Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Rheumatic fever wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
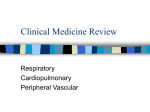
Cardiopulmonary History and Exam Wendy Blount, DVM Nacogdoches TX Housekeeping • All Handouts Including the PowerPoints are on you Flash Drive Proceedings – Or in your Printed Proceedings if you chose to purchase • Course materials are also downloadable at http://wendyblount.com Housekeeping • All Handouts Including the PowerPoints are on you Flash Drive Proceedings – Or in your Printed Proceedings if you chose to purchase • Course materials are also downloadable at http://wendyblount.com Housekeeping • All Handouts Including the PowerPoints are on you Flash Drive Proceedings – Or in your Printed Proceedings if you chose to purchase • Course materials are also downloadable at http://wendyblount.com Housekeeping • All Handouts Including the PowerPoints are on you Flash Drive Proceedings – Or in your Printed Proceedings if you chose to purchase • Course materials are also downloadable at http://wendyblount.com Housekeeping • Proceedings – TOC, Abbreviations, Evaluation – Put each PowerPoint handout behind the colored tab for that section and in front of the first blue subdivider – Then you will find client handouts, diagnostic and treatment aids, lab submission forms, etc. • CE certificates & evaluations in your notebook/packet – I will time and date my signature – Check off hours attended on the back, sign and date – Please complete the evaluation & turn it in when you get your certificate signed Housekeeping • • • • • • • • • Breakfast, coffee and registration 7:30-8am Morning Session 8am-12noon We’ll break the last 10 minutes of every hour Lunch break 12-12:30pm Afternoon Session 12:30-5pm Sat - Oncura Presentation 12:30-1:30pm PLEASE PARTICIPATE!! But take private conversations out in the hall Gold brads in bowls on the table to recycle Practical Medicine Philosophy • As referral medicine becomes more advanced, it by default becomes more expensive • Growing gap between general practice and specialty practices • These seminars help us fill those gaps • Everything we talk about this weekend can be done in a rural mixed animal practice • We will look at lots of x-rays, ultrasound images and videos, EKGs and listen to heart and lung sounds Practical Medicine Philosophy • Some are already doing these things – Echocardiogram, reading ECGs, defibrillating • Some will be ready to begin • Some will need some hand holding, at least at first – TexasVets – Yahoogroups – Moderator Rosemary Lindsey [email protected] – Oncura • Some will be happy to be better referring vets Agenda Saturday – 8am-12noon, 12:30-5pm • Cardiovascular History and Exam • ECG • Thoracic Radiographs • Cardio Lab work • Cases • (Sign CE Certificates) Agenda Sunday – 8am-12noon, 12:30-5pm • Update on CPR • Infectious Disease (cases) • Congenital & Valvular Disease (cases) • Heartworms in Dogs and Cats • Pericardial Disease, Hypertension (cases) • Neoplasia & Arrhythmias (cases) • Sign CE Certificates Signalment Age • Congenital disease – young • Myxomatous Valvular Disease – old • Exceptions – Cavalier King Charles Spaniels – mild PDA, PS, SAS – Reverse PDA Signalment Breed • Boston Terrier • Cavalier • Cocker Spaniel • Boxer • Doberman • English Bulldog • Golden Retriever HBT, ColTr CVD DCM, PS, PDA, 3rdAV HBT, PS, SAS DCM, Boxer CM, ASD DCM (Arrhythmia?) SAS, PS, CVD SAS Signalment Breed • Great Dane • GSD • Irish Setter • Irish Wolfhound • Keeshond • Labrador • Maine Coon • Newfoundland DCM, CVD PRAA, SAS, PDA PRAA DCM ToF (define), MVD TVD HCM DCM, SAS Signalment Breed • Persian/Himalayan • Pointer • Poodle • St Bernard • Samoyed • Schnauzer • Springer Spaniel • Yorkie HCM PRAA, SAS CVD, PDA, CB DCM ASD, PS SSS, CVD, PS, CB VSD CVD, CB, CT History - Collapse How can you tell the difference between seizure and syncope? – Urination/defecation/vocalization/paddling – Stiff/opisthotonus or flaccid • narcolepsy – Twitching and muscle fasciculations – Cyanosis, pallor – Abnormal behavior before and after – Duration of stiffness/opisthotonus Many times, you can’t (especially when short) History - Collapse What causes syncope? – Bradyarrhythmia • 3rd degree heart block • Sick sinus syndrome (define) (define) – Period of asystole • Sick sinus syndrome • Vagal surge (examples) – Abdominal dz & retching – Intubation (brachycephalic) History - Collapse What causes syncope? – Tachyarrhythmia burst • Vtach (define, causes) – BCM – Myocarditis (Chagas, Parvovirus) – Myocardial hypoxia – Abdominal pathology (spleen) • Supraventricular tachycardia (SVT) (define) • Re-entry pathway (define) • Atrial fibrillation (Afib) • SSS History - Collapse What causes syncope? – Obstruction of a great vessel or heart chamber • Thrombus • Neoplasia • Extramural mass – Increased oxygen demand can not be met due to severe cardiovascular or pulmonary disease • AKA Exercise intolerance History - Cough How can you tell the difference between cardiac and respiratory cough/dyspnea? – Honking cough, soft moist cough, dry hacking cough – Coughing/gagging up white foamy fluid, acting like something caught in the throat – Coughing up blood tinged fluid – Cough when drinking water, on tracheal palpation, or exercise induced cough – Presence of a murmur (big dog, little dog, cat) Many times, you can’t without PE/diagnostics History - Cough Cough on tracheal palpation – Any dog or cat will cough a few times on vigorous tracheal palpation – Prolonged coughing after tracheal palpation often indicates pathology (cardio or resp?) • equally likely with airway disease and cardiovascular disease History - Cough Dogs vs Cats – Coughing cats • much more likely to have respiratory disease than heart failure • Cats with heart failure more often present with acute and severe dyspnea, with no cough • Some cat owners can find it difficult to distinguish vomiting from coughing – Coughing dogs can have either or both Exam – Stethoscopes • • • • Ear pieces fit snugly in the ears Angle fits your ear canals Poor fit, and you’ll miss low intensity murmurs Tubing longer than 18 inches will dampen sounds Electronic stethoscopes (microphone based) • Difficult to distinguish heart from lung sounds • Difficult to distinguish patient from background noise • Meditron sensor based scope eliminates problems – Connect to computer & record for PCG consult Exam – Stethoscopes Pediatric stethoscope • For cats and small dogs • Will distort and decrease sound intensity if used on a medium or large dog Adult stethoscope • For medium to large dogs • Won’t localize murmurs properly in cats and small dogs Exam – Stethoscopes Diaphragm • Filters out low frequency sounds to hear high frequency sounds better • Press firmly against the chest Bell • For low frequency sounds (S3 S4 in dogs) • Press gently against the chest Auscultation Minimizing patient noise • Panting, whining – close mouth, occlude nostrils • Purring – – – – Aversives – turn water on, show another animal Gentle pressure on the larynx Cotton ball with alcohol to the nose Jiggle the doorknob • Sometimes sedation is needed (chart) – Acepromazine 0.0125-0.025 mg/lb, maximum 1 mg per dog – Butorphanol 0.1 mg/lb or buprenorphine 0.01-0.02 mg/kg – IV the fastest and most profound (30-45 minutes) Auscultation • Patient is standing in a quiet place – R Lateral recumbency and listen from bottom if muffled • Firm pressure with the diaphragm to avoid hair noises • get comfortable ausculting heart and palpating pulses at the same time • Listen for at least 2 minutes – Heart - R and L apex, L bases – L armpit – Lungs – RCr, RMidVentral, RDCd, LCr, LMidVentral, LDCd Auscultation • Is the murmur hemodynamically significant? – – – – Prolonged and loud - yes pansystolic - yes Diastolic - yes Low intensity, early systolic – maybe not so much Loudness is not necessarily correlated to presence of heart failure Auscultation – Lung Sounds • Snaps crackles and wheezes (cardio or resp?) – More likely respiratory in dogs (audio) – Not very sensitive for pulmonary edema – Beware similar hair rubbing noises • Pleural/pericardial Rubs (pleural rubs) (pericardial rubs) • Dull/absent lung sounds (dog vs cat) (causes) – Lung consolidation – Pneumothorax, pleural effusion • Harsh lung sounds with no murmur in cat – think asthma or heartworm disease (audio) Auscultation - Heart Sounds Normal Heart Sounds Auscultation - Heart Sounds Normal Heart Sounds • S1 – AV Valves close – Beginning of systole • S2 – Semilunar valves close – beginning of diastole • Tachycardia – which is which? – S2 shorter and higher frequency • Pulse is during systole (audio) Auscultation - Heart Sounds • Variable intensity S1 – arrhythmia • Louder S1 (AV slamming) – – – – – – Young, narrow chested dogs (Doberman) Increased sympathetic tone Anemia Fever Hypertension Advanced mitral valve disease Auscultation - Heart Sounds • Quieter S1 (AV softly closing or muffled) – – – – Obesity, barrel chested dogs Myocardial failure Pronounced 1st degree heart block hypervolemia Auscultation - Heart Sounds • Louder S2 (SL slamming) – – – – Hyperthyroidism Fever, anemia Heartworm Disease Cor pulmonale (define) • Quieter S2 (SL softly closing) – Myocardial failure (DCM, severe MR) Auscultation - Heart Sounds Third Heart Sound (Gallop) S3 (S1-S2-S3) S4 (S4-S1-S2) Split S2 Systolic Click Summation Gallop (S4-S1-S2-S3) Auscultation - Heart Sounds Third Heart Sound S3 – protodiastolic gallop (S1-S2-S3) – Rapid LV filling – early diastole (audio) – PMI R or L apex – low frequency (best heard with the bell) – At maximal mitral opening (E point on echo) – stiff LV or large diastolic volume – HCM, RCM, DCM, severe MR – Indicates myocardial failure – Usually a bad mamma jamma Auscultation - Heart Sounds Third Heart Sound S4 – presystolic gallop (S4-S1-S2) – – – – Atrial contraction - Late diastole (audio) PMI R or L apex, low frequency (bell) Stiff LV (HCM) Increased afterload • 3rd degree AV block • Myocardial failure (DCM, bad MR) – Sometimes heard in normal cats & giant dogs – not necessarily a bad mamma jamma Auscultation - Heart Sounds Third Heart Sound • Split S2 – – – – – – – PMI right heart base (left side) AoV PV don’t close at same time (PV later) Reverse PDA Pulmonary hypertension (HWDz, COPD) Severe RBBB relative PS of right to left shunts (ASD) normal variation in large dogs (audio) Auscultation - Heart Sounds Third Heart Sound Systolic Click – Very sharp, high frequency click of Mitral valve prolapse, in early CVD • Snapping of the chordae tendinae as they go taught – PMI left apex – Mid-Systolic (audio) (audio) – May be accompanied by a systolic murmur • Early, late, or holosystolic – Often years until CHF develops, if at all 3 Heart Sounds How Can you tell the difference? Does it Matter? – Systolic less likely pathogenic – Systolic Click sounds sharper – Diastolic more likely pathogenic – PMI heart base less likely pathogenic How Can you tell if S3 or S4? – Can’t tell if heart rate is > 160-180 (summation) – just do a cardio work-up Auscultation – Heart Sounds left PMI right 5 1 – left apex (MV) 4 – right apex (TV) 2 – left base (AoV) 5 – left armpit (PDA) 3 – right base (PV) – ausculted on the left Auscultation – Heart Sounds PMI (Point of Maximal Intensity) Left Apex – at palpable apical beat – S1 - MR (mild MR) (severe MR) Left Base – slide cranially & dorsally – S2 - SAS (audio) – S1, S2 - Ao endocarditis (audio) Right Base (left side) – S2 - PS (mild PS) (severe PS) Left Axilla – continuous - PDA (PDA) (severe PDA) Right Apex – S1 – TR – like MR but often quieter (audio) Auscultation – Heart Sounds Muffled Heart Sounds (causes) • Pleural, Pericardial effusion (*difference*) • Diaphragmatic hernia, thoracic masses • obesity What besides cardiac disease can cause a pathologic murmur? • Anemia, hypoproteinemia Why do puppies have innocent murmurs? • Musical, grade 1-2, short (audio) (mild MR) • Larger SV relative to great vessel size • Lower PCV and plasma proteins • Artifact – high frequency breath sounds Auscultation – Murmur Grade Grade 1 • Heard in a very quiet room, concentrating Grade 2 • easily heard on the PMI Grade 3 • Moderately loud Grade 4 • Very loud over much of the chest Grade 5 • Heard with edge of stethoscope on chest, palpable thrill Grade 6 • Heard with stethoscope off chest, palpable thrill Auscultation – Murmur Grade High grade murmurs are more likely to be associated with severe disease Severe disease can also be present with low grade murmur • Occasionally no auscultable murmur in the cat • DCM • ASD • VSD • Reverse PDA (right to left shunting) Dogs almost never have CHF without a murmur Cats can have CHF without a murmur Auscultation – Lung Sounds 6 points 3 Right, 3 Left – correspond to lung lobes Auscultation – Murmurs holosystolic • Starts at the end of audible S1 • Ends at the start of audible S2 • Murmur between the heart sounds Auscultation – Murmurs pansystolic • Starts at the beginning of S1 • Ends at the end of S2 • Just hear the murmur with no distinct HS Respiratory Sinus Arrhythmia • • • • • Heart rate increases during respiration Due to increased vagal tone Normal variation in dogs (not cats) No pulse deficits If present, heart failure is not likely – Increased sympathetic tone overrides • Pronounced in disease processes of increased vagal tone – – – – Increased CSF pressure Chronic respiratory disease Thoracic or abdominal disease After sedation Respiratory Sinus Arrhythmia • DDx – Afib with a normal ventricular rate – Frequent APCs or VPCs (maybe pulse deficits) – Intermittent SSS None of these vary consistently with the respiratory cycle • RSA is regularly irregular • Others are usually irregularly irregular (RSA) (PS with RSA) Physical Exam – Ascites • most common cause of cardiogenic ascites in cats – TVD • Tap and do fluid analysis to distinguish between transudate, modified transudate and exudate (handout) • Usually accumulates slowly, though owners often don’t notice until huge • If truly does develop over days, think pericardial tamponade or caval syndrome Exam – Mucous Membranes Cyanosis • > 4 g/dL of deoxygenated Hb in the blood – Severely anemic animals don’t turn blue – Even with life threatening hypoxia • Differential cyanosis (define) – Front of body pink, back of body blue – Reverse PDA, FATE (why rPDA) – Compare pulse oximetry or blood gases from front of body with rear of body – Weak or no femoral pulses, pain, paresis with FATE Exam – Pulses Technique • Occlude the pulse • Then slowly release pressure until maximum pulse is detected Pulse Pressure = Systolic – Diastolic • Femoral pulse usually not palpable when MAP <50mmHg • Dorsal pedal pulse not palpable when SAP <80mmHg Exam – Pulses Bounding Pulses (water hammer) • Increased systolic pressure (increased SV) – – – – – (causes) Aortic regurgitation Severe bradycardia Thyrotoxicosis (define EF, FS) Fever Anemia/hypoproteinemia • decreased diastolic pressure (diastolic runoff) – PDA – AV fistula – Aortic regurgitation (most common cause) • Aortic endocarditis > SAS Exam – Pulses Weak Pulses • Severely decreased SV – severe HF • Acutely decreased SV – hypovolemia • Decreased peripheral vascular resistance (shock) • Decreased arterial compliance (hypertension) Pulse peaks slowly and late in systole • Pulsus parvus et tardus (cause) • Severe SAS Exam – Pulses Short, Brisk Pulses (snappy) • Short, fast systole • Compensated MR (what happens to FS with MR) Pulse weak or absent during inspiration • Pulsus paradoxus • Systolic pressure falls during inspiration • With pronounced respiratory sinus arrhythmia • Exaggerated by pericardial effusion Exam – Pulses Alternating Weak and Normal Pulses • Pulsus alternans • Severe myocardial failure (define MF vs CHF) (causes) – DCM – RCM, UCM (define) – End stage valvular disease – Prolonged tachyarrhythmia or tachycardia Exam – Pulses Pulse Deficits (heart beat generates no pulse) • VPCs • Atrial fibrillation with VPCs • Tachyarrhythmia (inadequate filling) • Every other heart beat has a pulse deficit – Pulsus bigeminis – Caused by ventricular bigeminy (define) Totally chaotic heart sounds and pulses • Lots of multiform VPCs • Atrial fibrillation (audio) Exam – Jugular Veins • Clip or wet the fur over the jugular veins • Evaluate sitting or standing (not sternal) • Jugular Distension (causes) – suggests increased RA pressure (normal dogs cats?) • 2-3 cm H20 in cats, 5-8 cm H20 in dogs – Or less often jugular or caval occlusion • Jugular Pulse (normal dogs cats) – 5-8cm dorsal to RA in dogs, 2-3 cm in cats – Too high indicates increased right heart pressure • If abnormalities above not noted, occlude at thoracic inlet, and release • Hepatojugular reflux Exam – Jugular Veins Jugular distension, high pulse, +HJR • Jugular/caval occlusion (causes) – Heartworm disease – External mass (cyst, abscess, granuloma, neoplasia) – Thrombus (causes) • Decreased RV compliance – RV hypertrophy • PS, TOF, pulmonary hypertension – Restrictive CM – RVOT obstruction • Heartworm disease, neoplasia, thrombus Exam – Jugular Veins Jugular distension, high pulse, +HJR • RV volume overload – TR with RHF – VSD – HWDz • Compression on the RV, so it can’t fill – Pericardial effusion – constrictive pericarditis – Pericardial mass Evaluation of hepatic & splenic veins on US are even more sensitive for increased RV pressure Exam – Extremities Peripheral edema • rare • Often accompanied by diarrhea • Due to RHF Cold extremities • Due to RHF and venous stasis • Or saddle thrombus – Acutely painful, followed by lack of pain ( Cardiovascular Exam form ) Acknowledgements Smith FWK, Keene BW, Tilley LP • Rapid Interpretation of Heart and Lung Sounds, 2nd ed, 2006 Kvart C & Haggstrom J • Cardiac Auscultation and Phonocardiography, Veterinary Information Network Kittleson M • Small Animal cardiovascular Medicine, Veterinary Information Network. Chapter 3 – Signalment, History and Physical Examination