Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
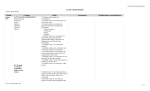
ED: Initial Empiric Antimicrobials for Management of Community-acquired Pneumonia (CAP) and Healthcare-associated Pneumonia (HAP) Condition Preferred treatment options Comments Outpatient- Being Discharged from ED Previously healthy AND No antibiotic therapy within the past 3 months Levofloxacin 750 mg orally every 24 hours for 5 days (dose adjust for renal insufficiency) **(If the patient has Medicaid, insurance covers moxifloxacin 400 mg orally every 24 hours, not levofloxacin. The treatment duration is the same)** OR Azithromycin 500 mg orally once on day 1 then 250 mg once daily on days 2 through 5 Macrolides are active against 70 – 80% of Streptococcus pneumoniae but resistance is increasing. They also have activity against atypical bacteria. During influenza season, would consider addition of an antiviral agent like oseltamivir or zanamivir depending on the susceptibilities of circulating virus if patient is at risk for severe disease or influenza related complications (e.g., asthma). Doxycycline is active against 85% - 90%of strains of S. pneumoniae and also has activity against H. influenzae and atypical bacteria. It is also inexpensive. Antibiotic therapy within the past 3 months OR Comorbid conditions (COPD, DM, Renal Insufficiency, Cirrhosis, CHF) Amoxicillin-Clavulanate 500/125 mg (1 tablet) orally every 6-8 hours for 5-7 days OR Cefpodoxime 200 mg orally every 12 hours for 5-7 days AND Azithromycin 500 mg orally every 24 hours on day 1 then 250 mg every 24 hours on days 2 through 5 OR Levofloxacin 750 mg orally every 11/17/10 If patient has received a fluoroquinolone recently, should strongly consider using a nonfluoroquinolone based regimen, and vice versa. During influenza season, would consider addition of an antiviral agent like oseltamivir or zanamivir depending on the susceptibilities of circulating virus. 24 hours for 5 days **(If the patient has Medicaid, insurance covers moxifloxacin 400 mg orally every 24 hours, not levofloxacin. The duration of therapy is the same)** If severe B-lactam allergy: Levofloxacin 750 mg orally every 24 hours for 5 days **(If the patient has Medicaid, insurance covers moxifloxacin 400 mg orally every 24 hours, not levofloxacin. The duration of therapy is the same)** Patient being admitted to a non-ICU setting with suspected CAP No recent hospitalization Ceftriaxone 1-2 g IV every 24 hours AND Azithromycin 500 mg orally or IV every 24 hours In patients > 80 kg, use ceftriaxone 2g every 24 hours. Please send 2 sets of blood cultures, a sputum culture if possible, and a urinary Legionella antigen. OR If severe B-lactam allergy: Levofloxacin750 mg orally or IV every 24 hours Pseudomonal Risk Please document “pseudomonal risk” Includes patients with history of structural lung disease (e.g., bronchiectasis, interstitial lung disease, chronic bronchitis, COPD, emphysema, pulmonary fibrosis, restrictive lung disease) AND frequent antibiotic use or chronic steroid use 11/17/10 Cefepime 1-2 g IV every 12 hours AND Azithromycin 500 mg orally or IV every 24 hours OR If severe B-lactam allergy: Levofloxacin 750 mg orally or IV every 24 hours once daily Addition of Vancomycin should Recent antibiotics: antibiotic for treatment of any infection within the past 3 months. If recent use of a fluoroquinolone, should strongly consider selection of a nonfluoroquinolone based regimen, and vice versa. Ceftriaxone and levofloxacin are active against >95% of S. pneumoniae strains. PLEASE DOCUMENT SUSPICION be based on patient’s acuity of illness and patient’s previous colonization status. If patient is Please send 2 sets of blood known to have a history of cultures, a sputum culture if MRSA, please add Vancomycin possible, and a urinary Legionella 15 mg/kg IV every 12 hours antigen. (rounded to nearest 250 mg). FOR PSEUDOMONAS Patient with severe CAP (being admitted to an ICU with CAP) Not recently hospitalized Ceftriaxone 2 g IV every 24 hours AND Azithromycin 500 mg IV every 24 hours Please send 2 sets of blood cultures, a sputum culture if possible, and a urinary Legionella If severe B-lactam allergy: antigen. Levofloxacin 750 mg IV every 24 hours For patients with CAP in the ICU, always cover S. pneumoniae and Legionella. Consider coverage for Staphylococcus aureus in the appropriate clinical situation. Addition of Vancomycin (15 mg/kg IV every 12 hours (rounded to nearest 250 mg) should be based on patient’s acuity of illness . Pneumonia post influenza or viral syndrome and/or a chest X-ray with necrotizing features should raise the suspicion for Staphylococcus aureus (MSSA or MRSA). Healthcare-associated pneumonia (HAP) Cefepime 1 - 2 g IV every 12 hours AND Azithromycin 500 mg orally or IV every 24 hours AND Vancomycin 15 mg/kg IV every Please send 2 sets of blood 12 hours (rounded to closest 250 cultures, a sputum culture if possible, and a urinary Legionella mg) antigen. Recently hospitalized or resident of a skilled nursing facility, chronic dialysis, immunocompromised If severe B-lactam allergy: 11/17/10 Antimicrobials should be modified based on previous culture data. Aztreonam 1-2 g IV every 8 hours AND Azithromycin 500 mg orally or IV every 24 hours AND Vancomycin 15 mg/kg IV every 12 hours (rounded to closest 250 mg) 1. Clin Infect Dis: 2007; 44: S27-S72. 2. Am J Respir Crit Care Med 2005; 171:388-416. 11/17/10