Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
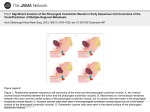
1 Head and Neck Mesenchyme of the head region is derived from paraxial and lateral plate mesoderm, and neural crest. Thickened regions of ectoderm are known as ectodermal placodes. Paraxial mesoderm (somites and somitomeres) forms the floor of the brain case and a small portion of the occipital region. A distinctive feature of the developing head and neck are the pharyngeal or branchial arches. Externally, each arch is partially separated by a pharyngeal (branchial) cleft or groove. Internally and opposite the clefts, each arch is defined by a pharyngeal pouch. At the end of the 4th week the center of the face has a stomodeum that is surrounded by the 1st arch. At 4 ½ weeks five prominences can be seen around the stomodeum. Above the stomodeum is one frontonasal prominence: lateral to the stomodeum are paired maxillary prominences, and a pair of mandibular prominences below the stomodeum. Later, nasal prominences will form above the stomodeum and just medial to the maxillary prominences to form the nose and part of the hard palate of the mouth. PHARYNGEAL ARCHES Each pharyngeal arch has a core of mesenchymal tissue. The core of each arch receives neural crest cells that migrate into the arches to contribute to the skeletal and connective tissue components for each arch. Neural crest-derived connective tissue components in the face include dermis and fat of the skin, cornea of the eye, odontoblasts, and stroma of glands. Mesoderm in the core of each arch will help form connective tissue, bone, and vascular components. Specifically, paraxial mesoderm (from somites or somitomeres) gives rise to skeletal face and neck muscles, as it does in virtually all of the body. As a result, each arch has its own cranial nerve, muscle, vascular (aortic arch), and connective tissue composition. It should be remembered that as the 5th aortic arch and 5th pharyngeal arch disappeared. First Pharyngeal Arch The maxillary process is the dorsal portion of the 1st pharyngeal arch. The mandibular process is a ventral portion of the 1st pharyngeal arch and it contains Meckel's cartilage. Meckel's cartilage disappears except for sphenomandibular ligament, the incus and malleus. Mesenchyme of the maxillary process creates the premaxilla (the part of the upper palate with the four incisors), maxillary, zygomatic, and part of the temporal bones. These bones and the mandible are formed by intramembranous ossification. Mesenchyme of the 1st arch, also contributes the dermis of the face Muscles of the 1st pharyngeal arch are muscle of mastication (temporalis, masseter, and pterygoids), anterior belly of the digastric, mylohyoid, tensor tympani, and tensor veli palatini. Hence, the motor nerve supply to the muscles of mastication is through the mandibular branch of the trigeminal nerve. The sensory supply to the face is via the three branches of the trigeminal nerve, ophthalmic, maxillary, and mandibular. Second Pharyngeal Arch Cartilages of the 2nd arch (hyoid or Reichert's cartilage) gives rise to the stapes, styloid process (temporal bone), stylohyoid ligament, and two parts of the hyoid bone (its lesser 2 horn and upper part of the body). Muscles of the hyoid arch are the stapedius, stylohyoid, posterior belly of the digastric, auricular, and muscles of facial expression. The facial nerve innervates these muscles; therefore, it is the nerve of the 2nd pharyngeal arch. Third Pharyngeal Arch The cartilage of the 3rd pharyngeal arch produces two other parts of the hyoid bone (the lower part of its body and its greater horns). Here, the musculature is only the stylopharyngeus muscle. Nerve of the 3rd arch is the glossopharyngeal nerve. Fourth and Sixth Arches Cartilagenous components of the 4th and 6th arches fuse to form the thyroid, cricoid, arytenoid, corniculate, and cuneiform cartilages of the larynx. Muscles of the 4th arch are the cricothyroid, levator veli palatini, and pharyngeal constrictors. These muscles are innervated by the nerve of the 4th arch, the superior laryngeal nerve. The intrinsic muscles of the larynx are supplied by the nerve of the 6th arch, the recurrent laryngeal nerve (from the vagus nerve). ARCH MUSCLES First temporalis, masseter, med. & Trigeminal lat. pterygoids, ant. belly root) digastric, mylohyoid, tensor tympani, tensor palatini muscles of facial expression, Facial post. belly digastric, stapedius, stylohyoid Second Third stylopharyngeus Fourth & Sixth most muscles of larynx, pharynx, soft palate BONES, LIGS., CARTILAGES NERVE (motor Glossopharyngeal Cranial X (XI via X) (Meckel's Cart.) malleus, incus, sphenomandibular ligament (Reichert's Cart.) stapes, styloid process, stylohyo id ligament, upper part and lesser horn of the hyoid. Lower part of hyoid and greater horn laryngeal cartilages PHARYNGEAL POUCHES There are five pharyngeal pouches in the human. They are internal and between the arches and are lined with epithelium of endodermal origin. The last pouch is considered as part of the 4th. 3 First Pharyngeal Pouch The 1st pharyngeal pouch forms the tubotympanic recess, which will come in contact with the 1st pharyngeal cleft (future external auditory meatus) directly opposite the pouch externally. The distal part of the 1st pouch will both form and line (with endodermal epithelium) the middle ear cavity and its proximal part, the auditory (Eustachian) tube. The 1st pouch lines the inner part of the tympanic membrane. Second Pharyngeal Pouch The 2nd pharyngeal pouch forms buds that enter the adjacent mesenchyme. The buds and the mesoderm form the primordium of the palatine tonsil that is later infiltrated with lymphatic tissue. The 2nd pharyngeal pouch remains as the palatine fossa in the adult. Third Pharyngeal Pouch In the fifth week, the 3rd pharyngeal pouch will develop structures from two of its parts. The epithelium of its dorsal part will form the inferior parathyroid gland. Its ventral part will develop into the thymus. Unlike the 1st and 2nd pharyngeal pouches, which maintain connection with the pharynx, the 3rd pouch loses its connection with the pharynx. The thymus and inferior parathyroid gland migrate caudally. The thymus will come to rest in the anterior thorax, and the inferior parathyroid gland will lie on the dorsal side of the thyroid gland. Fourth Pharyngeal Pouch Epithelium of the dorsal part of the 4th pharyngeal pouch forms the superior parathyroid gland. It, also, loses contact with the pharynx and comes to rest behind the thyroid gland. Parathyroid hormone elevates serum calcium levels. Fifth Pharyngeal Pouch The 5th pharyngeal pouch is considered part of the 4th pouch. It forms the ultimobranchial body, which will make the parafollicular cells, or C cells of the thyroid gland. C cells will produce calcitonin, which reduces serum calcium levels. PHARYNGEAL CLEFTS The 5-week old embryo has four pharyngeal clefts, which are external and covered with ectodermal epithelium. Only one contributes to a definitive structure and that is the external auditory meatus. The associated epithelium covers the external eardrum. The 2nd through 4th pharyngeal clefts merge and lose contact with the outside surface. These form a cervical sinus that disappears, normally. Birth Defects of the Pharyngeal Region Ectopic Thymic and Parathyroid tissue Some migrating tissues in the pouches may, while traveling to their final destinations, persist in the neck. Branchial Fistulas 4 Branchial fistulas occur when the 2nd pharyngeal arch fails to grow over the 3rd and 4th arches. When this occurs, the corresponding clefts remain continuous with the surface epithelium through a fistula. Such fistulas are found on the lateral aspect of the neck, directly anterior to the sternocleidomastoid muscle. These lateral cervical cysts are usually not evident at birth, but enlarge during childhood and may drain. Neural Crest Cells and Craniofacial Defects Neural crest cells are essential for formation of much of the craniofacial region and their disruption results in severe craniofacial malformations. Crest cells also contribute to the conotruncal endocardial cushions, which form the aorta and pulmonary artery from the truncus arteriosus. Hence, many infants with craniofacial defects have cardiac abnormalities. Abnormalities include persistent truncus arteriosus, tetralogy of Fallot, and transposition of the great vessels. Crest cells are particularly vulnerable to the harmful effects of retinoic acid. Examples of defects due to crest cell errors are the following: Treacher Collins syndrome – (mandibular dysostosis) - This is characterized by malar hypoplasia due to underdevelopment of the zygomatic bones, mandibular hypoplasia, down-slanting palpebral fissures, lower eyelid colobomas, and malformed ears. It is autosomal dominant with 60% arising from new mutations. Robin sequence – Like Treacher Collins syndrome, there are defects of the 1st arch. The primary defect is includes poor growth of the mandible resulting in a posteriorly displaced tongue. It occurs in 1/8500 births. DiGeorge anomaly – This occurs in about 1/2500 births. It includes a collection of severe disorders that includes velocardiofacial syndrome (VCFS) and conotruncal anomalies face syndrome. Velocardiofacial syndrome (VCFS) is a complex syndrome generally involving palatal defects, heart defects, learning disabilities and distinct facial features. It has been associated with over thirty different characteristics. The name comes from Latin: "velum" meaning palate, "cardia" meaning heart and "facies" meaning face. Patients with complete DiGeorge anomaly have immunologic deficiencies and hypocalcemia. TONGUE In the fourth week, the tongue emerges as two lateral swellings and one medial swelling (tuberculum impar): all three are part of the 1st pharyngeal arch. A second median swelling, the copula (hypobranchial eminence), is formed by mesoderm of the 2nd, 3rd, and 4th arch. Also, as part of the 4th arch, a final third median swelling will form the epiglottis. Immediately behind this third swelling is the laryngeal orifice, bordered by the arytenoid swellings. The lateral swellings overgrow the tuberculum impar and merge, thus forming the anterior two-thirds or body of the tongue. Here, the mucosa has sensory innervation by the mandibular branch of the trigeminal nerve (the 1st arch nerve). Behind the body of the tongue is the V-shaped sulcus terminalis, which separates it from the posterior one-third of the tongue. 5 The posterior or root of the tongue originates from the 2nd, 3rd, and 4th arches. Here, sensory innervation is supplied by the glossopharyngeal nerve: the 3rd arch tissue overgrows the 2nd arch (facial nerve). The epiglottis and adjacent mucosa are innervated by the superior laryngeal nerve (4th arch / vagus nerve). Tongue muscle are derived from occipital somites, therefore, motor innervation is via the hypoglossal nerve. Special sensory innervation (taste) to the anterior two-thirds of the tongue is provided by the chorda tympani branch of the facial nerve. Taste to the posterior one-third of the tongue is through the glossopharyngeal nerve. Defects of the Tongue Tongue-tie (ankyloglossia) – Here, the tongue is no freed from the floor of the mouth. Most, cases involve the frenulum extending to the tip of the tongue. THYROID GLAND The thyroid gland appears as an epithelial growth in the floor of the pharynx, between the tuberculum impar and the copula. This spot is at the foramen cecum and the thyroid gland will descend from this location to just below the thyroid cartilage. During its migration, the thyroid remains connected to the tongue by the thyroglossal duct. When it has reached its final position in front of the trachea it acquires an isthmus, which connects the two lobes of the thyroid. The thyroid begins to function about the end of the third month. Follicular cells produce the colloid that serves as the source of thyroxine (T4) and triiodothyronine (T3). Parafollicular cells (C cells) derived from the ultimobranchial body (5th pouch), serve as the source of calcitonin. Thyroid Duct and Thyroid Abnormalities Thyroglossal cyst – A thyroglossal duct may leave a cyst anywhere along the midline of the neck. About half are near the hyoid bone, and the rest, anywhere from the base of the tongue to the thyroid gland. Sometimes the cyst communicates with the outside to form a thyroglossal fistula. Cretinism - A congenital deficiency of thyroid hormone. Mental and growth retardation. FACE At the end of the fourth week, facial prominences (mostly of neural crest mesenchyme) are formed in the 1st pair of pharyngeal arches. Lateral to the stomodeum are the maxillary prominences. Mandibular prominences are caudal to the stomodeum. The frontonasal prominence is above the stomodeum. On both sides of the frontonasal prominence is thickened ectoderm, the nasal (olfactory) placodes. The placodes originate under the influence of the forebrain and form the first cranial nerves (olfactory nerve). In the fifth week, the nasal placodes invaginate to form nasal pits. Around each nasal pit, two prominences form: the lateral nasal prominence and the medial nasal prominence. 6 During sixth and seventh weeks, the maxillary prominences increase in size and compress the medial nasal prominences together at the midline. As the maxillary and medial nasal prominences fuse, the cleft between them disappears. Hence, the upper lip is formed by the two medial nasal prominences and the two maxillary prominences. The lower lip and jaw is formed by the merged mandibular prominences. Initially, the maxillary and lateral nasal prominences are separated by a deep trough, the nasolacrimal groove. The ectoderm of the nasolacrimal groove separates from the surface ectoderm and forms the nasolacrimal duct, with its upper portion forming the lacrimal sac. The nasolacrimal duct drains into the inferior meatus of the nasal cavity. The maxillary prominences form the zygomatic (malar or cheek bone) and maxillary bones and part of the temporal bones. The nose is formed from the five facial prominences. The frontal prominence forms the bridge, the merged medial nasal prominences form its crest and tip, and the lateral nasal prominences make the alae. INTERMAXILLARY SEGMENT (PREMAXILLA) As the medial nasal prominences merge to form the mid-portion of the upper lip plus the tip of the nose, they also merge at a deeper level. The structure formed by the two merged medial nasal prominences is the intermaxillary segment. Its constitution is: (1) a labial component, (2) an upper jaw component, and (3) a triangular primary palate. The intermaxillary segment is continuous with the rostral portion of the nasal septum. SECONDARY PALATE Although the primary palate is derived from the intermaxillary segment, the main part of the definitive palate is formed by two shelf-like outgrowths of the maxillary prominences. These palatine shelves appear in the sixth week, and attain a horizontal position above the tongue and fuse to form the secondary palate in the seventh week. Anteriorly, the shelves fuse with the triangular primary palate. The incisive foramen forms where the two shelves merge with the posteriorly directed apex of the primary palate. Facial Clefts Cleft Lip and Palate Cleft lip and cleft palate are relatively common malformations, with an incidence of 1 in 1000 and 1 in 2500 births, respectively. Structurally, cleft lip results from the lack of fusion of the maxillary and nasomedial processes. In the most common form of the defect, the entire premaxillary segment is separated from both maxillae. This results in bilateral clefts running through the lip and upper jaw between the lateral incisors and the canine teeth. Usually, the cause is hypoplasia of the maxillary process. Cleft palate results from incomplete or absent fusion of the palatal shelves. The problem may be major: (1) the entire palatal shelf may be cleft, or it may be minor (2) a bifid uvula. As with the cleft lip, cleft palate is usually multifactorial. Some chromosomal syndromes (trisomy 13) have a high incidence of cleft palate. Other cases may involve chemical teratogens (e. g., anticonvulsive drugs). The higher incidence of cleft palate in 7 females may be related to the palatal shelves in females fusing about a week later than they do in males, thus prolonging the susceptible period. Oblique Facial Cleft This rare defect results when the nasolateral process fails to fuse with the maxillary process. It manifests itself as an epithelially lined fissure running from the upper lip to the inner canthus of the eye. Median Cleft Lip This is from failure of the nasomedial processes to fuse: also rare. Holoprosencephaly Holoprosencephaly includes a broad spectrum of defect, all based on defective formation of the prosencephalon (forebrain) and structures whose normal formation depends on influences of the prosencephalon. Primary defects of the forebrain often manifest externally as facial malformations, typically as a reduction in tissue of the frontonasal process. In extreme cases, holoprosencephaly can take the form of cyclopia. In the near absence of upper and midfacial tissue, there is a convergence and fusion of optic primordia. The nose can be either absent or look like tubular proboscis, sometimes located above the eye. Frontonasal Dysplasia Frontonasal dysplasia includes various nasal malformations that result from excess tissue in the frontonasal process. This spectrum of anomalies usually includes a broad nasal bridge and hypertelorism (an excess distance between the eyes). NASAL CAVITIES At first, the oronasal membrane separates the nasal pits from the primitive oral cavity by way of primitive choanae. The choanae are on either side of the midline and behind the primary palate. The definitive choanae are formed when the secondary palate forms and fuses behind the primary palate. The choanae are communications between the posterior nasal cavities and the nasopharynx. Paranasal air sinuses develop as diverticula of the lateral nasal wall and extend into the maxilla, ethmoid, frontal, and sphenoid bones. TEETH Tooth development begins with the migration of neural crest cells into the regions of the upper and lower jaws. The overlying ectoderm then thickens into C – shaped bands called dental laminae. The dental laminae grow into the neural crest mesenchyme and primordial teeth begin to take shape as tooth buds. Tooth buds consist of an outer layer of dental lamina and an inner layer of dental epithelium. The tooth bud soon expands, passing through a mushroom-shaped cap stage before entering the bell stage. Mesenchyme that originates from the neural crest is inside the dome of the bell and forms the dental papilla. 8 The dental (stomodeal) epithelium component of the tooth bud gives rise to the enamel organ. Cells in the enamel organ, called ameloblasts, begin to secrete enamel. Adjacent and internal to the ameloblasts, cells of the dental papilla (neural crest) form odontoblasts that secrete dentin. Dentin that is above the gum line is called the crown, which is coated with enamel. Below the gum line dentin forms the root. Mesenchymal cells on the outside of the root differentiate into cementoblasts, which produce cementum. Outside the cementum a periodontal ligament forms, holding the tooth in its socket. There are a total of 20 deciduous teeth (milk teeth) that erupt in a certain sequence at 6 to 24 months after birth. These fall from the jaws and are replaced with an additional 12 teeth, making a total of 32 permanent teeth. Questions 1. The frontonasal, mandibular, and maxillary prominences form around the_________. a. cloaca b. stomodeum c. umbilical ring d. nasal placodes 2. Which of the following does not contribute to formation of the face? a. splanchnic mesoderm b. neural crest c. paraxial mesoderm d. ectoderm 3. Which of the following is a derivative of the 1st pharyngeal arch? a. stylohyoid ligament b. eustachian tube c. sphenomandibular ligament d. stapes 4. Which of the following is a derivative of the 1st pharyngeal cleft? a. Meckel's cartilage b. eustachian tube c. malleus d. external auditory meatus 5. The 1st pharyngeal pouch will give rise to the _____________. a. superior part of the body of the hyoid bone b. middle ear cavity c. external auditory meatus d. palatine fossa 6. The 2nd pharyngeal arch can form the ______________. a. superior part of the hyoid body and its lesser cornua 9 b. mandible c. anterior belly of the digastric muscle d. incus 7. The second pharyngeal cleft helps form the ____________. a. cervical sinus b. palatine fossa c. stylohyoid ligament d. muscle of mastication 8. The nerves that are associated with the 1st and 2nd arches are the __________, respectively. a. trigeminal / vagus b. trigeminal / facial c. facial / vagus d. vagus / trigeminal 9. The 3rd pharyngeal arch is associated the ________ nerve. a. trigeminal b. facial c. glossopharyngeal d. vagus 10. The thymus and inferior parathyroid glands are derivatives of ______________. a. 3rd pharyngeal cleft b. 4th pharyngeal pouch c. 3rd pharyngeal pouch d. 4th pharyngeal cleft 11. The superior parathyroid glands are derivatives of the _____________. a. 3rd pharyngeal cleft b. 4th pharyngeal pouch c. 3rd pharyngeal pouch d. 4th pharyngeal cleft 12. The ultimobranchial body is the ______ pouch and it gives rise to C cells that will _________ serum calcium. a. 4th / elevate b. 5th / elevate c. 4th / decease d. 5th / decrease 13. The 4th and 6th arches are related to the ________ and ________ nerves, respectively. a. glossopharyngeal / superior laryngeal b. superior laryngeal / recurrent laryngeal 1 0 c. recurrent laryngeal / glossopharyngeal d. recurrent laryngeal / superior laryngeal 14. Failure of neural crest migration can result in facial malformations and __________. a. ankyloglossia b. cervical cyst c. ectopic thymic and parathyroid tissue d. persistent truncus arteriosus 15. Early tongue development has a median swelling of the 1st pharyngeal arch called which of the following? a. copula b. foramen cecum c. sulcus d. tuberculum impar 16. The thyroid gland begins its descent from the _______, in the tongue, and terminates anterior to the trachea below the thyroid cartilage. Be specific! a. tuberculum impar b. foramen cecum c. sulcus terminalis d. incisive foramen 17. The upper lip is formed by the mergence and fusion of the _________ and __________ prominences. a. medial nasal / maxillary b. lateral nasal / maxillary c. medial nasal / frontonasal d. lateral nasal / frontonasal 18. The nasolacrimal ducts are formed by mergence and fusion of the _________ and __________ prominences. a. medial nasal / maxillary b. lateral nasal / maxillary c. medial nasal / frontonasal d. lateral nasal / frontonasal 19. The alae of the nose are formed by the _____________. a. nasal pits b. medial nasal prominences c. lateral nasal prominences d. frontonasal prominence 20. The premaxilla or intermaxillary segment is formed by the ________ prominences. 1 1 a. b. c. d. maxillary medial nasal frontonasal lateral nasal 21. Cleft lip is due to failure of the _______________ to fuse. a. nasolateral and maxillary processes b. palatine shelves c. nasomedial and maxillary processes d. nasal placodes 22. A defect in forebrain development can lead to concurrent problems with facial development called ___________. a. cleft palate b. holoprosencephaly c. tetralogy of Fallot d. DiGeorge's syndrome 23. Neural crest cells give rise to ______________ which make _________. a. ameloblasts / enamel b. ameloblasts / dentin c. odontoblasts / enamel d. odontoblasts / dentin