Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
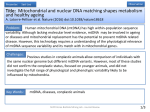
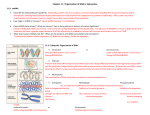
Reduction and Restoration of Mitochondrial DNA Content After Focal Cerebral Ischemia/Reperfusion Hong Chen, PhD; Chaur-Jong Hu, MD; Yong Y. He, MD; Ding-I Yang, PhD; Jan Xu, PhD; Chung Y. Hsu, MD, PhD Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Background and Purpose—Oxidative damage of mitochondrial DNA (mtDNA) in the ischemic brain is expected after ischemia/reperfusion injury. A recent study demonstrated limited patterns of mtDNA deletion in the brain after ischemia/reperfusion. We studied the ischemia/reperfusion-induced global changes of mtDNA integrity and its restoration in a rat model of transient focal ischemia in vivo. Methods—Changes in mtDNA content in the ischemic brain were assessed with the use of a rat stroke model featuring transient severe ischemia confined to the cerebral cortex of the right middle cerebral artery territory for 30 or 90 minutes. A new long polymerase chain reaction method, using mouse DNA as an internal standard, was applied to measure the relative content of intact rat mtDNA. Southern hybridization following alkaline gel electrophoresis was conducted in a parallel study to confirm long polymerase chain reaction results. Results—A reduction in mtDNA content was found after ischemia for 30 and 90 minutes. The mtDNA was restored to near nonischemic levels 24 hours after 30- but not 90-minute ischemia. Conclusions—These results confirm that ischemia/reperfusion causes mtDNA damages. Restoration of the mtDNA content to nonischemic levels after 30-minute ischemia raises the possibility that mtDNA repair or repletion occurs after brief ischemia. (Stroke. 2001;32:2382-2387.) Key Words: cerebral ischemia, focal 䡲 DNA damage 䡲 DNA, mitochondrial 䡲 DNA repair 䡲 rats M itochondria play a central role in necrotic and apoptotic cell death.1 A growing body of evidence has suggested that defects in mitochondrial DNA (mtDNA), such as mutations or deletions, may underlie the molecular mechanisms of various human diseases.2 In part because of the spatial proximity of mtDNA to the electron transport system, where oxidative phosphorylation occurs with the concomitant generation of free radicals or reactive oxygen species (ROS), the probability of oxidative damage to mtDNA is several times higher than nuclear DNA.3 Compelling evidence suggests that ischemia/reperfusion induces mitochondrial dysfunction by enhancing ROS generation, leading to the damage of intracellular proteins, lipids, and DNA.4 Previous studies have revealed specific patterns of mtDNA deletions, such as 3726, 4236, or 3867 bp, in transient global ischemia, traumatic brain injury, and focal ischemia.5,6 While the pathological consequence of such damages in brain injury models remains unclear, a strong correlation between the accumulation of oxidative mtDNA damage and the aging process has been established.7 Several cellular mechanisms, including endogenous free radical scavengers and intracellular antioxidants, are available to prevent mtDNA damage by ROS. In addition, the repair machinery removes the oxidative lesions on mtDNA. Furthermore, the replication systems may replenish the lost mtDNA. Both the repair and replication systems of mtDNA are distinct from those of nuclear DNA. For example, mitochondria appear to lack a nucleotide excision repair mechanism.8 Unlike nuclear DNA, mtDNA replication is coupled with the transcription process that is independent of the progression of cell cycle or replication of nuclear DNA.9 Nuclear DNA damages and subsequent repair occur after forebrain ischemia/reperfusion injury.10 –12 Limited patterns of mtDNA deletions have also been demonstrated in transient focal ischemia.6 However, the extent of mtDNA damage and its repair and/or replication have not been previously assessed in animal stroke models. Several approaches have been reported to measure the extent of mtDNA damage and repair. However, most of these methods allow the detection of a few deletion patterns. Quantitative assessment of the extent of mtDNA damage is limited by a number of technical pitfalls. These include variations in the yield of mtDNA during its isolation and the extent of mtDNA damage in the preparation process.8 We use a new long polymerase chain reaction (LPCR) method to explore changes in mtDNA content after ischemia/reperfusion in a rat stroke model, Received March 22, 2001; final revision received June 16, 2001;accepted June 22, 2001. From the Center for the Study of Nervous System Injury and Department of Neurology, Washington University School of Medicine, St Louis, Mo. Drs Chen and Hu contributed equally to this study. Correspondence to Chung Y. Hsu, MD, PhD, Center for the Study of Nervous System Injury and Department of Neurology, Washington University School of Medicine, 660 S Euclid Ave, Campus Box 8111, St Louis, MO 63110. E-mail [email protected] © 2001 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org 2382 Chen et al applying a novel internal standard to minimize the variations inherent to the assay procedures. Materials and Methods Focal Cerebral Ischemia/Reperfusion in Rats Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 A total of 48 male Long-Evans rats (weight, 300 to 350 g) were used in the present study. All animal procedures were approved by the Animal Care Committee of Washington University Medical Center and followed the guidelines for animal care established by the National Institutes of Health. The surgical procedures for focal ischemia affecting the cerebral cortex in the middle cerebral artery (MCA) territory have been previously described in detail13–15 with modifications. Briefly, the animals were anesthetized with a single injection of chloral hydrate (400 mg/kg IP). Body temperature was maintained at 37⫾0.5°C with a servo-controlled lamp connected to a rectal thermometer throughout surgery until recovery from anesthesia (return of righting reflexes). Microsurgical techniques were used to expose the right MCA. The MCA was ligated at the level of the inferior cerebral vein with 10-0 ophthalmic suture. Both common carotid arteries were then exposed by a midline cervical incision and clamped with vascular clips. At the end of ischemia (30 or 90 minutes), the suture was removed from the MCA, and common carotid arteries were unclamped to allow reperfusion for various period of time (0, 0.5, 4, or 24 hours). The animals were then decapitated under anesthesia to collect the brains. The right (ischemic) and left (control) MCA cortices were immediately dissected and separated from the subcortical structures.13 Samples were snapfrozen in liquid nitrogen and stored at ⫺70°C until use. In this model, ischemia for 30 minutes results in little or no infarction in the right MCA territory 24 hours after reperfusion. Ischemia for 90 minutes consistently generates a large infarct confined to the right MCA cortex at 24 hours.14,16 Total DNA Isolation Total DNA was purified with the use of the genomic DNA isolation kit from Qiagen. The frozen tissue was homogenized with a homogenizer and lysed with G2 buffer supplied in the kit. The amount of DNA was quantitatively determined with the use of PicoGreen (Molecular Probes), as previously described.17,18 LPCR for Quantification of mtDNA The mtDNA derived from rat or mouse brains was first linearized by digesting with restriction enzyme SacII (Promega). The quantification of intact mtDNA was achieved by means of a LPCR method19,20 with modifications. The reaction mixtures contained 0.4 ng of rat total DNA, 4 pmol of each oligonucleotide primer, 400 mol/L dNTP mixtures, and 0.5 U of LA Taq enzyme (Takara Shuzo Co, Ltd) in a total volume of 10 L. The same amount (0.4 ng) of total DNA derived from mouse brains was added to the polymerase chain reaction (PCR) reaction mixture to serve as an internal standard. The primers for the amplification of 14.3-kb mitochondrial genomes of both rat and mouse were 5⬘-ATATTT-ATCACTGCTGAGTCCCGTGG-3⬘ (forward) and 5⬘-AATTTCGGTTGGGGTGACCTCGGAG-3⬘ (reverse). The conditions for PCR consisted of denaturation for 1 minute at 94°C followed by 26 cycles of denaturation at 94°C for 15 seconds, annealing and extension at 68°C for 10 minutes, and a final extension at 72°C for 10 minutes. The PCR products were digested with restriction enzyme NcoI (Promega) at 37°C for 2 hours and fractionated through a 1% agarose gel containing 0.5 g/mL ethidium bromide. The DNA fragment of 14.3 kb represents the amplified rat mtDNA, whereas the 2 fragments of 7.0 and 7.3 kb, which cannot be resolved and therefore migrate as a single band on 1% agarose gel, represent the amplified mouse mtDNA that contains an NcoI restriction site. The intensities of these bands were assessed by image analysis (Molecular Dynamics) followed by the quantitative densitometer with the software ImageQuant (version 3.3, Molecular Dynamics). The relative content of rat mtDNA was derived by normalization with the mouse mtDNA in each sample. mtDNA in Focal Ischemia 2383 Alkaline Gel Electrophoresis and Southern Blotting Six micrograms of total DNA, including genomic and mitochondrial, was digested with 10 U of restriction enzyme SacII (Promega) to linearize mtDNA. After phenol/chloroform extraction and ethanol precipitation, the concentrations of the DNA samples were determined by the PicoGreen method, as described above. Five micrograms of each sample was loaded onto a 1% agarose gel. Gel electrophoresis was conducted at 0.5 V/cm for 24 hours in the buffer containing 30 mmol/L NaOH and 2 mmol/L EDTA. The gels were then neutralized, and DNA was transferred to Hybond N⫹ nylon membrane by capillary blotting. The membrane was prehybridized for 2 hours and hybridized overnight, both at 60°C, with the probes labeled with digoxigenin by PCR. This probe specifically recognizes the sequence of 16S ribosomal RNA (rRNA) in rat mtDNA. The labeling of this 413-bp 16S rRNA fragment was accomplished with the use of a PCR digoxigenin labeling/detection kit (Boehringer Mannheim Corporation) with the primer pair containing the following sequences: 5⬘-TAGAATGAATGGCTAAACGAGG-3⬘ (forward) and 5⬘-TTAATAGCTTCTGCACCATTGG-3⬘(reverse). Quantitative assessment of hybridization signal intensity was performed as previously described for LPCR. Statistical Analyses For comparisons between the left (control) and right (ischemic) MCA cortices at each time point, Student’s unpaired 2-tailed t test was used. For changes over time, 1-way ANOVA followed by Tukey test was used. A value of P⬍0.05 was considered significant. Results Optimization of LPCR Conditions A new strategy was applied in the quantitative LPCR to assess mtDNA contents by including a robust internal control. To optimize the experimental conditions for quantitative LPCR, we first test the amplification cycles (Figure 1A) and the amounts of template DNA (Figure 1B) to derive the optimal cycles and optimal mtDNA output within the linear ranges of the LPCR. A linear amplification pattern was achieved from 24 to 30 PCR cycles (Figure 1A) or between 0.1 and 0.8 ng total DNA (Figure 1B). For consistency, 26-cycle and 0.4-ng total DNA were selected for the subsequent experiments. LPCR for mtDNA Quantification Results in Figure 1 demonstrate that mtDNA can be successfully amplified out of a small fraction of total DNA isolated from the MCA cortex. However, the LPCR process could amplify slight variations inherently present in each sample and ultimately result in a substantial deviation in quantities of amplified products, leading to potentially erroneous conclusions. To resolve this issue, we developed a new LPCR approach to compare the relative rat mtDNA contents between different samples by including a known amount of mouse template DNA in each sample as an internal control. This approach is based on the high-sequence homology between the mouse and rat mitochondrial genomes with unique restriction enzyme sites not shared by the 2 species. Thus, the amplified products of rat and mouse mtDNA can be distinguished by a simple restriction enzyme digestion followed by gel electrophoresis. To ensure a linear correlation between the amounts of rat total DNA input and the amplified rat mtDNA in the presence of different amounts of the mouse template, we conducted LPCR using a combination of vari- 2384 Stroke October 2001 Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Figure 2. Validation of internal standards for LPCR. A, LPCR was performed with a combination of different amounts of rat and mouse templates. B, Representative LPCR assay of the relative mtDNA contents in the MCA cortices from rats subjected to 30- or 90-minute ischemia with or without reperfusion (4 or 24 hours). The numbers indicate the ratio of relative mtDNA contents between the ischemic right MCA cortex (R) and control left cortex (L) after normalization with the internal standards based on the mouse mtDNA template. Note that the ratio was restored to near 1.0 at 4 and 24 hours after 30-, but not 90-minute, ischemia. Figure 1. Optimization of experimental conditions for LPCR. A, Linear range of LPCR cycles. Rat total DNA (0.4 ng) was amplified with a primer pair specific for mtDNA for 22 to 30 cycles. Top, Ethidium bromide–stained agarose gel depicting the LPCR product of 14.3 kb. M indicates DNA molecular weight marker. Bottom, Correlation between the relative contents of amplified LPCR products and cycle numbers as determined by densitometry scanning of the agarose gel. B, Linear range of DNA input. Rat total DNA (0.1 to 0.8 ng) was amplified with mtDNA-specific primers for 26 cycles. The agarose gel and linear relationship between the amplified products and template inputs are shown in top and bottom panels, respectively. Data shown are representative of 3 independent experiments with similar results. able quantities of the rat and mouse templates to simultaneously amplify both mtDNA species. Despite the presence of both species, the relative content of the LPCR product of rat mtDNA is proportional only to the rat, but not the mouse, DNA input (Figure 2A). Thus, a linear relationship between the amounts of each template and the relative content of the respective PCR product can still be established with PCR mixtures containing DNA input from 2 different species (Figure 2A). Further analysis by densitometry scanning revealed that the amplification efficiencies are similar between the rat and mouse mtDNA within the linear ranges defined in preliminary studies (data not shown). Together these results suggest the feasibility to incorporate a known amount of mouse template to normalize the relative content of the rat LPCR product among different samples. A representative LPCR run to illustrate changes in mtDNA content in ischemic rat brains is shown in Figure 2B. The animals were subjected to either 30- or 90-minute focal ischemia followed by reperfusion for 0, 4, or 24 hours. The relative mtDNA content in the right MCA cortex was reduced by approximately half compared with the nonischemic left counterpart immediately after ischemia for 30 or 90 minutes. The amplified mouse LPCR product serving as internal standard for each sample remained unchanged. The relative mtDNA content was restored to near nonischemic levels at 4 and 24 hours after ischemia for 30, but not 90, minutes. Confirmation of LPCR Results by Southern Blot Analyses Southern blot analysis was implemented to further validate this LPCR method. We conducted 30- and 90-minute ischemia with or without reperfusion for 24 hours. A portion of total DNA prepared from these samples was subjected to alkaline gel electrophoresis and probed with a labeled 16S rRNA partial sequence in murine mitochondrial genome to quantitatively assess the relative contents of intact mtDNA. Another portion of the same DNA samples was subjected to the LPCR assay. When the results derived from Southern blotting (Figure 3A) and LPCR (Figure 3B) were compared, a strong correlation between these 2 methods for mtDNA quantitation could be established. Both approaches reveal that the mtDNA content, which was reduced as a result of 30-minute ischemia, was fully restored after 24-hour reperfusion, whereas 90-minute ischemia caused a reduction in mtDNA levels that was only partially restored at 24 hours. These findings suggest that LPCR is capable of providing an accurate, semiquantitative measure of the content of intact mtDNA. Reduction and Restoration of mtDNA Contents After Focal Ischemia To demonstrate that the LPCR assay of the mtDNA content is reproducible, we conducted another study in which 6 animals Chen et al Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Figure 3. Confirmation of LPCR results by Southern blot analysis. A, Rats were subjected to 30- or 90-minute ischemia with or without 24 hours of reperfusion. A portion of the total DNA isolated from the ischemic right MCA cortex (R) or the nonischemic left counterpart (L) was subjected to alkaline gel electrophoresis followed by hybridization with a mitochondrial 16S rRNA partial sequence labeled with digoxigenin, as described in detail in Materials and Methods. B, The same DNA samples used for Southern blotting were analyzed by LPCR. The numbers in the bottom rows in both A and B denote ratios of the relative mtDNA content in the ischemic right MCA cortex relative to the nonischemic left counterpart. Note the close association between relative mtDNA contents assessed by Southern blotting vs LPCR from the same set of samples. Representative data from 3 separate experiments with similar results are shown. per group were subjected to either 30- or 90-minute ischemia followed by reperfusion for 0, 0.5, 4, or 24 hours. In accord with results shown in Figure 2B and Figure 3, 30-minute ischemia caused a transient reduction of the relative content of intact mtDNA at the end of ischemia, suggesting extensive mtDNA damage that was partially restored as early as 30 minutes into reperfusion (Figure 4A). The relative mtDNA content recovered to levels comparable to the contralateral nonischemic counterpart after 4- or 24-hour reperfusion. In contrast, while 90-minute ischemia caused similar reduction in mtDNA contents, the restoration of mtDNA was not complete up to 24 hours after reperfusion (Figure 4B). Discussion A number of mechanisms may underlie the mtDNA damages after ischemic brain injury. The primary mechanism is likely to be oxidative stress. A major function of mitochondria is oxidative phosphorylation in the generation of energy supply to sustain normal cellular functions. ROS are byproducts of this important mitochondrial function. A higher steady state level of oxidative damage was noted in mtDNA than in nuclear DNA.3 Cerebral ischemia/reperfusion is accompanied by an increase in brain ROS content.21,22 ROS may damage mtDNA.4,23 Oxidative mtDNA damage may disrupt mitochondrial gene expression, resulting in mitochondrial dysfunction.24 Disturbances of mitochondria-specific gene expression occurred in the CA1 neurons at an early stage of reperfusion, leading to progressive failure of energy production and ultimately neuronal death.25 Mitochondrial swelling may also contribute to mitochondrial dysfunction. Cerebral mtDNA in Focal Ischemia 2385 Figure 4. Reduction and restoration of relative mtDNA contents after MCA ischemia/reperfusion. The relative mtDNA contents in animals that had undergone 30-minute (A) and 90-minute (B) ischemia without or with reperfusion for 0.5, 4, or 24 hours were compared. The relative content of mtDNA in each ischemic right MCA cortex (in percentage) was derived by using the nonischemic left MCA in the same animal as the denominator (100%). Values are mean⫾SEM; n⫽6. *P⬍0.05 compared with the nonischemic side; #P⬍0.05 compared with other groups by 1-way ANOVA followed by Tukey test. hypoxia-ischemia has been shown to cause mitochondrial swelling and calcium accumulation in the neonatal rat brain.26 Severe mitochondrial swelling may lead to the rupture of mitochondrial membranes, with resultant release of mtDNA that is susceptible to endonuclease digestion. Under such circumstances it is likely that mitochondrial swelling may contribute to the decreased mtDNA contents after ischemia/ reperfusion, which is an irreversible process. If this indeed occurs in vivo, then such a reduction of mtDNA contents can only be replenished with regeneration of mitochondria. In the present study a decrease in mtDNA content was restored to near control levels in the rats subjected to 30-minute, but not 90-minute, ischemia. It is therefore possible that short-term ischemia did not result in irreversible mitochondrial dysfunction, allowing oxidative mtDNA damages to be repaired or replenished. This may be one of the reasons why restoration of mtDNA was observed only in the rat brains subjected to 30-minute, but not 90-minute, ischemia. Endonuclease activation may also cause mtDNA damage. Nuclear DNA fragmentation mediated by endonucleases is a common feature of cells dying of apoptosis or necrosis and has been noted in the ischemic brain after cerebral ischemia/reperfusion.16 Whether mtDNA damage involves endonuclease action remains to be determined. After 30-minute ischemia, the mtDNA content was reduced initially but fully restored after 4- and 24-hour reperfusion. The recovery that began as early as 30 minutes after reperfusion could be due to DNA repair, replication, or both. 2386 Stroke October 2001 Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Measurement of mtDNA content based on the LPCR method does not distinguish between mtDNA repair and mtDNA replication. An increase in mtDNA content has been shown to be the early molecular event of human cells in response to mild oxidative stress such as exposure to hydrogen peroxide.27 It remains to be determined whether a change in mitochondria number occurs in the rat brain cortices after cerebral ischemia/reperfusion. Despite the changes in mtDNA contents as determined by LPCR, it is important to note that higher DNA content may not necessarily represent higher DNA integrity and/or mitochondrial function. The primer pair for LPCR was designed such that a PCR product of 14.3 kb was amplified out of the total mtDNA, which is 16.3 kb. Since the amplified products cover approximately 88% of the whole mtDNA genome, we believe that it is a reasonable index for the integrity of endogenous mtDNA present in the rat brains after ischemia/reperfusion. It should be noted, however, that higher DNA content may not represent higher DNA integrity and function. At least 3 mechanisms may contribute to failure in restoring mtDNA content to nonischemic levels after 90-minute ischemia. First, severe oxidative stress may render the damaged mtDNA irreparable. Severe ischemia/reperfusion can induce acute tissue necrosis.13 Second, severe ischemic injury may result in certain types of mtDNA damages that are irreparable because of the lack of specific DNA repairing mechanisms. For example, UV-induced pyrimidine dimers are not removed from mtDNA since mitochondria do not possess nucleotide excision repair machinery.28 Finally, irreversible release of mtDNA through ruptured mitochondrial membrane secondary to mitochondrial swelling may occur after severe ischemic brain injury. Electron microscopy may be used to examine the ultrastructure of mitochondria at subcellular level. Previously LPCR has been shown to be a sensitive method to assess the extent of DNA damage, repair, or replication, in a semiquantitative fashion.29 In this study we report a new approach using a simple and universally applicable internal standard to reduce variations inherent to PCR. The highsequence homology shared by the target DNA (rat mtDNA) and internal standard (mouse mtDNA) allows the concomitant amplification of both rat and mouse mtDNA using only 1 pair of primers with approximately similar efficiencies. The end products derived from the target template are then distinguished from the internal standard by NcoI restriction enzyme digestion because the recognition sequence of NcoI is only present in the mouse, but not rat, mtDNA. Similar strategy can be applied to determine the mouse mtDNA levels with the use of rat mtDNA as internal standards. A number of control experiments were conducted to assess the reliability and sensitivity of this LPCR approach. We optimized the cycle numbers to be used such that maximal sensitivity may be achieved without overamplification (Figure 1A). Pilot experiments were conducted to establish a linear relationship between the quantities of template DNA and those of LPCR products (Figure 1B). When templates from 2 species were amplified simultaneously, the amounts of LPCR products yielded were only in proportion to the respective templates (Figure 2A). Southern blot analysis coupled with alkaline gel electrophoresis confirmed the LPCR results (Figure 3). This LPCR method, however, carries certain limitations. For examples, this method does not address the patterns of oxidative mtDNA damage. Moreover, this LPCR technique cannot provide spatial information with regard to the distribution of mtDNA lesions or changes in mtDNA content in a specific area of brain cortex that may sustain irreversible mtDNA damage and undergo apoptosis. Other in situ techniques will have to be developed to characterize the spatial distribution of mtDNA lesions, including those at the subcellular level. In conclusion, short-term (30-minute) ischemia caused transient reduction in mtDNA content, which was nearly restored to nonischemic levels within 4 hours of reperfusion; longer duration of ischemia, causing a large infarct, was associated with reduction in mtDNA content that was not fully restored on reperfusion up to 24 hours. The mechanism(s) that restore mtDNA content after brief ischemia to near nonischemic levels remains to be explored but may involve mtDNA repair and/or repletion. Acknowledgments This work was supported by grants NS25545, NS28995, and NS40525. We thank Dr Grace Ku for her critical review. References 1. Halestrap AP, Doran E, Gillespie JP, O’Toole A. Mitochondria and cell death. Biochem Soc Trans. 2000;28:170 –177. 2. Brown MD, Wallace DC. Molecular basis of mitochondrial DNA disease. J Bioenerg Biomembr. 1994;26:273–289. 3. Richter C. Oxidative damage to mitochondrial DNA and its relationship to ageing. Int J Biochem Cell Biol. 1995;27:647– 653. 4. Chan PH. Role of oxidants in ischemic brain damage. Stroke. 1996;27: 1124 –1129. 5. McDonald RP, Horsburgh KJ, Graham DI, Nicoll JA. Mitochondrial DNA deletions in acute brain injury. Neuroreport. 1999;10:1875–1878. 6. Zeng Z, Zhang Z, Yu H, Corbley MJ, Tang Z, Tong T. Mitochondrial DNA deletions are associated with ischemia and aging in Balb/c mouse brain. J Cell Biochem. 1999;73:545–553. 7. Barja G, Herrero A. Oxidative damage to mitochondrial DNA is inversely related to maximum life span in the heart and brain of mammals. FASEB J. 2000;14:312–318. 8. Croteau DL, Stierum RH, Bohr VA. Mitochondrial DNA repair pathways. Mutat Res. 1999;434:137–148. 9. Taanman JW. The mitochondrial genome: structure, transcription, translation and replication. Biochim Biophys Acta. 1999;1410:103–123. 10. Liu PK, Hsu CY, Dizdaroglu M, Floyd RA, Kow YW, Karakaya A, Rabow LE, Cui JK. Damage, repair, and mutagenesis in nuclear genes after mouse forebrain ischemia-reperfusion. J Neurosci. 1996;16: 6795– 6806. 11. Nagayama T, Lan J, Henshall DC, Chen D, O’Horo C, Simon RP, Chen J. Induction of oxidative DNA damage in the peri-infarct region after permanent focal cerebral ischemia. J Neurochem. 2000;75:1716 –1728. 12. Nagayama T, Simon RP, Chen D, Henshall DC, Pei W, Stetler RA, Chen J. Activation of poly(ADP-ribose) polymerase in the rat hippocampus may contribute to cellular recovery following sublethal transient global ischemia. J Neurochem. 2000;74:1636 –1645. 13. Chen ST, Hsu CY, Hogan EL, Maricq H, Balentine JD. A model of focal ischemic stroke in the rat: reproducible extensive cortical infarction. Stroke. 1986;17:738 –743. 14. Yip PK, He YY, Hsu CY, Garg N, Marangos P, Hogan EL. Effect of plasma glucose on infarct size in focal cerebral ischemia- reperfusion. Neurology. 1991;41:899 –905. 15. He YY, Hsu CY, Ezrin AM, Miller MS. Polyethylene glycol-conjugated superoxide dismutase in focal cerebral ischemia-reperfusion. Am J Physiol. 1993;265:H252–H256. Chen et al 16. Du C, Hu R, Csernansky CA, Hsu CY, Choi DW. Very delayed infarction after mild focal cerebral ischemia: a role for apoptosis? J Cereb Blood Flow Metab. 1996;16:195–201. 17. Ahn SJ, Costa J, Emanuel JR. PicoGreen quantitation of DNA: effective evaluation of samples pre- or post-PCR. Nucleic Acids Res. 1996;24: 2623–2625. 18. Singer VL, Jones LJ, Yue ST, Haugland RP. Characterization of PicoGreen reagent and development of a fluorescence-based solution assay for double-stranded DNA quantitation. Anal Biochem. 1997;249: 228 –238. 19. Barnes WM. PCR amplification of up to 35-kb DNA with high fidelity and high yield from lambda bacteriophage templates. Proc Natl Acad Sci U S A. 1994;91:2216 –2220. 20. Cheng S, Fockler C, Barnes WM, Higuchi R. Effective amplification of long targets from cloned inserts and human genomic DNA. Proc Natl Acad Sci U S A. 1994;91:5695–5699. 21. Cao W, Carney JM, Duchon A, Floyd RA, Chevion M. Oxygen free radical involvement in ischemia and reperfusion injury to brain. Neurosci Lett. 1988;88:233–238. 22. Chan PH. Reactive oxygen radicals in signaling and damage in the ischemic brain. J Cereb Blood Flow Metab. 2001;21:2–14. mtDNA in Focal Ischemia 2387 23. Floyd RA, Carney JM. Free radical damage to protein and DNA: mechanisms involved and relevant observations on brain undergoing oxidative stress. Ann Neurol. 1992;32:S22–S27. 24. Murakami K, Kondo T, Kawase M, Li Y, Sato S, Chen SF, Chan PH. Mitochondrial susceptibility to oxidative stress exacerbates cerebral infarction that follows permanent focal cerebral ischemia in mutant mice with manganese superoxide dismutase deficiency. J Neurosci. 1998;18:205–213. 25. Abe K, Kawagoe J, Itoyama Y, Kogure K. Isolation of an ischemiainduced gene and early disturbance of mitochondrial DNA expression after transient forebrain ischemia. Adv Neurol. 1996;71:485–503. 26. Puka-Sundvall M, Gajkowska B, Cholewinski M, Blomgren K, Lazarewicz JW, Hagberg H. Subcellular distribution of calcium and ultrastructural changes after cerebral hypoxia-ischemia in immature rats. Brain Res Dev Brain Res. 2000;125:31– 41. 27. Lee HC, Yin PH, Lu CY, Chi CW, Wei YH. Increase of mitochondria and mitochondrial DNA in response to oxidative stress in human cells. Biochem J. 2000;348(pt 2):425– 432. 28. Clayton DA, Doda JN, Friedberg EC. The absence of a pyrimidine dimer repair mechanism in mammalian mitochondria. Proc Natl Acad Sci U S A. 1974;71:2777–2781. 29. Ferre F. Quantitative or semi-quantitative PCR: reality versus myth. PCR Methods Appl. 1992;2:1–9. Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Reduction and Restoration of Mitochondrial DNA Content After Focal Cerebral Ischemia/Reperfusion Hong Chen, Chaur-Jong Hu, Yong Y. He, Ding-I Yang, Jan Xu and Chung Y. Hsu Downloaded from http://stroke.ahajournals.org/ by guest on August 10, 2017 Stroke. 2001;32:2382-2387 doi: 10.1161/hs1001.097099 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2001 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/32/10/2382 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/