Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
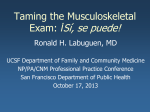
Pressure pain threshold of Popliteus muscle in knee pain subjects A Protocol submitted to HOSMAT HOSPITAL EDUCATIONAL INSTITUTE Bangalore DISSERTATION RESEARCH By Zakirhusen V. Moria M.P.T. 1st year M.P.T (Musculoskeletal and sports) Guide: Dr. R. Dev Anand (PT) 1 RESEARCH APPROVAL Pain pressure threshold of Popliteus muscle in knee pain subjects Research proposal approved by Institutional ethics Committee On 19/11/2010 INSTITUTIONAL ETHICS COMMITTEE HOSMAT HOSPITAL EDUCATIONAL INSTITUTE BANGALORE -25. 2 CONTENTS Page No. 1 INTRODUCTION 04 1.1 Background of the study 04 1.2 Statement of the problem 06 1.3 Objective of the study 06 1.4 Hypothesis 06 1.5 Null Hypothesis 06 1.6 Operational Definition 06 1.7 Clinical significance 07 2 REVIEW OF LITERATURE 08 3 METHODOLOGY 10 3.1 Study Design 10 3.2 Study Setting 10 3.3 Inclusion Criteria 10 3.4 Exclusion Criteria 10 3.5 Materials 10 3.6 Sample size 10 3.7 Procedure 11 3.8 Outcome measures 12 3.9 Data analysis 18 4 REFERENCES 5 APPENDIX 19 Appendix I 22 Appendix II 23 Appendix III 26 Appendix IV 27 3 Key word: Pain pressure threshold-PPT Popliteus muscle-PM 1 INTRODUCTION 1.1 Background of the study PM is a small muscle that runs in the posterior part of the knee. It is a thin , flattened and triangular shaped muscle which forms the floor of popliteal fossa.It originates on the lateral surface of the lateral femoral condyle(in front of and below the lateral collateral ligament origin) and also from the fibular head. It also has a origin stemming from the posterior horn of the lateral meniscus. The tendon then courses under the lateral collateral ligament becomes extra-articular before joining its muscle belly, which inserts into medial to the posterior surface of tibia just above the soleal line.1,2,.3 Located at the back of the knee, semimembtinosus muscle and overlying semitendinousus tendon forms the upper medial border of Popliteal fossa.The biceps femoris muscle forms the upper lateral border. Lower medial and lateral head is formed by gastrocnemius muscle. The PM is believed to have number of functions, made possible by its unique ability to reverse its origin and insertion , depending upon on whether the femur or the tibia is fixed. PM is a primary, dynamic,transverse plane rotatoy knee joint stabilizer.It is an important controller of knee rotation during stance phase of locomotion.4 4 Unlocks the knee joint from its locked position by internally rotating tibia. Helps the Postrior cruciate ligament maintain stability by preventing excessive posterior translation of tibia. Prevents excessive external and varus rotation of the tibia during knee flexion. Popliteus is referred to the main internal rotator of the knee that is in charge of stabilizing 1.a.: Referred pattern of are knees at cutting or stopping. People involved inFig. frequent cutting pain or stopping trigger point PM. considered to be at higher risk for accumulated micro strain of of popliteus. Hypertrophy and adaptive shortness of popliteus associated with rotational malalignment might also Fig.1 b.:anterior Site forknee PPTpain examination be found and responsible for the development of Idiopathic .5 of PM. Myofascial pain syndrome (MPS) is characterized by pain originating from trigger points at muscle and fascia associated with muscle spasm, tenderness, motion restriction, fatigue, and sometimes autonomic dysfunction of the related region.6 Myofascial pain of Popliteus presents as pain in the back of the knee when crouching and running or walking , especially going downhill or downstairs. Movement examination will show that resisted flexion and resisted medial rotation is painful posterior. 7 Knee dysfunction subjects report one or more of the following symptoms such as: Painful knee flexion-extension or difficulty in completing final degrees of flexion ROM or Pain during weight bearing flexion-extension activity or difficulty in maintaining fully flexed position for longer time period. 8 The PM dysfunction may primarily exhibit a lack of knee extension and external rotation on femur. This may be attributed to 1. The PM may be hyperactive in the presence of a poorly functioning quadriceps muscle group. The key role of PM is to control posterior tibial translation during movement. Inefficient quadriceps will cause overactive of PM to help maintain posterior stability.4 2. A weak hamstring results in hypertrophy of the PM to control tibial rotation in stance phase.4 3. Hypertrophy due to overuse of the PM caused by to poor biomechanics, running surfaces or poor training progression.4 5 Patient with PM tenderness also complains of radiating anterior knee pain .Although anterior knee pain is very common; the mechanism for the development of anterior knee pain is still controversial. It has been widely attributed to abnormal quadriceps angle (Qangle), however, it was also proposed that anterior knee pain is a multi-factorial problem and not only limited to malalignment in the frontal plane. Recently, malalignment in the transverse plane, namely knee version (KV), was considered to be one of the causes for the development of idiopathic anterior knee pain (IAKP) that failed to conservative management.1,5 Pressure pain threshold(PPT) refers to minimal pressure (force) which induces pain. The pressure threshold meter (PTM) is a force gauge with a rubber disc of 1cm2 surface. The instrument has been proven to be useful in clinical practice for quantification of deep muscle tenderness. Assessment of sensitivity to pain can be diagnosed by PTM.4,9,10 Travell and Simons (1999) have stated that when PM is involved in the complaint of posterior knee pain, Patient examination will reveal tenderness of its tendon as well as region over its tendinous attachment to the femur, sometimes referred to the Gastrocnemius area. 11 Pee-Yun lee demonstrated that subjects with Lower External rotation-Internal rotation ratio will show significantly lower Pain pressure threshold at both Pes Anserinus and PM.5,12 1.2 Statement of problem Popliteus dysfunction is often neglected area of clinical examination. Knee dysfunction subjects are seldom assessed for Popliteus dysfunction as symptoms are not clear in Popliteus dysfunction subjects. 1. 3 Objective of the study To check PPT of Popliteus muscle in knee pain subjects. To compare it with normal leg. 1.4 Hypothesis In knee pain subjects PPT of PM will be low in comparison with normal knee. 6 1.5 Null hypothesis PPT of PM is not significantly different from normal knee. 1.6 Operation definition Trigger point-patient with active trigger point will show jump sign; an indication of trigger point location in which patient forcefully pulls away when trigger point is contacted. Non-specific knee pain refers to pain at knee due to non-pathological;soft tissue dysfunction or biomechanical dysfunction (spasm, length-tension, flexibility, strength deficit). 1.7 Clinical significance By measuring PPT of affected and unaffected side, normal pressure threshold of PM will be established. Strategies to increase the PPT level of affected side can be devised. By improving the PPT of subject, it’s easy to treat the Myofascial Dysfunction because patient will be less apprehensive and will be able to withstand more pressure. 7 2.0 REVIEW OF LITERATURE Anatomy of Popliteus The PM is a thin flat, triangular muscle, which forms part of the floor of the popliteal space. It arises by a strong tendon, from a depression on the outer side of the external condyle of the femur, and from the posterior ligament of the knee join, and is inserted into inner two-third of the triangular surface .The tendon of PM is covered by biceps femoris and the lateral collateral ligament(LCL).12 PM is described as Flattened triangular shaped muscle. Its broad belly attaches medially to the posterior surface of the tibia above the soleal line, tapering to an apex as it approaches the knee joint.13 PM originates from the lateral femoral condyle near LCL and inserts along the proximal 1012cm of the poster medial tibial surface forming the floor of the Popliteal fossa.14 Role of Popliteus John Nyland et al in the year 2005 stated that the Popliteus muscle acts as a dynamic guidance system for monitoring and controlling subtle transverse and frontal-plane knee joint movement.1 Kun Hwang(2010) in 13 cadaveric study stated that ,PM is internal rotator of leg on femur or an external rotator of femur upon tibia and also flexor of tibia .When standing with knees flexed , it contracts to help prevent forward displacement of femur on tibia.20 Basmajian and Lovejoy (1971)studied in 20 subject, found that, with the leg free to move, the Popliteus muscle was activated by voluntary effort to produce medial rotation of the leg at knee angles between knee straight and 90° of flexions in the sitting and prone positions.7 Travell and Simons (1992) stated that Trigger point in the knee joint primarily refers to the back of the knee joint during crouching , running or walking especially during walking downhill or downstairs. The Trigger point tightness of PM restricts the ROM passive lateral rotation and weakens active medial rotation of the led with the knee flexed nearly 90o.The relatively small restriction of full knee extension (usually only 5° or possibly 10°) is often not clearly appreciated until retesting after treatment. Only then is the full range of normal extension for that patient's knee identified.16 Musculoskeletal dysfunction and symptoms Musculoskeletal pain manifest as localized, regional or widespread pain. Musculoskeletal pain is typically described by patient as a drilling, tight, radiating and diffuse pain sensation with pain referrals and is often accompanied by deep tissue hyperalgesia or allodynia. 8 Affected muscle often display pain during movements, subjective weakness, increased fatigability, stiffness and slightly restricted range of motion.6 Algometric measurement of PPT Andrew A Fischer (1986) did study in 24 male and 26 female subjects established standards for pressure threshold as well as the reproducibility and validity Pressure algometry over normal muscles and Standard values validity and reproducibly of Pressure threshold.9 Chesterson, Linda did a study on “Interrater Reliability of algometry in measuring pressure pain threshold in Healthy humans, Using multiple rater” and concluded that Algometer is highly reliable measures of PPT with minimal observer error.(ICC=0.91).15 Delaney GA, Mckee AC, did a study on Trapezius muscle for trigger point sensitivity, of right and left side, for interratter and intrarater reliablity. ICC=0.86 and ICC=0.92 for interratter reliability and ICC=0.91 and ICC=0.80 for intraratter reliability.24 Ethne L Naussbaum, laurie Downes stated that PPT is a reliable measure, and repeated algometry does not change pain threshold in healthy muscle with experimental induced DOMS over 3 consecutive days.The PPT can be used to evaluate the development and decline of muscle tenderness. Reliability is enhanced when all measurements are taken by one examiner.13 9 3 METHODOLOGY 3.1 Study Design Observational design Descriptive study 3.2 Study Setting HOSMAT hospital,Physiotherapy Out patient department. 3.3 Sample size 60 subjects 3.4 Inclusion Criteria Non-specific knee pain. Tenderness over Popliteal space. Pain/Inability to fully flex or extend the knee actively. Painful resisted flexion and/or internal rotation. Painful and/or deficient passive knee external rotation. 3.5 Exclusion Criteria Acute post-operative knee joint. Knee join inflammation and gross swelling. Neurological impairment. Infectious Knee joint. Baker’s cyst. Popliteal abscess. Venous or Arterial disorders. Asymmetry in Popliteal space. 10 3.6 Instruments and Materials Pressure Algometer (fig no.2) 1 Cm2 rubber tip for Algometer Goniometer Visual analogue scale Lysholm Knee Scoring Scale 3.7 Outcome measures Primary Outcome measure-PPT of PM Affected and Unaffected leg Secondary Outcome measure Range of motion-Knee joint Functional Impairment-Lysholm knee rating scale Muscle strength-Manual MMT Flexibility of Hamstring Visual analogue scale 11 3.8 Procedure: Phase I: Familiarization of Algometer by researcher The familiarization shall be done on normal healthy subjects( students of Hosmat education institute ,Bangalore). The simple random sample of (N=10) will be done from the aggregate student list of Hosmat educational institute. 5 male and 5 female students will be selected as sample.and a written consent shall be obtained. The subjects shall be instructed to assume the following positions. The algometer probe will lowered at respective muscle spots and subjects will be asked to report sensation of pain distinct from pressure.This procedure will be repeated on both the sides and will be performed within a same day. The aim of the procedure would be to learn to pressurize at constant rate of 5 N/S.6 The instrument practice session shall be done on 8 different location (muscle spots). Muscle to be examined Trapezius Deltoid Biceps Brachi Common extensor origin 1st dorsal interossei Quadriceps Hamstrings Popliteus Position of the subjects Sitting with arm relaxed Location of PPT Midpoint between C7 and acromian24 Sitting with arm relaxed 5 cm below acromian process30 Seated with arm horizontal 1/4th distance from elbow abduction with elbow full crease to the lateral border of extension & forearm acromian over bicep muscle supinations belly30 Supine line with palm on Most prominent part over treatment couch lateral epicondyl17 Sitting with hand supported on Over the belly of 1st dorsal table interossei when thumb & index finger held close together.15 Supine lying 15 cm above the base of patella16 Prone with knee 900 flexion Over the bulk of muscle 16 Prone lying with knee flexed Over the belly of muscle11 . to 20 Phase II: Assessment of PPT in knee pain subjects: Interested subjects coming to the Physiotherapy department will be screened for inclusion and exclusion criteria by a therapist II (who is not part of in the study). On satisfying the screening, subject shall be taken into study after taking a written consent 12 Familiarization of subject After screening,the subject shall be positioned in prone lying with pillow support under ankle with knees flexed to 200 by therapist II.To familiarize the subject with the Algometer, the shoulder shall be placed in abduction of 1200 with external rotation to lie on the couch with elbow in 900 by the researcher. To familiarize the subject with Algometer, common extensor origin of left forearm shall be marked . Now, the researcher will instruct the subject to report the subjective feeling of pain distinct from pressure. After that he researcher shall apply the force through Algometer at constant rate of 5N/s. The subject is instructed when he/she shall feel pressur/pain on the area tested during algometry. The subject is asked to say “stop” as soon as sensation of pain distinct from pressure or discomfort will reach and bring to notice to the researcher. The Algometer shall be retracted and reading of the Algometer shall be recorded as the PPT of that area. This shall be repeated for 5 trials, to enable the subject better understand the PPT level Examination of the PPT of PM The subject shall now be assessed for PPT in the same position described above. The researcher shall toss a coin to find the order of the assessment(left or right leg first) , irrespective of the side affected. The head of the coin shall represent Right side and tail shall represent left. This ensures the observer bias in minimal. The popliteal space will be palpated by the researcher to find the trigger point location.PPT of PM is measured at the belly of muscle.The Algometer probe will be lowered at constant rate of 5 N/s perpendicular to the tissue. The patient will be asked to say “stop” as soon as sensation of pain is felt. At this point Algometer probe will be immediately released and reading shall be taken. PPT shall be measured 3 times with rest interval of 15 seconds.(Fig no.4) After measuring PPT in one knee, the same procedure shall be performed on the contralateral knee for 3 repetitions with rest interval of 15 seconds. The average of PPT shall be used for data analysis. Following the assessment of primary outcome, the secondary outcome of shall be assessed. Active knee range of motion assessment Flexion: The subject will be positioned in supine lying and will be asked to bend the knee as much as he can. Extension: The subject will be positioned in high sitting at the edge of the bed and with both the hand on thigh. The subject will be asked to straighten knee as much as he/she can without lifting the thigh. Both reading shall be documented by the Goniometer(Fulcrum at lateral epicondyle).29 . 13 Functional impairment: The subject shall be instructed to fill the Lyscholm knee rating scale(LKS) and the scores shall be used for data analysis. Flexibility: Hamstring: 90/90 or Active knee extension hamstring flexibility test.28 Procedure: Hamstring: 90/90 or Active knee extension hamstring flexibility test. Procedure: The subject lies supine with arm across the chest. The hip being tested shall be passively flexed until thigh is vertical, while opposite leg fully extended. The subject is has to extend the knee as much as he can. Measurement: Any deficit in knee joint extension shall be recorded by goniometer. Muscle Strength: Manual muscle testing for grade 4 and grade 5 Hamstring muscle: Procedure-subject prone with knee 450 flexion. The researcher shall place one hand over ankle and other at posterior thigh. Resistance is applied in the direction of knee extension for grade 4 and 5 while subject shall flex his knee while in neutral rotation.29 . Visual analogue scale/VAS:(Appendix III) The subject is instructed to mark his/her level of pain at rest and during aggravating factor(position/movement).The aggravating factor shall be recorded on the VAS chart.The subject shall mark on a line which is marked “No pain” on one side and “Max pain’ on the other side. 14 Flow chart depicting the procedure Patient with knee pain reported to Outpatient department in Hosmat hospital Screening by other therapist II for inclusion and exclusion criteria Subject position in prone lying by therapist II Familiarization of subject with Algometer by the researcher at common extensor origin Coin toss randomization for the side of assessment PPT of Right knee PM assessed firstly then left PPT Left knee PM assessed first then Right Primary outcome noted (PPT) Thorough assessment of Affected knee (Appendix) Secondary outcome measure assessed Data tabulation Data analysis 15 3.9 Data analysis (1) Demographic data: Mean (SD) (2) Comparison of PPT between affected and unaffected leg using paired t-test. 16 4.0 References 1. Narusha Lachman, Yavuz Kocabey,Joseph Brosky, Remziye Altun,David Caborn, John Nyland.Anatomy ,Function and Rehabilitation of Popliteus Musculotendinous complex.J Orthop Sports Phys Ther. 2005;35(3):165-7 2. Stephanie Woodley, Susan Macer. Anatomy in practice: the popliteus muscle. New Zealand Journal of Physiotherapy 34(1):25-9. 3. Dr Ian Macintyre. Anatomy and Function of the Popliteus muscle. Available from URL//www.sportsperformancecentres.com 4. Poplitus Muscle and Tendon. The Forum of Benfleet running club.Available from URL//http://benfleetrunningclub.myfastforum.org/popliteus_muscle_and_tendon_ab out495.html. 5. Pei-Yun, Lee. The Role of Knee Version in the Development of Idiopathic Anterior Knee Pain.Available from URL//http://etdncku.lib.ncku.edu.tw/ETT-db/ETDsearch/view-etd?URN=etd-0713105-144721. 6. Hakguder A, Birtane M, Gurcan S, Kokino S, Turan FN. Efficacy of Low Level laser therapy in myofascial pain syndrome:An algometric and thermographisc evaluation. Lasers Surg Med. 2003:33(5):339-43. 7. Basmajian JV,Lovejoy JF Jr. Functions of the PM in a man. A multifactorial Electromyographic study. J bone joint surg. Am 1971;53:557-562 8. Faletti C,De Stefano N, Guidice G, Larciprete M. Knee impingement syndromes. Eur J Radiol . 1998 May:27 Suppl 1:S60-9. 9. Fischer AA. Pressure algometery over normal muscles.Standard values,validity and reproducibility of pressure threshold. Pain.1987 Jul:30(1):115-26. 17 10. Fischer AA. Application of pressure algometry in manual medicine.J Man Med ;5:145-50 11. W-L Chen, P-Y Lee, J-S Li, T-h Huang, C-Y Yang and H Peng. The Relationship among Lysholm score, structural measure, Muscle imbalance and functional performance in college basketball players with anterior knee pain.Journal of Biomechanics(January 2007). 40.Supplement 2,pg S335-S335 12. Lee Winson C.C., Zhang,Ming, Arthut . Mak How well different regions of residual limb tolerate presssure?. Available from URL//http://eprints.qut.edu.au/2953/ 13. Nussbaum EL,Dowes L. Reliability of clinical pressure-pain measured on consecutive days.Phys Ther.1998 Feb;78(2):160-9 14. Fischer AA. Pressure threshold meter: Its use for quantification of tender spots. Arch phys med Rehabilit Nov;67(11) 836-8 15. Chesterton LS, Sim J,Wright CC, Foster NE. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters.Clin J Pain.2007Nov-Dec:23(9):760-6 16. Travell JG,Simons D, Baldmore. Myofascial pain dysfunction: The trigger point manual, vol 2; the lower extremities. Williams and Wilkins 1992. 17. Young A,Stokes M,Iles JF. Effects of joint pathology on muscle. Clinical Orthopaedics and Related Research .1987 June:(219); 21-27. 18. Stratford P .Electromyography of the quadriceps femoris muscles in subjects with normal knees and acutely effused knees. Physical Therapy March1982 vol(3)62; 279-83. 19. Flemming Enoch, A Review of the Anatomy . Physiology and Function of Popliteus Muscle. Avialable from URL//http://www.kineticcontrol.com/document/clinic/litreview_popliteus_pdf. 18 20. S.English, D.Perret. Posterior knee pain. Curr Rev Musculoskeletal Med. 2010 October:3(1-4):3-10 21. Bill Vicenzino, Jane Brooksbank, Joanne Minto, Sonia Offord, Aatit Paugmali.Initial effects of elbow taping on painful grip strength and Pain pressure threshold. J Orthop Sports Phys Ther. Volume 33(7) July 2003 22. Kun Hwang, Kyon Moo Lee, Seung Ho Hun, Sun Goo Kim.Shape and Innervation of Popliteus muscle. Anat Cell Biol.43:165-68(2010) 23. Reeves JL, Jeeger B, Graff-Radford Sb. Reliability of the pressure algometer as a measure of myofascial trigger point sensitivity . Pain 1986;24(3);313-321 24. Delaney GA ,Mckee AC. Inter and intra-rater reliability of the pressure threshold meter in measurement of myofascial trigger point sensitivity . Am J Phys Med Rehabil 1993;72(3);136-39 25. Graven-Nielsen T, Arendt-Nielsen L.Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat Rev Rheumatol 2010 Oct;6(10):599-606. 26. Helen J. Hislop, Jacqueline Montgomery, Muscle Testing, 6th edition, W.B. Saunders.1995. 27. Marta Imamura, Satiko Tomikawa Imamura, Helena H. S. Kaziyama, Rosa Alves Targino, Wu Tu Hsing, Luiz Paulo Marques de Souza, et al. Impact of nervous system hyperalgesia on pain , disability and quality of life in patient with knee osteoarthritis: a controlled analysis. Arthritis and Rheumatism. Vol 59(10)oct 2008: 1424- 31. 28. 90/90 active knee extension (AKE)Hamstring flexibility test. Available from URL//http.//www.topendsports.com/test/flex-9090htm 29. Cynthia C Norkin, D Joyce White, Measurement of joint motion:A guide to goniometry.2nd edition. F.A.Davis Company. 30. Florence P. Kendall, Elizabeth K. McCreary, Patricia G. Provance.Muscle testing and function with posture and pain.5th edition. Lippincott Williams and Wilkins. 19 5 APPENDIX 5.1 Appendix I HOSMAT College of Physiotherapy Rajiv Gandhi University Consent Form I ________________________________ agree to take part in the research study conducted by MORIA ZAKIRHUSEN V , Postgraduate student (M.P.T. Musculoskeletal & Sports), HOSMAT College of Physiotherapy, Rajiv Gandhi University, entitled. “PAIN PRESSURE THRESHOLD OF POPLITEUS MUSCLE IN KNEE PAIN SUBJECTS” I acknowledge that the research study has been explained to me and I understand that agreeing to participate in the research means that I am willing to Provide information about my health status to the researcher Allow the researcher to have access to my medical records, pertaining to purpose of the study Participate in evaluatory program. Make myself available for further follow up.(If needed) I have been informed about the purpose, procedures, measurements and risks involved in the research and my queries towards the research have been clarified. I provide consent to the researcher to use the information, video or audio recordings, for research and educational purpose only. I understand that my participation is voluntary and can withdraw at any stage of the research project. I understand that no monetary benefit will be given for participation in this research study. Name of the applicant – Signature Date Signature of the researcher 20 Appendix II Screening form Name: Age: Sex: Occupation: Hospital number: Chief complaints: Inclusion criteria: Pain/ Tenderness in popliteal space Non-specific knee pain Inability to fully flex/extend knee joint Painful resisted flexion and internal rotation Painful/deficient of knee external rotation Exclusion criteria: Acute post-operative knee joint Gross knee swelling of knee joint Knee joint inflammation Infectious joint Baker’s cyst Popliteal abscess Venous/Arterial disorders Asymmetry in Popliteal space 21 Research study subject number: Primary outcome chart: PPT of PM 1st trial 2nd trial 3rd trial Average Affected side Right knee Left knee Assessment form: History: On observation: Attitude of the limb at rest Gait pattern On palpation: Tenderness Local temperature Trigger point identification On examination: 22 Secondary outcome chart: Right knee Left knee Range of motion Flexion Extension Muscle Strength Hamstring Visual analogue scale Flexibility Hamstring Functional impairment(Appendix IV) 23 Appendix III Visual Analogue Scale: No pain Maximum pain VAS at rest No pain Maximum pain VAS with aggravating state 24 APPENDIX IV 25 26 27 28