Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Taming the Musculoskeletal
Exam: İSí, se puede!
Ronald H. Labuguen, MD
UCSF Department of Family and Community Medicine
NP/PA/CNM Professional Practice Conference
San Francisco Department of Public Health
October 17, 2013
Objectives
1. To learn principles of examining
patients with common joint problems
2. To learn common clinical scenarios for
common musculoskeletal problems
3. To learn how to approach diagnosis
and treatment of common
musculoskeletal problems in primary
care and urgent care settings
Objectives
4. To review elements of the physical
examination of the shoulder, elbow,
hand/wrist, hip, knee, ankle, and foot
5. To develop a systematic physical
examination of the shoulder and knee
Principles: Approaching Joint
Problems
• Learn typical clinical scenarios for
common joint problems:
– History
– Chief complaints
– Timing/duration of symptoms
– Typical findings
Principles: Approaching Joint
Problems
• Know functional anatomy, physical
examination techniques for each
joint
• Initial and subsequent treatment
• Red flags: need for referral or
immediate treatment
Common Joints
• Upper extremity:
– Hand/wrist
– Elbow
– Shoulder
• Lower extremity:
– Hip
– Knee
– Ankle
– Foot
Case 1: Hand/Wrist
• 43 yo man c/o
hand numbness
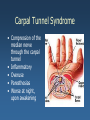
Carpal Tunnel Syndrome
• Compression of the
median nerve
through the carpal
tunnel
• Inflammatory
• Overuse
• Paresthesias
• Worse at night,
upon awakening
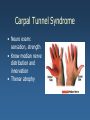
Carpal Tunnel Syndrome
• Neuro exam:
sensation, strength
• Know median nerve
distribution and
innervation
• Thenar atrophy
Carpal Tunnel Syndrome
• Tinel’s sign
• Phalen’s sign
• Flick sign
Carpal Tunnel Syndrome
• NSAID’s
• Volar (cock-up) wrist
splint
• Steroid injection
• Surgery
Other Common Hand and Wrist
Problems
•
•
•
•
Arthritis
De Quervain tenosynovitis
Fall on outstretched hand (FOOSH)
Fractures: phalanges, metacarpals,
scaphoid (navicular), distal radius
• Ganglion cyst
• Trigger finger
• Mallet finger
Case 2: Elbow
• 43 yo man c/o
pain in elbow
Lateral Epicondylitis
• Tears/microtears in
tendons originating
at lateral epicondyle
• Overuse of forearm
muscles
• Inflammatory
• Constant symptoms
– Aching night pain
referring to humerus
Lateral Epicondylitis
• Pain on palpation just
distal to lateral
epicondyle
• Pain with resisted
– Active extension
(passive flexion) of wrist
– Supination
– 3rd finger extension
Lateral Epicondylitis
• NSAIDs
• Tennis elbow
brace
• Steroid injection
• Surgery
Other Common Elbow Problems
• Arthritis
• Fractures: distal humerus, radial
head
• Medial epicondylitis
• Olecranon bursitis
• Nerve compression syndromes
• Rupture of distal biceps tendon
Radial Head Fracture
• Most common fracture in adults
• FOOSH, axial load to distal radius
• TTP @ radial head
• Ballotable hemarthrosis
Lateral
epicondyle
Radial
head
Case 3: Shoulder
• 43 yo man c/o
right shoulder
pain
Impingement Syndrome
• Inflammation of
subacromial bursa
and rotator cuff
tendons
• Overuse
• Continuum of
pathology
Impingement Syndrome
• Anterior and
lateral shoulder
pain
• Gradual onset
• Overhead activity
• Worse at night
• Can’t sleep on
affected side
Impingement Syndrome
• Palpation
– Greater tuberosity
– Subacromial
bursa
• Signs:
– Neer
– Hawkins
– Supraspinatus
impingement
Impingement Syndrome
• NSAIDs
• Rest
• Stretching &
strengthening
• Steroid injection
• Surgery
Other Common Shoulder
Problems
•
•
•
•
•
•
•
Acromioclavicular arthritis/injury
Arthritis
Fractures of the clavicle, humerus, scapula
Rotator cuff tear
Biceps tendon rupture
Shoulder instability
Superior Labrum Anterior-to-Posterior (SLAP)
lesions
• Thoracic outlet syndrome
http://en.wikipedia.org/wiki/File:Luxation_epaule.PNG
Shoulder Exam
• Inspection
• Range of Motion
• Palpation
Shoulder Exam
• Special tests
– Impingement signs: Neer, Hawkins
– Strength testing: Supraspinatus,
external/internal rotation
– O’Brien’s test (SLAP lesion)
– Apprehension sign (glenohumeral
instability)
Case 4: Hip
• 63 yo man c/o
thigh pain
Osteoarthritis of the Hip
• Degenerative
• Loss of articular
cartilage
• Primary or
secondary
• Trauma
• Osteonecrosis
• Previous joint
infections
Osteoarthritis of the Hip
• Gradual onset of anterior
thigh or groin pain
• Buttock or lateral thigh
pain
• Referred pain to distal
thigh, knee
• Initially only with
activity; more constant
later
• Decreased ROM
• Limp, stiffness
Osteoarthritis of the Hip
• ROM: loss of
internal rotation
first
• Fixed external
rotation and
flexion
contracture
• Antalgic gait
• Abductor lurch
Osteoarthritis of the Hip
• X-rays:
– Joint space
narrowing
– Osteophytes
– Subchondral cysts
– Subchondral
sclerosis
Osteoarthritis of the Hip
• Pain/antiinflammatory
medication
• Activity
modification
• Assistive device
• NWB exercise
• Steroid injections
• Surgery
Other Common Hip Problems
• Osteonecrosis of the hip
• Snapping hip
• Hip strains
• Trochanteric bursitis
• Fractures: pelvis, proximal femur
Case 5: Knee
• 34 yo woman c/o
knee pain
Management of Patellofemoral Pain Syndrome
SAMEER DIXIT, M.D., AND JOHN P. DIFIORI, M.D., UNIVERSITY OF CALIFORNIA, LOS ANGELES,
LOS ANGELES, CALIFORNIA
MONIQUE BURTON, M.D., UNIVERSITY OF WASHINGTON, SEATTLE, WASHINGTON
BRANDON MINES, M.D., EMORY UNIVERSITY, ATLANTA, GEORGIA Am Fam Physician 2007;75:194-202,
204. Copyright © 2007 American Academy of Family Physicians
Patellofemoral Pain
• Overuse/
overloading
• Diffuse, aching
anterior knee pain
• Sometimes caused
by patellar
malalignment
Patellofemoral Pain
• Feels like knee
“catches” or might
“give way”
• Worst when
– Running
– Going up/down
stairs
– Kneeling,
squatting
– Getting up after
sitting for a while
Patellofemoral Pain
• Weight bearing
stance and gait:
– Patellae point to
each other
– Knock-knees
– Foot pronation
Patellofemoral Pain
• Excessive femoral
anteversion (hip internal
rotation > external
rotation by 30°+)
• J sign (patella moves
laterally >1 cm near full
extension)
• Tight hamstrings,
quadriceps
• Patellar grind test
• Patellar apprehension test
Lateral patellar tracking
("J" sign).
As the knee is extended from 90
degrees flexion (A) to full
extension (B), the patella
demonstrates an abnormal path,
deviating laterally at full
extension.
Patellar mobility testing.
Depicted is medial glide testing
performed on the right knee.
The patella is grasped in the resting
position (A), then translated medially (B).
The extent of displacement is described
in relation to the width of the patella and
measured in quadrants (C).
Displacement of less than one quadrant
medially indicates tightness of the lateral
structures. Displacement of more than
three quadrants is considered
hypermobile.
Patellar tilt test.
This test assesses for tightness of
the lateral structures.
The knee is extended and the patella
is grasped between the thumb and
forefinger. The medial aspect of the
patella is then compressed
posteriorly while the lateral aspect is
elevated.
If the lateral aspect of the patella is
fixed and cannot be raised to at least
the horizontal position (0 degrees),
the test is positive and indicates tight
lateral structures.
This also can be seen in patients
with patellofemoral osteoarthritis.
Patellar grind (or inhibition) test.
While the patient is in the supine position with the knee extended, the
examiner displaces the patella inferiorly into the trochlear groove
(pictured). The patient is then asked to contract the quadriceps while the
examiner continues to palpate the patella and provides gentle resistance
to superior movement of the patella.
The test is positive if pain is produced, although comparison to the
contralateral knee is needed to interpret the result.
Patellofemoral Pain
• X-rays
– Rule out malalignment,
arthritis
Patellofemoral Pain
• Relative rest
• Quadriceps
strengthening
• Increase flexibility in
quadriceps and
hamstrings
• Brace
• Analgesics
• Surgery
“The knee is the worst-designed
joint in the human body.”
Other Common Knee Problems
•
•
•
•
•
•
•
Ligament injuries: ACL, MCL, LCL, PCL
Arthritis
Bursitis (prepatellar, pes anserine)
Iliotibial band syndrome
Meniscal tear
Patellar/quadriceps tendinitis
Popliteal (Baker’s) cyst
Knee Exam
• Inspection
• Palpation
• Special tests
– Ligament
– Meniscus
Knee Exam
• ACL – Lachman’s
• PCL – Posterior drawer, sag sign
• MCL – valgus stress
• LCL – varus stress
• Meniscus – McMurray’s
circumduction, Apley’s grind,
Thessaly
Knee X-ray Tips
• Ottawa Ankle Rules
– Age ≥ 55
– Unable to bear weight 4 steps
– Unable to flex to 90°
– Isolated tenderness of patella
– Tenderness at fibular head
• Weight bearing films for dx of OA
RAZIB KHAUND, M.D., SHARON H. FLYNN, M.D., Iliotibial Band Syndrome: A
Common Source of Knee Pain Am Fam Physician 2005;71:1545-50
Ober's test.
The patient lies down with the unaffected side
down and the unaffected hip and knee at a 90degree angle.
If the iliotibial band is tight, the patient will have
difficulty adducting the leg beyond the midline and
may experience pain at the lateral knee (arrows).
Case 6: Ankle
• 43 yo man c/o acute ankle injury and pain
Ankle Sprain
• Inversion injury
• Stretching or tearing
of lateral ligaments
Ankle Sprain
• Watch out!
– Fractures (e.g.,
avulsion fracture at
base of 5th
metatarsal)
– Distal or proximal
fibula fracture
– Peroneal tendon
tear or subluxation
– Lisfranc injury
Ottawa Ankle Rules
Ankle Sprain
•
•
•
•
•
NSAIDs, RICE
?Ambulatory cast
WBAT
Early mobilization
Rehab:
–
–
–
–
Strengthening
Proprioception
Agility
Endurance training
Other Common Ankle Problems
• Achilles tendonitis or rupture
• Chronic lateral ankle pain
• Fractures
Case 7: Foot
• 43 yo man c/o chronic heel pain
Plantar Fasciitis
• Microtrauma of the
plantar fascia at the
insertion in the
medial tuberosity of
the calcaneus
• Overuse
• Inflammatory
• More common in
women, overweight
Plantar Fasciitis
• Insidious onset
• Worst when arising
from resting
position, prolonged
standing/walking
Plantar Fasciitis
• Focal pain and
tenderness over
medial calcaneal
tuberosity and 1-2
cm distally along
plantar fascia
• Pain with passive
dorsiflexion of toes
• Achilles tendon
tightness
Plantar Fasciitis
• Stretching
• Anti-inflammatory
treatments
• Orthotics (heel
pad)
Plantar Fasciitis
• Tension night splint
Plantar Fasciitis
• Steroid injection
• Surgery
Other Common Foot Problems
•
•
•
•
•
•
•
Bunion
Fractures
Interdigital (Morton) neuroma
Metatarsalgia
Posterior heel pain
Tarsal tunnel syndrome
Turf toe (1st MT joint sprain)
Summary: See? İse puede!
• Joint complaints are commonly seen in
family medicine
• Learn the functional anatomy of the
joints and how it relates to the physical
exam
• Learn typical historical scenarios for
common joint problems and the workup
associated with each
References
• Greene WB, ed. Essentials of Musculoskeletal
Care, 3rd ed. Rosemont (Ill.): American
Academy of Orthopaedic Surgeons, 2005.
• American Family Physician, various articles.
• Joseph Moore, MD, Elbow, Wrist and Hand
Injuries, AAFP 2013 Ann. Sci. Assembly.