Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Ebola virus disease wikipedia , lookup
Tuberculosis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Leptospirosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
West Nile fever wikipedia , lookup
Henipavirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Epidemiology of HIV/AIDS wikipedia , lookup
Diagnosis of HIV/AIDS wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
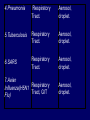
THE IMPACT OF TRANSMISSIBLE DISEASE IN THE PRACTICE OF DENTISTRY INTRODUCTION Many diseases are encountered in dental practice. The most common infectious disease we may encounter or give importance to in dental practice are bloodborne diseases or diseases that need transfer of body fluids such as blood or serum from the infected to the recipient. INFECTIOUS DISEASES COMMONLY ENCOUNTERED IN DENTISTRY CONDITION HABITAT ROUTES OF TRANSMISSION Oral, pharynx, ano-genital, skin, viscera, eye. Contact lesion exudate, saliva, sexual contact, blood. SEXUALLY TRANSMITTED DISEASES 1.Herpetic infections 2.Acute Oral, gingiva, herpetic pharynx. gingivostomatiti s Fingers, hands. 3.Herpetic Whitlow 4.Gonococcal infections Oral, pharynx, genitals. Contact lesion exudate, blood, saliva. Contact lesion exudate, blood, saliva. Contact lesion exudate, blood, saliva, nasopharyngeal secretions. 5.Chlamydial infections Genitals, eyes, oropharynx Contact lesion exudate, genital secretions, secretions from eye. 6.Trichomonal infections Contact lesion, Genitals, oral, mucosa, saliva, oropharynx, blood, body gastrointestinal fluids. 7.Condyloma Acuminatum Ano-genital Contact lesion, skin, oral, mucosa, blood. mucosal areas. 8.Syphilis 9.Infectious Mononucleosis 10.Hepatitis B virus Infection Genitals, skin, oral mucosa, oro pharynx. Contact-lesion, mucosa, saliva,blood, body fluids. ContactSkin, oral mucosa, saliva, mucosa, lesion exudate. genitals, parotids, saliva. Liver, blood,body fluids. Contactblood,saliva,bo dy fluids. 11.Hepatitis D virus Infection Liver, blood. Contact-blood, saliva, body fluids. 12.Hepatitis C virus Infection Liver blood. Contact-blood, saliva, body fluids. 13.Human Blood, oral Immunodeficien mucosa, skin. cy Virus Infection Contact-blood, semen, nonintact skin, Respiratory Diseases 1.Common cold Upper Respiratory Tract. 2.Sinusitis 3.Pharyngitis Aerosol, Contact. Upper Respiratory Tract. Aerosol, droplet. Upper Respiratory Tract Aerosol, droplet. 4.Pneumonia Respiratory Tract. Aerosol, droplet. 5.Tuberculosis Respiratory Tract. Aerosol, droplet. 6.SARS Respiratory Tract. Aerosol, droplet. 7.Avian Respiratory Influenza(H5N1 Tract, GIT Flu) Aerosol, droplet. Childhood Diseases 1.Chicken pox Oral, skin. Droplet, contact 2.Herpangia Oral, Oropharynx. Droplet, contact 3.Hand, foot & mouth disease Oral, hands, feet. Droplet, contact 4.Rubella & Rubeola Respiratory tract, oral skin. Droplet, contact 5.Mumps Parotids, pancreas, testis, CNS. Droplet, contact 6.Cytomegalo Virus Infection Droplet, contact Salivary glands Other Common Conditions 1.Hepatitis A virus Infection Liver, Ingestion, rarely gastrointestinal blood. tract. 2. Hepatitis E virus Infection Liver, Ingestion, rarely gastrointestinal blood. tract. ORAL LESIONS ASSOCIATED WITH INFECTIOUS DISEASE HEPATITIS Viral hepatitis refers to a primary infection of the liver. Caused by any of the heterogenous group of ‘hepatitis viruses’ which currently consists of types A, B, C, D, E and G. All the hepatitis viruses are RNA virus. Except type B which is DNA virus. HBV and HCV commonly causes occupational spread of infection. Hepatitis mainly transmitted through Fecal-Oral route Transfer of body fluids either parenterally/sexual contact. Diagnosis -detection for Ag*IEM *ELISA *Isolation -detection for Ab*IgM indicates recent infection * IgG -recent/remote infection and immunity. Treatment – General Preventive Measures Health education Improvement of personal hygiene Strict attention to sterility – Immunisation Passive Immunisation Active Immunisation – Plasma Derived Vaccine – Recombinant yeast hepatitis B HEPATITIS VIRUS HEPATITIS C LESION COMPARISON OF HEPATITIS VIRUSES TYPE A B C D (super /piggyback virus) E G TTV (recently identified virus) SOURCE Feces Blood and body fluids Blood and body fluids Blood Feces Blood and body fluids Blood possib ility feces PRIMARY FecelMODES oral OF TRANSMI SSION Percuta neous; permuc osal;se xual Percuta neous; permuc osal Percuta Percuta Fecelneous; neous oral permuc osal Blood INCUB ATION PERIO D. RISK OF CHRON IC INFECT ION 15-50 days. No chronic infectio n 50-60 days. Varies with age: Adults 5-10%; Children 2550%; Infants >85% 15-150 days. Very high 15-150 days. 5% when acquire d as coinfectio n with HBV; >70% when acquire d as a 2nd infectio n in chronic HBV carrier 15-60 days. No chronic infectio n Unknow Unknow n. n. Unknow Unclear n whether chronic infectio n occurs Protec tive immun ity after infecti on? Yes; AntiHAV Ab Usually; Ab to core Ag, and surface Ag are produce d; Ab (HbsAg) are produce d; Ab HbsAg is most protecti ve; chronic carrier states exists. No; antiHCV Ab is produce d but is usuallay not protecti ve. Because Unknow HDV n infection requires previous infection or coinfection with HBV, protecti ve immunit y is similar to hepatitis B Unknow n Unknow n VACCI NE AVAIL ABLE? Yes Yes No Yes No No No (HBV vaccine protect s against HDV) • India with a population of approximately 1 billion stills harbors approximately 30 million HBV carriers. • HBV is responsible for about 68% of cirrhosis of liver and 80% of hepatocellular carcinoma in India. HUMAN IMMUNODEFICIENCY VIRUS NOT single factor has affected the practice of dentistry since the early 1980’s more than acquired immunodeficiency syndrome. HIV is a condition where transmission occurs through contact with blood and other body fluids. This disease was identified in June 1981 and has been the plague of the 20th century. Initially seen among homosexuals later in all parts of society- heterosexuals, females and children. The initial HIV infection progresses into a more severe and debilitating condition where it is associated with a variety of other infections and is called Acquired Immuno Deficiency Syndrome (AIDS) In the EARLY stages- infection - may not be noticeable and may be accompanied by symptoms such as weakness, arthralgias or - even totally asymptomatic. On progression- infection - may be associated with a variety of conditions. HAIRY LEUKOPLAKIA ORAL CANDIDIASIS Some of the ORAL LESIONS associated with HIV infection and AIDS – Hairy Leukoplakia, Kaposi’s, Sarcoma, Candidiasis, etc. Systemic conditions associated with AIDSprotozoal, fungal, other viral and myobacterial infection. Diagnosis – Detection of Ag Test for p24 core Ag- represent acute/sero conversion – Detection of Ab Screening test- ELISA Confirmatory test- Western blotting KAPOSIS SARCOMA EXTENSIVE KAPOSIS SARCOMA Treatment – General Management – Treatment and prophylaxis of oppurtunistic infections and tumours – Immunorestorative Measures – Antiviral therapy India is among the highest caseload of HIV infected people with about half the population in sexually active stage .i.e.15 years and above(0.3%). Population of India is 1 billion and the population with HIV is 2.4 million. First HIV case was detected in 1986 by Dr S. Solomon. The spread of HIV in India has been diverse with much of India having a low rate of infection and the epidemic being more prevalent in the southern region and the far north-east. Highest HIV prevalence rate in India – Far north-east i.e. Manipur, Nagaland- due to unsafe injection drug use, sex workers. – Southern states i.e. Tamil Nadu, Andhra Pradesh, Karnataka- due to sexual contact – West i.e. Maharashtra, Gujarat In 2000 Larry Kramer, the co-founder of the AIDS Coalition to Unleash Power, reminded the world that AIDS crisis is more devastating than ever. “Even if we were to find a cure tomorrow, millions and millions of people will die. You were all told this before it was too late. Now it is too late. So sit back and watch the destruction of world.” Dealing with the HIV and its consequences may prove to be the greatest challenge ever faced by the dental profession. The manner in which dentistry responds to this challenge may, to a large degree, shape dentistry’s FUTURE. TUBERCULOSIS Tuberculosis is one of the oldest infectious diseases known to humans. Causative organism- M.tuberculosis Transmission by inhalation of infective droplets expelled through cough by an infectious patient with active pulmonary disease. Mostly affects lungs But can virtually affect every organ system in the body. TB is able to produce acute to latent chronic disease TUBERCULOUS LUNGS ORAL TUBERCULOUS LESION Diagnosis – – – – – – – – Sputum AFB Gastric lavage BAL Trans Bronchial Biopsy PCR Culture ESR Mantoux test – – – – Rifampicin INH Ethambutol Pyrazinamide Treatment Tuberculosis has been and continues to be taking a terrible toll on the Indian population. Causes 3,64,000 deaths annually. There were more than 1.8 million new TB cases in India in 2004. It represents 1/5th of all TB cases worldwide. ORAL TUBERCULOUS LESION RISK TO THE PATIENT • Health care workers; primarily physicians and dentists, have a 3 fold to 5 fold higher prevalence of HBV than the general population does. • HBV transmission had been well documented from dentists to patients. • Since the early 1970’s when serologic testing became available for HBV, the CDC had reported on 20 clusters of HBV transmission to more than 300 patient from infected health care workers. • In 12 of the clusters the health care worker did not routinely use gloves, and some reported skin lesions that could have promoted the transmission. • Nine of these clusters were linked to dentists or oral surgeons. • Most of the reports were before the acceptance of Universal Precautions. • The CDC suggested that “the limited no .of reports of HBV transmission from HCWs to patients in recent years may reflect the adoption of Universal Precautions and increased use of HBV vaccine. • Recent reports of HBV transmission from a health care worker to patients during performance of invasive, exposure-prone procedures are not among dentists, but refer to a surgeon who is HBeAg +ve and had not been vaccinated against HBV. • Factors of transmission were more likely related to irritations on the surgeon’s fingers and virus which may have escaped through tiny holes in the gloves was found in the glove washings. • However transmission from HIV infected dental health care workers to patients had not yet been reported. • HERPES transmission occur mostly from from dental hygienists to patients. • HCV transmission in health care facilities has also been documented. • Simultaneous transmission of HIV and HCV to a health care worker who sustained a deep needlestick injury from an HIV/HCV infected source patient in 1990 was reported. • Use of zidovudine was declined. • Researchers at the International Conference on Emerging Diseases convened in 2000 reported that Health Care Workers had a 20 to 40 times greater risk of contracting HCV from an accidental needlestick than HIV. RISK TO DENTAL HEALTH CARE WORKERS • The first case of occupationally aquired HIV infection, by needlestick, was reported in Africa in 1984. • As of December 31, 1999, 56 health care workers had been reported to CDC as having a documented occupational transmission of HIV. • Among the documented cases – – – – 48 reported percutaneous exposure. 5 blood splashes to eyes, nose or mouth. 2 percutaneous + mucocutaneous exposure 1 reported an unknown route. • Reporting occupational incidents to agencies is important in tracking not just seroconversion but the routes and circumstances of injury as well. • CDC has 2 programs for voluntary reporting: – Incidents related to Known HIV infected source individuals reported to – The National Studies for Infectious Disease. – Documented HIV seroconversion reported to – local/state health department, which further reports to CDC. – Reports of medical device failures that may facilitate the injury should go to the FDA Medwatch program. • In February 1995, OSHA issued a guide to dental employer obligations as a follow-up to the bloodborne pathogens std in regard to occupational exposure. • The employer is obligated to provide, not perform, a confidential medical evaluation and follow-up by a licensed health care professional at no cost to the employee. • The medical services that the employee must be offered are counseling, collection and testing of the employees blood, post exposure prophylaxis and evaluation of reported illness. • The employer is obligated to pay the cost of treating the incident and not the cost of the subsequent disease should seroconversion occur. • The current U.S. Public Health Service recommendation is that health care workers who are exposed to HIV on the job should, in many cases, take zidovudine and other antiretroviral drugs after exposure to reduce their risk of becoming infected. • Most percutaneous injuries occurred outside the patient’s mouth, most on the hands of the dentist. Burs were the most common source(37%), followed by syringe needles(30%), sharp instruments(21%) and orthodontic wires(6%). • The best estimates of risk to health care workers: – 0.3% for HIV transmission from percutaneous exposures and 0.09% for mucous membrane exposures – 3-10% for HCV – 30% for HBV transmission from after percutaneous injury from an infected patient. PREVENTION & INFECTION CONTROL Even if cure is available, protection from the untoward effects and discomforts of each disease would be desirable. Because many diseases can go undetected for long periods of time, the focus must be on preventing disease transmission from providers to patients, vice versa and between patient and family. Methods for the prevention and infection control includes: Medical history Vaccinations Protective Attire and Barrier Techniques Handwashing and Care of Hands Use and Care of Sharp Instruments and Needles Disinfection in the Dental Laboratory Use and Care of Handpieces, Antiretraction Valves, and Other Intraoral Dental Devices Attached to Air and Water Lines of Dental Units Single-Use Disposable Instruments Sterilization and Disinfection of Instruments Cleaning and Disinfection of Dental unit and Environmental Surfaces Use of Extracted Teeth in Dental Education Settings Disposal of Waste Materials Boil Water Advisories Dental Unit Water Quality Infection Control in Public Health Settings WHEN CAN INFECTED CLINICIAN RETURN TO WORK? CONDITION WHEN SHOULD ONE RETURN TO WORK/WHAT IS TO BE DONE? Conjunctivitis Staph. Aureus Strep. Group A After discharge ceases. After lesions have healed. 24 hrs after starting effective antimicrobial treatment. After resolution of acute infection. Viral Respiratory Infection Active tuberculosis After treatment with antimicrobials. Positive skin test for TB After evaluation of infectious status, chest X ray, and treatment if needed till deemed non-infectious. After symptoms resolves. Influenza Pediculous (hair lice) After treatment provided and no lice. After lesions heal. Herpetic Whitlow After lesions heal, need to be Orofacial Herpes regularly on anti-herpes medicines for the rest of the life. After lesions dry and crust out . Chicken pox After lesions dry and crust out. Shingles HCV seropositive Need to use UP/SP, Proper Aseptic HIV/AIDS Measles Mumps Rubella Pertussis Techniques to protect patients, Anti-viral Medication,Monitoring. After anti-retroviral therapy started, US/SP and expert panel/ Infectious Diseases MD to monitor clinician. After 7 days from the appearance of rash. After 9 days from start of parotitis. After 5 days from the appearance of rash. After 5 days from the start of effective antimicrobial therapy. HBV After deemed HBe antigen –ve, UP/SP and expert panel /Infectious diseases MD to monitor clinicial. After symptoms resolve. Diarrhea After starting effective antimicrobial Amoebiasis therapy and symptoms resolve. After symptom resolves. Enteroviral Infections After 7 days from the onset of HAV jaundice. LEGISLATION AND LITIGATION Refusals to treat people with HIV/AIDS by dentists and other health care professionals may well be the most common and blatant form of discrimination against people with HIV today. TITLE III OF THE AMERICANS WITH THE DISABILITIES ACT Is specific in the type of discriminatory conduct that is prohibitted. According to this it is illegal to do the following: 1. Deny an HIV +ve patient the “full and equal enjoyment ”of dental services or Deny an HIV +ve patient the “oppurtunity to benefit” from dental services in the same manner as other patients. 2. Establish for the privilege of receiving dental services ”eligibility criteria” that tend to screen out patients who have tested +ve for HIV. 3. Provide “different or separate” services to patients who are HIV +ve or fail to provide services to patients in the most “integrated setting”. 4.Deny equal services to a person who is known to have a “relationship“ or “association” with a person with HIV, such as a spouse, partner, child, or friend. Although the AWDA has specific prohibitions against discrimination by places of public accommodation, it does permit the denial of services to an individual where there is a “direct threat to the health and safety of others”. DECISIONS Implementation of a policy that the dentist would not discriminate on the basis of HIV/AIDS. Paying the estate of the complaint $20,000 in compensatory damages + $9,000 in civil penalitiesUnder Title III of the AWDA the Department of Justice (In East Hartford). Agreement including staff training on non discrimination and requirements to provide “equal services” to persons with HIV and “send periodic reports to DOJ for the monitoring of compliance” & Payment of $80,000 for compensatory damage for refusal to treat an HIV +ve patient- Federal Govt. (In Houston) In addition (Owner and Managing companies of Castle Dentals) paid $10,000. Ruling of PRETEXT against the referal and compensatory payment of $25,000+$ 25,000 for punitive damage+ maintenance of policy of nondiscrimination for refusing treatment for an HIV +ve patient and refering to specialized clinic- Federal Court in New Jersy. THE FUTURE • During 1996 World Congress of the American Dental Association, members who questioned the efficacy of Universal Precautions were soundly defeated by the scientific community reaffirming the effectiveness of Universal Precautions. • Courts have decided that it is safe to provide oral health services to persons with HIV/AIDS, But appeals to these decisions will determine the future role of the profession, the protection of the HIV infected, and the safety of providing oral health care services. REFERENCES Clinical Periodontology – CARRANZA’S Clinical Periodontology – RATEITSCHAK JHONG’S Community Dental Health – GLUCKS , MORGANSTEIN Textbook of Microbiology – ANANTHANARAYANA Textbook of Microbiology – BAVEJA Indian Dentist Research and Review. Internet THANKYOU