Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
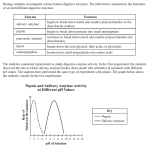
ELEVATED SERUM AMYLASE ASSOCIATED WITH BRONCHOGENIC CARCINOMA REPORT OF CASE* M U R R A Y J . W E I S S , M.D., H U G H A. E D M O N D S O N , M . D . , AND M A X I N E YVERTMAN, A.B. From the Laboratory of the Los Angeles County Hospital and the Departments of Pathology and Medicine, School of Medicine, University of Southern California, Los Angeles, ' California Almost any disease process that involves the pancreas or salivary glands directly or indirectly may produce an elevation of the blood amylase. Deviation from the normal amylase values (50-150 units) has been reported in many diseases foreign to these two structures. Among these is an unexplained elevation of serum amylase occasionally seen in pulmonary diseases such as pneumonia and tuberculosis. Adrenal insufficiency (in dogs),10 retroperitoneal tumors, 10 mesenteric cyst,10 thyroid lesions,1, 10 cholecystic disease,6 7 intestinal obstruction,10 portal or mesenteric vein thrombosis,10 perforated peptic ulcer,3 appendicitis,0 and hypophysectomized animals3 have also been reported as being associated with elevated blood diastase. In addition we have observed high amylase values in myocardial infarction and dissecting aneurysm.4 Because amylase is excreted in the urine, high blood levels can be expected in many diseases coincidental with impaired renal function.6, s> 10 In our experience serum amylase values above 500 units are almost exclusively related to pancreatitis or salivary gland disease. High values in other associated diseases are usually below this figure. Perusal of the American literature revealed the highest reported amylase value to be 25,600 units.2 This was associated with an acinar cell carcinoma of the pancreas. It has been stated that the occasional elevated amylase value not caused by pancreatic or salivary gland disease will rarely be a source of diagnostic confusion. The problem presented by the patient of the case herein reported was that of exceptionally high amylase values without pancreatic disease. R E P O R T O F CASE Clinical Data A 45-year-old housewife was admitted to the hospital on May 11, 1949. She had been in fair health until J a n u a r y 1949, when she experienced vague aching pain in the epigastrium and right upper q u a d r a n t , radiating around the right (lank and into the right shoulder. This pain was not related to meals or breathing. There was no cough, hemoptysis or j a u n dice. She had lost 25 pounds a t the time of admission. On physical examination she was pale and cachectic, but not icteric. Decreased resonance was elicited at the base of the right lung. The edge of the liver was nodular, irregular, hard and palpable 6 cm. below the right costal margin. T h e laboratory findings were as follows: hemoglobin, 14.5 Gm. per 100 ml. blood; leukocytes, 31,250 per cu. mm. with 84 per cent polymorphonuclear neutrophils; erythrocytic * Received for publication, J u n e 11, 1951. 1057 1058 WEISS, EDMONDSON AND WERTMAN sedimentation rate (Wintrobe), 26 mm. in one hour; nonprotein nitrogen, cephalin flocculation, blood sugar, and icterus index within normal limits; serum albumin 3.1 and serum globulin 3 Cm. per 100 ml.; thymol turbidity, 8 units; serum calcium (repeated), 7.7 rag. per 100 ml. Blood amylase and urinary diastase levels ranged as follows: May 5, blood amylase, 5450 units;* May 11, blood amylase 16,000 units, urinary diastase 19,04S units; May 14, amylase 8400 units and urinary diastase 17,400 units with a total urinary output in 24 hours of 153,000 units. Foci of infiltration were seen in the right upper lung field by x-ray. Upper gastrointestinal roentgen studies with barium revealed no abnormalities. The patient received symptomatic care but slowly became worse and died on May 21, 1949. The clinical diagnosis was pancreatic carcinoma with metastases. Pathologic Findings At necropsy the upper lobe of the right lung was densely adherent by fibrous adhesions to the parietal pleura. In the anterolateral segment there was a hard indurated lesion 2.5 cm. in diameter over which the visceral pleura was puckered. On section the indurated lesion was composed of gray-white tumor tissue. Thick fibrous strands coursed through the entire apical segment. The middle and lower lobes were without change. The lower lobe of the left lung contained an embolus which had produced an extensive hemorrhagic infarct. Both pleural cavities were free of fluid. The liver weighed 2750 Gm. and was filled with circular to irregularly shaped masses of tumor, some discrete, others confluent. Their average diameter was 8 mm. The twelfth thoracic vertebra and the right ilium were infiltrated with gray-white tumor. There was no evidence of metastasis to the retroperitoneal lymph nodes. The pancreas was normal in size and appearance. The ducts were patent and free of any abnormality. Because of autopsy restrictions the salivary glands were not dissected, but no changes were noted on palpation. Tissue amylase study. A portion of the tumor from the liver was ground and assayed for amylase. It contained 4100 units per 103 Gm. of tissue. Unfortunately other organs were not assayed as a control. Histologic findings. In sections through the tumor the neoplastic cells to a large extent had used the lung parenchyma as scaffolding for their growth. Most of the tumor had an adenomatous arrangement, the cells being tall columnar, with moderate sized hyperchromatic nuclei. Mitoses were numerous and vacuoles in the cytoplasm were present to a variable degree (Fig. 1). Fat stains disclosed some of these vacuoles to be fat. Mucin stains were negative. The neoplastic cells tended to grow into the small bronchi and bronchioles, replacing normal epithelium (Fig. 2). Not infrequently neoplastic cells with granular hyaline cytoplasm were noted. These were believed to represent primitive squamous cells. In two sections wide areas of old pigmented scar tissue contained tumor, thus raising the possibility of origin of the cancer in a healed subapical tuberculous lesion. In other sections of lung the tumor had grown widely into * The test for amylase activity in our laboratory is done by a modification of Somogyi's method." It is measured by the hydrolysis of a starch solution under given conditions and 1 unit is equivalent to 1 rag. of sugar per 100 ml. of the fluid in question. HIGH SERUM AMYLASE AND LUNG CANCER 1059 F i e . 1 (upper). Adenocarcinoma with intracytoplasmic vacuoles. Hematoxylin and eosin. X 320. F I G . 2 (lower). Growth of cancer cells into bronchiole. Hematoxylin and eosin. X 4S0. 1060 WEISS, EDMONDSON AND WERTMAN vascular channels; here the arrangement was not adenomatous but medullary. Sections of the left lower lobe disclosed only hemorrhage and necrosis. The metastases in the liver were numerous, large, and likewise more medullary in character. Intravascular growth was obvious. In sections of the pancreas there was no dilatation of the ducts, but many of the ducts contained pink-staining debris and a few, areas of epithelial hyperplasia. No evidence of obstruction to the duct system or of pancreatitis was perceived. The presence of a unilateral lung tumor composed of both columnar and squamous cells with the metastatic pattern described was considered good evidence for a primary lung cancer. COMMENT No previous reports of elevated serum amylase values associated with bronchogenic carcinoma were noted in the literature. However, it has been reported TABLE 1 SERUM AMYLASE IN PULMONARY D I S E A S E CLINICAL DIAGNOSIS Bronchogenic carcinoma Bronchogenic carcinoma Bronchogenic carcinoma Bronchogenic carcinoma Bronchial asthma or bronchogenic carcinoma Lung abscess Far-advanced pulmonary tuberculosis Bronchial asthma Hemoptysis, etiology undetermined SERUM AMYLASE (UNITS) 102 246 <100 <100 575 <100 <100 <100 <100 that other pulmonary diseases, such as pneumonia, not infrequently are associated with elevation of serum amylase.9 The possibility that the mucosal secretions of the bronchi and trachea might play a role in amylase production was entertained by us. Thus neoplasms originating from the bronchial mucosa epithelium might occasionally form enough of the enzyme to elevate the serum amylase. Values ranging from 600 to 12,000 units were obtained from material aspirated at bronchoscopy and from bronchial scrapings at necropsy. However, amylase determinations on material aspirated from the trachea through a tracheotomy tube in patients on whom a laryngectomy had been performed, gave values of less than 100 units. In these patients there was no possibility of contamination with saliva. This is important, as the diastatic activity of saliva is extremely high: by our methods the range was between 50,000 and 125,000 units. Blood amylase determinations were done on a group of unselected patients with varied pulmonary diseases. The results are listed in Table 1. Although an occasional elevated value was noted, no conclusions could be drawn. HIGH SERUM AMYLASE AND LUNG CANCER 1061 Another source of error in differential diagnosis in patients with elevation of serum amylase has recently been publicized by Gross and associates.6 They •noted that the administration of codeine and other opiates would result in an elevated blood amylase. This factor was not operative in our patient, as aspirin was the only analgesic administered until late in the disease when narcotics were necessary. The mechanism involved in the elevation of serum amylase has not been established. Ligation of the pancreatic or parotid duct results in a transient elevation. Pancreatectomy causes a transient fall, following which the diastatic activity soon returns to normal.3 Liver disease is usually associated with normal or low blood amylase values.3 There was no evidence that the pancreas or salivary glands caused the high amylase in our patient. Therefore the mechanism responsible for the amylase elevation is unknown. The possibility that the tumor cells might have formed the enzyme is to be considered, but since determining the amylase content in the liver metastasis we have been unable to detect any amylase activity in several bronchogenic carcinomas procured at autopsy. That bronchogenic carcinoma may occasionally be associated with a high value of serum amylase is of some clinical importance in a negative sense in that search for other causes of the condition need not necessarily be made. SUMMARY A case of bronchogenic carcinoma with exceptionally high serum amylase values is reported. No explanation can be offered concerning the mechanism of its production. REFERENCES 1. BARTLETT, W., J R . : Effects upon blood amvlase of variations in thvroid activity. Proc. Soc. Exper. Biol, and Med., 36: S43-S4S, 1947. 2. C O M F O R T , M. W., B U T T , H . R., BAGGENSTOSS, A. H . , O S T E R B E R G , A. E . , AND P R I E S T L Y , J. T.: Acinar cell carcinoma of pancreas: Report of case in which function of carcinomatous cells was suspected. Ann. I n t . Med., 19: S0S-S16, 1943. 3. COMPORT, M. W., AND OSTERBERG, A. E.: Serum amylase and serum lipase in the diagnosis of disease of the pancreas. M. Clin. N o r t h America, 24: 1137-1149, 1940. 4. EDMONDSON, H . A., B E R N E , C. J., H O M A N N , R. E . , J R . , AND W E R T M A N , M . : T h e calcium, potassium, magnesium, and amylase disturbances in acute pancreatitis. Am. J. Med., in press. 5. G R O S S , J. B . , COMFORT, M. W., M A T H I E S O N , D . R., AND P O W E R , M . H . : E l e v a t e d values 6. 7. 8. 9. 10. 11. for serum amylase and lipase following the administration of opiates: A preliminary report. Proc. 'Staff Meet., Mayo Clin., 26: S1-7S, 1951. L E W I S O N , E . F . : T h e clinical value of the serum amvlase test. Surg., Gynec. and Obst., 72: 202-212, 1941. M C C A L L , M. L., AND R E I N H O U ) , J. G . : An evaluation of the clinical significance of serum amylase and lipase determinations. Surg., Gynec. and Obst., 80: 435-440, 1945. M C C O R K L E , H., AND GOLDMAN, L.: T h e clinical significance of the serum amylase test in the diagnosis of pancreatitis. Surg., Gvncc. and Obst., 74: 439-445, 1942. POLOWE, D . : Blood amylase. Am. J . Clin. P a t h . , 13: 2SS-301, 1943. POLOWE, D . : Blood amvlase activity in pancreatitis and other diseases; a simple diagnostic aid. Surg., Gynec. and Obst., 82: 115-130, 1946. SOMOGYI, M.: Micromethods for estimation of diastase. J. Biol. Chem., 125: 399-414, 1938.