward policy resulted in
very low total pay for the length and scheduling of hours spent at work or in work related
activities. Paying a premium for overtime was primarily confined to providers in the public
sector, with most LADPs upholding this convention but only a quarter of homes and IDPs.
Unsocial hours payments were either not made or were more a matter of pence than a
significant proportion of the hourly wage. This lack of compensation for unsocial hours was
particularly significant in a sector where almost all staff were involved in weekend work and
many in early and late hours and night work. A significant share of providers also passed the
upfront costs of entering work (such as CRB checks, uniforms and induction training) on to
new recruits. Overall homes pay lower rates than IDPs and the IDPs in turn pay far lower
rates than the LADPs. Moreover, there is no trade-off between pay and other benefits; LADPs
pay the highest rates of pay and also pay for unsocial hours, travel time and upfront costs of
entering work. The independent sector homes and IDPs pay low rates of pay and do not
conform to good practices in these other areas of reward.
Contractual arrangements were also found to be different between the public and the
independent sector with evidence of a very strong employer-led model of flexibility among
homes and especially among IDPs. The public sector LADPs had followed a standard
approach to employment relationships by providing guaranteed hours to care workers while
the bulk of IDPs offered zero hours contracts only. This seemed to provide IDP managers
with a useful tool of workforce control enabling them to draw on a readily available pool of
employees for the required schedule of hours but the result was that even staff who worked
regularly full-time hours or longer and had been regularly employed for several years were
given no employment or wage guarantees. In homes, care workers were more likely to be
offered guaranteed hours and were also more likely to work full-time than in IDPs. In both
homes and IDPs only a minority of providers claimed to be able to match hours with
employee preferences all of the time.
354
With respect to working time the key difference in schedules was between domiciliary and
homes rather than public versus independent sector. Working time schedules were very
fragmented in domiciliary care and managers adopted a wide range of different solutions,
involving either split shifts to allow for continuity of care or more consolidated shifts by
banding together morning and dinner times and teas and evening care periods. In care homes,
managers also struggled with care rotas that respected minimum staffing ratios, which seemed
to vary between homes. Weekend working was extremely widespread in the sector with
nearly three fifths of IDPs, seven in ten homes and nine in ten LADPs reporting that all their
staff were engaged in regular weekend working.
Opportunities to exercise discretion at work so as to improve the quality of care may be
considered an indicator of both job quality and the quality of user care. Managers‟ responses
indicate that there were more obstacles facing workers in IDPs than in homes. This is
confirmed by our index measure of work organisation which is significantly worse for IDPs
than homes (with LADPs in between). However, a similar share of both homes and IDPs
(around a fifth) believed workers did not have sufficient time to develop better relationships
with users.
Two final areas of HR practices investigated concerned opportunities for development (such
as through training and appraisals) and for performance management, including the
expression of individual or collective voice. Although all providers were strongly engaged in
training provision, including induction training and training to NVQ level 2, attainment of
NVQ qualifications was higher in homes than in IDPs. More than half of homes and LADPs
had more than 70% of care workers qualified to level 2 compared to only a third of IDPs.
Nine in ten homes had already met the now abolished national target of having at least half
the staff trained to level 2 compared to just two thirds of IDPs. The two key factors cited by
managers in explaining failure to reach the target were high staff turnover and training related
problems such as funding. Use of appraisals was frequent throughout the sector and most
providers favoured soft over hard methods to improve performance, but poor performance,
including absenteeism, had at times to be tolerated in four out of ten IDPs. While all LADPs
had union recognition agreements, only 8% of IDPs and 15% of homes recognised unions. All
providers held regular staff meetings, although IDPs were least likely to organise these on a
frequent basis.
4. What role do provider characteristics play in shaping HR practices and
outcomes?
In our investigation of the impact of provider characteristics, including size, ownership,
profit/not-for-profit status and CQC star rating, we deployed different descriptive and
statistical methods. The first half of part IV presented the results of what are essentially
multiple correlation tests that compare the differences in mean scores between our quality
indices of HR practices and provider characteristics. Because correlations based on simple
cross-tabulations may produce misleading results, we also applied multivariate regression
analysis and presented these results in the second half of part IV. Thus while the cross-
355
tabulations offer a valuable guide to possible associations between variables, in this final part
of the report we attribute greater weight to the evidence from the multivariate statistical
models in pulling together the various results. The short answer to this fourth research
question is that evidence for systematic differences by provider characteristics (other than
between homes, IDPs and LADPs described above) was patchy. Drawing on both our cross
tabulations of HR practices and our multivariate analyses we can summarise the effects as
follows.
Beginning with the size of provider (measured by numbers employed), we might expect larger
homes and larger IDPs to design and implement better HR practices, drawing upon their
better equipped HR teams, and to enjoy better HR outcomes. The findings, while mixed, do
not support this argument. Among homes, it is clear that the larger the size the worse the
quality index of pay levels (including minimum and normal rates of pay, premium payment
for unsocial hours and pay for training) and the worse the overall summary index of HR
practices. And among IDPs, larger organisations have a worse index of pay strategies, which
covers HR practices of providing opportunities for pay improvement, career development and
upfront costs of starting work. With regard to HR outcomes, larger homes and larger IDPs
have worse recruitment and retention outcomes (measured on the basis of managers‟ views)
and larger homes also experience a worse (quantitative) measure of staff turnover excluding
new recruits. These are the main findings supported by the regression results.
Other possible associations with organisational size are highlighted by the multiple
correlation tests (Anovas). These suggest, for example, that smaller homes may have been
more likely to offer better career opportunities, less likely to require regular weekend working
and enjoyed better training outcomes than medium and large homes. Only one result suggests
better practices among larger homes, namely, the greater use of appraisals. Among IDPs, the
results are mixed: for example, larger IDPs had higher shares of staff working long hours and
were less likely to pay for induction training, but on the other hand were more likely to offer
time off for training and less likely to require weekend working (contrary to the result for
homes).
A second important distinguishing characteristic among providers is the form of ownership.
We distinguished between national chain, local chain and single establishment. As with size,
one might anticipate those providers that are members of national chains to be able to invest
in better HR practices and enjoy better HR outcomes than local chain and, especially, single
establishment providers. Again, however, the evidence does not support such an argument.
Among homes the regression results suggest ownership type has no significant effect on HR
practices; local chain homes appear to exert a positive influence on the quality index of pay
levels but the effect is not statistically significant. HR outcomes among homes are influenced
by ownership type, but it is single establishment homes, not chains, that enjoyed better
performance, namely with respect to training outcomes and with respect to both quantitative
measures of staff turnover (with and without new recruits). Among IDPs, local chain
providers have a better index of pay strategies than national chain providers and this combines
with better HR outcomes in the form of recruitment and retention and training; unlike homes
there is no association with the quantitative measures of staff turnover.
356
Again, the multiple correlation tests are suggestive (although not fully substantiated) of other
possible associations. The results are mixed. For example, national chain homes were less
likely than single establishment homes to make unsocial hours payments and more likely than
local chain homes to have staff working long hours. On the other hand, national chain homes
were more likely than single homes to provide regular pay uprating and to pay the upfront
costs of starting work, and national chain and single homes were more likely to allow for
workers to exercise discretion than local chains. For IDPs, the correlation tests reveal very
few effects of ownership type: like homes, national chain IDPs were more likely to have staff
working long hours than local chains but on the other hand national and local chain IDPs were
more likely to carry out staff appraisals than single IDPs.
A third organisational characteristic we investigated is the star rating, from 1 to 3, assigned to
the provider by the Care Quality Commission. While the overall variation of practices and
outcomes was small, our analyses nevertheless attributed some broadly positive effects
associated with a provider‟s star rating. Because the star rating may be interpreted as a
performance outcome rather than an exogenous organisational characteristic (such as size of
ownership type) we did not use this variable in our regression results. We did, however,
explore its associations with HR practices and outcomes using the less sophisticated multiple
correlation tests. These reveal the following. Compared with homes rated 1* and 2*, 3*
homes paid significantly higher rates and were more likely to make unsocial hours payments.
However, 3* homes had worse employee voice practices than 1* and 2* homes. Among IDPs,
the net balance of effects was similarly positive with 3* IDPs more likely to pay for
qualifications than 2* IDPs and less likely to have all staff working regular weekends than 1*
IDPs, but less likely to pay for travel time and for paid breaks than 1* IDPs.
A fourth characteristic is the profit status of the provider organisation – either for profit or not
for profit. As might be expected, our regression results show quite clearly that not-for-profit
providers offered significantly better quality HR practices than for-profit providers (both
homes and IDPs) and not-for-profit homes also enjoyed lower levels of staff turnover than
for-profit homes. This result is quite striking. The for-profit status of IDPs also emerges as the
most statistically significant variable in shaping the summary index of HR practices and the
index of pay strategies, and in both cases the effect is negative. Among homes, the for-profit
status is strongly and negatively associated with the summary index of HR practices and the
index of pay levels. Among homes, for-profit status is also significantly and negatively
associated with turnover outcomes, with for-profit homes experiencing higher levels of staff
turnover than not-for-profit homes.
5. What is the impact of the external policy and commissioning environment
and the local labour market demand factors on HR practices?
To explain the patterns of recruitment and retention of the social care workforce and the
associated HR practices that we identified in the telephone survey of providers we
investigated the differential effects of the type of LA commissioning context on the quality of
HR practices in providers, distinguishing the level of fees paid for care services and the
357
partnership (or cost minimising) orientation of the LA. In addition, we explored the impact of
varying local labour market conditions, drawing out two dimensions – the median level of
female part-time pay in the local area and a composite index of labour demand, as described
in part I. The results paint a complex picture of inter-related effects, but certain overall
findings are clear:
LA fee levels have a positive, albeit weak, association with good HR practices,
especially pay practices and working time practices;
the partnership orientation of LAs has mixed effects on the quality of pay
practices for homes but significant positive effects on both pay practices and
the overall quality of HR practices for IDPs;
the level of local labour market demand positively influences the quality of pay
levels, pay strategies and HR practices, especially for homes;
In more detail, our results are as follows. With regard to the role of LA fee levels, three
findings deserve highlighting. First, the level of fees paid by an LA positively influenced the
quality of pay practices of providers. With regard to actual pay levels, the relationship was
positive but relatively weak: an additional £1 in fees translated into just 19p (IDPs) and 14p
(homes) extra for a care worker‟s hourly pay. The regression results only identified a
significant effect of LA fees on pay levels for homes, not for IDPs. This is an important result
since it both confirms to some extent managers‟ views that their ability to set pay was
constrained by the level of LA fees but it also clearly shows that there was only limited
willingness among the independent sector homes and IDPs to raise pay. Other pay practices
were also positively associated with high fee paying LAs, including the practice of paying a
premium for unsocial hours working among both homes and IDPs. A further important result
is that both homes and IDPs in high fee paying LAs (compared to those in medium and low
fee LAs) were more likely to reward care workers with additional pay for acquiring
qualifications. Relatedly, the results of multivariate tests show that the level of LA fees was
positively associated with our summary index of pay strategies for IDPs, which includes
practices of pay upgrade opportunities, payment of upfront costs of starting work and internal
career opportunities.
A second set of findings shows that LA fee levels also influenced the quality of working time
practices, although not in a consistently positive direction. For homes, weekend working was
less commonly required of all staff in high fee paying LAs compared to low fee paying LAs.
But long hours working in homes (hours per day and/or days per week) was in fact more
likely in high fee LAs than in medium and low fee areas. For IDPs, high and medium fee LAs
were positively associated with the practice of giving workers time off for training compared
to low fee paying LAs.
Thirdly, LA fee levels appear to have a counter-intuitive association with the quality of
practices that shape work organisation. Homes in low fee paying LAs score higher on
measures of discretion at work than homes in high fee paying LAs; the results specifically
refer to the index measure of work organisation that captures the likelihood that care workers
exercised acquired skills, had the freedom to organise tasks to improve care quality and
358
enjoyed opportunities to exchange ideas with other colleagues. It is not clear why such
opportunities would be more prevalent in homes paid low fees by the commissioning LA. For
IDPs the results point to a non-linear association with LA fees; the aggregate index measure
of work organisation is positively associated with both low fee and high fee paying LAs; the
same result applies to the sub-index measure of time discretion. However, the multivariate
regression results do not identify a significant role for LA fee levels in shaping work
organisation. Other factors aside from the LA commissioning context would appear to matter
in determining workers‟ opportunity to exercise discretion at work.
Our categorisation of LAs according to commissioning orientation suggests there is a broadly
positive association between partnership approaches and the quality of pay and HR practices
for IDPs (confirmed by the multivariate regression results) but for homes the statistical
evidence is rather mixed. For homes, the practices of paying a premium for unsocial hours
and providing opportunities for pay improvements were more likely in partnership LAs. Also,
statistical (anova) tests suggest that pay levels in homes were significantly higher in
partnership LAs than in mixed and cost minimising LAs. However, the regression results in
contrast identify a negative association (albeit not strongly statistically significant); it is
therefore difficult to draw a firm conclusion about the impact of partnership LAs on pay
levels in homes. For IDPs, our index measures of pay levels and pay strategies are both
highest in partnership LAs and the significance of this positive association is confirmed by
our regression results. A contrary finding for homes, however, suggests that cost minimising
LAs are more likely to be associated with the practice of paying for training than partnership
and mixed LAs.
In common with the relationship with level of fees, partnership LAs were associated with a
lower tendency for homes to require weekend working among care workers (compared to
mixed LAs). Yet, similar to the fee levels again, the association with long hours working in
homes was contrary to expectations with long hours and/or long days less likely in mixed
LAs. For IDPs, the partnership orientation had one significant association with working time
practices, namely that IDPs in cost minimising LAs were most likely to expect care workers
to tolerate changes in hours or location at short notice. A counter-intuitive result for homes
was that cost minimising LAs were associated with better quality employee development and
voice practices.
With regard to local labour market conditions our findings point to a strong tendency of
providers to respond to strong labour market conditions by improving their HR practices. The
implications for the current period are therefore that all providers may be less likely to
improve the quality of HR practices as labour markets have slackened. For homes, our index
measures of quality of pay levels, working time and the summary of HR practices were all
positively associated with strong demand areas. For IDPs, several results follow those for
homes, including positive associations with quality of pay levels, payment for unsocial hours
and a lesser requirement of staff to work weekends. As with LA commissioning practices, the
association with work organisation measures was counter-intuitive for both homes and IDPs.
The regressions results confirm the general direction of the statistical (anova) tests. In
particular, it is the level of female part-time pay in the locality that drives the quality of pay
359
strategies among IDPs (including opportunities for pay improvement and payment of upfront
staff costs) and for homes while the level of female part-time pay is strongly and positively
associated with the summary index of HR practices, it is the summary measure of local labour
demand that drives the quality of pay strategies.
6. The evidence presented in parts III and IV is complemented by the case-study findings
presented in part V. These case studies revealed variations among providers in the same
LA as well as across LAs. The LA commissioning environment appears to have more
influence on some aspects of HR practice more than others: for example pay and the
nature of contracts offered to care workers were related to being in a higher fee paying
LA, but the improvements were only marginal. In other aspects such as training and
working time, firm level policies are even more significant with limited effects from the
LA commissioning. Using case-study data to compare and contrast the practices put in
place by the same national providers located in different LAs shows that the policies of
national chains are playing a significant role in both shaping HR practices and in limiting
the actual impact of favourable commissioning practices on employment terms and
conditions. These findings suggest that the LA commissioning environment may be an
enabler of better practice but there are variations between providers in the extent to which
they respond to more favourable commissioning practices. Furthermore, although there is
variation in practices across providers this variation is around a very low level of basic
employment conditions and protections. However, national providers in keeping pay
levels relatively similar in LAs offering very different fee levels may either be securing a
high profit rate on their investments in high paying areas or may be using these profits to
offset losses in low fee paying areas; that is there may be cross subsidies between the
high and low fee paying LAs. What is the combined impact of HR practices,
environmental conditions and organisational characteristics on the quality of
recruitment and retention outcomes?
Using a combination of statistical techniques we interrogated the multiple internal and
external effects described above on four inter-related measures of recruitment and retention
outcomes that drew on both qualitative and quantitative measures from the telephone survey
dataset. Given the different challenges facing IDPs and homes, we consider the main headline
results for each separately.
We find that retention in IDPs,was more clearly related than in homes to interactions between
the key external influences of commissioning and contracting practices and labour demand
conditions with the internal HR practices of providers, as specified in our analytical
framework. Thus we find evidence of a strong positive association between the quality of pay
strategies pursued by IDPs with both the level of LA fees and the level of female part-time
pay in the local area. While the statistical analyses only demonstrate a significant association,
we believe it is highly likely that these external conditions acted as a trigger for better pay
strategies among IDPs. The regression results demonstrate that these same better pay
strategies not only have value for the care workers (more opportunities for pay uprating and
premium payments for weekend working), but also are effective in reducing staff turnover;
360
the result holds for the two quantitative measures of staff turnover (for all care workers and
for all excluding new recruits). These results hold even with the relatively low range of pay
levels provided by the independent sector providers in our study based on a rather low rate of
pay increases in response to higher LA fee levels, and even with the rather high levels of staff
turnover found for the independent sector providers. The implication is that with either more
favourable commissioning and contracting practices or more responsiveness of providers to
fee levels, further improvements in turnover rates could be anticipated.
Better practices in managing working time in IDPs are also positively associated with better
recruitment and retention outcomes, both with regard to our qualitative measure (drawing on
managers‟ perceptions) and with regard to our quantitative measure, at least with respect to
the practice of providing time off for training. Importantly, these positive associations, which
trace the linkages between external conditions, internal HR practices and recruitment and
retention outcomes, are contingent upon certain organisational characteristics. Larger IDPs,
holding all other factors constant, are more likely to experience worse recruitment and
retention outcomes (on two of the three measures) and local chain IDPs experience better
recruitment and retention outcomes than national chains according to our qualitative measure.
For homes, the findings point to a different set of possible causal relationships. There is a
direct association between lower staff turnover on the two quantitative measures of staff
turnover and more emphasis on the HR recruitment practice of recognising the value of skills,
qualifications and care experience in the selection of new recruits. We saw in part III that this
practice is not very common among homes (or IDPs, although it is among LADPs); while
most homes valued the desirability of skills and experience very few believed such attributes
were necessary to do the job. This result therefore illustrates the potential pay-off in terms of
reduced staff turnover for those managers who do attribute greater value to experiences of
informal and formal caring, acquired qualifications and past training among job applicants.
The practice in homes of not requiring care workers to regularly work weekends is also
associated with lower staff turnover (on one measure). This is an important result given the
statistical association between this particular HR practice and the LA commissioning
environment as noted above; namely, that homes in high fee paying, partnership LAs are less
likely to require regular weekend working. One measure of labour demand – the level of
female part-time pay in the locality – is negatively associated with the quantitative measure of
total staff turnover. Again, this is especially significant given the strong positive association
between this indicator of labour demand and the overall summary measure of the quality of
HR practices in homes. The particular organisational characteristics of homes also play a role.
The size of homes has the same association with recruitment and retention as we found for
IDPs – that is, larger homes have worse recruitment and retention outcomes - but the
contingency effect of ownership type is different with single establishment homes faring
better.
A fourth outcome measure reflects the effectiveness of providers in developing a skilled care
workforce, estimated by combining data on the share of workers with NVQ level 2 and
managers‟ ambitions to meet a 50% target. The results for IDPs and homes are similar in the
361
cross tabulations of training outcomes by the indicator of strong, medium, weak labour
demand that combines information on local pay and employment/unemployment rates for
women. In areas of strong labour demand both IDPs and homes have worse measures of
training outcomes. However, when in the regression analysis we separate out pay levels from
employment/ unemployment conditions we find it is strong local labour demand that reduces
training outcomes for IDPs but the level of female part-time pay that has this effect for
homes. This last result may be surprising given the association of high female part-time pay in
the area with reduce staff turnover and better overall HR practices although the impact on
staff turnover is only found of the overall measure for homes and for only for turnover
excluding new recruits for IDPs. One interpretation of this result is that higher job mobility in
strong labour demand areas, whether through poaching or staff quits in search of better job
opportunities, may make it difficult for managers to keep up with training new recruits.
362
VI.3. Recruitment and retention from a care worker and user
perspective
7. What factors shape the recruitment of care workers?
The case studies identified a number of factors that shape recruitment into the sector. Firstly,
the personal motivations and experiences of care workers reveal the „pull‟ factors into care
jobs. In particular, informal experiences of caring in the home for elderly relatives and/or
children had often led to a commitment and desire to care for others and do meaningful work
and these intrinsic features of the job are an important explanation as to why people enter the
sector. Other features of the job that are shaped by HR practices more directly, such as
training opportunities and convenient working time, were also found to be important
influences on decisions to enter the sector. Secondly, the recruitment process was
characterised by a high degree of informality which was also a trend indicated by the
telephone survey. The informality of the process led to an important role for social networks;
many care workers entered the sector by word-of-mouth recruitment. This informality was
found to provide advantages from both the employer and employee perspective.
From an employee perspective the informality of the recruitment process allowed them to
make use of social networks which not only provided information on job opportunities but
also provided encouragement to enter. This encouragement came not only through factual
information about the work but the care workers in their social networks were often clearly
passionate about their work.
From an employer perspective this form of recruitment was useful in selecting workers who
already had some knowledge of what care work entailed and were therefore less likely
perhaps to quit at an early stage due to misconceptions over the nature of the work. This may
account for employers‟ tendency at the recruitment stage to emphasise informal caring
experiences and attitudes, in contrast to formal skills and qualifications. Moreover, word of
mouth recruitment also provided a useful way of recruiting some younger workers, often
younger family members of existing care workers. These benefits were being increasingly
recognised by employers, including national providers, who were trying to capitalise on the
potential of informal word-of-mouth recruitment methods by using bonus voucher schemes to
encourage existing care workers to introduce friends and family into the sector.
8. What factors influence the retention of care workers?
Our case study research revealed that just over half of the care workers we interviewed
anticipated that they would still be working for their current employer in five years time and
88% intended to be still working in the sector. While we are unable to show whether this
long-term commitment will lead to high levels of retention in practice, what it did reveal is
the relatively high level of job satisfaction experienced by care workers. This satisfaction was
found across the cases studies located in different LAs and representing different types of
363
providers. Job satisfaction related to the rewarding nature of the job and the opportunity to
help and care for others. Also, for workers engaged in domiciliary work, job satisfaction also
related to the opportunities provided by the nature of the work for autonomy and discretion.
This high satisfaction with the job was found alongside revealed low satisfaction with key HR
practices, in particular pay practices. Two thirds of care workers reported that they felt their
pay was unreasonable for the work they did and the lack of travel pay and payment for
unsocial hours were key areas of dissatisfaction. A further concern was that the spread of
electronic monitoring might reduce total reward still further by restricting paid work time to
time actually spent in people‟s houses rather than at work. In contrast all those employed by
LAs expressed a high level of satisfaction with pay. Importantly their knowledge that the
independent sector often did not pay for travel and unsocial hours shaped their satisfaction
with their own pay and benefits.
The reported high job satisfaction and commitment to the work, despite dissatisfaction with
pay, could suggest that care workers become what England (2005) has described as „prisoners
of love‟; that is, they become trapped in low paid work due to their engagement with and
concern for their clients. Retention of care staff thus relies to a great extent on altruistic
motivations and the intrinsic rewards of the job. However, while we have presented strong
evidence of such motivations among current care staff, it is notable that most of these staff
had previously worked in low paid, low skilled jobs in sectors such as retail, hospitality,
administration, and factory work. These jobs were low paid and often described as
monotonous. Care workers contrasted the monotony of other jobs with their experiences of
care work which they found to be both more challenging and more rewarding. The limited
opportunities available to unqualified workers mean many will accept low pay in exchange
for interesting work because the opportunity to have both is not considered as an available
option. Thus these findings should be put into the context of care workers‟ educational
backgrounds, work histories and expectations about wages. The negative effects on employee
morale of low wages and other poor employment conditions may be greater if the recruitment
network for social care were to widen to groups with either more positive past experiences of
employment or with a currently wider range of alternative employment options or career
choices.
Certain bundles of HR practices proved to be important in understanding why care workers
seemed to accept low pay and intended to stay. Our case study findings show that satisfaction
with working time and training opportunities meant that some of the high levels of
satisfaction and commitment to the sector were indeed because of the HR practices in place.
The majority of the care workers we interviewed worked hours that matched their preferences
and there is no doubt that care workers valued this aspect of the job and that this is a key
factor in retention. Another way of showing this effect is that those care workers who were
not working the hours that matched their preferences were more likely to express an intention
to leave. However, those satisfied with their hours had often been able to negotiate specific
schedules that fitted their own particular needs and which were not necessarily even typical of
the organisation they worked for. These working time schedules would thus either not be
attractive to the majority of potential recruits, or alternatively represented specific
364
arrangements –for example not working weekends- that could not be generalised to all staff
due to the service demands on the organisation. Training opportunities provided another
example of an HR practice that could help with retention. Although many of the training
opportunities on offer in the sector were often a direct result of statutory regulation, they were
also valued by care workers as many had experienced few opportunities to gain qualifications
in the past. Even though the majority did not have aspirations to progress, opportunities for
training made them feel valued by their employer and care workers felt committed to their
employer because of this.
In general, we also found no evidence of the so-called „supermarket effect‟ where care
workers leave the sector for better paying, less demanding jobs in the retail sector. Rather, it
was the „pull‟ of the NHS and nurse training that were the reasons most often given for
intentions to leave. The better terms and conditions of employment in the NHS mean that
when care workers stated they intended to leave for a job in the NHS, pay is likely to be a
factor shaping this choice.
9. Is care workers‟ job commitment influenced by the nature of the job and does
it involve trade-offs between „bad‟ and „good‟ aspects of the job?
The overwhelming reason for high job satisfaction and commitment expressed by the
interviewed care workers related to the nature of the work and in particular the opportunities
to help people, work with the elderly and build relationships with service users. This
represents an example of complementarity between user-centred services and employeecentred work organisation. Research on older people‟s definition of quality care has shown
the importance that users attach to „process outcomes‟, such as feeling valued and respected,
being treated as an individual, and being cared for by staff that demonstrate a caring
motivation (Francis and Netten 2004, Glendinning et al. 2008). Our case study research has
revealed that the opportunity to focus on these aspects of the job is central to the high levels
of job satisfaction and commitment to care work reported by care workers. The ability to
develop good relationships with service users was a defining aspect of job quality as well as a
defining aspect of service quality. However, evidence about the nature of work organisation
and whether this facilitated good quality care and good quality jobs was at times
contradictory. Care workers‟ accounts reveal higher levels of discretion than reported to us by
management in the telephone survey. In some cases the LA commissioning environment
enabled this, as for example in the local authority RN where key performance indicators
relating to continuity of care were set. In other cases it could prohibit this, for example with
the use of electronic monitoring. However, in many cases it was simply the way care workers
managed the boundaries between commissioned tasks and user expectations that was key to
their high levels of job satisfaction and to good quality service. This was often despite the
formal system of work organisation in place rather than because of it.
365
The opportunity to develop relationships with users allowed room for discretion and in this
sense care work does not fit the standard classification of low paid, routine work. As
suggested above, some care workers appear to be making trade-offs between these „good‟
aspects of the job and the „bad‟ aspects of the job, in particular low pay. Yet it may be the
case that low pay is only accepted because other dimensions of HR practice are in place that
accommodate care workers‟ specific needs. For example, care workers in our case studies
were generally satisfied with their working hours and training opportunities. And while
prospects for promotion are usually identified as a „good‟ aspect of a job, the importance
attached to this feature depends on the aspirations of the workforce. Because many of the care
workers did not in fact have aspirations to progress, the limited career opportunities on offer
were not identified as a particularly „bad‟ aspect of the job for many of those interviewed.
However, this lack of aspiration was also shaped by the poor additional rewards for senior
status within social care coupled with a requirement to take more responsibility but reduce
involvement in hands on care. Whether this group is typical in the trade-offs it makes will be
discussed in the next section. It also needs to be recognised that care workers working for
different types of providers may be making different types of trade-offs. For care workers
working for LADPs, pay and benefits were a „good‟ aspect of the job but they faced less
flexibility in terms of hours as this group were less likely to work hours that matched their
personal preferences. For this group working time could be described as the „bad‟ aspect of
the job but was accepted because of the relatively good pay and benefits on offer, especially
when compared to those on offer in the independent sector.
366
VI.4. Prospects for recruitment and retention under expanding
demand: the policy issues
The final research question explored relates to the context in which this research was funded,
namely the expectation of increased demand for the social care workforce, in relation to both
quantity and quality. We draw on evidence from each stage of the research and from each of
the above eight questions to ask:
10. What are the prospects of meeting current and future increased demands for
a social care workforce under present conditions - that is, without major
changes in commissioning arrangements, the policies of provider
organisations and the conditions of employment?
The evidence across all stages of this research project suggests that while the current
arrangements are just about delivering the current level of commissioned services, the model
of delivery of social care for the elderly is in a fragile state. There is positive evidence that
providers are achieving adequate levels of recruitment, albeit supplemented by recruitment of
migrants and with clear shortages in some key areas. But providers of all types are
experiencing relatively high levels of staff turnover and significant problems in achieving and
retaining a trained workforce, particularly in domiciliary care. The sector is also very reliant
both on the easing of recruitment conditions in the recession, and on a workforce that for a
variety of reasons has accepted to work under poor employment conditions, primarily
because of the intrinsic rewards associated with the work.
The sustainability of even this quantity and level of service would be even more in doubt in
normal labour market demand conditions but there was little evidence, whatever the
conditions, that the sector was in position to realise aims in relation to expansion in quantity
of service, improvements in quality of service or the delivery of long term strategic change.
This last aim includes both movement towards a more holistic and integrated approach to the
delivery of social care for the elderly and towards a more user-centred service which does not
put in jeopardy the development and stability of an effective supply side of both providers and
social care workers.
It is also clear from all stages of the project, that while LA commissioning and contracting,
provider HR practices and the experiences of care workers all play a part in shaping the
current quality and level of delivery, the impact of each of these elements cannot be looked at
in isolation. Thus, LA commissioning sets the general set of conditions for both providers and
the workforce operating in the independent sector of social care and must bear considerable
responsibility, together with central government, for the current state of the sector and its
ability to deliver on the three aims of expansion, improved quality and strategic change.
Nevertheless, our research also demonstrates that, where LAs do take the initiative to develop
a more favourable commissioning environment for better social care delivery, the
367
opportunities offered to providers to enhance their HR practices and improve recruitment and
retention are not necessarily taken up.
Good LA commissioning practice is thus a necessary rather than a sufficient condition for
improvements in HR practices and in HR outcomes in the sector. There is also a need to
consider the strategies and policies of the providers themselves. Providers may not be keen,
unless pushed by commissioning or other regulatory practices, to improve employment
conditions for care staff. This reluctance may be reasonably based upon concerns over the
future, given the rapidly changing and uncertain policy, budgetary and labour market context.
However, they may also be regarded as too ready to take as much advantage as they can of
their committed workforce by, for example failing to offer guaranteed hours even to staff
working regular full-time or even longer hours, in part because the zero hours contracts makes
it easier for them to demand flexibility in the number and timing of hours from their staff.
Particularly significant here are the policies and strategies of the increasingly dominant
national chains whose perspectives extend beyond the immediate LA and may be relatively
unaffected by any specific initiatives in commissioning that are pursued only at a local level.
Finally, we also need to bring in the attitudes and experiences of both current and potential
care workers. Here again some potential contradictions in possible strategies for change
within social care may be identified. The factors that have led the current social care
workforce both to enter and to stay in social care, and to develop a relatively strong
commitment to care work, cannot necessarily be built upon to expand the pool of recruits to
social care or to develop a higher quality workforce, measured in conventional terms of
accredited skills and qualifications and formal career ladders. There appear to be two main
sources of supply into care work as presently organised; those who come into care work as a
result of social networks involved in care, or their own experience of informal care; and those
who have found social care to be an opportunity for more satisfying work compared to other
more routinised and less meaningful jobs to which they have access. Both groups also often
fall into the category of those who have had limited previous opportunities for training and
development.
A further factor in retention has been the recruitment of very local staff with specific needs
for particular hours schedules. Working time arrangements in domiciliary care are far from
employee friendly in any conventional sense; they involve variable hours at unsocial times
and also frequently unpaid breaks and split shifts. However, individual employees, and
primarily those located in the immediate area, may find either that these hours fit their
specific circumstances or that they are able to negotiate specific schedules within the range
available that suit their current needs. All these factors may tend to reinforce commitment of
the existing staff, but operate against the expansion of the pool of recruits as staff may have to
be brought in from wider geographical areas, and to be attracted from groups who have a
wider range of alternative jobs and training and development opportunities. If providers
model their recruitment and retention strategy on what currently makes for the most
committed care workers, they may not realise the need for a strategic change to recruitment,
work organisation, employment conditions and career opportunities if the available pool of
recruits to social care is to be expanded.
368
Although the factors that may inhibit recruitment and retention in social care are interlinked,
in order to clarify the policy implications of these findings we will consider these first under
three main and relatively separate headings – commissioning and contracting, HR practices of
providers and the organisation of work and careers - before returning to the need for a more
integrated approach. We focus here primarily on improvements that may be needed within the
current framework for commissioning social care. We address later the significance of our
findings for the move to personal budgets.
Commissioning and contracting practices
If the objective of commissioning is to set the conditions for expansion, quality enhancement
and/or driving long term strategic change then there is a need to address four main problems.
The first is that budgetary constraints appear to be the overwhelming influence on actual LA
commissioning practices. Even though many people in LAs involved in commissioning are
very aware of the need to foster and develop the supply side, they are often unable to put
these concerns into practice, or to do so only in marginal ways, through additional training
support or limited quality uplifts to otherwise very tight fee payments. A second and related
problem is that commissioning practice is variable across both space and time; LAs are
making different compromises between competing agendas and are thus sending out mixed
messages to key national actors such as national chains. However, within a particular LA the
policy and practices are also subject to rapid changes, such that the consistency of the
message even at the local level may not be strong.
Third, short term needs largely take priority over longer term strategic developments, not only
in relation to fostering the local supply structure but also in developing strategic partnerships
with other services such as health and housing or in developing new ways of commissioning
including outcome based commissioning where users have more input into the composition
and quality of services delivered. The priority to the short term reflects both of the first two
problems, that is the immediate imperative of the budget and the changing political balances
across competing agendas. Movements to outcome-based care may also run counter to budget
imperatives to introduce electronic monitoring to take costs out of the service However, the
focus on the short term is also an outcome of practical problems that LAs encounter when
they engage in more strategic developments. In working together with health on elderly care,
problems arise because of the potential dominance of health in the partnership or because of
the difficulties of working across two public bodes with different views, for example, on the
benefits of fair commissioning and with different budget constraints, different regional or
geographical boundaries and different processes of intra-organisational restructuring.
The fourth problem is that LAs are not paying sufficient attention to the employment
consequences of their commissioning practices. In many respects LAs hide behind the notion
of business to business contracting to evade the responsibility that they must share for
employment practices in the sector; as our evidence shows, employment practices are not only
poor, but in some areas may even be on the margin of legality. Nevertheless LAs consider the
issue of payment of travel time between clients to be an issue for the independent providers
369
even though they fail to include payments for travel time in their commissioning, except in
the margin above the national minimum wage in their fees for one hour of care. Likewise no
specific provision is made for training time and the decisions to simplify fee structures in the
interests of minimising transaction costs carry with them the implications that wages are
unlikely to be higher for work involving more skill and intensity of care or for work outside
of standard working hours - whether overtime or unsocial hours. LAs are increasing their
monitoring of providers‟ HR practices but are treating the meeting of quality thresholds more
as an additional requirement on providers and not as an indicator of what elements of their
own commissioning and contracting practices may need to change.
HR practices of providers
The evidence presented in the report suggests that by and large providers in social care do not
deliver even the basic guarantees to employees associated with an employment relationship,
rather than a casual employment contract. Thus within the domiciliary care sector, in
particular, staff cannot expect to be given any guarantees of hours or wages, they are not
necessarily paid for all the time they spend at work, receive at most limited compensation for
working unsocial, flexible and long hours and are unlikely to be rewarded more than a few
pence per hour for additional skills and experience. Even those taking positions of
responsibility can expect an uplift of no more than £1 an hour at most. Many of these
conditions appear to follow directly from LA commissioning practices, but even when LAs
offer more favourable commissioning and contracting most of the benefits are not passed to
employees. National providers are developing some company-wide policies but are
continuing to fix pay and other conditions at a local level. However, this approach seems to be
more about ensuring that a national scale does not price them out of work in some low paying
LAs than a means of upward adjustments of wages.
Some of our results suggest that it is only when local labour market conditions push turnover
rates above acceptable levels that providers may be dragged into providing what many would
regard as basic employment conditions and guarantees. One area where providers have
developed HR practices beyond the basics is in training, where most care workers felt they
were offered training beyond what they had experienced in other low paid jobs. One issue for
the future is whether the removal of the training target from CQC care standards will have an
adverse impact on future training provision. The other main area of good HR practice where
providers appear to do more than is required of them statutorily is in relation to efforts to fit
working time schedules to staff preferences. The extent of this accommodation may be
exaggerated as various comments by managers referred to accommodating within the
constraints of their very specific needs to deliver care in short chunks throughout the day and
evening or to provide 24/7 care as in the case of homes. Nevertheless, the efforts made to
accommodate their preferences were valued by the staff in the case studies and this suggests
that this is one way in which the local managers may aim to recruit and retain staff within the
limits of the overall poor employment conditions. It may be worth noting that managers‟
ability to juggle schedules to offer staff hours that fit their needs may be further constrained
under personal budgets as one of the benefits of personal budgets is held to be the opportunity
370
to users to have more choice and control over their care. How this may affect the working
time arrangements for care staff has not been widely debated.
Overall we found little evidence of a more strategic approach towards recruitment and
retention; reliance on word-of-mouth recruitment and offering flexibility to match individual
circumstances in working hours may be a means of securing a stable workforce under current
conditions but these approaches set limits to the extent to which providers can develop
ambitions to expand or upskill the workforce.
The overall policy conclusions must be that providers cannot be simply trusted to respond to
more favourable commissioning and contracting and to improve employment conditions or to
develop longer term strategic approaches without some specific incentives or constraints. This
suggests that improvements are likely to require regulatory development – just as, for
example, the improved level of the national minimum wage and the move to 28 days paid
holiday have probably done most to improve conditions in this sector in the 2000s. It also
suggests that improved employment conditions need to be built into LA commissioning and
contracting strategies, but these requirements need to be funded by the LAs rather than simply
added in as an additional requirement without the complications taken into account in the
commissioning and contracting price. Another issue that needs to be considered is the
possibility of developing longer term partnership approaches with local providers; currently
there is a lot of discussion of partnerships but these are contingent on future competitive
tenders. Current partners or preferred providers may be encouraged to improve quality and
invest in their workforce in line with an LA‟s quality framework but they have no guarantee
that at the next tender they will not be rejected on the basis of too high prices. Such risks may
be even greater for providers who may be encouraged to develop a more strategic approach to
the recruitment and development of the workforce by offering not only better employment
conditions but also perhaps more training and development opportunities and more extended
career ladders. Such strategic turns require a long lead in and a stable and favourable
commissioning environment, conditions that are unlikely to prevail under current
arrangements.
The organisation of work and careers
The case studies revealed the current reliance on a workforce with specific characteristics that is, a largely female workforce with low qualifications, social and family networks with
links to the sector, very locally based and with very specific working time preferences. This
group was also found to have high levels of job satisfaction linked to their unrewarding work
experiences in the past as well as the nature of their present job. While this group of women
are a reliable workforce, provider practices and employment conditions that can appeal
beyond this group need to be put in place. However, a number of obstacles currently prohibit
this.
371
Firstly, if the sector is to expand and appeal to under-represented groups, such as men or
indeed women with higher levels of qualifications, there are limits to how far the sector can
rely on localised recruitment practices that are predicated on informality. This will only
access a certain pool of female recruits, often those with no or low-level educational
attainment who are looking for work where low-level qualifications are not a barrier to entry.
Moreover, this pool of workers is contracting as the educational levels of women rise.
Secondly, it would appear that for too long the sector has relied on workers being „prisoners
of love‟, willing to accept low wages because of the intrinsic rewards of doing meaningful
work. While workers with few qualifications and limited opportunities may be willing to
accept such a trade-off, if the sector is to expand it may not be able to find new pools of
potential recruits willing to do so, quite apart from the social justice question as to whether
committed workers should be rewarded with lower pay. Furthermore, it is a trade-off that
cannot be made until people enter the sector in the first place and we do not know how many
people are deterred from entering because of the low pay levels on offer. This is exacerbated
by the better pay and opportunities on offer in inhouse local authority services and in the
NHS. The „pull‟ of the NHS and nurse training were the reasons most often given by care
workers for intentions to leave.
Thirdly, while workers were generally satisfied with their hours, the case study research
revealed the idiosyncratic nature of the hours worked by care workers. The hours were
unpredictable and variable, fragmented across the day, and did not fit standard notions of
family friendly flexible working. The hours suited care workers with very specific needs and
circumstances who often needed to work locally. This sort of working time would not
constitute flexible working to many and because legislation has ensured that more standard
notions of family friendly flexible time are now available in many organisations, the sector
cannot rely on its image as „flexible‟ as a way to expand the sector in the future.
Thus, to expand the quantity of recruits and provide a more diverse workforce that may also
have the capacity for further quality improvements there are clear needs to:
i)
go beyond the informality of recruitment and to recruit across wider segments
both geographically and by gender, age, ethnicity and qualifications;
ii)
to stop taking for granted that the nature of the work will compensate for poor
working conditions and provide terms and conditions that are at least
comparable to the main competitors such as the NHS;
iii)
provide for more stable and guaranteed hours at work, albeit still with
opportunities to tailor working hours to preferences and circumstances of the
staff.
However, at the same time there could be strategies that build on the positive aspects of the
work, as revealed by our case study research, in developing systems of work organisation on
the one hand and career structures on the other. Four elements in such a strategy can be
identified. First, and above all, there needs to be scope built into the organisation of care work
that enables and encourages staff to develop relationships with users. This is a key factor in
372
explaining high levels of satisfaction in the job and is key to both retention of staff and good
quality of care. The intrinsic features of the job, caring for the elderly and doing meaningful
work, bring high levels of job satisfaction and work organisation that supports this should be
part of providers‟ recruitment and retention strategy as well as part of their remit to provide
quality care. Any changes relating to work organisation need to be put in place with the
consultation of care workers and users as this is an area of HR practice where quality service
and quality jobs complement each other. At present this aspect of the work may be developed
more through the discretionary action of care workers than through it being an objective in the
design and organisation of work; if the high levels of satisfaction that we uncovered are to be
the basis for further development of the quantity and quality of the care workforce, we would
suggest that such activities need to be explicitly allowed for and rewarded in the job. The
commissioning environment and provider responses to this must build on the strengths of the
sector by offering interesting and rewarding jobs that are meaningful and allow time for care
workers and service users to develop relationships and be flexible in their approach to care.
This will improve both recruitment and retention and the quality service for users.
The second point follows from the first and that is that the use of electronic monitoring needs
to be carefully assessed and the benefits of improved data and reduced transaction costs and
direct care costs for LAs weighed against the possible loss of opportunities for delivery of
high quality care, with consequences for recruitment and retention as well as for the users of
care.
A third element that provides a positive base for further development is the generally positive
attitude of care workers to opportunities to training and to acquiring qualifications. This
proved particularly appealing to those who had, for example, been made redundant late in life
and wanted to start a new career and to younger workers who had not gained qualifications in
education. This may suggest that social care should develop an eclectic approach to
recruitment, providing opportunities for those who have missed out on earlier chances for
education and training while also raising the overall profile of social care as a career choice
by offering opportunities for training and development.
Finally social care needs to develop more opportunities to progress which do not take the
more senior and experienced care workers away from hands on care. This could involve
combining hands on care work with supervisory and mentoring roles or providing more
opportunities to move into re-ablement work at higher wage levels. Current specialisations of
LAs in the higher skilled work may be restricting those opportunities as LA departments may
not be recruiting as they reduce in size. As this problem eases through natural wastage it may
be important to encourage transfer from the more routine work into more specialised areas as
a means of retaining staff within the sector and providing them with both more rewards for
experience and new challenges. Opportunities to progress may prove to be particularly
important to recruit and retain men, on the basis of the small sample we interviewed.
However, this also means that it is even more necessary to create a range of career
opportunities as otherwise the relatively few men in the sector may be found occupying most
of the higher level positions if they are more active in bargaining for quick progression.
373
Summary of key policy recommendations.
The key policy recommendations to achieve better recruitment and retention outcomes
include the following.
Stronger partnership arrangements are needed with providers, either at LA level or
through a national system of care commissioning, involving increased obligations on
both sides. Longer term guarantees of contracts or of preferred provider status need to
offered to enable providers to make a step change in their employment practices ( but
these arrangements should be designed to foster and not reduce the diversity of
supply).
LAs or a national care commission should promote better and reasonable employment
conditions through both better resourcing and more stringent requirements on
providers to meet higher HR standards.
Attention also needs to be paid to maintaining or improving the intrinsic rewards from
the work, potentially calling into question the practice of fragmented commissioning
of care packages, backed up by electronic monitoring.
Likewise there needs to be a more partnership approach to developing working time
arrangements that meet both user and care worker needs, perhaps by moving away
from the fragmentation of care commissioning by task and narrow time periods.
These recommendations should together provide the environment in which providers
can start to extend their recruitment pool and begin to attract and retain staff beyond
the immediate vicinity and to provide both better employment conditions and more
opportunities for advancement within social care work.
Attention should also be paid to how to facilitate the development of high quality reablement and specialist services to ensure that users are not unnecessarily placed in
residential care. The delivery of specialised and short term care could require
consideration of a return to more guaranteed employment conditions and higher paid
employment, possibly within the public sector or under more stable and higher paying
contracts with specialist providers. The further development of specialist services
could also provide the important missing elements of opportunities for care workers to
progress without loss of involvement in hands on care.
Implications of our findings in the context of the move to personalisation
There are several ways in which our findings would support a move towards a more user
centred system of care as a means of recruiting and retaining a larger and more skilled social
care workforce. In particular, to the extent that this offered care workers more opportunities
for developing relationships with users and more opportunities to exercise discretion in the
ways in which they provided care, then this change in direction could promote the intrinsic
value of the work and enhance retention. However, these benefits may not necessarily be
achieved under current proposals for the mode of implementing personalisation. This applies
in particular if the proposals result in the user being the direct employer. In this latter scenario
even the above listed potential benefits of enhanced discretion and more opportunity to form
relationships would not necessarily be realised as the dual role of the user as the person
374
receiving the care and the employer of the care giver could inhibit the formation of a good
relationship. Care workers mentioned concerns about the lack of back up from managers in
their decisions on care provision, about their discomfort at the idea of being paid by the user
and about the potential problems of how they would be able to cope with a user who was
difficult or aggressive.
An important concern is how work would be scheduled and organised without the role of the
intermediary, the employer; this was a critical factor in care workers‟ job satisfaction.
Although opportunities to schedule care to meet their own needs is an important positive
attraction of personalisation for users, it is not clear how the difficult trade-offs between the
ideal time for a care visit and the competing demands from many users would be met. The
scheduling problem in principle could be eased by care workers caring for only one or a
smaller number of users but this would increase the need to expand the available workforce
and reduce the possibility of the job providing for full-time employment for those in need of a
full salary. Care workers we interviewed were concerned that caring for only one user might
prove less fulfilling compared to their current involvement with many users or might lead
them to be too involved, making it difficult to retain some distance from the user. They were
also concerned about job security if a user were to die or to move into residential care. The
ending of the job with the loss of a user could also enhance the risk of loss of skilled workers
to the sector as a whole; when workers are displaced from employment there is no guarantee
that they will confine their job search to the same field of work and having just been made
unemployed they might be unwilling to risk this happening a second time by entering into
another contract with an individual user.
Beyond these concerns over the move to directly employed personal assistants, our research
also pointed to a number of more institutional and budgetary concerns over personalisation as
currently proposed. Those most commonly raised by providers related to the poaching of their
staff and the increased difficulty in securing payment for services. For LAs the most common
concerns were over the impact on costs, the possibility that users would choose not to
purchase the more expensive re-ablement services, even though their long term costs of care
might then increase, and the problems user choice posed for organising care provision by
geographical area to minimise travel time and guarantee supply. The general uncertainty over
the future role of LAs and providers in the provision of services was also inhibiting more
strategic thinking and development, particularly with respect to integration with health.
Finally there was the problem of adding to the existing ambiguity over who had the
responsibility to provide training. Under personalisation three sets of agents might be
involved- the LA, the provider (if the PA were hired through an agency) and the user who
might be asked to pay for the training or the time spent training. In general it seems unlikely
in a sector where public funding inevitably shapes the market that strategic aims will be
achieved, or even the current quality and quantity of care maintained, without some continued
planning of provision at either LA or national level. If policies are not put in place to enable
strategic developments to be maintained and strengthened, the outcome could be moves away
from re-ablement and care in the users‟ homes and back to the more expensive and less
desired outcome of residential care.
375
There thus seems to be an urgent need for further consideration of the appropriate modes of
implementing greater user choice in social care. Greater clarity is needed in the future roles of
LAs and existing providers in acting as commissioners, brokers or intermediaries with the
users and detailed consideration needs to be given to appropriate forms of employment
relationships and employment organisation in a caring profession. More clearly needs to be
done to enable users to have more say over how and when their care is delivered but there is
little evidence that the full consequences for the employment relationship of a move towards
directly employed personal assistants or even personal budgets have been considered. A
comprehensive study of the experiences of personal assistants is urgently required, together
with more policy thinking on how care staff are to be provided with adequate training and
some form of employment security under the new budget holding arrangements.
Towards a rebalancing of the care debate
A key premise of this research has been that, in order for the quality of care to be maintained
and enhanced, it is vital to do more to recruit and retain skilled and committed care workers.
What has been missing in current debates over social care is any serious consideration of
employment. While there has rightly been an increased recognition that the voice of the care
user needs to be heard more, the voice of the care worker is still silent when one examines the
main policy debates and documents. The consequence is that the implications of social care
policies, whether towards competitive outsourcing or user-centred care delivery, for the
quality of employment relationships in social care are often ignored or hidden. This is a
surprising feature of public policy in this service area where the quality of care cannot be
divorced from the quality and commitment of the person delivering the care. Thus, whatever
direction social care policy moves in, we would argue for the need to give greater
consideration to the employment arrangements that could be reasonably expected to deliver
the committed and skilled workforce that the care users in turn deserve and need.
376
Appendix
I.A. Appendix part I
I.A1. Social Care Workforce Project -Telephone interview including common
questions and specific questions for domiciliary care providers and for care
homes
Because of the importance of recruitment and retention for care providers we are carrying out this
survey in an effort to find out what is happening in the sector what you think about the current
situation and how it could be improved.
1. General information
1.1
1.2
1.3
1.4
1.5
1.6
1.7
1.8
1.9
1.10
1.11
1.12
1.13
1.14
1.15
Agency name ………………………………………………
Interviewee Name ………………………………………………………
Position
………………………………………………
(If unable to find out in advance) Number of branches/offices ………
Which LAs does this branch hold contracts with?
What proportion of your service users are local authority funded?
Do you do any work for the NHS?
YES
NO
If yes What kind of work is this? (e.g. intermediate care)
CARE HOMES ONLY What percentage of your beds are currently vacant?
Who is responsible for HR issues on a day to day basis?
Do you have a specialist human resources manager or department
If yes, where located?
What support do they provide? (e.g. grievance and disciplinary)
Do you have a formal recognition agreement with any trade union?
YES
NO
If yes, which?
ADVANCE
1.A
How many staff do you employ?
a) This branch
b) Total (if applicable)
1.B
How many of the staff at this branch are care workers?
1.C
How many of your care staff are permanent ……..temporary……… external agency workers
……….?
1.D
What proportion of hours are done under a) block b) spot contracts?
1.E
Do you collect figures on staff absenteeism?
YES / NO
1.F
(If yes) How is this measured
What is the rate of absenteeism?
377
2. Recruitment and retention of care workers
Now we would like to ask you some questions about recruitment and retention of care workers.
ADVANCE
2.A
What proportion of your staff are
under 30
………………………………..
over 50 ………………………………..
over 60 ………………………………..
Female
………………………………..
White British ………………………………..
White other
………………………………..
Black or Asian ………………………………..
Over the past twelve months
How many new starters have you recruited?...............
How many are still with you?..........................................
How many other staff have left?......................................
What proportion of your staff have been with you over 2 years?..................
And over 5 years? …………………………………………...
NOTE If the agency/branch opened in the last 5 years please state date it opened and the
share of staff who have been with you since that date
2.B
Date……………………….
2.1
2.2
2.3
2.4
2.5
Share of staff ………………………….
Are you happy with the composition of your workforce?
YES
NO
If NO, would you prefer to have
Tick relevant box
more younger employees
more older employees
more men
more women
a more ethnically diverse profile
Which of the following applies to you?
Tick relevant box
a)We currently have the right number of staff
b) We currently have more staff than we need.
c) We currently have fewer staff than we need
If c), how many more staff would you be keen to take on?
How easy or difficult is it to recruit care staff?
Tick relevant box
1. Very difficult
2. Quite difficult
3. Neither difficult nor easy
4. Quite easy
5. Very easy
378
2.6
2.7
Has this changed since the summer of 2008?
If it is difficult to recruit, what are the main reasons? (No prompt).
Tick relevant boxes
Local competitors (e.g. new supermarkets)
Higher (or lower) wages elsewhere
Changing nature of care work
Working time schedules
Transport costs
High (low) local unemployment
Other – please specify
2.8
Are there any specific shortages (for night work, weekend work etc. or other specific
shortages)?
Tick relevant box
Night
Weekend
Other specific shortages
ADVANCE
2.C
What methods do you normally use to fill vacancies?
Tick relevant boxes
Use
Tick all that
apply
Most effective
Pick one only
Word-of-mouth recommendations from existing staff or others
List of interested applicants
Schools, colleges
Jobcentre Plus
Other agencies
Press advertising (local, regional or professional press)
Notice in office or shop window
Internal advertisement
Fee charging, private employment agency,
Any other way? (Please specify)
………………………………………………
2.D Which of the following do you normally use as part of the recruitment process?
Tick if
normally
used
Formal job descriptions and person specifications
Application form
CV
Initial telephone screening
References
Extra info
If yes Requires full
work history?
If yes Before or after
379
Formal interview
Informal interview
Aptitude testing
interview?
If yes With whom?
IF yes With whom?
IF yes –
At interview
At induction?
2.E
Which of the following factors do you consider a) necessary b) desirable c) most important when
recruiting care workers?
Necessary
Desirable Most
Tick relevant boxes
(Tick all
(Tick all
important
that apply) that
(tick one
apply)
only)
Availability for early starts or evening work
Availability for weekend work
Recommended by another employee
Skills related to care work
Experience of caring for family member or friend
Formal experience of care work (e.g.care home, other
home/agency)
Qualifications - NVQ2 or above in care
Positive attitude/ friendly nature
Ability to drive
Own transport
Lives locally
Other (please specify)
2.9
Is it easy for you to meet your recruitment criteria?
YES
NO
If no, what are the main reasons? (prompt using questions below):
Appropriate availability to match our service needs
Appropriate skills
Appropriate age range
Who already have appropriate experience/qualifications
Who are willing to gain appropriate qualifications
With appropriate attitude (friendly nature, motivated, positive attitude)
Who live locally.
2.10
What is the most frequent reason you find an applicant unsuitable for a care job?
……………………………………………………………………………………
2.11
Do you turn down staff who would, in your view, be acceptable care workers?
VERY OFTEN OFTEN
OCCASIONALLY
ALMOST NEVER
NEVER
2.12
Do you find that you are taking on staff who do not have as many of the desirable qualities as
you would like?
380
VERY OFTEN OFTEN OCCASIONALLY
ALMOST NEVER
NEVER
2.13
If unable to recruit staff locally do you
Tick relevant boxes
extend recruitment efforts to surrounding areas
attempt a more national recruitment drive
use other agencies
contact agencies/intermediaries who are seeking work for migrant workers
recruit abroad directly yourself?
2.14
Approximately how many migrant workers (defined as living in the UK for less than two
years) do you have working for you?
…………………………………………………………………………………………
2.15
What are the two most common nationalities?
…………………………………………………………………………………………
2.16
In the past two years approximately how many staff have you failed to recruit due to
a) delays with CRB checks
b) failure to pass CRB checks?
2.17
Do you consider staff turnover to be
VERY HIGH?
QUITE HIGH
ABOUT RIGHT/ACCEPTABLE
QUITE LOW
VERY LOW
2.18
What are the main reasons for staff care workers leaving? (No prompt)
Tick relevant boxes
Work for another care provider
Work for the NHS
Work for the Local Authority
Work in a different sector
More convenient working time
Better pay
Full-time education
Nurse training
Not suitable, dismissal
Family responsibilities
Other
2.19
Do you normally recruit senior care workers/team leaders/supervisors/managers from within
your existing staff or externally?
381
3. Pay
3.1
What is the range of hourly rates of pay for care staff (minimum/average/maximum)?
3.2
DOMCARE ONLY Are there different rates of pay for personal care and domestic work? (If
yes, what?)
3.3
DOMCARE ONLY (If applicable) Are there different rates of pay for those providing
intermediate care?
3.4
How do these rates compare with other domiciliary care providers in the area?
LOWER
ABOUT THE SAME
HIGHER
3.5
If there is more than one pay rate used, what are the main reasons for differences in pay rates
(give details of pay rates): (PROMPT FOR THOSE NOT MENTIONED - CAN I JUST CHECK
ARE THERE ANY DIFFERENCES IN PAY RELATED TO AGE, EXPERIENCE , ….
Age
Experience (including special probation rate)
Qualification
Weekend work
Night work
Length of Service/increments
Other (please specify)
3.6
Is there a regular upgrading of pay?
3.7
What are the main factors influencing pay upgrading? (PROMPT FOR THOSE NOT
MENTIONED)
Change in NMW
Performance Related
Completion of qualifications
Incremental salary scales
Commissioning price
Employee‟s request
Profitability
Other
3.8
DOMCARE ONLY How do you compensate for travel costs/travel time? (NO PROMPT)
Included in hourly rate
Supplement – flat rate
Supplement - percentage
Higher rate for call lasting under an hour
Mileage allowance
Reimbursement of petrol costs
Re-imbursement of public transport costs
Other
3.9
Do you provide uniforms?
YES
NO
3.10
(If yes) are staff required to pay for them?
3.11
Do you pay for CRB checks?
YES
NO
3.12
(If no) does that cause a significant drop out among those applying for vacancies (apart from
any other pay issues)?
3.13
CARE HOMES ONLY Do any service users make extra financial payments?
382
4. Organisation of Work
Work Scheduling
4.1
DOMCARE ONLY What are the hours of care provision?
4.2
DOMCARE ONLY How important is it to organise working hours to provide continuity of
care (1-5 scale)?
4.3
DOMCARE ONLY How important is it to organise working hours to fit employees‟
circumstances (scale 1-5)?
4.4
DOMCARE ONLY What kind of contracts do you offer for care staff?
Zero hours only – percentage of staff
Guaranteed hours - percentage of staff
4.5
In practice, what percentage of staff work:
under 16 hours
16-30 hours
over 30 hours
over 45 hours?
4.6
What is the maximum number of days a week that care staff work?
4.7
How many care staff occasionally/regularly work weekends?
4.8
DOMCARE ONLY Do care workers work alone or in pairs?
4.9
DOMCARE ONLY What is the minimum/average length of visit?
Are visit lengths tightly defined?
4.10
How is working time organised?
4.11
DOMCARE ONLY Is there a minimum length of a work period?
4.12
Do staff work:
continuous shifts
split shifts (morning shift and evening shift on same day)
Permanent early shift
Permanent late shift
4.13
DOMCARE ONLY Excluding travel time, what happens if there is a gap between service
users? Prompt: Unpaid break (only paid for contact hours)
Paid break
4.14
DOMCARE ONLY (If applicable) Are there different working time arrangements for care
workers providing intermediate care?
4.15
CARE HOMES ONLY Do all staff work some weekends? Or are there weekend/weekday
only schedules?
4.16
If there is a need for additional hours do you:
Ask existing staff to work extra hours
Use external agencies
Subcontract to other care providers?
4.17
DOMCARE ONLY How easy is it to find staff willing to work additional hours?
What about at short notice (2-3 days notice) or very short notice (the same day)?
4.18
Are care workers ever paid overtime premia?
YES
NO
4.19
If yes, does this apply to all staff or only those contracted to work a certain number of hours
per week. If so, how many hours?
383
4.20
Are your care staff able to get work schedules that match their preferences for particular
hours?
Tick relevant box
All of the time (1)
Most of the time (2)
Some of the time (3)
Occasionally (4)
Rarely (5).
4.21
CARE HOMES ONLY Do you have minimum staffing levels
YES
NO
4.22
CARE HOMES ONLY If yes, what are they?
Communication
4.23
Do you hold staff meetings?
YES
NO
4.24
{If yes) How frequently?
4.25
Do you carry out attitude/ staff satisfaction surveys? (If yes) Can we have a copy?
Performance
4.26
How is performance (of staff) monitored?
4.27
User surveys by care provider
User surveys by LA
Visits by supervisors
Observation
Electronic monitoring
Other (please specify)
What are the most common problems of poor performance that you encounter?
Absenteeism
Timekeeping
Skimping on time or services provided to
service users
Complaints from service users (over
attitude, competence, completion of tasks
etc.
Other (please specify)
4.28
What has been the most effective way you have found of dealing with problems of poor
performance?
Disciplinary action
Loss of wages
Training
Electronic monitoring
Other (specify)
384
4.29
Do you carry out staff appraisals?
YES
NO
4.30
(If yes) How often? Who carries these out?
4.31
Do recruitment difficulties mean that you are sometimes forced to put up with some problems
of poor performance?
4.32
Do your staff have opportunities to improve their performance in any of the following ways:
Yes
To some
No
Don‟t know
Tick relevant boxes
extent
Having enough time to carry out the work
to a high standard
Having the opportunity to put into practice
the training/qualifications they have gained
Being free to prioritise and carry out tasks
in ways that they feel will improve the
quality of care?
Having the opportunity to spend time
talking to service users
Being encouraged to exchange ideas with
other carers of new ways of working/best
practice
4.33
Would you expect workers to tolerate any of the following as part of their job (tick all that
apply)?
Regularly
Occasionally
Never
Working longer than scheduled due to
unanticipated needs of service users
Variations in hours or location at short notice
Working in very unsanitary conditions
Working with aggressive service users (due to
dementia etc.)
Working alone late at night (after 10 pm)
4.34
Do you consider rates of staff absenteeism to be:
VERY HIGH
QUITE HIGH ACCEPTABLE
QUITE LOW VERY LOW
5. Training and Development
5.1
Describe the induction training offered to new recruits:
How long is induction?
Is it offered by yourselves, LA, other external body?
Who pays for the induction?
Are staff paid for attending induction training?
5.2
For new staff who already have experience of care work, approximately how long does it
normally take before they are able to do their job as well as employees already working here? :
1) One week or less,
2) More than one week, up to one month,
3) More than one month, up to six months,
4) More than six months, up to one year,
5) More than one year
385
5.3
How do you identify training needs? (prompt if necessary)
Appraisal
Employee request
ADVANCE
5.A
What training courses are offered to staff?
Compulsory
Optional
Health and Safety
Food hygiene
Service user handling
Use of equipment
Infection control
First aid
Medication management
Dementia care
Diabetes care
Loss and depression in elders
Parkinson‟s care
NVQ 2
Others (please specify)
5.4
Refer to grid on advance information sheet - Who organises the training? (e.g. employer, LA,
other external body).
Where the LA organises the training:
Where other….
Who delivers the training?
Who delivers the training?
Is training devised specifically for providers?
Is training devised specifically for providers?
Is it provided free of charge?
Is it provided free of charge?
If it is not free, who pays the course fee?
If it is not free, who pays the course fee?
5.5
Are staff paid for time spent training?
5.6
Do they get time off from care duties to attend or do they attend outside their normal working
hours?
5.7
Does this apply to all courses? (Prompt – optional courses).
5.8
Does the local authority provide help with access to funding for training?
5.9
How many care staff have the following formal qualifications?
NVQ2
NVQ3/4
nursing qualifications
other relevant qualifications?
(Check – if any staff have NVQ3/4 or nursing qualifications are they employed as care
workers or in more professional/management jobs?
5.10
DOMCARE ONLY If agency provides intermediate care (Q1.6) Do staff providing
intermediate care need extra qualifications?
5.11
If yes, what qualifications?
5.12
How likely are you to meet the 50% NVQ2 target?
Already met/ will meet soon/ experiencing difficulties. (Check with CSCI)
386
5.13
5.14
5.15
If not yet met, what factors make it difficult to meet this target: NO prompt.
staff turnover
staff motivation
pressure of work (e.g. scheduling, fatigue)
other
Do any staff need to have NVQ3?
YES
NO
(If yes) Are they recruited externally or internally trained?
6. Relationship with NAMED LA
(Prompt – remind interviewee that their answers will be
treated confidentially)
6.1
How would you describe your relationship with NAMED LA (1-5 scale)
6.2
What is the main problem, if any, you have you experienced in your dealings with the LA?
Obtain from the LA interview/questionnaire whether LA organises a providers’ forum and how
often it meets.
If it does:
6.3
How frequently do you attend? (always, mostly, occasionally, never).
6.4
How useful is the forum on a five point scale? (1-5)
6.5
How much importance does the NAMED LA place on providers‟ HR practices in the
tendering process?
6.6
What monitoring if any does the LA undertake itself or does it rely on CSCI?
7. Policy and regulatory environment
7.1
How satisfied are you with the CSCI‟s a) set of quality standards b) system of quality ranking?
(1-5 scale)
7.2
Star rating:
Do you consider your own ranking to be fair?
ADVANCE –DOM ONLY
7.A
Which of the following quality care standards do you find most challenging? (Tick up to 4)
Care needs individually assessed
Service users treated with respect, valued and right to privacy upheld
Policies and procedures on medication and health related activities protect service
users
Health, safety and welfare of service users is promoted and protected
The risk of accidents and harm happening to service users and staff is minimised
Service users are protected from abuse, neglect and self harm
The well-being, health and security of service users is protected by the agency‟s
policies and procedures on the recruitment and selection of staff
Service users know that staff are appropriately trained to meet their personal care
needs
Service users know and benefit from having staff who are supervised and whose
performance is appraised regularly
Service users receive a consistent, well-managed and planned service
Service users, relatives and representatives are confident that their complaints will be
listened to, taken seriously and acted upon
387
ADVANCE: CARE HOMES ONLY
7.A
Which of the following quality care standards do you find most challenging? (Tick up to 4)
No service user moves into the home without having his/her needs assessed and
assured that these will be met
Service users assessed and referred solely for intermediate care are helped to
maximise their independence and return home
Service users‟ health, personal and social care needs are set out in an individual
plan of care
Service users‟ health care needs are fully met
Service users, where appropriate, are responsible for their own medication and
protected by the home‟s policies and procedures for dealing with medicines
Service users feel they are treated with respect and their right to privacy upheld
Service users find the lifestyle experienced in the home matches their
expectations and preferences and satisfies their social, cultural, religious and
recreational interests and needs
Service users maintain contact with family/friends/representatives and the local
community as they wish
Service users are helped to exercise choice and control over their lives
Service users receive a wholesome, appealing balanced diet and pleasing
surroundings at times convenient to them
Service users and their relatives and friends are confident that their complaints
will be listened to, taken seriously and acted upon
Service users are protected from abuse
Service users live in a safe, well maintained environment
The home is clean, pleasant and hygienic
Service users‟ needs are met by the numbers and skill mix of staff
Service users are in safe hands at all times
Service users are supported and protected by the home‟s recruitment policy and
practices
Staff are trained and competent to do their jobs
Service users live in a home run and managed by a person who is fit to be in
charge, of good character and able to discharge his or her responsibilities fully
The home is run in the best interests of service users
Service users‟ financial interests are safeguarded
The health, safety and welfare of service users and staff are promoted and
protected
7.3
What change, if any, would you most like to see in the inspection/regulatory system?
7.4
What, if any changes in the LA‟s commissioning/contracting arrangements would do most to
assist you in recruiting and retaining a stable and motivated social care workforce? Prompts:
388
Improvements in commissioning price
Variations in price by type of service and time of delivery
Higher guaranteed volume of work
More scope to determine how care is delivered (e.g.
commissioning in hours not minutes)
More integrated approach by LA to care provision
More time per service user
Other?
7.5
What changes to HR policies/practices would do most to improve recruitment and retention,
and have you implemented any of these changes in your organisation in order to improve recruitment
and retention?
HR policies that
Have implemented
Tick relevant boxes (prompt)
would do most to
improve R and R
Improved opportunities for training
Pay increases
Recognition of variations in service time of day/weekends/ type of care
/skill etc
Improved opportunities for internal
promotion
Flexible hours/hours to suit
Improved Non-pay benefits
More scope for care workers to
exercise discretion over how to
provide care
Any other?
7.6
DOMCARE ONLY What problems/opportunities do you anticipate as a result of an increase
in direct payments and individual budgets?
7.7
Do you have any concerns that proposed new regulations limiting non EU migrants will affect
your ability to recruit sufficient or sufficiently skilled care staff?
8.
Further information
(If interviewee unable to answer any of the questions) Could we get back to you for the answer to this
question?
We will be selecting a small number of providers interviewed for more in-depth case study research.
This will involve researchers visiting the organisation to interview a sample of care workers. If you
are chosen would you be willing to take part in this? Would it be possible for some of your staff to
attend a focus group to discuss issues for the case studies?
389
Appendix Table I.A1. Classifying female demand conditions in the selected LAs
Female
employment rate
in relation to
average for
Great Britain
69.4a
a
Female
unemployment rate
in relation to Great
Britain average
female
unemployment rate
of 6.1b
Share of women
who are inactive
but wanting a
job compared to
Great Britain
average of 6.6c
Classification
of female
employment
conditions
based on
columns 1-3d
Female parttime hourly
earnings
relative to
Great Britain
average f
AH
M
L
M
5
M
ON
L
M
M
3
L
RT
L
M
M
3
M
RN
H
M
M
5
H
UY
M
M
L
4
L
AD
M
H
M
3
L
AW
L
H
L
3
H
IL
L
H
H
2
L
OM
L
H
M
2
L
XD
H
L
M
6
H
HD
M
M
L
5
M
TE
L
H
H
2
L
LK
H
L
L
6
M
RD
M
M
M
4
M
H=2.2 to 7.9 %points above GB average, M=0.6 to 1.3 % points below GB average L= 3.4 to 10.3 % points
below GB average 2008
b
H=1.4 to 3.2 %points above GB average, M=0.7 below to 0.9 %points above GB average L= 1.6 to 7.9 %
points below GB average 2008
c
H=2.6 %points above GB average, M=0.3 below to 1 %point above GB average L= 1.2 to 3.4 % points below
GB average 2008
d
Scores computed as 3,2,1 H, M, L column 1 plus average of scores on columns 2 and 3 where 1,2,3 correspond
to H,M,L.
f
H=£1.13 to £2.97 above GB average, M=-1p below to 43p above GB average L= -78p below to £-1.91 below
GB average (2009)
Source: LFS on NOMIS for 2008, Ashe table 2009 8.6a for part-time earnings
390
Figure I.A1. Strong, medium and weak labour demand conditions
Female employment
conditions – low to high
High pay
Medium pay
2
3
IL, OM, TE
AW
4
Note:
RT
ON, AD
RD
UY
5
RN
AH,HD
6
XD
LK
Weak demand: white
Medium demand: light grey
Strong demand: dark grey
Low pay
391
IV.A. Appendix part IV
IV.A1. Technical notes explaining the standardised dataset - Indicators, subindices and indices
The analysis in part IV of the report draws on a standardised dataset that we constructed from
the telephone survey general data set. Four principles guided the construction of the
standardised dataset, as follows.
i)
Selection of providers: inclusion of providers on the basis of no less than 10% missing
values from the list of standardised indicators
-
resulted in the selection of 102 out of 105 providers from the full sample
of independent sector providers.
ii)
Selection of indicators: inclusion of indicators for use with the standardised data set on
the basis of a) their potential for explaining variations in HR practices and outcomes
and b) having less than 10% missing values (after elimination of providers with more
than 10% missing as in i) above)
iii)
Construction of sub-indices: designed in order to group together indicators that
measure similar dimensions to HR practices
iv)
Construction of indices: designed to provide overall summary measures of HR
practices in a particular HR domain.
The following tables provide details of the various indicators, sub-indices and indices, along
with a note referencing the table or figure in the report that provides descriptive statistics.
392
Appendix Table IV.A1. HR practice indicators, sub-indices and Xindices: standardised data set.
HR practice
indicators
Description and range of scores
For data
distributions see
tables in part III
Sub-indices (unweighted
average of the component
indicators)
X indices (unweighted
average of the
component sub-indices)
IP1
Pay level (minimum)
Very low = 0; Low = 0.25; Medium = 0.50; High = 0.75;
Pay
(normal)
Verylevel
high=
1
Very low = 0; Low = 0.25; Medium= 0.50;High = 0.75;Very high =
1Regular uprating of pay
Table III.14 and Fig.
III.11
Table III.15, Table
III.41and Fig. III.12
SIPAYLEVEL
INDEX OF PAY
LEVELS
Table III.19
SIPAYUPGRADE
XPAYLEVELS
Table III.16
Fig.III.16
SIPAYUNSOCIAL
IP2
IP3
No, or not regular = 0; Yes = 1
IP8
IP9
IP10
Extra pay for weekend work
No=
Yes=
Extra0;pay
for1 night work
No = 0; Yes = 1
overtime premia for extra hours
No = 0; Yes = 1
IP14
Payment of staff for time spent training
No = 0; Some courses=0.5; all = 1
Table III.20
SIPAYTRAIN
IP13
Payment of staff for attending induction training
No =0; Partly/ Reimbursed after specified time in post = 0.5; Yes = 1
Pay for CRB checks
No (+staff pay but reimbursed if stay) = 0; 50/50 = 0.5; Yes (+but
staff
reimburse
if leave
time)
= 1uniforms) = 1
Pay for
uniforms
Yes =within
0; Nospecified
(or only for
extra
Table III.22
SIPAYTR
AIN
Table III.21
SIPAYUPFRONT
Table III.21
Table III.14 and
III.15
SIPAYIMP
IP11
IP12
IP4
IP5
Pay upgrade opportunities
(normal pay minus minimum pay) zero= 0; 1p-20p = 0.25; 21p-40p
Differences
in pay
rates£1byorreason
= 0.50; 41p-99p
= 0.75;
over =1of experience or incremental
scales?
No = 0; Yes = 1
SIPAYUPFRONT
INDEX OF PAY
STRATEGIES
XPAYSTRAT
Table III.16
392
393
IP6
IP15
IHR1
IHR2
IHR3
Differences in pay rates by reason of qualification?
No
= 0; Yes = 1to become senior care workers
Opportunities
No seniors = 0; Externally only = 0.33; Both internally and
externally = 0.67;
Internally only
=1
Recognition
agreement
with trade unions (Q109)
No = 0; Yes = 1
Frequency of staff meetings
Less frequently than once a year = 0; Between once every three
months and once a year = 0.33; Between once every month and
every
three months =satisfaction
0.67; Everysurveys
month or more frequently = 1
Staff attitude/staff
Table III.16
Table III.5
SIPAYOPPCAR
Fig III.35
SIEMPVOICE
EMPLOYEE
DEVELOPMENT
INDEX
Table III.46
XEMPDEV
Fig.III.35
No = 0; Yes = 1
IHR4
IHR5
Frequently of appraisals?
No appraisal =0; Less frequently than annual= 0.2; once a year =0.4;
every six months to once a year =0.6; every 3 to 6 months= 0.8;
More
frequentlyofthan
3 months=1
Identification
training
needs
Table III.41
SIEMPAPP
Table III.41
No system = 0; Employee request = 0.5; appraisal alone or appraisal
plus employee request = 1
IRC1
IRC3
IRT5
IWT3
IWT4
IWT5
Formality of recruitment
Word of mouth recommendations=0; Other agencies/ internet/ open
days/any other way or notice in shop window=0.5;
Press
advertising
or job
centre qualifications
plus=1
Importance
placed
on skills,
or experience in
recruitment: score of 0=0; a score of 1-4=0.5; a score of 5-8=1
Role of push factors in staff quits
one or more push factors=0; no push factors=1
Work schedules that fit staff preferences for particular hours?
Occasionally/some of the time = 0; Most of the time =0.5; All of the
time = 1
Percentage of staff regularly working weekends?
100 percent = 0; Less than 100 percent = 1
Availability for weekend work as recruitment requirement
Table III.4
SIRECRUITPR
Table III.7 and fig.
III.5
Table III.15
SIRECRSELEC
INDEX OF
RECRUITMENT AND
RETENTION
PRACTICES
SIRECRETEN
XRRPRACT
Fig. III.21
SIWTSTFFPREF
Fig. III.20
SIWTWEND
Fig.III.4
WORKING TIME
INDEX
XWT
393
394
Yes = 0; No = 1
IWT6
IWT8
IWT9
IWO1
IWO2
IWO3
IWO4
IWO5
Maximum number of days that care staff work
7 = 0; 6 = 0.5; 5 or less = 1
Share of staff working over 45 hours
Over 6 percent = 0; 1-5 percent = 0.5; Less than 1 percent = 1
Table III.24
SIWTLHOURS
Time off from care duties to attend training?
No = 0 Sometimes = 0.5 Yes = 1
Time to carry out the work to a high standard
No = 0 To some extent = 0.5; Yes = 1
Opportunities to develop good relationships with service users
No = 0; To some extent = 0.5 Yes = 1
Opportunity to put into practice their training/ qualifications
No = 0; To some extent = 0.5;Yes = 1
Freedom to prioritise and carry out tasks in ways to improve the
quality of care
Encouragement
exchange
No = 0; To some to
extent
= 0.5; ideas
Yes = with
1 other carers of new ways
of working/best practice
No = 0; To some extent = 0.5
Yes = 1
Table III.20
SIWTTOFFTRAIN
Table III.45
SIWOTIME
Table III.23, and fig.
III.19 and fig. III.27
Table III.45
Table III.45
WORK
ORGANIZATION
INDEX XWO
SIWODISCRET
Table III.45
Table III.45
Note: index of all HR practices is called-XHRPRACT and is the result of the average of XPAYLEVELS, XPAYSTRAT, XEMPDEV, XRRPRACT, XWT, and XWO
394
395
Appendix Table IV.A2. HR outcome indicators, sub-indices and Xindices: standardised data set
HR outcome indicators
Description and range of scores
For data
distributions see
tables in part III
Sub-indices
SITRAINSKILDEV
(unweighted average of
the component
indicators)
IOUT1
Percentage with NVQ2 (Q194)
<46 %= 0 46–55 %= 0.33 56-69% = 0.67
>69%= 1
Table III.36 and
fig.III.28
IOUT2
Likelihood of meeting the 50 percent NVQ2 target
Experiencing difficulties = 0
Will meet soon = 0.5 Already met = 1
Fig. III.29
IRC5
Difficulty in recruiting care workers
very difficult=0 quite difficult =0.25
neutral=0.5 quite easy=0.75 very easy=1
Fig. III.1
IRC7
Staff shortages in particular areas Yes=0
No=1
Staff turnover considered to be: very high=0 quite
high=0.25 about right=0.5
quite low=0.75 very low=1
Table III.3
Fig. III.7
SITO
Absenteeism among care staff considered to be:
very high=0 quite high=0.25 acceptable =0.5 quite
low=0.75 very low=1
Fig. III.34
SIABSENT
IRT1
IRT6
X indices (unweighted
average of the
component sub-indices)
TRAINING/SKILL
DEVELOPMENT
OUTCOME INDEX
XTRAINSKILDEV
SIRECDIFF
INDEX OF R&R
OUTCOMES
XRROUTCOMES
395
396
Appendix Table IV.A3. HR practice indicators: non standardised data set.
HR practice Indicators
(excluded from
standardised data
set due to too high
missing variables)
Description and range of scores
For data
distributions see
tables in part III
IP7
Pay levels compared to other agencies/homes
Lower = 0; About the same = 0.5; Higher = 1
Most effective method of dealing with poor performance?
Disciplinary only = 0; „Soft‟ measures plus disciplinary = 0.5;
Training and „soft‟ measures only =1;
Not addressed
IOUT3
Do you have the Investors in People Award?
No = 0 Yes = 1
Fig. III.31
HR practice
indicators specific
to domiciliary care
Description and range of scores
For data
distributions see
tables in part III
IPDOM1
Compensate for travel costs/travel time
No extra pay = 0; Mileage or reimbursement = 0.5;
Supplement or higher rate for short call = 1
Fig. III.15
IHRDOM1
Performance monitored by electronic monitoring
Yes = 0; No = 1
Domiciliary care workers expected to tolerate variation in
hours or location at short notice
Yes = 0; Occasionally = 0.5; Never = 1
Fig. III.32
Paid break between service users
No = 0; Yes = 1
Minimum length of a work period (QDO149a)?
No minimum = 0; One hour or less = 0.5; More than one hour = 1
Fig. III.24
Important attached to organising working hours to fit
employees’ circumstances
very unimportant/ unimportant/neutral = 0; important = 0.5; very
important = 1
Minimum length of a visit
No min/15-29 minutes = 0; 30 minutes = 0.5; More than 30
minutes = 1
Staff required to work alone late at night
Yes = 0 Occasionally = 0.5 Never = 1
Table III.26
Contracts offered to care staff
All zero hours = 0
mix zero and guaranteed hours = 0.5 all guaranteed hours = 1
Fig. III.18
IHR7
IWTDOM1
IWTDOM2
IWTDOM3
IWTDOM4
IWTDOM5
IWTDOM6
IWTDOM7
Table III.42,
Fig. III.22
Fig. III.23
Fig. III.23
Table III.32
396
397
Appendix Table IV.A4. HR outcome indicators: non standardised data set
HR outcome
Indicators
(excluded from
standardised data
set due to too high
missing variables)
Description and range of scores
For data
distributions see
tables in part III
IRT2
Share of new starters in the last 12 months that have been
retained
less than 70%=0; 70-99%=0.5; 100%=1
Fig. III.8
IRT3
Overall level of staff turnover in the last 12 months
30%+=0; 10-29%=0.33; 1-9% =0.67; 0%=1
Staff turnover excluding new recruits (as a percentage of staff
12 months previously)
>30%=0; 20-29%=0.33; 10– 19%= 0.67; 0-10%=1
Fig. III.10
IRT9
Fig III.9
397
398
IV.A.2. Descriptive statistics for indicators, sub-indices and indices from the standardised dataset
Table IV.A5. HR practices by size
Homes
All
SIPAYLEVEL
Pay levels
0.33
SIPAYUPGRADE
Regular upgrading of pay
0.91
0.91
0.91
0.93
0.78
0.79
0.79
0.75
SIPAYUNSOCIAL
Pay for unsocial hours
0.28
0.31
0.30
0.19
0.44
0.40
0.46
0.45
SIPAYTRAIN
Pay for training
0.91
0.91
0.90
0.95
0.79
0.77
XPAYLEVELS
Index of pay levels
0.61
0.61
0.61
0.60
0.63
0.93**
(L)
0.65
0.63
0.65**
(VSS)
0.59
SIPAYIMP
Opportunities for pay improvement
0.44
0.44
0.38
0.52
0.46
0.43
0.51
0.40
SIPAYOPPCAR
Opportunities for career
0.78
0.77
0.88
0.82
0.72
Payment of upfront costs
0.83
0.86
0.64**
(VS)
0.85
0.81
SIPAYUPFRONT
0.92**
(ML)
0.76
0.67
0.77
0.67
0.58
XPAYSTRAT
Index of pay strategies
0.68
0.71
0.67
0.67
0.65
0.69
0.67
0.57
SIEMPVOICE
Employee voice practices
0.50
0.49
0.47
0.57
0.54
0.50
0.56
0.54
SIEMPAPP
Employee appraisal
0.65
0.66
0.60
0.68
0.61
Index of employee development
practices
Formality of recruitment process
0.58
0.57
0.59
0.55
0.62
0.57
0.58
0.63
0.75**
(S)
0.66**
(S)
0.55
0.64
XEMPDEV
0.57**
(ML)
0.52**
(ML)
0.55
0.72
0.77
0.71
0.69
Selection by skills, qualifications or
experience
Role of push factors in staff quits
0.58
0.54
0.64
0.55
0.62
0.63
0.67
0.69
0.68
0.64
0.54
0.50**
(L)
0.57
0.63
0.75**
(VSS)
0.33
Recruitment and retention practices
index.
Work schedules that fit staff preferences
0.61
0.62
0.62
0.58
0.63
0.61
0.65
0.59
0.64
0.59
0.71
0.57
0.61
0.65
0.63
0.55
SIRECRUITPR
SIRECRSELEC
SIRECRETEN
XRRPRACT
SIWTSTFFPREF
Small
0.33
Medium
& Large
0.35
All
0.50
IDPs
Very Small& Medium
Small
0.49
0.50
Very
small
0.31
Large
0.53
398
399
SIWTWEND
Weekend working
0.29
0.35
0.41**
(S)
0.77
0.32
0.31
0.58
0.30
0.77
0.17**
(ML)
0.84
SIWTLHOURS
Long hours/long weeks
0.80
0.73
0.59
0.62
0.70
SIWTTOFFTRAIN
Time off for training
0.87
0.94
0.84
0.82
0.86
0.96
0.83
0.85
XWT
Index of working time practices
0.65
0.66
0.64
0.64
0.63
0.63
0.66
0.60
SIWOTIME
Time discretion at work
0.96
0.97
0.95
0.96
0.83
0.79
0.88
0.79
SIWODISCRET
Task discretion at work
0.93
0.96
0.94
0.88
0.84
0.85
0.83
0.86
XWO
Index of work organisation practices
0.95
0.96
0.95
0.92
0.84
0.82
0.85
0.83
XHRPRACT
Overall index of HR practices
0.68
0.69
0.67
0.68
0.66
0.66
0.67
0.64
Table IV.A6. HR outcomes by size
Homes
All
Very
small
Small
Medium
& Large
All
IDPs
Very
Medium
small
& small
0.37
0.45
Large
SIRECDIFF
Recruitment difficulties
0.69
0.56
0.76
0.72
0.38
SITO
Perceptions of staff turnover
0.72
0.72
0.82
0.55
0.52
0.45
0.61
0.40
SIABSENT
Perceptions of absenteeism
0.63
0.66
0.70
0.48
0.46
0.52
0.47
0.40
XRROUTCOMES
Index of recruitment and retention
outcomes
Index of training outcome
0.68
0.64**
0.76**
0.58**
0.45
0.44
0.51
0.34
(ML)
(ML)
(VS &S)
0.87
0.84
0.70
0.63
0.67
0.69
0.44
XTRAINSKILDEV
0.81
0.24
399
Table IV.A7. HR practices by ownership
400
All
Homes
Local
National
chain
chain
SIPAYLEVEL
SIPAYUPGRADE
Pay levels
Regular upgrading of pay
0.33
0.91
0.36
0.93
SIPAYUNSOCIAL
Pay for unsocial hours
0.28
0.31
SIPAYTRAIN
XPAYLEVELS
SIPAYIMP
SIPAYOPPCAR
SIPAYUPFRONT
Pay for training
Index of pay levels
Opportunities for pay improvement
Opportunities for career
Payment of upfront costs
0.91
0.61
0.44
0.78
0.83
XPAYSTRAT
SIEMPVOICE
SIEMPAPP
XEMPDEV
SIRECRUITPR
SIRECRSELEC
0.68
0.50
0.65
0.58
0.58
0.58
SIRECRETEN
XRRPRACT
SIWTSTFFPREF
SIWTWEND
SIWTLHOURS
Index of pay strategies
Employee voice practices
Employee appraisal
Index of employee development practices
Formality of recruitment process
Selection by skills, qualifications or
experience
Role of push factors in staff quits
Recruitment and retention practices index
Work schedules that fit staff preferences
Weekend working
Long hours/long weeks
0.95
0.64
0.41
0.76
0.80*
(N)
0.66
0.53
0.64
0.59
0.68
0.54
0.37
1.00*
(S)
0.17**
(S)
0.92
0.61
0.45
0.70
0.93**,*
(S, L)
0.69
0.50
0.66
0.58
0.57
0.62
SIWTTOFFTRAIN
XWT
SIWOTIME
Time off for training
Index of working time practices
Time discretion at work
0.87
0.65
0.96
SIWODISCRET
XWO
Task discretion at work
Index of work organisation practices
0.93
0.95
XHRPRACT
Overall index of HR practices
0.68
0.57
0.60
0.57
0.44
0.89*
(N)
0.86
0.69
0.91**,*
(S,N)
0.89
0.90**,*
(S,N)
0.68
0.72
0.64
0.67
0.24
0.71*
(L)
0.83
0.61
0.99*
(N)
0.93
0.96*
(L)
0.68
0.67
0.61
0.64
0.29
0.80
IDPs
Local
National
chain
chain
Single
home
All
Single
home
0.27
0.83*
(N)
0.35**
(N)
0.89
0.58
0.44
0.87
0.76**
(N)
0.69
0.49
0.64
0.57
0.51
0.58
0.50
0.78
0.49
0.80
0.49
0.76
0.55
0.82
0.44
0.37
0.45
0.48
0.79
0.63
0.46
0.81
0.67
0.93
0.64
0.52
0.87
0.72
0.76
0.62
0.45
0.82
0.65
0.73
0.64
0.45
0.76
0.69
0.65
0.54
0.64
0.59
0.72
0.62
0.70
0.56
0.59
0.57
0.55
0.55
0.64
0.57
0.65
0.61
0.72
0.62
0.64
0.44
0.65
0.55
0.86
0.68
0.70
0.60
0.65
0.23
0.81
0.54
0.63
0.61
0.32
0.73
0.60
0.57
0.64
0.37
0.59
0.52
0.62
0.68
0.45
0.70
0.55
0.70
0.67
0.12
0.58
0.90
0.65
0.98
0.86
0.63
0.83
0.95
0.64
0.85
0.82
0.66
0.85
0.75
0.53
0.75
0.96
0.97**
(L)
0.68
0.84
0.84
0.83
0.84
0.82
0.84
0.91
0.83
0.66
0.65
0.66
0.67
400
401
Table IV.A8. HR outcomes by ownership
All
Homes
Local
National
chain
chain
Single
home
All
IDPs
Local
National
chain
chain
Single
home
SIRECDIFF
Recruitment difficulties
0.69
0.67
0.74
0.65
0.38
0.46
0.38
0.28
SITO
Perceptions of staff turnover
0.72
0.68
0.69
0.76
0.52
0.58
0.49
0.52
SIABSENT
Perceptions of absenteeism
0.63
0.66
0.58
0.65
0.46
0.53
0.41
0.55
XRROUTCOMES
Index of recruitment and retention outcomes
0.68
0.67
0.67
0.69
0.45
0.52
0.43
0.45
XTRAINSKILDEV
Index of training outcome
0.81
0.77*
(S)
0.71**
(S)
0.93**,*
(N,L)
0.63
0.86*
(N)
0.56*
(L)
0.60
401
402
Table IV.A9. HR practices by star ratings
Homes
IDPs
All
1*
2*
3*
All
1*
2*
3*
0.19*
(3*)
0.88
0.13**
(3*)
0.91
0.52**
(3*)
0.36
0.67
0.83
0.62**
(3*)
0.58**
(3*)
0.66
0.62
0.27
0.58
0.34
0.50
0.44
0.51
0.50
0.90
0.24**
(3*)
0.91
0.60*
(3*)
0.42
0.77
0.80
0.66**
(3*)
0.55**
(3*)
0.67
0.61
0.77
0.60
0.39*
(1*)
0.96
0.46**
(1*,2*)
0.92
0.68**,*
(1*,2*)
0.53
0.87
0.90
0.77**
(1*,2*)
0.35**
(1*,2*)
0.58
0.47
0.31
0.54
0.78
0.44
0.67
0.39
0.82
0.44
0.70
0.47
0.79
0.63
0.71
0.55
0.78
0.64
0.85
0.63
0.46
0.81
0.67
0.65
0.58
0.72
0.69
0.67
0.40
0.80
0.66
0.62
0.60
0.90
0.70
0.73
0.54
0.57
0.55
0.49
0.64
0.59
0.72
0.62
0.78
0.68
0.70
0.50
0.61
0.58
0.73
0.65
0.65
0.57
0.67
0.60
0.63
0.49**
(2*)
0.63
0.21
0.78
0.88
0.62
0.61
0.66**
(1*)
0.60
0.28
0.82
0.85
0.64
0.85
0.57
0.54
0.63
0.50
0.57
0.56
0.65
0.50
0.59
0.73
0.37
0.74
0.88
0.68
0.61
0.32
0.73
0.86
0.63
0.63
0.38
0.64
0.93
0.65
0.60
0.50
0.65
0.90
0.66
0.60
0.50
0.65
0.90
0.66
SIPAYLEVEL
Pay levels
0.33
SIPAYUPGRADE
SIPAYUNSOCIAL
Regular upgrading of pay
Pay for unsocial hours
0.91
0.28
SIPAYTRAIN
XPAYLEVELS
Pay for training
Index of pay levels
0.91
0.61
SIPAYIMP
SIPAYOPPCAR
SIPAYUPFRONT
XPAYSTRAT
Opportunities for pay improvement
Opportunities for career
Payment of upfront costs
Index of pay strategies
0.44
0.78
0.83
0.68
SIEMPVOICE
Employee voice practices
0.50
SIEMPAPP
XEMPDEV
SIRECRUITPR
SIRECRSELEC
0.65
0.58
0.58
0.58
SIRECRETEN
XRRPRACT
Employee appraisal
Index of employee development practices
Formality of recruitment process
Selection by skills, qualifications or
experience
Role of push factors in staff quits
Recruitment and retention practices index
SIWTSTFFPREF
SIWTWEND
SIWTLHOURS
SIWTTOFFTRAIN
XWT
Work schedules that fit staff preferences
Weekend working
Long hours/long weeks
Time off for training
Index of working time practices
0.64
0.29
0.80
0.87
0.65
0.67
0.61
402
403
SIWOTIME
SIWODISCRET
XWO
XHRPRACT
Time discretion at work
Task discretion at work
Index of work organisation practices
Overall index of HR practices
0.96
0.93
0.95
0.68
1.00
0.94
0.97
0.64
0.94
0.93
0.94
0.68
0.98
0.92
0.95
0.69
0.83
0.84
0.84
0.66
0.96
0.83
0.90
0.65
0.79
0.84
0.81
0.66
0.90
0.87
0.88
0.68
Table IV.A10. HR outcomes by star ratings
Homes
IDPs
All
1*
2*
3*
All
1*
2*
3*
SIRECDIFF
Recruitment difficulties
0.69
0.68
0.69
0.68
0.38
0.54
0.38
0.26
SITO
Perceptions of staff turnover
0.72
0.69
0.72
0.73
0.52
0.46
0.54
0.45
SIABSENT
Perceptions of absenteeism
0.63
0.66
0.61
0.65
0.46
0.42
0.48
0.43
XRROUTCOMES
Index of recruitment and retention outcomes
0.68
0.67
0.67
0.69
XTRAINSKILDEV
Index of training outcome
0.81
0.83
0.79
0.85
0.45
0.63
0.47
0.65
0.47
0.65
0.38
0.55
403
404
Table IV.A11. HR practices by LA commissioning practice
All
SIPAYLEVEL
Pay levels
0.33
Homes
Partnership
Mixed LAs
LAs
IDPs
Partnership
Mixed
LAs
LAs
Cost
Minimising
LAs
All
Cost
Minimising
LAs
0.50
0.55
0.48
0.45
0.44**
0.27**
0.24**
(M C)
(P)
(P)
0.83
0.15**
0.93
0.31
0.78
0.44
0.82
0.52
0.88
0.40
0.58
0.37
0.79
0.74
0.83
0.81
SIPAYUPGRADE
SIPAYUNSOCIAL
Regular upgrading of pay
Pay for unsocial hours
0.91
0.28
0.98
0.37**
(M)
(P)
SIPAYTRAIN
Pay for training
0.91
0.89**
0.89**
0.98**
(C)
(C)
(M P)
0.67**
0.54**
0.61
0.63
0.66
0.64
0.55
(M)
(P)
0.54**
0.41
0.33**
0.46
0.55
0.43
0.36
0.81
0.67
0.65
0.54
0.64
0.59
0.85
0.66
0.68
0.54
0.68
0.61
0.79
0.72
0.65
0.56
0.63
0.60
0.78
0.65
0.60
0.52
0.58
0.55
XPAYLEVELS
SIPAYIMP
SIPAYOPPCAR
SIPAYUPFRONT
XPAYSTRAT
SIEMPVOICE
SIEMPAPP
XEMPDEV
SIRECRUITPR
SIRECRSELEC
SIRECRETEN
XRRPRACT
SIWTSTFFPREF
SIWTWEND
Index of pay levels
Opportunities for pay
improvement
Opportunities for career
Payment of upfront costs
Index of pay strategies
Employee voice practices
Employee appraisal
Index of employee
development practices
Formality of recruitment
process
Selection by skills,
qualifications or experience
Role of push factors in staff
quits
Recruitment and retention
practices index.
Work schedules that fit staff
preferences
Weekend working
0.61
0.44
(C)
0.78
0.83
0.68
0.50
0.65
0.58
(P)
0.77
0.84
0.72
0.46
0.63
0.55*
0.81
0.80
0.67
0.49
0.61
0.55*
0.76
0.85
0.65
0.59
0.72
0.66*
(c)
(c)
(M P)
0.58
0.51
0.62
0.51
0.72
0.70
0.83
0.60
0.58
0.58
0.53
0.68
0.62
0.62
0.59
0.67
0.67
0.57
0.78
0.57
0.54
0.64
0.50
0.42
0.61
0.55
0.64
0.59
0.63
0.65
0.64
0.56
0.64
0.58
0.67
0.69
0.63
0.59
0.66
0.67
0.29
0.46**
0.12**
0.27
0.38
0.37
0.31
0.48
404
405
SIWTLHOURS
SIWTTOFFTRAIN
XWT
SIWOTIME
SIWODISCRET
XWO
XHRPRACT
Long hours/long weeks
Time off for training
Index of working time
practices
Time discretion at work
Task discretion at work
Index of work organisation
practices
Overall index of HR practices
(M)
(P)
0.71**
0.93**
0.74**
(M)
(P C)
(M)
0.93**
0.75**,*
0.93*
(M)
(P,C)
(M)
0.65
0.67
0.62
0.96
0.93
0.95
0.98
0.90
0.94
0.68
0.69
0.80
0.87
0.64
0.63
0.63
0.67
0.90
0.98
0.81
0.88
0.66
0.64
0.64
0.60
0.67
0.97
0.95
0.96
0.93
0.94
0.93
0.83
0.84
0.84
0.84
0.88
0.86
0.88
0.81
0.84
0.75
0.82
0.78
0.66
0.68
0.66
0.68**
0.66
0.62**
(C )
(P)
P, M, C used to indicate difference from partnership, mixed and cost minimising LAs respectively
Table IV.A12. HR outcomes by LA commissioning practice
All
SIRECDIFF
Recruitment difficulties
0.69
SITO
SIABSENT
XRROUTCOMES
Perceptions of staff turnover
Perceptions of absenteeism
Index of recruitment and
retention outcomes
Index of training outcome
0.72
0.63
0.68
XTRAINSKILDEV
0.81
Homes
Partnership
Mixed
LAs
LAs
0.60*
(C)
0.78
0.66
0.68
0.70
0.68
0.64
0.67
Cost
Minimising
LAs
0.80*
(P)
0.68
0.57
0.68
0.75**
(M)
0.94**
(P C)
0.73**
(M)
IDPs
Mixed
LAs
All
Partnership
LAs
0.38
0.36
0.38
Cost
Minimising
LAs
0.39
0.52
0.46
0.45
0.58
0.44
0.46
0.48
0.47
0.45
0.44
0.50
0.44
0.63
0.55
0.73
0.63
H, M, L used to indicate difference from high, medium and low fee paying LAs respectively
405
406
Table IV.A13. HR practices by LA fee level
All
SIPAYLEVEL
Pay levels
0.33
SIPAYUPGRADE
SIPAYUNSOCIAL
Regular upgrading of pay
Pay for unsocial hours
0.91
0.28
SIPAYTRAIN
XPAYLEVELS
Pay for training
Index of pay levels
0.91
0.61
SIPAYIMP
Opportunities for pay improvement
0.44
SIPAYOPPCAR
SIPAYUPFRONT
XPAYSTRAT
SIEMPVOICE
SIEMPAPP
XEMPDEV
SIRECRUITPR
SIRECRSELEC
SIRECRETEN
XRRPRACT
SIWTSTFFPREF
SIWTWEND
Opportunities for career
Payment of upfront costs
Index of pay strategies
Employee voice practices
Employee appraisal
Index of employee development practices
Formality of recruitment process
Selection by skills, qualifications or experience
Role of push factors in staff quits
Recruitment and retention practices index.
Work schedules that fit staff preferences
Weekend working
0.78
0.83
0.68
0.50
0.65
0.58
0.58
0.58
0.67
0.61
0.64
0.29
SIWTLHOURS
Long hours/long weeks
0.80
SIWTTOFFTRAIN
XWT
SIWOTIME
Time off for training
Index of working time practices
Time discretion at work
0.87
0.65
0.96
Homes
Low fees Medium
fees
0.20**
0.34
(H)
0.83
1.00
0.25
0.13**
(H)
0.93
0.88
0.55**
0.59
(H)
0.37**
0.38
(H)
0.81
0.77
0.79
0.82
0.66
0.66
0.52
0.57
0.68
0.64
0.60
0.60
0.50
0.72
0.57
0.51
0.61
0.60
0.56
0.61
0.68
0.60
0.17*
0.23
(H)
0.84**
0.95**
(H)
(H)
0.89
0.75
0.65
0.63
0.94
0.98
High
fees
0.47**
(L)
0.97
0.39**
(M)
0.91
0.69**
(L)
0.55**
(L)
0.75
0.88
0.73
0.45
0.62
0.53
0.59
0.64
0.79
0.67
0.61
0.46*
(L)
0.66**
(M L)
0.89
0.66
0.97
All fees
0.38
IDPs
Low fees
Medium
fees
0.54
0.57
High fees
0.50
0.80
0.36
0.75
0.40
0.80
0.58
0.78
0.44
0.85
0.60
0.74
0.61
0.78
0.68
0.79
0.63
0.26
0.57
0.52
0.46
0.80
0.70
0.59
0.55
0.54
0.54
0.71
0.57
0.40
0.56
0.67
0.29
0.82
0.65
0.68
0.52
0.69
0.60
0.74
0.63
0.60
0.65
0.60
0.49
0.82
0.69
0.68
0.56
0.67
0.62
0.70
0.67
0.60
0.66
0.63
0.31
0.81
0.67
0.65
0.54
0.64
0.59
0.72
0.62
0.54
0.63
0.63
0.38
0.63
0.66
0.62
0.64
0.73
0.58
0.92
0.98
0.68
0.70
0.97
0.63
0.92
0.90
0.64
0.83
406
407
SIWODISCRET
Task discretion at work
0.93
0.93
0.95
0.96**
(H)
0.95
XWO
Index of work organisation practices
XHRPRACT
Overall index of HR practices
0.82
0.81
0.91
0.84
0.95
0.89**
(L)
0.93
0.87
0.67
0.70
0.66
0.75*
(M)
0.62**
(H)
0.91**,*
(L,H)
0.70
0.84**
(M)
0.66**
(L)
0.68
0.66
H, M, L used to indicate difference from high, medium and low fee paying LAs respectively
Table IV.A14. HR outcomes by LA fee level
SIRECDIFF
SITO
Recruitment difficulties
Perceptions of staff turnover
SIABSENT
XRROUTCOMES
Perceptions of absenteeism
Index of recruitment and
retention outcomes
Index of training outcome
XTRAINSKILDEV
All
fee level
0.69
0.72
Low fees
0.75
0.69
Homes
Medium
fees
0.64
0.65
0.63
0.68
0.63
0.69
0.81
0.86**
(P)
High fees
All fees
0.64
0.78
0.38
0.52
0.55
0.61
0.67
0.70
0.46
0.45
0.95**
(P)
0.68**
(M L)
0.63
IDPs
Low fees
Medium
fees
0.38
0.39
0.37**
0.60**
(M)
(L)
0.43
0.54
0.39
0.51
0.71
0.67
High fees
0.35
0.55
0.40
0.43
0.49
H, M, L used to indicate difference from high, medium and low fee paying LAs respectively
407
408
Table IV.A15. HR practices by labour demand level
Homes
All
IDPs
Strong
demand
0.46**,*
(W,M)
0.98**
(W)
0.40**
(W)
0.92
Medium
demand
0.31*
(S)
1.00**
(W)
0.31
0.94
Weak
demand
0.20**
(S)
0.79**
(S M)
0.12**
(S)
0.89
0.64**
(W)
0.39
All
Strong
demand
0.56**
(W)
0.82
Medium
demand
0.56**
(W)
0.75
Weak
demand
0.38**
(S M)
0.75
0.79
0.56**
(M W)
0.73
0.31**
(S)
0.81
0.38
(S)
0.84
0.50**
(S,M)
0.38
0.63
0.67
0.61
0.59
0.46
0.48
0.56
0.36
SIPAYLEVEL
Pay levels
0.33
SIPAYUPGRADE
0.91
SIPAYUNSOCIAL
Regular upgrading of
pay
Pay for unsocial hours
SIPAYTRAIN
Pay for training
0.91
XPAYLEVELS
Index of pay levels
0.61
SIPAYIMP
Opportunities for pay
improvement
Opportunities for
career
Payment of upfront
costs
Index of pay strategies
0.44
0.69**
(W)
0.52
0.78
0.75
0.83
0.79
0.81
0.80
0.72
0.90
0.83
0.85
0.85
0.79
0.67
0.69
0.59
0.72
0.68
0.71
0.69
0.65
0.65
0.66
0.63
0.66
Employee voice
practices
Employee appraisal
0.50
0.51
0.54
0.47
0.54
0.53
0.53
0.56
0.65
0.63
0.73
0.61
0.64
0.62
0.60
0.69
Index of employee
development practices
Formality of
recruitment process
0.58
0.57
0.64
0.54
0.59
0.57
0.56
0.63
0.58
0.62
0.52
0.56
0.72
0.70
0.77
0.70
SIPAYOPPCAR
SIPAYUPFRONT
XPAYSTRAT
SIEMPVOICE
SIEMPAPP
XEMPDEV
SIRECRUITPR
0.28
0.50
0.78
0.44
408
409
SIRECRSELEC
0.58
0.62
0.51
0.58
0.62
0.62
0.63
0.63
0.67
0.71
0.67
0.63
0.54
0.64
0.58
0.38
0.61
0.65
0.57
0.59
0.63
0.65
0.66
0.57
0.64
0.59
0.63
0.69
0.38
0.45
0.48
0.20
Long hours/long weeks
0.80
0.64
0.64
0.66
0.63
SIWTTOFFTRAIN
Time off for training
0.87
0.90
0.95
0.96
0.78
XWT
Index of working time
practices
Time discretion at
work
Task discretion at
work
Index of work
organisation practices
Overall index of HR
practices
0.65
0.64
0.66
0.68
0.57
0.98
0.72**
(S)
0.06**
(S M)
0.87**
(S)
0.76**
(S)
0.60*
(S)
0.96
0.63
SIWTLHOURS
0.57**
(W)
0.48**
(W)
0.73**
(W)
0.93**
(W)
0.68*
(W)
0.95
0.63
SIWTWEND
Selection by skills,
qualifications or
experience
Role of push factors in
staff quits
Recruitment and
retention practices
index
Work schedules that fit
staff preferences
Weekend working
0.83
0.96**
(S)
0.97*
(S)
0.69**
(S)
0.97**
(S)
0.97**
(S)
0.64**
(S)
0.84
0.88**
(M)
0.86
0.63**
(S W)
0.82
0.92**
(M)
0.83
0.87**
(M)
0.68
0.72**
(S W)
0.64
0.88**
(M)
0.65
SIRECRETEN
XRRPRACT
SIWTSTFFPREF
SIWOTIME
SIWODISCRET
XWO
XHRPRACT
0.29
0.96
0.93
0.95
0.68
0.87**
(M W)
0.91**,*
(W,M)
0.70**
(M W)
0.33**
(W)
0.80
0.92
0.67
0.84
0.66
S, M, W used to indicate difference from strong, medium and weak labour market demand areas respectively
409
410
Table IV.A16. HR outcomes by labour market conditions
Homes
IDPs
All
Strong
demand
Medium
demand
Weak
demand
All
Strong
demand
Medium
demand
Weak
demand
SIRECDIFF
Recruitment difficulties
0.69
0.70
0.67
0.69
0.38
0.36
0.38
0.40
SITO
Perceptions of staff turnover
0.72
0.76
0.65
0.71
0.52
0.52
0.50
0.52
SIABSENT
Perceptions of absenteeism
0.63
0.67
0.54
0.64
0.46
XRROUTCOMES
Index of recruitment and
retention outcomes
Index of training outcome
0.68
0.71
0.62
0.68
0.45
0.43*
(M)
0.44
0.63**,*
(W,S)
0.50
0.39**
(M)
0.43
0.81
0.72**
(W)
0.76*
(W)
0.94**,*
(S,M)
0.63
0.46**.*
(W, M)
0.73*
(S)
0.78**
(S)
XTRAINSKILDEV
410
411
IV.A3. Technical notes on our presentation of results from the multivariate
statistical analysis
For all our regression analyses we used the backwards method. This method works by
beginning with an examination of the combined effect of all independent variables on the
dependent variable. Then in a series of steps, the independent variables that offer the weakest
explanatory value are removed and a new analysis is performed. As with other regression
methods, the final results provide coefficients for each independent variable that signify the
degree to which each one, when combined with the others, contributes to predicting the
dependent variable.
We have considerably simplified the results generated from our regression analysis and
therefore wish to provide a brief explanation of the format of tables used in the report. Each
table of results adopts the following general form43:
Effects of environmental factors and organisational characteristics on different indices
of HR practices for homes
b. X HRPRACT
Coefficient
Significance
LA fee levels
0.24
*
Single establishment
0.17
Private for profit
-0.46
i) With LA fees
Etc.
Coefficient
Significance
Female part-time pay
0.17
n.s.
n.s.
Single establishment
0.12
n.s.
***
Private for profit
-0.47
***
ii) With labour demand
Etc.
Note: OLS regression, sample 52 (homes) and 50 (IDPs). Adjusted R 2 of 0.32 (model i), 0.31 (model ii).
Since the backwards regression method removes those independent variables that are weakest
in terms of their predictive power, the tables do not list all the independent variables that
were included in the first step but rather those that remain in the nth step, selected because it
has best predictive power as estimated by the adjusted R2.
For each table, the title clarifies the nature of the relationship being tested and identifies the
independent variables and the dependent variable, in this case the summary X index HR
practices. The independent, explanatory variables are listed in the left-hand column. The
column „coefficients‟ presents the estimated effects of each variable on the outcome or
dependent variable. In all tables we use the standardised (beta) coefficients. Because the
dependent variables used are measured on a continuous 0-1 scale the interpretation of
coefficients is relatively straight forward. In the above example using the first model that
includes the LA fee variable (and excludes the labour demand variable) the results suggest
43
We borrow here from the style and explanation of statistical results presented in Gallie et al. (1998).
411
412
that for every unit increase in standard deviation of LA fees, holding all other factors
constant, the X index HRpractices increases by 0.24 times a standard deviation. For
dichotomous variables, such as Single establishment and Private for profit, the coefficient
refers to the effect on the dependent variable compared to the reference variable; in this case,
National chain and Voluntary not for profit, respectively. For example, the results generate a
negative standardised coefficient for the variable Private for profit, which means that
compared to Voluntary for profit homes there is negative impact on the dependent variable X
HRPRACT, again holding all other factors constant.
The importance of each variable is estimated by applying a t-statistic to measure the
statistical significance. To simplify the presentation the tables only present the result that is
derived from the t-statistics following a „starring‟ convention. A single * indicates a
minimum 90% confidence level (p < 0.1), ** indicates a 95% confidence level (p < 0.05) and
*** a 99% confidence level (p < 0.01). The abbreviation n.s. means the result is not
statistically significant.
Estimates of the adjusted R2 (the coefficient of determination) and sample size are provided
in the notes to each table. The R2 shows the proportion of variability explained by the
variables included in the model and for our regression method varies from 0 to 1. In the
above example, the first model had an adjusted R2 of 0.32, which means that the predictors
account for 32% of the variation of the index X HRpractices. The results presented in part IV
are confined to those where the independent variables in a particular model offer relatively
strong explanatory value. We therefore exclude from the text all results where neither the R2
nor the adjusted R2 exceeds 0.2. The one exception is for the model that explores the effects
on the index X Paylevels for IDPs, which has an adjusted R2 of 0.11 (with LA fees) and 0.12
(with labour demand), since we wished to compare the results with those for homes where the
models produce a higher value R2.
412
413
IV.A4. Description of variables for regression analyses
The following tables list the independent and dependent variables used in the regressions
presented in section IV.5.1 and IV.5.2.
Table IV.A17. Variables in regressions investigating indices of HR practices
Dependent variables
Independent variables
Notes
XHRPRACT
XPAYLEVELS
XPAYSTRAT
XRRPRACT
XEMPDEV
XWT
XWO
LA Partnership
LA fees levels
% dependency on LA
Local labour demand
Female part-time pay
Size
Ownership (3 categories):
national chain
local chain
single establishment
Private sector/ Voluntary sector
Partnership = 3, Mixed = 2, Cost minimisers = 1
For homes only
Range of 2-6
Median level of earnings (£) in local area
Converted into 2 dummies:
Dummy1 (Local chain= 1; others= 0)
Dummy2 (Single establishment= 1;
others=0)
Dummy (Private = 1; Voluntary= 0)
Table IV.A18. Variables in regressions investigating the HR outcomes
XRROUTCOMES and XTRAINSKILDEV
Dependent variables
Independent variables
XRROUTCOMES
XTRAINSKILDEV
XHRPRACT
XPAYLEVELS
XPAYSTRAT
XRRPRACT
XEMPDEV
XWT
XWO
LA Partnership
LA fees levels
% dependency on LA
Local labour demand
Female part-time pay
Size
Ownership (3 categories):
national chain
local chain
single establishment
Private sector/ Voluntary sector
Notes
Partnership = 3, Mixed = 2, Cost minimisers = 1
For homes only
Range of 2-6
Median level of earnings (£) in local area
Converted into 2 dummies:
Dummy1 (Local chain= 1; others= 0)
Dummy2 (Single establishment= 1;
others=0)
Dummy (Private = 1; Voluntary= 0)
413
414
Table IV.A19. Variables in regressions investigating the HR outcomes RT3 and RT9
Dependent variables
Independent variables
RT3
P2
RT9
P3
Notes
P4
P8
P11
HR1
HR4
HR5
HR7
IRC1
RC3
WT3
WT4
WT9
PDOM1
Only for IDPs
WTDOM2
Only for IDPs
WTDOM4
Only for IDPs
WTDOM7
Only for IDPs
LA Partnership
Partnership = 3
Mixed = 2
Cost minimisers = 1
LA fees levels
% dependency on LA
For homes only
Local labour demand
Range of 2-6
Female part-time pay
Median level of earnings (£) in local area
Size
Ownership (3 categories):
national chain
local chain
single establishment
Private sector/ Voluntary sector
Converted into 2 dummies:
Dummy1 (Local chain= 1; others= 0)
Dummy2 (Single establishment= 1;
others=0)
Dummy (Private = 1; Voluntary= 0)
414
415
IV.A5. Detailed results of selected regression models
The following results serve to accompany summary tables presented in Part IV section 5.3.
For the staff turnover measures, RT3 and RT9, we have used the logarithm of the actual
turnover rate, which means that the higher the measure the higher the level of staff turnover
and the worse the HR outcome.
Table IV.A20. The effects of environmental factors, organisational characteristics and
HR practices on measures of staff turnover for IDPs
a. Overall staff turnover (RT3)
Model i: With LA fees
Coefficient
Significance
Code
IP3
IP4
IP11
IHR1
IRC1
IRC3
IWT9
Female part-time pay
Regular uprating of pay
Pay uprating opportunities
Pay for CRB checks
Recognition agreement with
trade unions
Use of formal recruitment
methods
Skills and qualifications
desirable among job applicants
Time off from care duties to
attend training
Model ii: With labour demand
Coefficient
Significance
-0.26
0.47
-0.42
0.39
-0.40
**
***
***
***
***
-0.26
0.47
-0.42
0.39
-0.40
**
***
***
***
***
0.40
***
0.40
***
-0.23
*
-0.23
*
-0.20
*
-0.20
*
Note: OLS regression, sample 37 (IDPs). Adjusted R2 of 0.62 (model i), 0.62 (model ii).
b. Staff turnover excluding new recruits (RT9)
Model i: With LA fees
Coefficient
Significance
Code
IP3
IP4
IP8
IP11
IHR1
IRC1
IWT9
IWTDOM4
IWTDOM7
Partnership
Size
Regular uprating of pay
Pay uprating opportunities
Payment for weekend work
Pay for CRB checks
Recognition agreement with
trade unions
Use of formal recruitment
methods
Time off from care duties to
attend training
Work schedules that fit staff
preferences
Offering guaranteed hours
contracts
Model ii: With labour demand
Coefficient
Significance
0.46
0.24
0.28
-0.58
-0.35
0.43
-0.72
***
*
**
***
**
***
***
0.59
0.33
--0.61
-0.43
0.39
-0.75
***
**
-***
***
***
***
0.63
***
0.70
***
-0.30
**
-0.27
**
0.26
**
0.34
**
0.34
**
0.43
**
Note: OLS regression, sample 37 (IDPs). Adjusted R2 of 0.62 (model i), 0.56 (model ii).
415
416
Table IV.A21. The effects of environmental factors, organisational characteristics and
HR practices on measures of staff turnover for homes
a. Overall staff turnover (RT3)
Model i: With LA fees
Coefficient
Significance
Code
IRC3
Female part-time pay
Single establishment
Private for profit
Skills and qualifications
desirable among job applicants
-0.34
-0.26
0.23
-0.33
**
*
*
**
Model ii: With labour demand
Coefficient
Significance
-0.34
-0.26
0.23
-0.33
**
*
*
**
Note: OLS regression, sample 45 (homes). Adjusted R2 of 0.19 (model i), 0.19 (model ii).
b. Staff turnover excluding new recruits (RT9)
Model i: With LA fees
Code
IRC3
IWT4
Single establishment
Private for profit
Skills and qualifications
desirable among job applicants
% of staff who regularly work
weekends
Model ii: With labour demand
Coefficient
Significance
Coefficient
Significance
-0.28
0.24
-0.26
*
*
*
-0.28
0.24
-0.26
*
*
*
-0.28
*
-0.28
*
Note: OLS regression, sample 45 (homes). Adjusted R2 of 0.18 (model i), 0.18 (model ii).
416
417
V.A. Appendix part V
Table V.A1. Simplified identifier codes for case study organisations
Code in
telephone survey
XD
XD.HN.4
XD.H.5
XD.D.1
XD.D.3
XD.DIH.1
Case study code
for Part V
XD
XDHome1
XDHome2
XDDom1
XDDom2
XDLADP
RN
RN
RN.H.3
RN.H.1
RN.D.1
RN.D.2
RN.DIH.1
RNHome1
RNHome2
RNDom1
RNDom2
RNLADP
ON
ON.HN.1
ON.H.2
ON.D.1
ON.D.3
ON.DIH.1
ON
ONHome1
ONHome2
ONDom1
ONDom2
ONLADP
IL
IL
IL.H.4
IL.H.3
IL.HIH.1
IL.D.1
IL.D.2
ILHome1
ILHome2
ILLAHome
ILDom1
ILDom2
Table V.A2. Job positions of case study interviewees
Position of interviewees
Roles involving direct care work
Care Worker
Care Worker with Supervisory Role
Care Coordinator and Care Worker
Line Manager / Senior Car Worker
Roles involving organising/supporting care
work
Care Coordinator
Nurse with supervisory role
Service Manager
Line Manager/Coordinator
All
Female
Male
Migrant
Workers
69
14
3
2
62
13
2
2
7
1
1
6
5
2
2
1
5
2
2
1
1
417
418
Table V.A3. Working Hours of Case Study Interviewees by LA
XD
RN
ON
IL
All LAs
Domiciliary
workers per
LA
10.0
20.0
60.0
10.0
Care homes
workers per
LA
0.0
40.0
60.0
0.0
LA providers
workers per
LA
0.0
40.0
60.0
0.0
All providers
workers per
LA
4.0
32.0
60.0
4.0
No. of respondents
Under 16 hrs
16-30 hours
30-45 hours
Over 45 hours
10
11.1
22.2
44.4
22.2
10
0.0
37.5
50.0
12.5
5
0.0
60.0
40.0
0.0
25
4.5
36.4
45.5
13.6
No. of respondents
Under 16 hrs
16-30 hours
30-45 hours
Over 45 hours
9
0.0
20.0
60.0
20.0
8
10.0
20.0
70.0
0.0
5
0.0
100.0
0.0
0.0
22
4.0
36.0
52.0
8.0
No. of respondents
Under 16 hrs
16-30 hours
30-45 hours
Over 45 hours
10
0.0
18.2
63.6
18.2
10
0.0
20.0
70.0
10.0
5
0.0
80.0
20.0
0.0
25
0.0
30.8
57.7
11.5
No. of respondents
Under 16 hrs
16-30 hours
30-45 hours
Over 45 hours
11
5.0
20.0
57.5
17.5
10
2.6
28.9
63.2
5.3
5
0.0
70.0
30.0
0.0
26
3.1
33.7
54.1
9.2
Total respondents
40
38
20
98
Under 16 hrs
16-30 hours
30-45 hours
Over 45 hours
418
419
Bibliography
Akerlof, G. and Yellen, J. (1986) Efficiency Wage Models of the Labour Market, Cambridge:
CUP.
Andrews, G. and Phillips, D. (2000) „Moral dilemmas and the management of private
residential homes: the impact of care in the community reforms in the UK‟, Ageing and
Society, 20, 5, 599-622.
Andrews, G. and Phillips, D. (2002) Changing local geographies of private residential care
for older people 1983-1999: lessons for social policy in England and Wales, Social
Science and Medicine, 55, 1, 63-78.
Angel, C. (2007) A Fair Price For Care, A UKHCA Position Statement. Sutton: United
Kingdom Homecare Association (www.ukhca.co.uk/downloads.aspx?id=114).
Appelbaum, E., Bailey, T., Berg, P. Kalleberg, A. (2000) Manufacturing competitive
advantage: The effects of high performance work systems on plant performance and
company outcomes. Cornell University Press: Ithaca, NY.
Appelbaum, E., Bosch, G., Gautie, J, Mason, G, Mayhew, K. Salverda, W., Schmitt, J., and
Westergaard-Nielson, N. (2010) „Introduction and Overview‟ in J. Gautie and J. Schmitt
(eds) Low-Wage Work in the Wealthy World, New York: Russell Sage Foundation
Audit Commission (1997) Take Your Choice Audit Commission, London.
Balloch, S., Banks, L. and Hill, M. (2004) „Securing quality in the mixed economy of care difficulties in regulating training‟, Social Policy and Society, 3 (4): 365-374.
Barber, A. and Bretz, R. (2000) „Compensation, attraction and retention‟, in S. Rynes and B.
Gerhart (eds.) Compensation in Organisations: Current Research and Practice, San
Francisco: Jossey-Bass.
Barth, E. and Dale-Olsen, H. (2009) „Monopsonistic Discrimination, Worker Turnover, and
the Gender Wage Gap‟ IZA DP No. 3930 The Institute for the Study