Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Rheumatic fever wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
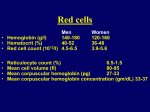
Nephrol Dial Transplant (2005) 20 [Suppl 7]: vii3–vii6 doi:10.1093/ndt/gfh1099 Anaemia and heart failure: statement of the problem Basil S. Lewis, Basheer Karkabi, Ronen Jaffe, Rita Yuval, Moshe Y. Flugelman and David A. Halon Department of Cardiovascular Medicine and the Cardiovascular Clinical Research Unit, Lady Davis Carmel Medical Center and Bruce Rappaport School of Medicine, Technion-IIT, Haifa, Israel Abstract While advances in treatment strategies and pharmacotherapy have produced a dramatic reduction in the mortality of patients with heart failure during the past 15 years, there is still a major challenge to improve patient well being, reduce hospitalizations and reduce mortality further. The prevalence of heart failure is not decreasing, and heart failure is currently a cause for hospitalization in >25% of admissions to internal medicine and cardiology departments. It has recently become apparent that anaemia is present in 20–30% of patients with heart failure, and the severity of anaemia has important implications regarding outcome and prognosis. Anaemia may be due to a number of causes, including iron and vitamin deficiency, insidious blood loss, haemodilution, renal impairment and bone marrow depression with resistance to erythropoietin. In the presence of a damaged heart and often coronary artery disease, anaemia may worsen contractile ability and systolic function, while the necessary volume load and ventricular hypertrophy which accompany anaemia contribute to diastolic dysfunction. Preliminary data show that appropriate treatment of anaemia, based on correction of the underlying cause, with, in most patients, the addition of exogenous erythropoietin and iron therapy, improves ventricular function and clinical status. Treatment of anaemia has opened a new frontier in the management of heart failure. We await the results of ongoing clinical trials for more detailed imformation regarding appropriate haemoglobin targets, choice of medication and dosing and the degree of improvement that may be expected when the issue of anaemia is properly addressed. Keywords: anaemia; erythropoietin; heart failure; iron deficiency; renal failure Correspondence and offprint requests to: Basil S. Lewis, MD, FRCP, Louis Edelstein Professor of Medicine and Medical Research, Department of Cardiovascular Medicine, Lady Davis Carmel Medical Center, 7 Michal Street, Haifa 34362, Israel. Email: [email protected] Introduction Although we have witnessed a dramatic reduction in the mortality of patients with heart failure during the last 15 years, from a 12 month mortality of 52% in the placebo arm of the CONSENSUS I trial [1] to 17% for similar patients in the treatment arm of the MERIT-HF study [2], the mortality and morbidity of the disease present a continuing challenge to the medical community. The incidence of heart failure is increasing, with an estimated 500 000 new cases in the USA alone each year. Heart failure was the discharge diagnosis in 27.4%, and suspected heart failure was present in another 6.2% of 1095 consecutive patients hospitalized in internal medicine/cardiology departments in a recent survey in Israel (Figure 1). The current management of heart failure includes treatment aimed at improving cardiac function, haemodynamics and overall patient well being. We aim to reduce mortality and the need for repeat cardiac hospitalizations with its inherent load on the already overburdened health care system of most countries. In recent years, attention has been drawn to the deleterious effect of anaemia on patients with heart failure and the potential benefit of appropriate treatment [3–7]. Here we will outline key issues regarding the pathophysiology of anaemia in heart failure and provide a physiological basis for what treatment of anaemia may achieve in heart failure patients. Prevalence of anaemia in heart failure patients Anaemia, defined as a haemoglobin level of <12 g%, has been noted in a considerable number of patients with heart failure. We surveyed the prevalence of anaemia in 367 consecutive patients hospitalized with heart failure or suspected heart failure in two major medical centres in the Haifa area. The patients represented a typical heart failure population: age ranged from 37 to 98 years (Table 1), 57% were males, 29% had diabetes mellitus (8% insulin dependent, 21% oral agents), in 61% there was a diagnosis of ß The Author [2005]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please email: [email protected] vii4 B. S. Lewis et al. SUSPECTED CHF 68 (6.2%) NO CHF CHF 727 (66.4%) 300 (27.4%) Fig. 1. High prevalence of heart failure (HF) or suspected HF in consecutive patients hospitalized over two 6 week periods in internal medicine, cardiology and cardiac surgical departments in two major medical centres in Israel. HF or suspected HF was present in 33% of patients. Table 1. Haemoglobin and creatinine values in patients hospitalized for heart failure in Haifa Age (years) LVEF (%) Hb (g/dl) Creatinine (mg/dl) Median First quartile Third quartile Range 78 35 12.4 1.30 71 25 11.0 1.00 86 50 14.0 1.72 37–98 4–70 5.1–17.7 0.1–9.0 red blood cell and plasma volume. Patients with haemodilution tended to do worse than patients with true anaemia, which suggests that volume overload may be an important mechanism contributing to the poor outcome in anaemic congestive heart failure (CHF) patients. A number of other factors contribute to anaemia in patients with heart failure. Iron deficiency is not uncommon following poor nutrition and decreased absorption, with gastrointestinal blood loss in a population of patients almost universally treated with antiplatelet drugs such as aspirin and/or chronic anticoagulation with warfarin. Renal failure is common due to common disease aetiology (diabetes mellitus, systemic hypertension and atherosclerotic vascular disease) or due to unrelated causes. In addition and importantly, the immunomodulator role of tissue necrosis factor and interleukins in heart failure is associated with resistance to erythropoietin at a bone marrow level, with decreased haemoglobin production. Under these circumstances, circulating erythropoietin levels should be very high. Thus, while measured circulating erythropoietin levels may be normal or mildly elevated in heart failure patients, exogenous erythropoietin is effective in raising haemoglobin. Since most heart failure patients are elderly, there may be other unrelated causes for the development of anaemia, and these should be carefully looked for. Ventricular function in heart failure hypertension, and 8.2% had suffered a recent episode of acute myocardial infarction. Systolic left ventricular (LV) function was reduced in most patients. The median LF ejection fraction (EF) was 35%. Haemoglobin values in these heart failure patients ranged from 5.1 to 17.7 g/dl. The median value was 12.4 g/dl, lower quartile <11.0 g/dl, upper quartile >14.0 g/dl (Table 1), meaning that in almost half the patients, haemoglobin was <12.0 g/dl. The findings were similar but slightly worse than those reported in the European Heart Failure Survey [8], where haemoglobin values were <11 g/dl in 18% of men and 23% of women. Renal dysfunction was very common. Mean serum creatinine was 1.6±1.2 (range 0.1–9.0) mg% and the median value 1.3 mg%, implying abnormal renal function in at least half the patients. In the European survey, renal dysfunction was reported to have complicated the management of patients with known or suspected heart failure in 18% of cases [8]. Aetiology of anaemia in heart failure There are many potential reasons for development of anaemia in chronic heart failure, including bone marrow depression, reduced intestinal iron uptake, and dilution as a consequence of sodium and water retention [9]. Androne et al. [10] examined the prevalence of haemodilution in a subset of 37 ambulatory anaemic patients with 131I-tagged albumin to measure The contractile state of the LV may be assessed from the instantaneous relationships between force, velocity and fibre length. The Starling series of curves characterizes the systolic contractile potential of the heart and may be estimated at catheterization or semi-invasively by construction of pressure–volume loops, by the end-systolic pressure–volume relationship or on a more simple daily basis by measurement of LVEF by invasive or non-invasive methodology. The nature of the contraction abnormality depends on the aetiology of the disease. Heart failure due to coronary artery disease is characterized by regional ventricular contraction abnormalities, hypertensive heart failure or valvular disease by global reduction in LV contraction. Diastolic ventricular function may be described in terms of the diastolic pressure–volume curve, itself the result of a number of determinants including inherent LV relaxation properties, the compliance of the ventricle and the extraneous influences of the right ventricle and pericardial system, where the parallel elastic component represents the distensile abilities of the interstitial and other para-myocardial LV structures [11]. Abnormal diastolic function (decreased compliance/increased stiffness) is represented by an upward and leftward shift to the pressure–volume curve. An increased ventricular volume (volume load) shifts the patients upward and to the right along the pressure–volume curve, and in patients with decreased compliance, LV end-diastolic pressure The problem of anaemia in heart failure may indeed rise very sharply since the diastolic compliance curve is exponential. The three major causes of diastolic dysfunction—ischaemia, fibrosis and ventricular hypertrophy—are frequently present in heart failure patients. Effect of anaemia on haemodynamics of the damaged left ventricle Patients with anaemia suffer from volume load of the cardiovascular system, while oxygen carrying capacity is reduced. Heart rate is increased. This means that ventricular volumes are larger, with greater demands on energy expenditure. The increased plasma volume produces eccentric hypertrophy, where ventricular dimensions increase disproportionally to the ability to increase wall thickness. Cardiac mass in anaemic animals increased by as much as 25% [12]. Wall stress increases [13,14]. While systolic cardiac function may be unaltered (or even compensatorily enhanced) in the presence of moderate anaemia and in the absence of underlying heart disease [15,16], systolic function may indeed be considerably reduced in the damaged heart of patients in heart failure or in patients with very severe anaemia. In children with severe iron deficiency anaemia, the ratio of LV end-systolic wall stress to the LV volume index (and cardiac index) decreased when the haemoglobin concentration was 6 g/dl, indicating a decrease in LV contractility and LV dysfunction, and resulted in circulatory congestion [17]. After iron repletion, LV function was shown to improve before the rise in haemoglobin level, suggesting that correction of functional abnormalities may also be the result of correction of iron metabolism at the tissue level [18]. In diastole, the increased volume is associated with further deterioration regarding filling pressures in the presence of an already compromised end-diastolic pressure–volume relationship (Figure 2). Relationship between anaemia and clinical outcome The severity of anaemia is an independent predictor of outcome [19–21]. A lower baseline haemoglobin value was associated with increased risk of short-term adverse clinical events [22]. In population studies, the cause of anaemia has not always been well defined. This is potentially important because iron deficiency anaemia may alter endothelial function [23]. In contrast to studies in established chronic heart failure, the haemoglobin level in new cases of heart failure was not always independently associated with prognosis when age and serum creatinine concentration were included in the analysis [24]. The adverse effects of anaemia on survival might be a consequence of chronic heart failure rather than a separate process causing disease progression. In a large series of 12 065 patients with new-onset heart failure studied in Canada [25], anaemia vii5 Anemia LVEDP Fig. 2. Ventricular pressure–volume loops in health (control loop), in patients with decreased compliance (filled loop) and in patients with anaemia (dotted line). Anaemia is associated with volume load and shift of the loop to the right. Systolic function may be preserved (as shown) or reduced if anaemia decreases systolic contraction. Left ventricular end-diastolic pressure (LVEDP) is increased following the exponential nature of the diastolic pressure–volume curve. was common and an independent prognostic factor for mortality. In our series of hospitalized heart failure patients in Haifa, 12 month mortality/repeat hospitalization was more frequent in patients with haemoglobin <11 g/dl (lowest quartile vs all others) (51 vs 41%, P ¼ 0.07), while 12 month mortality was marginally but not significantly higher (36 vs 27%, P ¼ 0.12). The very high 36% 12 month mortality and 51% mortality/ cardiac rehospitalization rates were staggering and imposed a heavy burden on health care resources. Similar data were reported by Kosiborod et al. [26], who found that after adjusting for demographic and clinical factors, each 1% reduction in haematocrit was associated with a 2% greater 1-year mortality. Effect of treatment and role of erythropoetin in heart failure patients At a clinical level, anaemia has an important effect on exercise tolerance in chronic heart failure [27]. Mancini et al. [28] showed that in a placebo-controlled study, administration of erythropoetin was associated with a significant increase in haemoglobin, peak VO2 and exercise duration. Resting and hyperaemic forearm vascular resistance and indices of the rate of muscle oxidative capacity were unchanged in both groups, suggesting that erythropoietin enhances exercise capacity by increased oxygen delivery from increased haemoglobin concentration. In addition, erythropoietin has potentially beneficial effects on the endothelium, including anti-apoptotic and pro-angiogenic activities [29]. Erythropoetin may be associated with an increase in circulating endothelial progenitor cells [30,31], and these are currently the subject of extensive investigation as potentially therapeutic targets in patients with acute and chronic myocardial ischaemia and/or damage. Reports that erythropoietin may have pro-thrombotic or platelet-activating effects, or produce hypertension appear to be less important clinically in light of vii6 preliminary clinical trials [3,4] based on administration of erythropoietin and iron therapy in heart failure patients. Implications for treatment and management The high prevalence of anaemia in heart failure patients presents both a new challenge and a new therapeutic opportunity in the management of patients with heart failure. Treatment of anaemia, using a judicious combination of iron and erythropoetin therapy, improves ventricular function and clinical status in patients with chronic renal failure. It now appears that the same is true in patients with heart failure, many of whom suffer from additional renal impairment. The inter-relationships between heart failure, anaemia and renal insufficiency are currently the subject of intense research activity [6] and is also the theme of this Supplement. We await the results of new trials to define the advantage to be gained in terms of mortality, morbidity and cost savings [32] by treating anaemia in heart failure patients. Conflict of interest statement. None declared. References 1. Swedberg K, Kjekshus J. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). Am J Cardiol 1988; 62: 60A–66A 2. The MERIT-HF Investigators. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353: 2001–2007 3. Silverberg DS, Wexler D, Blum M et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol 2000; 35: 1737–1744 4. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001; 37: 1775–1780 5. Silverberg DS, Wexler D, Iaina A. The importance of anemia and its correction in the management of severe congestive heart failure. Eur J Heart Fail 2002; 4: 681–686 6. Silverberg D, Wexler D, Blum M et al. The cardio-renal anaemia syndrome: does it exist? Nephrol Dial Transplant 2003; 18 [Suppl 8]: VIII7–VIII12 7. Silverberg DS, Wexler D, Blum M et al. Erythropoietin should be part of congestive heart failure management. Kidney Int Suppl 2003; 64: S40–S47 8. Cleland JG, Swedberg K, Follath F et al. The EuroHeart Failure survey programme—a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J 2003; 24: 442–463 9. Steinborn W, Doehner W, Anker SD. Anemia in chronic heart failure—frequency and prognostic impact. Clin Nephrol 2003; 60 [Suppl 1]: S103–S107 10. Androne AS, Katz SD, Lund L et al. Hemodilution is common in patients with advanced heart failure. Circulation 2003; 107: 226–229 B. S. Lewis et al. 11. Lewis BS, Gotsman MS. Current concepts of left ventricular relaxation and compliance. Am Heart J 1980; 99: 101–112 12. Rakusan K, Cicutti N, Kolar F. Effect of anemia on cardiac function, microvascular structure, and capillary hematocrit in rat hearts. Am J Physiol 2001; 280: H1407–H1414 13. Gaasch WH. Left ventricular radius to wall thickness ratio. Am J Cardiol 1979; 43: 1189–1194 14. Frohlich ED, Apstein C, Chobanian AV et al. The heart in hypertension. N Engl J Med 1992; 327: 998–1008 15. Singh PI, Verma K, Sood S. Noninvasive evaluation of left ventricular function in chronic severe anemia. Jpn Heart J 1989; 30: 129–136 16. Bahl VK, Malhotra OP, Kumar D et al. Noninvasive assessment of systolic and diastolic left ventricular function in patients with chronic severe anemia: a combined M-mode, two-dimensional, and Doppler echocardiographic study. Am Heart J 1992; 124: 1516–1523 17. Hayashi R, Ogawa S, Watanabe Z et al. Cardiovascular function before and after iron therapy by echocardiography in patients with iron deficiency anemia. Pediatr Int 1999; 41: 13–17 18. Alvares JF, Oak JL, Pathare AV. Evaluation of cardiac function in iron deficiency anemia before and after total dose iron therapy. J Assoc Physicians India 2000; 48: 204–206 19. Horwich TB, Fonarow GC, Hamilton MA et al. Anemia is associated with worse symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol 2002; 39: 1780–1786 20. Szachniewicz J, Petruk-Kowalczyk J, Majda J et al. Anaemia is an independent predictor of poor outcome in patients with chronic heart failure. Int J Cardiol 2003; 90: 303–308 21. Mozaffarian D, Nye R, Levy WC. Anemia predicts mortality in severe heart failure: the prospective randomized amlodipine survival evaluation (PRAISE). J Am Coll Cardiol 2003; 41: 1933–1939 22. Felker GM, Gattis WA, Leimberger JD et al. Usefulness of anemia as a predictor of death and rehospitalization in patients with decompensated heart failure. Am J Cardiol 2003; 92: 625–628 23. Pereira AA, Sarnak MJ. Anemia as a risk factor for cardiovascular disease. Kidney Int Suppl 2003; 64: S32–S39 24. Kalra PR, Collier T, Cowie MR et al. Haemoglobin concentration and prognosis in new cases of heart failure. Lancet 2003; 362: 211–212 25. Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12 065 patients with new-onset heart failure. Circulation 2003; 107: 223–225 26. Kosiborod M, Smith GL, Radford MJ et al. The prognostic importance of anemia in patients with heart failure. Am J Med 2003; 114: 112–119 27. Kalra PR, Bolger AP, Francis DP et al. Effect of anemia on exercise tolerance in chronic heart failure in men. Am J Cardiol 2003; 91: 888–891 28. Mancini DM, Katz SD, Lang CC et al. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation 2003; 107: 294–299 29. Smith KJ, Bleyer AJ, Little WC et al. The cardiovascular effects of erythropoietin. Cardiovasc Res 2003; 59: 538–548 30. Bahlmann FH, DeGroot K, Duckert T et al. Endothelial progenitor cell proliferation and differentiation is regulated by erythropoietin. Kidney Int 2003; 64: 1648–1652 31. Bahlmann FH, De Groot K, Spandau JM et al. Erythropoietin regulates endothelial progenitor cells. Blood 2004; 103: 921–926 32. Gregory DD, Sarnak MJ, Konstam MA et al. Impact of chronic kidney disease and anemia on hospitalization expense in patients with left ventricular dysfunction. Am J Cardiol 2003; 92: 1300–1305