Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
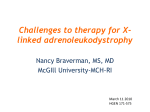
UvA-DARE (Digital Academic Repository) Translational studies in X-linked adrenoleukodystrophy Engelen, M. Link to publication Citation for published version (APA): Engelen, M. (2012). Translational studies in X-linked adrenoleukodystrophy General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) Download date: 10 Aug 2017 Extension of the phenotype Chapter 6 X-linked adrenomyeloneuropathy due to a novel missense mutation in the ABCD1 start codon presenting as demyelinating neuropathy Marc Engelen1,2, Anneke J. van der Kooi1, Stephan Kemp2, Ronald J.A. Wanders2, Erik A. Sistermans3, Johannes T.M. Koelman1, Hans R. Waterham2, Björn M. van Geel1, 4, Marianne de Visser1 Department of Neurology and 2Laboratory Genetic Metabolic Diseases, Academic Medical Center, Amsterdam; Department of Clinical Genetics, VU Medical Center, Amsterdam; and 4Department of Neurology, Medical Center Alkmaar, The Netherlands 1 3 Journal of the Peripheral Nervous System (2011) 16: 353 – 355 81 6 Chapter 6 6 X-linked adrenoleukodystrophy (X-ALD) is caused by mutations in the ABCD1 gene which encodes the adrenoleukodystrophy protein (ALDP), a peroxisomal transmembrane protein (Mosser et al 1993; Moser et al 2001). Several often overlapping phenotypes can be distinguished. Approximately, half of all patients develop adrenomyeloneuropathy (AMN), characterized by slowly progressive spastic paraparesis, peripheral neuropathy, sphincter dysfunction, and adrenocortical insufficiency (Moser et al 2001). We present a patient with an unusual neuropathy who was shown to have X-ALD caused by a mutation in the ABCD1 gene. A 27-year-old man presented with exercise-related weakness and fatigue in the legs which progressed slowly over the last 2 years. Three years prior to presentation he shortly used testosterone replacement therapy for decreased libido. Family history was negative for neuromuscular and endocrinological disorders. Physical examination revealed slight generalized wasting and weakness of the legs and decreased sensation for light touch at the dorsum of both feet with decreased position sense of the toes. Pes cavus was not present. Deep tendon reflexes were normal, and plantar reflexes were flexor. Electrophysiologic findings were compatible with a mild, symmetric demyelinating neuropathy confined to the lower limbs (Table 1). Serum creatine kinase activity was elevated (270 U/L, normal <193 U/L). Normal or negative results were obtained for thyroid stimulating hormone, sodium and potassium, and vasculitis parameters (anti-neutrophil cytoplasmic antibody, antinuclear antibody and complement levels). Cerebrospinal fluid examination showed elevated protein (0.66 g/L, upper limit of normal 0.49). DNA analysis revealed no mutations in the PMP22 gene. Refsum’s disease was considered, but the concentration of phytanic acid in plasma was normal. When phytanic acid levels are determined in our laboratory, we routinely include very long-chain fatty acids (VLCFA) as well. The VLCFA plasma C26:0 concentration was 4.32 μmol/L (normal 0.45–1.32 μmol/L), and C26:0/C22:0 ratio was 0.09 (normal ≤0.02). These results prompted mutation analysis of the ABCD1 gene, which revealed a missense mutation (c.1A>G) in the start codon of the ABCD1 gene, resulting in the substitution of the initiator methionine to a valine residue (p.Met1Val). The effect of the mutation on the stability of ALDP was investigated in cultured skin fibroblasts by means of immunofluorescence (IF) microscopy analysis and western blot analysis (Ligtenberg et al 1995). Both IF and western blot analysis showed no detectable ALDP (Figure 1). These data indicate that most likely translation is not initiated. Endocrinological investigations revealed mild adrenocortical insufficiency with a dehydroepiandrosteron sulphate level of 5.9 µmol/L (normal 8–17) that did not increase after administration of tetracosactide. The basal morning cortisol level was 250 μmol/L (normal 220–650) with a normal increase after administration of tetracosactide. The adrenocorticotropic hormone level was 14 ng/L (normal <55). There was also testicular insufficiency with a testosterone level of 7.9 nmol/L (normal 12.3–20), sex hormone binding globulin 18 nmol/L (normal 16–38), free androgen index 59.5 (normal 49–89), luteinizing hormone (LH) 4.0 U/L (<15), and follicle stimulating hormone (FSH) 3.1 U/L (normal 1.0–10.0). MRI of the cerebrum (Loes X-ALD severity score 0) (Loes et al., 1994) and spinal cord was normal. Additional DNA analysis revealed that the patient’s mother was an asymptomatic carrier for X-ALD. Recently, the patient’s tendon reflexes have become more brisk, suggestive of spinal cord involvement. X-ALD is a clinically heterogeneous disorder. Most patients either have childhood cerebral adrenoleukodystrophy or the AMN phenotype (Moser et al 2001). Our patient’s presentation is unusual in that he presented with exercise-related weakness and fatigue in the legs and was found to have a demyelinating neuropathy, only in the legs. We found one similar case in a series of teenagers with polyneuropathy (Kararizou et al 2006). Detailed 82 3.2 10.3 Tibial R 6.3 5.3 Tibial L Tibial R 3.3 6.6 Ulnar R Sural R Extensor digitorum brevis Peroneal L 76.4 31.5 Abductor digiti quinti Ulnar R 44.0 29.6 Abductor pollicis brevis 34 53 51 Sensory nerve conduction velocity (m/s) Minimal latency (ms) 5.0 18.4 18.3 Sensory nerve action potential (µV) Muscle F-waves 4.0 Median L Median L Nerve 31 28 52 52 43.4 1.9 4.7 19.8 18.6 Distal latency (ms) Sensory nerve Skin temperature was kept at 32 °C. Abnormal figures are shown in bold. L, left; R, right. M-wave (ms) Nerve H-wave (ms) 6.0 6.7 Peroneal L H-waves 19.5 3.2 20.5 3.5 Distal Proximal Motor nerve compound compound conduction muscle action muscle action velocity potential potential (m/s) (mV) (mV) Ulnar R Distal latency (ms) Median L Motor nerve Table 1: Electroneurographical features. Extension of the phenotype 6 genetic analysis and nerve conduction findings were not reported. Recently a patient with pes cavus, spasticity and a primarily demyelinating neuropathy with variable, focal slowing of motor nerve conduction velocities (NCVs) but relative preservation of motor and sensory 83 Chapter 6 Figure 1: The p.Met1Val mutation affects ALDP stability. The level of ALDP in fibroblasts from controls and X-ALD patients was determined by western blot analysis as described previously (Wanders et al., 1995). A monoclonal antibody, directed against an epitope between the amino acids 279 and 482 of the human ALDP was used. Lanes 1 and 4, protein extracts from two different control subjects; lane 2, the index patient; lane 3, protein extract from an X-ALD patient with a p.Arg554His mutation that results in no detectable ALDP (www.x-ald.nl). 6 amplitudes was described who was found to have both a PMP22 gene deletion consistent with a hereditary neuropathy with liability to pressure palsies and a c.1166G>A mutation in the ABCD1 gene, causing an amino acid substitution at codon 389 (p.Arg389His) (Hodapp et al 2006). Whether polyneuropathy in AMN patients is primarily demyelinating or axonal by nerve conduction studies is controversial. We have reported previously that polyneuropathy in this condition is predominantly axonal on electrophysiological examination (van Geel et al 1996), whereas Chaudhry et al. have reported that demyelination occurs more frequently (Chaudhry et al 1996). This is corroborated by histological studies of nerve biopsies of patients with AMN in whom also either a predominantly demyelinating or axonal neuropathy can be observed even within the same family (Schröder et al 1996). It is important to realize that X-ALD should be considered in the differential diagnosis of polyneuropathy at presentation, whether it is predominantly axonal or demyelinating. References Chaudhry V, Moser HW, Cornblath DR. 1996. Nerve conduction studies in adrenomyeloneuropathy. J Neurol Neurosurg Psychiatr 61:181–185. Hodapp JA, Carter GT, Lipe HP, Michelson SJ, Kraft GH, Bird TD. 2006. Double trouble in hereditary neuropathy: concomitant mutations in the PMP-22 gene and another gene produce novel phenotypes. Arch Neurol 63:112–117. Kararizou E, Karandreas N, Davaki P, Davou R, Vassilopoulos D. 2006. Polyneuropathies in teenagers: a clinicopathological study of 45 cases. Neuromuscul Disord 16:304–307. Ligtenberg MJ, Kemp S, Sarde CO, van Geel BM, Kleijer WJ, Barth PG, Mandel JL, van Oost BA, Bolhuis PA. 1995. Spectrum of mutations in the gene encoding the adrenoleukodystrophy protein. Am J Hum Genet 56:44–287. Loes DJ, Hite S, Moser H, Stillman AE, Shapiro E, Lockman L, Latchaw RE, Krivit W. 1994. Adrenoleukodystrophy: a scoring method for brain MR observations. AJNR Am J Neuroradiol 15:1761–1766. Moser H, Smith K, Watkins P, Powers J. 2001. X-linked adrenoleukodystrophy. In: The Metabolic & Molecular Bases of Inherited Disease. Scriver R, Beaudet AL, Sly WS, and Valle D (Eds). McGraw-Hill Inc., New York, pp 3257–3301. Mosser J, Douar AM, Sarde CO, Kioschis P, Feil R, Moser H, Poustka AM, Mandel JL, Aubourg P. 1993. Putative X-linked adrenoleukodystrophy gene shares unexpected Homology with ABC transporters. Nature 361:726–730. Schröder JM, Mayer M, Weis J. 1996. Mitochondrial abnormalities and intrafamilial variability of sural nerve biopsy findings in adrenomyeloneuropathy. Acta Neuropathol 92:64–69. van Geel BM, Koelman JH, Barth PG, Ongerboer de Visser BW. 1996. Peripheral nerve abnormalities in adrenomyeloneuropathy: a clinical and electrodiagnostic study. Neurology 46:112–118. Wanders RJ, Dekker C, Ofman R, Schutgens RB, Mooijer P. 1995. Immunoblot analysis of peroxisomal proteins in liver and fibroblasts from patients. J Inherit Metab Dis 18 (Suppl1):101–112. 84